
Shabana Ali*, Asad Ali Azeemi, MBBS, FCPS (Medicine)**, Saffia Shoukat***
*Assistant Professor of Anatomy, Islamic International Medical College, Riphah International University, Islamabad (Pakistan)
**Research fellow, Islamabad (Pakistan)
*** Associate Professor of Anatomy, Islamabad Medical and Dental College, Behria University
Correspondence: Dr Asad Ali Azeemi,MBBS, FCPS (Medicine); E-mail: aaazeemi@gmail.com
ABSTRACT
Introduction: Spina bifida is an important developmental defect of vertebral column. There are various types of spina bifida. The commonest one is spina bifida occulta (SBO), in which patients do not show any sign and symptoms as there is no herniation of spinal canal contents. This lesion is present at birth. Incidence of spina bifida decreases with age. The prevalence of spina bifida is related to various factors. Genetic predispositions, environmental factors and teratogenic effects of the drugs are important. It may be caused by the prenatal use of drugs like valproic acid. Sacral hiatus is used for caudal epidural block. We conducted this cross sectional study to find out the incidence of SBO in our population.
Methodology: This was an observational descriptive study. This study was carried out in Islamic International Medical College Rawalpindi. The duration of study was six months. Bones were studied in five different medical colleges of Rawalpindi with the consent of the concerned authorities. A total of 200 sacra were selected. The damaged and defective bones were excluded. All the studied bones were complete. All bones were studied for prevalence of SBO in our population. Bones having apex of sacral hiatus till S4 were considered normal. The remaining bones were divided into four grades according to level of failure of closure of sacral laminae. Bones with partial closure between two or more adjacent sacral vertebrae (incomplete spina bifida) were included in Grade I and II. Bone with sacral hiatus extending beyond S4 ( long hiatus)were included in grade III and all bones with open dorsal wall representing the complete failure of fusion of the laminae from S1-S5 were included in grade VI. Results were analyzed by SPSS 17.
Results: The spina bifida was found in 69 bones with an overall incidence of 34.5% among 200 bones. Out of 69 variants, bones were grouped in two groups; one having complete and incomplete SBO among adjacent vertebrae, other having long hiatus. Prevalence of grade-1 SBO was 5.5% while it was 4.5% for grade- IV SBO. Region between S1- 2 was the most common site for grade-1 anomaly. Incidence of long hiatus from S5-3 was higher i.e., 46 (23%) while 2 sacra had hiatus ending at S2.
Conclusion: Presence of spina bifida occulta should always be kept in mind while dealing with patients of backache, urinary and neurological symptoms. It may also be the cause of failure of caudal epidural block.Studies with larger sample size and including different ethnic groups from different regions of Pakistan are required to note the regional and ethnic disparities in the anatomy of the sacral hiatuses.
Key words: Sacrum; Long hiatus; Spina bifida; Backache, Caudal epidural block
Citation: Ali S, Azeemi AA, Shoukat S. The prevalence of spina bifida occulta in Pakistani population: A study of dry human sacra. Anaesth Pain & Intensive Care 2014;18(2):157-161
INTRODUCTION
Vertebral column faces a number of developmental defects. These defects are common and variable, ranging from a single defect involving only one vertebra to full length defects of spine1. Spina bifida is an important developmental defect of spine. There are various types of spina bifida. Commonest one is spina bifida occulta (SBO) where patients do not show any sign and symptoms because there is no herniation of spinal canal content. It is discovered either accidently on radiograph or posthumously on the study of dry human sacra. More severe forms of spina bifida presents with clinical signs and symptoms due to involvement of spinal meninges and nerves.
The lesion is present at birth. Incidence of spina bifida decreases with age as two halves of the posterior arch fuse between the ages of 5 and 8 years.2 A higher incidence is found in parents having multiple vertebral anomalies along with SBO.1 More severe types of spina bifida occur in families having higher incidence of spina bifida.
The prevalence of spina bifida is related to various factors;3 genetic predispositions, environmental factors, teratogenic effects of drugs are important.4 It may be caused by the prenatal use of drugs like Valproic acid.5 Some of the cases are preventable by genetic counseling and regular administration of folic acid6 during pregnancy. For this purpose, information is required concerning the prevalence of spina bifida.7
The outcomes depend upon the number of segments involved. As the number of segments involved increases, there are more chances of neurological as well as urological dysfunction.8
Spina bifida can be associated with number of disorders like intraspinal lipoma, tethered cord syndrome, genitourinary dysfunction, increased incidence of disc pathology, lumbar spondylolysis, foot deformities and syringomyelia.8 Although vast majority of people with SBO are asymptomatic, but they may exhibit functional disorders of lower urinary tract in children. Complete spina bifida has definite neurologic outcomes.9-11
The sacral hiatus is used in caudal epidural anesthesia to act on the sacral and coccygeal nerves. This is often employed to relax the perineal musculature for painless childbirth as well as anal, perineal, urological, gynecological operations that do not involve the anterior abdominal wall.12
The reliability, success and safety of caudal epidural anesthesia depend upon the ability to locate the hiatus and to define is anatomical variations.13
The risk for neural tube defects is approximately 3 to 7%. It is more common in first born children. There is also evidence for involvement of second degree relatives in the SBO. A family in whom spina bifida cystica had already occurred, their second child can have multiple congenital vertebral defects.14
Relationship between SBO and various conditions needs to be determined by population based studies. Nevertheless, a preliminary analysis about the prevalence of SBO in dry human sacra gives a fair idea about the importance of further studies in population at increased risk of severe grades of this malformation.
Due to clinical importance of SBO, a number of studies have been carried out internationally to see its prevalence. Keeping in view the clinical importance of morphology of sacrum, this study was designed to see the prevalence of spina bifida in Pakistan by using the bony landmarks of the sacrum. It is hoped that this will help to improve the success rate of caudal epidural block and it will help clinicians in the management various disorders.
METHODOLOGY
This was an observational descriptive study. This study was carried out in Islamic International Medical College Rawalpindi. Bones were studied in five different medical colleges of Rawalpindi and two medical colleges in the Peshawar after the consent of concerned authority. Duration of study was 8 months from May 2011- December 2011. A total of 200 Pakistani sacra were selected. The damaged and defected bones were excluded. All the studied bones were complete. Bones having apex of sacral hiatus till S4 were considered normal. We observed all bones for long sacral hiatus and complete spina bifida. Bones with partial closure between two or more adjacent sacral vertebrae were grouped as incomplete spina bifida and all those having open dorsal wall representing the complete failure of fusion of the laminae from S1-S5 were labeled as complete spina bifida. Bones with sacral hiatus extending beyond S4 were considered as having long hiatus.
The bones were observed and findings were divided into four grades, e.g. I-IV;
Grade 1- incomplete spina bifida between two adjacent sacral vertebrae
Grade 2- incomplete spina bifida among more than two adjacent vertebrae
Grade 3- long sacral hiatus involving more than two sacral vertebrae
Grade 4- complete spina bifida involving all sacral arches.
Results were analyzed by SPSS 17.
RESULTS
The prevalence of spina bifida and long hiatus in dry human sacra of Pakistani population is summarized in Tables 1 and 2.
|
Spina bifida level |
Grade |
Frequency |
Percentage |
|
S1-2 |
I |
7 |
3.5 % |
|
S2-3 |
I |
2 |
1 % |
|
S3-4 |
0 |
0 |
0 |
|
S2-3-4 |
II |
1 |
0.5 % |
|
S3-4 |
I |
2 |
1 % |
|
Open canal |
IV |
9 |
4.5% |
|
Total |
21 |
10.5% |
Table 1: Prevalence of spina bifida occulta in Pakistani population
|
Description |
No. |
Percentage |
| Long hiatus ending at S2 |
2 |
1 % |
| Long hiatus ending at S3 |
46 |
23 % |
| Total |
48 |
24 % |
Table 2: Prevalence of long hiatus in Pakistani population
The spina bifida was found in 69 bones with an overall prevalence of 34.5 % among 200 bones. Out of 69 variants, bones were grouped in two groups; one having SBO among adjacent vertebrae, and the other having long hiatus.
In first group, grade-1 SBO showed higher prevalence and was found in 9 bones with overall prevalence of 5.5%. Region between S1-2 was the most common site for grade-1 anomaly. Grade-II SBO was seen only in 0.5% of bones while none of all had grade-3 SBO. Grade-4 SBO was a common anomaly with prevalence of 4.5%.
In second group, bones were classified according to the length of sacral hiatus. Prevalence of long hiatus from S5-3 was higher i.e., 46 with percentage of 23%, while 2 sacra had hiatuses ending at S2.

Figure 1: Open dorsal wall; complete spina bifida
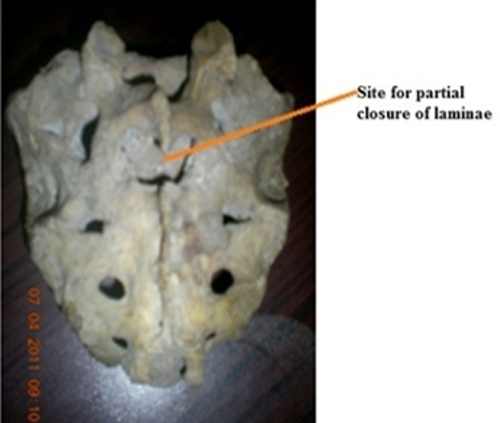
Figure 2: Partial closure of dorsal wall between S1 and S2; incomplete spina bifida

Figure 3: Long sacral hiatus ending at S2

Figure 4: Partial closure of dorsal wall between S1 and S2; incomplete spina bifida
DISCUSSION
Spina bifida is a congenital anomaly of multifactorial origin. SBO develops due to the hypoplasia of one or both components of neural arch. This anomaly occurs frequently in human beings. It is as common in males as in females and young adults show high rate of occurrence15.The incidence of SBO decreases with age, possibly as a result of new bone formation or calcification8.
Knowledge of the length of sacral hiatus is very important to avoid dural puncture during caudal epidural block. As the apex lies higher in long hiatus, precaution should be taken to decide the length of needle to be introduced into the canal. However, a low apex requires a long needle.
In this study, we identified that sacral hiatal variations are of two types: long hiatus of sacrum, and sacra with independent SB at various levels. Long hiatus at S3 level was more common: it matches with the prevalence in Indian population sacra where it was30%,16 and in another study it was found to be 20.6%.17 Long hiatus up to S2 was relatively uncommon, which is closer to the Indian population with a prevalence of 2.63%18, 3.42%19 and0.5% 17 as sited by different studies.
Incidence of SBO varies among different population: it was 1% in Japanese population,20 and 1.5%19 and 2 %17 in Indian population. But the values are very high among other populations; it being 17% among Israeli population, 28.1% among Chinese population and only 3.33% in the Egyptians.21 The most common site of spina bifida for Chinese22 and Israeli people was at S1–2, while long hiatus from S3 to S5 was the most common among Egyptian people. Prevalence of complete SBO was very high in our population as compared to <2% of British,23 zero% in Australian24 and 3.33% in Egyptian population.21
SBO can occur at any segment of the sacrum. Researchers have used many ways to calculate the incidence of SBO. Some used dry bones and others used x-rays and CT scans. Research has proved that a great portion of sacra may be varied among various populations.
Location of spina bifida is very important and has a number of clinical implications. A wide range of clinical problems may develop in people with SBO. Patients can have urological as well as neurological symptoms.25 Urinary complaints include upper and lower neuron types of bladder and urethral dysfunctions.10The commonest defects reported are between either at S1 or between S1 and S2.13 SBO of S1 leads to posterior herniation of lumbar vertebrae and risk of this particular herniation increases with advancement of age.26 Studies on children with primary nocturnal enuresis have proved that its treatment outcomes depend upon location of SBO; the patients with SBO of L5 and S1 are less responsive to treatment.11 On plain abdominal x-ray, significant correlation has been found between lower urinary tract dysfunction and presence of SBO.27
CONCLUSION
Presence of spina bifida occulta should always be kept in mind while dealing with patients of backache, urinary and neurological symptoms. A large disparity in the results among various populations can be due to genetic endowment and environmental conditions. The prevalence of spina bifida occulta in our population was found to be equivalent to Indian population. Studies with larger sample size and including different ethnic groups from different regions of Pakistan are required to note the regional and ethnic disparities in the anatomy of the sacral hiatuses.
REFERENCES
- Davies RW. Congenital vertebral anomalies: etiology and relationship to spina bifida cystica. Journal of medical genetics 1975;12:290. [PubMed][Free Full Text]
- Mehdizadeh M, Roohi A, Hemami M and Esfahani ST. Is there any association between spina bifida occulta and primary vesicoureteral reflux? Iran J Pediatr 2010;20:349-352. [PubMed][Free Full Text]
- Källén B, Löfkvist E. Time trends of spina bifida in Sweden 1947-81. J Epidemiol Community Health. 1984;38:103-7. [PubMed][Free Full Text]
- Windham GC, bjerkedal T. Secular trends of neural tube defects by demographic subgroups in Norway 1977-81. Niph Ann 1982;5:57-67. [PubMed]
- Ceylan S, Duru S, Ceylan S. Valproic acid sodium-induced spina bifida occulta in the rat. Neurosurg Rev 2001;24:31-4. [PubMed]
- Lary JM, Edmonds LD. Prevalence of spina bifida at birth–United States, 1983-1990: a comparison of two surveillance systems. MMWR. CDC Surveillance Summaries: MMWR CDC Surveill Summ. 1996;45:15-26. [PubMed][Free Full Text]
- Andrew E, Czeizel, Dudas I. prevention of the first occurrence of neural tube defects by periconceptional vitamin supplementation. N Engl J Med 1997;327:1832-5. [PubMed][Free Full Text]
- Gregerson DM. Clinical consequences of spina bifida occulta. J Manipulative Physiol Ther. 1997;20:546 – 50. [PubMed]
- Silverman FN, Slovis TL. Congenital malformations, In: Kuhn JP, Slovis TL, Haller JO (eds): Coffey’s pediatric diagnostic imaging. 10th ed. Mosby: Philadelphia, 2004;pp. 654-67.
- Sakakibara R, Hattori T, Uchiyama T, Kamura K, Yamanishi T. Uroneurological assessment of spina bifida cystica and occulta. Neurourol urodyn 2003;22:328-334. [PubMed]
- Miyazato M, Sugaya K, Nishijima S, Owan T, Ogawa Y. Location of spina bifida occulta and ultrasonographic bladder abnormalities predict the outcome of treatment for primary nocturnal enuresis in children. Int J Urol 2007;14:33-8. [PubMed]
- Mohammad S, Khan A. Clinical anesthesia for students.2nd edition. The Army Press: Pakistan; 1989
- Ilana EN, Thiago NF , Arthur VRS, Pedro PK. Caudal epidural anesthesia: an anesthetic technique exclusive for pediatric use? Is it possible to use it in adults? What is the role of the ultrasound in this context? Rev Bras Anesthesiol 2011;61:123-132. [PubMed]
- Doolin MT, Barbaux S, McDonnell M, Hoess K, Whitehead AS, Mitchell LE. Maternal genetic effects exerted by genes involved in homocysteine remethylation influence the risk of spina bifida. Am J Hum Genet 2002;71:1222–1226. [PubMed][Free Full Text]
- Fidas A, MacDonald HL, Elton RA, Wild SR, Chisholm GD, Scott R. Prevalence and patterns of spina bifida occulta in 2707 normal adults. Clin Radiol 1987;38:537- 42. [PubMed]
- Kumar A, Sharma A, Singh P. Anatomical study on dry human sacra for caudal epidural block. J Anaesth Clin Pharmacol. 2010;26:94-96.
- Rajapur P. Morphometric study of sacral hiatus using dry human sacra. MD thesis. Rajiv Gandhi University of Health Sciences, Bangalore. India;2008.
- Aggarwal A, Aggarwal A, Harjeet, Sahnni D. Morphometry of sacral hiatus and its clinical relevance to caudal epidural block. Surg Radiol Anat. 2009;31:793-800. [PubMed]
- Nagar SK. A study of sacral hiatus on dry human sacra. J Anat Soc India. 2004;53:18-21.
- Sekiguchi M, Yabuki S, Satoh K, Kikuchi S. An anatomic study of the sacral hiatus: A basis for successful caudal epidural block. Clin. J. Pain. 2004;20:51–54. [PubMed]
- El‐Din S, Mohamed A, El Banna RAE. Congenital anomalies of the vertebral column: a case study on ancient and modern Egypt. Int. J Osteoarchaeol 2006;16:200-207. [Journal Abstract]
- Wu LP, Li YK, Li YM, Zhang YQ, Zhong SZ Variable morphology of the sacrum in a Chinese population.Clin Anat 2009;22:619-626. [PubMed]
- Saluja PG. The incidence of spina bifida occulta in a historic and a modern London population. J Anat 1988;158:91–93. [PubMed][Free Full Text]
- Albrecht TL, Scutter SD, Henneberg M. Radiographic method to assess the prevalence of sacral spina bifida occulta. Clin Anat 2007;20:170-4. [PubMed]
- Begeer JH, Wiertsema GP, Breukers SM, Mooy JJ, ter Weeme CA. Tethered cord syndrome: clinical signs and results of operation in 42 patients with spina bifida aperta and occulta. Z Kinderchir 1989;44:5-7. [PubMed]
- Avrahami E, Frishman E, Fridman Z, Azor M. Spina bifida occulta of S1 is not an innocent finding. Spine (Phila Pa 1976) 1994;19:12-5. [PubMed]
- Samuel M, Boddy SA. Is spina bifida occulta associated with lower urinary tract dysfunction in children? J Urol 2004;171:2664-6. [PubMed]
