
Haxhire Gani, PhD*, Vjollca Beqiri**, Pirro Prifti***, Majlinda Naco, PhD*, Rudin Domi*, Orjana Janushaj, PhD*, Bilbil Hoxha, PhD****
*Consultant Anaesthesist Reanimatore Doctor; **Nurse; ***Associate Professor; ****Consultant Urologist
Rruga e Dibres, Qendra Spitalore Universitare “Mother Teresa”. Tirana (Albania).
Correspondence:Haxhire Gani, Rruga “5 Maj”, perballe kolegjit “Tirana Jonë ” Kulla Nr .2,Allias.Tirane (Albania); E-mail: haxhiregani@yahoo.com; Cell: 0355 672053588
ABSTRACT
Background and objectives: Sevoflurane is widly used in pediatric anesthesia as children tolerate it well, but it often gives postoperative agitation. The objective of this study was to test the effect of small doses of ketamine together with midazolan in reducing agitation from sevoflurane in children.
Methodology: We enrolled 80 children from 3-10 years old, undergoing urological surgery under general anesthesia, in this randomized double blind prospective study. Participants were randomly divided into two groups. The first group (Group M) received midazolam 0.5 mg/kg orally and the second group (Group KM) received oral midazolam plus ketamine 2 mg/kg. For general anesthesia, we used sevoflurane. Induction was done with fentanyl, thiopental and sexamethonium and then the patient was intubeted. Five different levels were used to measure the degree of agitation. Agitation was managed by fentanyl 1 µg/kg IV and total dose used was noted.
Results: The demographic data were statistically equivalent in both groups. There was no significant difference between two groups regarding awakening period or hospital discharge. Patients in Group KM had a significantly lower agitation score compared to Group M. (Mann Whitney T=15; p<0.01). Fentanyl consumption was significantly greater in Group M compared to the Group KM.
Conclusion: Adding small doses of ketamine by mouth beside midazolam reduces episodes of agitation after sevoflurane anesthesia in children undergoing urology procedures without delaying hospital discharge.
Key words: General anesthesia; Urology surgery; Fentanyl; Sevoflurane; Postanesthesia agitation
Citation: Gani H, Beqiri V, Prifti P, NacoM, Domi R, Janushaj O, Hoxha B. Oral midazolam plus ketamine compared to midazolam only to reduce agitation in children undergoing urological surgery after sevoflurane anesthesia. Anaesth Pain & Intensive Care 2014;18(3):237-240
INTRODUCTION
Sevoflurane is widely used in pediatric anesthesia because it is well tolerated by inhalation, gives fast induction and recovery, has lower level of hepatic toxicity and offers hemodynamic stability. Regardless of its advantages, there is a growing concern that sevoflurane causes postanesthesia agitation (PAA) in pediatric patients. Research shows that the incidence of agitation may be as high as 67%. Both desflurane and sevoflurane, which are more insoluble agents, have been associated with a higher level of postoperative emergence agitation as compared to halothane and propofol.7,8-20
Agitation in children can present as disorientation in time and place, confusion, and decreases child’s level of responsiveness. Furthermore, it causes hypersensitivity to pain and motor hyperactivity in the immediate post procedure period. These changes can lead to serious complications including removal of surgical dressings, contaminating the wound, and removal of IV lines and/or Foley catheter. A situation like this is unacceptable by parents or attendants. Regardless of the use of anti-anxiety medication and analgesics, nothing has been effective in preventing agitation in children who received sevoflurane as an anesthetic. This complication may also lead to extended hospital stay and delayed recovery. Midazolam and/or ketamine are widely used in pediatric anesthesia and are found to decrease emotional trauma, and secure gradual induction but their ability to decrease agitation has been controversial.21-24
The objective of this study is to discover the effect that ketamine has on agitation post surgery when ketamine is used with midazolam on children that used sevoflurane and are undergoing urology procedures, compare with cases when children used only midazolam.
METHODOLOGY
This study took place in UHC Mother Teresa for one year from September 2012-September 2013.In the urology clinic participants of this study were 80 healthychildren between 3-10 years of age, operated in our clinic with no other active disease. All clinical and lab readings were within normal limits. Participants had urology surgery using general anesthesia. Participants were randomly divided into two groups, the first group, Group-M, received midazolam 0.5 mg/kg and the second group (Group-KM) received midazolam and ketamine 2 mg/kg.
Children with mental developmental problems such as Down syndrome and epilepsy were not included on the study. On the pre-op visit weight of all children was recorded to effectively calculate pre-medication dose. The drugs for pre-medication were prepared by one of the anesthesiologists in a syringe and was given to the nurse. With parents’ cooperation this medication was given to children on the morning of the scheduled surgery. Anesthesia was induced with sevoflurane for 1-2 min, IV line established and atropine 0.015 mg/kg, fentanyl 1µg/kg, thiopental 8 mg/kg, and suxamethonium 1 mg/kg given and endotracheal intubation performed. Maintenance of anesthesia was carried with sevoflurane in O2 and N2O. After intubation 0.01 mg/kg pancuronium and ketoprofen were given to the child. All participant were continuously monitored with EKG, pulse oximeter and non-invasive arterial blood pressure every 5 min. At the end of the procedure sevoflurane was discontinued, O2 100% started and muscle relaxation was reversed withneostigmine and atropine.
Statistical analysis: Statistical analysis of the data was performed using SPSS-11 software. Continuous variables were compared by means of t-test. Chi square was used to compare the proportions between variables and Mann-Whitney test was used to compare the score between groups. Statistical significance was set for p≤0.05. All tests are two-tailed.
Table 1: Preoperative behavior scales
| Acceptance score (palatability) | |
| Good | 1: Readily accept 2: Dislike but accept |
| Poor | 3: Held down/forced to accept 4: Refuses to open mouth after tasting |
|
Agitation level score |
Description |
| 1 | Deep sleep not responding to stimulant |
| 2 | Sleeping, but responsive to stimulant and movement. |
| 3 | Awake and responds normal. |
| 4 | Crying and very difficult to comfort. |
| 5 | Unacceptable behavior, pt wild and dangerousCan be stopped only if is restrained. |
Once the patients were out of the operating room the parents were required to stay with them.
To manage agitation we used fentanyl 1µ/kg IV.
RESULTS
The demographic data of the patients e.g. age, weight, sex of the patients and the duration of the operation in minutes is shown in Table 1. The mean duration of the surgery was 84.27 ± 17.02 in the midazolam group and 85.6 ± 23.31in ketamin plus midazolam group. The average age was equivalent in both groups 4.15 ± 1.07 vs. 4.18 ± 1.1 in the midazolam group vs. ketamine plus midazolam group respectively.
There was statistically no difference in average weight in the groups 18.5 ± 3.4 vs. 18.2 ± 3.1(P 0.8). Similarly M:F ratio was equivalent in both groups (Table 3).
Table 3: Demographic data
|
Parameter |
Group M N 40 |
Group KM N 40 |
test |
p-value |
| Age in years (Mean ± SD) |
4.15 ± 1.07 |
4.18 ± 1.1 |
t= -0.12 |
0.8 |
| Weight in kg (Mean ± SD) |
18.5 ± 3.4 |
18.2 ± 3.1 |
t= 0.41 |
0.5 |
| GenderMale |
29 (72.5%) |
28 (70%) |
||
| Female |
11 (27.5%) |
12 (30%) |
χ2=0 |
0.8 |
| Surgery procedure in min(Mean ± SD) |
84.27 ± 17.02 |
85.6 ± 23.31 |
t= -0.29 |
0.7 |
No statistical difference was observed between two groups with regard to baseline characteristics e.g. age, gender, weight and the health status of the children as well as the length of surgical procedures.
Table 4: Comparison of agitation level and fentanyl consumption between two groups
|
Parameter |
Group M |
Group KM |
| Fentanyl consumed (ug) (Mean±SD). |
7.5±10.12 |
1.4±1.2 |
| Agitation levelScore 1 |
4 |
1 |
| score 2 |
5 |
0 |
| score 3 |
3 |
1 |
| score 4 |
3 |
1 |
| score 5 |
10 |
2 |
t-test = 3.7 p<0.001
Fentanyl consumption was significantly greater in Group M compared to the Group KM.
Figure 1. Comparison of agitation level between two groups
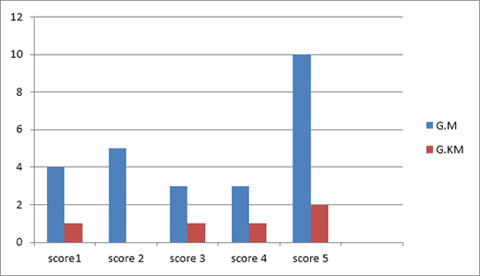
Mann Whitney T=15; p<0.01
Patients in Group KM had a significantly lower agitation score compared to Group M. (Mann Whitney T=15; p<0.01).
Figure 2: Time period that patients opened the eyes (min)

t = -14.6; p<0.001
The time period to open the eyes was greater among the patients in the Group KM (t = -14.6; p<0.001)but not significant statistically. The amount of fentanyl used was also more in the Group M compared to Group KM.
DISCUSSION
Even though there is an increased3levelof postanesthesia agitation level with the use of sevoflurane, in the majority of cases the agitation level decreases after 20-30 min and children recovered by themselves. Pain could be a cause of agitation as well.4It has been seen that the intra-operative administration of non steroidal anti-inflammatory agents5 decreases agitation due to sevoflurane. Use of clonidine, dexmedetomidine, and fentanyl has been proven to decrease agitation after anesthesia with sevoflurane. Agitation may be associated with pain, as there is evidence that it is reduced when both groups receive ketoprofen for pain. Agitation after propofol6has shown to be less severe and patients recover faster compared with to sevoflurane. Increased agitation level with the use of sevoflurane is explained with the effect of the gas on nervous system, especially in children. Episodes of epilepsy have been noted in the post-anesthesia period with sevoflurane in non-epileptic children. This reaction can be connected with the fast accumulation of sevoflurane in the brain. When γ-aminoabutric acid ergcproperties and sevoflurane can cause changes in balance between and innervations of synaptic neurons. Ketamine is an NMDA receptor antagonist and it can stop “wind up phenomenon” (central sensitization) on the spinal neurons.7 Exactly in this effect are ketamine’s analgesic, amnesic, psychomimetic and neuroprotective effects connected.8 To some extent oral preventive use of ketamine gives a better analgesic effect compared with the group that received only midazolam; and it also leads to decreased post-anesthesia agitation level with sevoflurane. Some previous studies also mentioned this effect of ketamine and the use of ketamine as a preventive agent in pediatric anesthesia. In these studies ketamine was not used by mouth but by parenteral route, which can lead to high and fast build-up of concentration in the brain and may present with the side effect of this medication.
Limitations: A small sample size of the patients makes the significance of this study limited but it may serve to supplement other studies that have discussed the use of ketamine as a preventive measure for post-anesthesia agitation associated with sevoflurane.
CONCLUSION
Ketamine use, beside oral midazolam as pre-medication in children undergoing urology procedures decreased post-anesthesia agitation incidence when sevoflurane is used as inhalational agent without delaying recovery process or hospital discharge.
REFERENCES
1.Samarkandi A, Naguib M, Riad W, Thalaj A, Alotibi W, Aldammas F et al. Melatoninvs.midazolam premedication in children :double –blind, placebo-controlled study .Eur J Anesth 2005 ; 22-; 189-196. [PubMed]
2. Roelofse JA, Louw LR, Roelofse PG. A double blind randomized comparison of oral trimeprazine-methadone and ketamine-midazolam for sedation of pediatric dental patients for oral surgical procedures. Anesth Prog 1998; 45: 3–11. [PubMed][Free Full Text]
3. Deshpande S, Platt MP, Aynsley-Green A. Patterns of the metabolic and endocrine stress response to surgery and medical illness in infancy and childhood. Crit Care Med 1993;21:S359 – 61. [PubMed]
4. Aspinall RL, Mayor A. A prospective randomized controlled study of the efficacy of ketamine for postoperative pain relief in children after adenotonsillectomy. Paediatr Anaesth 2001; 11: 333–336. [PubMed]
5. Marcus RJ, Victoria BA, Rushman SC .and Thompson J. P. Comparison ketamine and morphine for analgesia after tonsillectomy children. Br J Anaesth 2000; 84: 739–742. [PubMed][Free Full Text]
6. Viitanen H, Annila P, Viitanen M, Yli-Hankala A. Midazolam premedication delays recovery from propofol-induced sevofluranee anesthesia in children 1–3 yr. Can J Anaesth 1999;46:766 –71. [PubMed]
7. Liu HT, Hollmann MW, Liu WH , Hoenemann CW, Durieux ME. Modulation of NMDA receptor function by ketamine and magnesium: Part I. Anesth Analg 2001; 92: 1173–1181. [PubMed]
8. Woolf CJ, Thompson SW. The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain 1991; 44: 293–299. [PubMed]
9. Welborn LG, Hannallah RS, Norden JM, Ruttimann UE, Callan CM. Comparison of emergence and recovery characteristics of sevoflurane, desflurane, and halothane in pediatric ambulatory patients. Anesth Analg 1996;83:917-20. [PubMed]
10. Grundmann U, Uth M, Eichner A, Wilhelm W, Larsen R. Total intravenous anesthesia with propofol and remifentanil in paediatric patients: a comparison with a desflurane-nitrous oxide inhalation anaesthesia. Acta Anaesthesiol Scand 1998;42:845. [PubMed]
11. Lerman J, Davis PJ, Welborn LG, Orr RJ, Rabb M, Carpenter R. Induction, recovery and safety characteristics of sevoflurane in children undergoing ambulatory surgery: A comparison with halothane. Anesthesiology 1996;84:1332-40. [PubMed][Free Full Text]
12. Sury MR, Black A, Hemington L, Howard R, Hatch DJ, Mackersie A.. A comparison of the recovery characteristics of sevoflurane and halothane in children. Anaesthesia 1996;51:543-6. [PubMed]
13. Lapin SL, Auden SM, Goldsmith LJ, Reynolds AM. Effects of sevoflurane anaesthesia on recovery in children: a comparison with halothane. Paediatr Anaesth 1999;9:283-6. [PubMed]
14. Beskow A, Westrin P. Sevoflurane causes more postoperative agitation in children than does halothane. Acta Anaesthesiol Scand 1999;43:536. [PubMed]
15. Davis PJ, Greenberg JA, Gendelman M, Fertal K. Recovery characteristics of sevoflurane and halothane in preschool-aged children undergoing bilateral myringotomy and pressure equalization tube insertion. Anesth Analg 1999;88:34-8. [PubMed]
16. Cravero JP, Beach M, Dodge CP, Whalen K. Emergence characteristics of sevoflurane compared to halothane in pediatric patients undergoing bilateral pressure equalization tube insertion. J Clin Anesth 2001;12:397-401. [PubMed]
17. Cravero J, Surgenor S, Whalen K. Emergence agitation in paediatric patients after sevoflurane anaestheaia and no surgery: a comparison with halothane. Paediatr Anaesth 2000;10:419-24. [PubMed]
18. Picard V, Dumont L, Pellegrini M. Quality of recovery in children: sevoflurane versus propofol. Acta Anaesthesiol Scand 2000;44:307-10. [PubMed]
19. Uezono S, Goto T, Terui K, Ichinose F, Ishguro Y, Nakata Y. Emergence agitation after sevoflurane versus propofol in pediatric patients. Anesth Analg 2000;91:563-6. [PubMed]
20. Cohen IT, Finkel JC, Hannallah RS, Hummer KA, Patel KM. Rapid emergence does not explain agitation following sevoflurane anaesthesia in infants and children: a comparison with propofol. Paediatr Anaesth 2003;13:63-7. [PubMed]
23. Viitanen H, Annila P, Viitanen M, Yli-Hankala A. Midazolam premedication delays recovery from propofol-induced sevoflurane anesthesia in children 1 – 3 years. Can J Anaesth 1999;46:766-71. [PubMed]
24. Cohen IT, Drewsen S, Hannallah RS. Propofol or midazolam do not reduce the incidence of emergence agitation associated with desflurane anaesthesia in children undergoing adenotonsillectomy. Paediatr Anaesth 2002;12:604-9.
