
Dinesh Singh*, Sulekha Saxena**, Jai Shree Bogra***, Ajay Kr. Chaudhary****, Girish Chandra***, Shashi Bhushan***
*Associate Professor, **MD Student, ***Professor, ****Assistant Professor
Department of Anesthesiology, KG’s Medical University, Lucknow (India).
Correspondence: Dr. Sulekha Saxena, MD Student, Department of Anesthesiology, King George Medical University, Lucknow (India); Cell: 09359618480; E-mail: dr.sulekha2008@rediffmail.com
ABSTRACT
Objective: To study the comparative effects of parenteral and oral glutamine therapy on biochemical parameters and reduction in the hospital stay of critically ill patients.
Study design: Randomized controlled trial.
Study site: Trauma Ventilatory Unit, Trauma Centre, King George Medical University, Lucknow.
Methodology: 120 critically ill patients aged 16-60 years admitted to Trauma Ventilatory Unit, Trauma centre KGMU, Lucknow. The patients were randomly divided into 3 equal groups, 40 in each group: Group A (control group) received no glutamine; Group B received oral glutamine 20 g/d for 5 days and Group C received l-alanyl-l-glutamine dipeptide 0.3 g/kg/d by intravenous infusion for 5 days. Complete blood count was done at regular intervals of 24 hours. Total proteins and serum albumin were recorded at 5 day intervals. Single blinding was done.
Results: The total leukocyte counts (TLC) levels in all the three groups increased after the treatment and the observed increase was least evident in Group C (18.7%), followed by Group B (32.5%) and it was the highest in Group A (38.2%). A similar observation was made for CRP and lymphocyte levels in all of the three groups. However, a significant decrease was found in total protein and albumin levels. The mean duration of hospital stay of Group C was the least followed by Group B and Group A.
Conclusion: Parenteral glutamine in a dose of 0.3 g/kg/d was more efficacious than 20 g/d oral glutamine in increasing/decreasing in the biochemical parameters after the therapy. The duration of hospital stay was similar in all the groups after treatment.
Key words: Glutamine; C-reactive protein; CRP; Hospital stay
Citation: Singh D, Saxena S, Bogra JS, Chaudhary AK, Chandra G, Bhushan S. A comparative study of the parenteral and oral glutamine on biochemical parameters and on the duration of ICU stay in critically ill patients. Anaesth Pain & Intensive Care 2013;17(2):123-127
INTRODUCTION
Standard amino acid formulations do not contain amino acid glutamine, due to pharmaceutical stability problems. In the past glutamine was considered a non-essential amino acid, therefore its omission from parenteral nutritional preparations was not considered to be a problem; rather it was thought that the human body would synthesise its own. Glutamine has an essential role in acid-base balance, nitrogen transport and maintaining muscle mass and function, and it is an energy source for rapidly dividing cells particularly those of the immune system and the gut. As the most abundant amino acid in the body, it is now recognised that glutamine synthesis and release is insufficient to meet demands under severe metabolic stress. Glutamine must therefore be supplied from extraneous nutritional sources if its normal level is to be maintained. Several studies have shown that glutamine level decreases markedly after major surgery and during critical illness. Decreased serum glutamine has been associated with immune dysfunction in animal models and death or infectious complications in septic patients. Glutamine is the most prevalent free protein amino acid in the humans. In the extracellular fluid it constitutes approximately 25%.1 Free glutamine concentrations differ in various tissue pools with considerable differences between species in tissue free glutamine concentrations. While it is often possible to make qualitative analysis concerning human metabolism on the basis of animal studies,2 a quantitative understanding may require direct measurement of glutamine in humans. Plasma contains only a very small proportion of the free glutamine pool. The main use of glutamine in the basal state as well as during critical illness is as an oxidative substrate. Endogenous production of glutamine may become insufficient during critical illness. The shortage of glutamine is reflected as a decrease in plasma concentration, which is a prognostic factor for poor outcome in sepsis. Because glutamine is a precursor for nucleotide synthesis, rapidly dividing cells are most likely to suffer from a shortage. Therefore, exogenous glutamine supplementation is necessary. The major part of endogenously produced glutamine comes from skeletal muscle. It has been seen that for patients staying for a long time in the intensive care unit (ICU), the muscle mass decreases rapidly, which leaves a tissue of diminishing size to maintain the source of glutamine. The rationale for treatment with glutamine supplementation in critically ill patients is the shortage of glutamine, the clinical evidence, and the fact that it is not harmful to patients. Grou et al3 in a multicenter, prospective, double-blind, randomized trial, studied in 2011, the clinical efficacy of alanine-glutamine dipeptide-supplemented total parenteral nutrition defined by the occurrence of nosocomial infections.
The objective of the present study was to evaluate the effect of parenteral glutamine and oral glutamine in critically ill patients with the primary objective to measure changes in the biochemical parameters such as total leukocyte count, C-reactive protein (CRP), lymphocyte count, serum protein and serum albumin levels. The secondary objectives were to measure the effect on duration of hospital stay, morbidity and mortality.
METHODOLOGY
The study was conducted from August 2011 to July 2012 on critically ill patients aged 16-60 years, admitted to Trauma Ventilatory Unit, Trauma Centre, King George Medical University Lucknow. The study was approved by the Institutional Ethical Committee. The informed consent from each of the patient was taken before enrollment.
Using assumptions about the primary endpoint, we assumed that a sample size of 40 in each group was required to differentiate between the two groups.
Participants were randomised by sealed envelope after enrolment. Numbers in the envelopes were generated by a computer generated randomization table (http://www.randomization.com), based on blocks of three to assign patients to treatment group or placebo group. The patients were divided into following three groups:
Group A (control group): No glutamine administration
Group B: Oral glutamine 20 g/d for 5 days
Group C: l-alanyl–l-glutamine dipeptide 0.3 g/kg per day intravenous infusion for 5 days
Baseline parameters such as age, total leukocyte count, CRP, lymphocyte count, serum protein and serum albumin levels were estimated on Day 1 by standard methods in the pathology laboratories of the institute. After that, complete blood count was recorded at regular intervals of 24 hours; total protein and albumin levels were recorded at 5 day intervals along with blood culture and urine culture. Single blinding was done; only the patients were blinded to the study group.
All the patients undergoing study were monitored for pulse rate, blood pressure (systolic, diastolic and mean), respiration and electrocardiography. All the patients were investigated daily for TLCand lymphocyte counts; while total proteins, serum albumin and CRP were measured on day 1 and day 5. The secondary efficacy variable e.g. length of hospital stay was noted.
Data analysis: Data were summarized as Mean±SE. The outcome measures (lymphocyte count, total leukocyte count, CRP, serum total protein and albumin levels) of three groups were compared by two factor (Groups and Days) repeated measures analysis of variance (ANOVA) using general linear models (GLM) and the significance of mean difference within and between the groups was done by Newman-Keuls post hoc test. Age and duration of hospital stay between the groups were compared by one factor ANOVA and the significance of mean difference between the groups was done by Newman-Keuls test. A two-sided (α=2) p<0.05 was considered statistically significant.
RESULTS
In all three groups, the proportion of males was higher than the females. On comparing the sex proportion (M/F) between the three groups, χ2 test revealed similar (p>0.05) sex proportion between the three groups (M/F: 30/10 vs. 24/16 vs. 16/4, χ2=2.13; p=0.34). Among the three groups, the mean age of Group C was the highest followed by Group A and then Group B. Demographic data and duration of surgery was similar among the groups; mean age 38.05 ± 3.38years, 35.40 ± 2.89 years and 44.70 ± 2.87 years in control group, oral glutamine group and Parenteral glutamine group respectively (Table 1). Thus, all the three groups were comparable according to age and sex. There was no significant differences among the groups according to type of trauma, surgical process and co-morbidities (Data not shown).
Table 1: Demographic profile of the patients
|
Demographic profile |
Group A (n=40) |
Group B (n=40) |
Group C (n=40) |
χ2 and p-value |
|
| Gender | Male |
30 (75%) |
24 (60%) |
32 (80%) |
2.13, 0.34 |
| Female |
10 (25%) |
16 (40%) |
8 (20%) |
||
| Age in years* | mean ± SD |
38.05 ± 0.38 |
35.40 ± 0.89 |
44.70 ± 0.87 |
2.46, 0.09 |
| Range |
(17-60) |
(16-59) |
(24-60) |
||
The total leukocyte counts (TLC) levels in all the three groups increased after the treatment and the observed increase was the least in Group C (18.7%), followed by Group B (32.5%); Group A showing the highest increase (38.2%). The CRP levels in all three groups increased after the treatment. The increase was 49.6% in Group C, 54.4% in Group B and 62.3% in Group A being the highest. The lymphocyte count in all three groups increased after the treatment and the increase was 28.8%, 37.9% and 41.0% in Group C, Group A and in Group B respectively. The increase in lymphocyte count from day 1 to day 5 was statistically significant (p<0.0001). The total protein levels in all the three groups significantly decreased (p=0.0002) by 23.3%, 36.7% and 39.6% in Group C, Group B and Group A respectively. The albumin levels in all three groups decreased after the treatment. The decrease was 5.3%, 16.1% and 24.1% in Group C, Group B and Group A respectively (p<0.01) (Table-2).
Table 2: Day by day changes in the biochemical parameters (Mean ± SE) of three groups
|
Groups |
Day 1 (Baseline) |
Day 5 |
% mean change (Day 1-5) |
p-value |
| Total leukocyte count levels (cells/mm3) | ||||
| Group A |
6005.00 ± 111.33 |
9720.00 ± 473.71 |
+38.2% |
<0.0001* |
| Group B |
5820.00 ± 140.23 |
8627.50 ± 144.98 |
+32.5% |
<0.0001* |
| Group C |
5805.00 ± 119.31 |
7140.00 ± 198.60 |
+18.7% |
<0.0001* |
| C Reactive Protein levels (mg/l) | ||||
| Group A |
17.07 ± 0.75 |
45.26 ± 6.70 |
+62.3% |
0.0002* |
| Group B |
16.54 ± 0.98 |
36.30 ± 3.55 |
+54.4% |
0.0006* |
| Group C |
15.71 ± 0.85 |
31.16 ± 2.25 |
+49.6% |
0.009* |
| Lymphocyte count levels (cells/mm3) | ||||
| Group A |
1417.50 ± 23.02 |
2282.50 ±102.55 |
+37.9% |
<0.0001* |
| Group B |
1308.60 ± 65.47 |
2217.50 ± 92.29 |
+41.0% |
<0.0001* |
| Group C |
1479.00 ± 69.41 |
2077.50 ± 85.08 |
+28.8% |
<0.0001* |
| Serum protein levels (g/l) | ||||
| Group A |
5.91 ± 0.12 |
4.23 ± 0.15 |
-39.6% |
0.0002* |
| Group B |
6.09 ± 0.14 |
4.46 ± 0.19 |
-36.7% |
0.0002* |
| Group C |
6.41 ± 0.16 |
5.20 ± 0.15 |
-23.3% |
0.0002* |
| Serum albumin levels (g/l) | ||||
| Group A |
3.81 ± 0.08 |
3.07 ± 0.07 |
-24.1% |
0.0002* |
| Group B |
4.08 ± 0.11 |
3.52 ± 0.09 |
-16.1% |
0.0001* |
| Group C |
3.89 ± 0.09 |
3.70 ± 0.09 |
-5.3% |
0.0001* |
*Significant
The mean duration of hospital stay of Group C was the least followed by Group B and Group A. On comparing the mean duration of three groups, ANOVA revealed similar (p>0.05) hospital stay of all three groups (F=2.98, p=0.06). In other words, treatments did not change the duration of hospital stay (Fig 1).
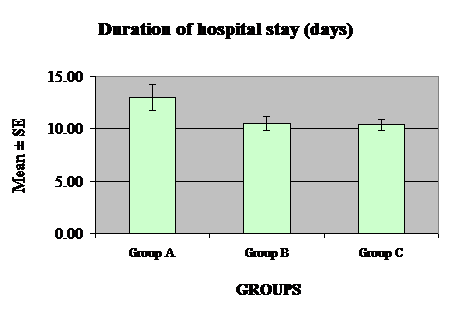
Fig. 1: Mean (± SE) Duration of hospital stay of three groups
DISCUSSION
This study was conducted to compare the efficacy of parenteral glutamine and oral glutamine. We measured lymphocytes count on each day of the therapy in the three groups. The TLC level in all the three groups increased after the treatment and the increase was evident least in Group C followed by Group A; Group B being with the highest increase. Similarly, the total leukocyte count levels in all three groups increases after the treatment and the increase was evident least in Group C followed by Group B and Group A the highest. However, the TLC levels differed significantly between Group A and Group C at day 2 and between all three groups at day 5. Keeping with this background, it is pertinent to speculate about the particular mechanism underlying the effect of glutamine dipeptide in causing reversal of the clinical and biochemical signs of critical illness. Obviously, there are distinct priorities of glutamine utilization during stress yet it is likely that the observed beneficial effects with supplemental glutamine are interrelated. The line of reasoning is supported by the fact that obvious beneficial effects on the immune system and GI tract can be achieved with low amount of supplemental glutamine4. In our study, total protein levels in all three groups decreased after the treatment and the decrease was evident least in Group C (23.3%) followed by Group B (36.7%) and Group A with the maximum (39.6%) decrease. Total protein levels did not differed between the three groups at day 1, while at day 5 it differed significantly between Group A and Group C and Group B and Group C. This result was in contrast to study done by Griffith et al (1997),5 in which he found that there was no change in protein and albumin levels after treatment for five days with glutamine. Similar changes were studied by Sunil et al (2007)6 in studies of using glutamine enriched TPN in patients of acute pancreatitis. In the body, glutamine is used for the nitrogen requirements of immune system cells, enterocytes, for nitrogen resources of metabolic activities, and for filling the glutamine pool.7,8 In some studies, it has been shown that TPN without glutamine had similar beneficial effects on the nitrogen balance like the glutamine enriched TPN.9,10
The level of CRP is the indicator of the most important biological function in the body, the role of which is to recognize and to stimulate the clearance of the cell remnants. In our study, the mean percent change in the CRP levels, from day 1 to day 5, increased in all the groups after the treatment. This increase was least evident in Group C (49.6%) followed by Group B (54.4%) and Group A the maximum increase (62.3%). At day 5, mean CRP level of Group C increased significantly (p=0.008) less as compared to Group A. The decrease in the treatment group was pronounced, but the values were still higher than the normal. The high CRP levels may be due to the presence of the factors that affecting the CRP levels such as fever, leukocytosis and surgical operation as well as the presence of the inflammation. In a previous study investigating the effects of standard and glutamine-enriched PN on AP, CRP levels were determined for the evaluation of systemic inflammatory response, and CRP concentrations of the patients had decreased in the treatment group, whereas CRP level in the control group had decreased at the first week and increased thereafter. Glutamine is, generally, accepted as an immune modulatory agent. In many studies performed on humans and animals, glutamine has beneficial effects on the immune system cells and their functions, thus reduction in infection rates was observed.11
We measured lymphocytes count on each day of the therapy in the three groups. In all three groups it increased significantly after the treatment. However, in some other studies, these effects have not been observed.4,17
In our study, total protein and albumin levels in all three groups significantly decreased after the treatment. Total protein levels did not differ between the three groups at day 1 while at day 5 it differed significantly (p<0.001) between Group A and Group C and Group B and Group C. This result was in contrast to study done by Griffith (1997),5 in which he found that there was no change in protein and albumin levels after treatment for five days with glutamine.
Several previous studies reported that glutamine supplementation to TPN shortens the length of hospital stay.15,12,14,16 In our study, the mean duration of hospital stay of Group C was the least followed by Group B and Group A.
CONCLUSIONS
Parenteral glutamine in a dose of 0.3 g/kg/d is more efficacious than 20 g/d oral glutamine in optimising the biochemical parameters in critically sick patients. However, the duration of hospital stay remains unaffected after the treatment.
REFERENCES
- Bergström J, Fürst P, Norée LO, Vinnars E. Intracellular free amino acid concentration in human muscle tissue. J Appl Physiol 1974;36:693-7. [PubMed]
- Fürst P. Regulation of intracellular metabolism of amino acids. In: Bozetti F, Bionogi R, editors. Nutrition in trauma and cancer sepsis. Karger: Basel; 1985.
- Grau T, Bonet A, Miñambres E, Piñeiro L, Irles JA, Robles A, et al. The effect of l-alanyl-l-glutamine dipeptide supplemented total parenteral nutrition on infectious morbidity and insulin sensitivity in critically ill patients. Crit Care Med. 2011 Jun;39(6):1263-8. [PubMed]
- Van der Hulst RR, Van Kreel BK, Von Meyenfelt MF, Brummer RJ, Arends JW, Deutz NE, Soesters PB. Glutamine and the preservation of gut integrity. Lancet 1993;44:1363–1365. [PubMed]
- Griffiths RD. Outcome of critically ill patients after supplementation with glutamine. Nutrition 1997;13:752-4. [PubMed]
- Kumar S, Kumar R, Sharma SB, Jain BK. Effect of oral glutamine administration on oxidative stress, morbidity and mortality in critically ill surgical patient. patients. Indian J Gastroenterol. 2007;26:70-73. [PubMed]
- Ziegler TR, Szeszycki EE, Estivariz CF, Puckett AB, Leader LM. Glutamine: from basic science to clinical application. Nutrition 1996;12:68–70. [PubMed]
- Furst P, Pogan K, Stehle P. Glutamine dipeptides in clinical nutrition. Nutrition 1997;13:731–737. [PubMed]
- Sitzman JV, Steinborn PA, Zinner MJ. Total parenteral nutrition and alternate energy substrates in treatment of severe acute pancreatitis. Surg Gynecol Obstet 1989;168:311–317. [PubMed]
- Scolapio JS, Malhi-Chowla N, Ukleja A. Nutrition supplementation in patients with acute and chronic pancreatitis. Gastroenterol Clin North Am1999;28:695–707. [PubMed]
- O’Riordain MG, Fearon KC, De Beaux A. Effects of glutamine on immune function in the surgical patient. Nutrition 1996;12:84–86. [PubMed]
- Ziegler TR, Bye RL, Persinger RL, Young LS, Antin JH, Wilmore DW. Effects of glutamine supplementation on circulating lymphocytes after bone marrow transplantation: a pilot study. Am J Med Sci 1998;315:4–10. [PubMed]
- Karwowska KA, Dworacki G, Trybus M, Zeromski J, Szulc R. Influence of glutamine enriched parenteral nutrition on nitrogen balance and immunological status in patients undergoing elective aortic aneurysms repair. Nutrition 2001;17:475–8. [PubMed]
- Ockenga J, Borchert K, Rifai K, Manns MP, Bischoff SC. Effect of glutamine-enriched total parenteral nutrition in patients with acute pancreatitis. Clinical Nutrition 2002;21(5): 409-16. [PubMed]
- McBurney M, Young LS, TR Ziegler, Wilmore DW. A costevaluation of glutamine supplemented parenteral nutrition in adult bone marrow transplant patients. J Am Diet Assoc 1994; 94(11):1263–6. [PubMed]
- Neri A, Mariani F, Piccolomini A, Testa M, Vuolo G, Di Cosmo L. Glutamine supplemented total parenteral nutrition in major abdominal surgery. Nutrition 2001;17:968–9. [PubMed]
