
Aparna Girwalkar-Bagle*, Marry Samuel**, Sandeep Choudhary***
*Associate professor; **Professor; ***Resident
Department of Anesthesiology, Pad. Dr. D Y Patil Medical College, Pimpri, Pune, Maharashtra (India)
Correspondence: Dr Aparna Girwalkar (Bagle), Flat No. 103, Aster 1, Sukhawani Campus, opp. Vallabhnagar Bus Stand, Pimpri, Pune, Maharashtra (India); Mobile: 91-9922504009; E-mail: draparnabagle@gmail.com
ABSTRACT
Laparoscopic surgical techniques have expanded tremendously within the last two decades and increasingly being used to treat intraperitoneal pathology. These minimally invasive techniques offer decreased operating time, decreased morbidity and decreased length of hospital stay. These procedures, however, are not completely safe and without potential morbidity. Massive and life threatening extraperitoneal pneumodissection after laparoscopic procedures is one of the uncommon complications associated with it. Here we describe a case of massive subcutaneous emphysema with prolonged hypercarbia.
Keywords: Subcutaneous emphysema; Hypercarbia; Laparoscopic surgery
Citation: Girwalkar-Bagle A, Samuel M, Choudhary S. Massive subcutaneous emphysema and hypercarbia associated with laparoscopy. Anaesth Pain & Intensive Care 2015;19(1):50-53
INTRODUCTION
Subcutaneous emphysema is defined as the presence of gas (e.g. CO2) within the subcutaneous tissues.¹ It is identified by an increased smooth bulging of the skin and by deep palpation that produces a crackling sensation (crepitus) as the gas moves through the tissue.
A 4 point scale was used for comparing varying degree of subcutaneous emphysema as follows;¹
0 = no subcutaneous emphysema
1 = mild emphysema with crepitus at trocar insertion sites or in the groin
2 = marked emphysema with crepitus extending to the abdomen and thighs
3 = massive emphysema extending to the chest or neck and face
Facial and neck swelling indicate the severity of peumodissection. However, clinically significant subcutaneous emphysema after laparoscopic procedures is not frequent, varying in incidence from 0.43 % to 2.34%.¹
The use of laparoscopic surgical techniques is ever-increasing to treat intraperitoneal pathology. To perform a laparoscopic intra-abdominal procedure, gas must be insufflated under pressure into the peritoneal cavity to establish a pneumoperitoneum to allow visualization of intra-abdominal contents. Carbon dioxide is the most widely used gas for insufflation due to its noninflammability, good patient tolerance, and high diffusability with subsequent rapid rate of elimination. It is, however, not free of morbidity and is associated with a variety of complications.2,3 The systemic absorption of CO2 gas from the peritoneal cavity can cause hemodynamic decompensation and cardiovascular compromise from hypercarbia and resulting acidosis.4,5 Here we present a case of subcutaneous emphysema with prolonged hypercarbia.
CASE REPORT
A 30 year old female weighing 60 kg, ASA PS 1, diagnosed as primary infertility and multiple uterine fibroids, was posted for laparoscopic myomectomy under general anesthesia. There was no significant medical or surgical history. All preoperative investigations were normal.
In operating room standard monitors (5- lead ECG, blood pressure, pulse oximeter and end tidal CO2 analyzer) were placed. Preoperative vital signs were SpO2 100%, pulse 96/min, BP 120/76 mmHg. Premedication inj. ondensetron 4 mg, inj. glycopyrrolate 0.2 mg, inj. midazolam 1 mg and inj. fentanyl 100 µg was given. The patient was preoxygenated with 100% O2 for 3 min. Induced with inj. propofol 100 mg and short acting muscle relaxant succinylcoline 100 mg was given. She was intubated with endotracheal tube 7.5 mm and was maintained on O2, N2O (50:50), isoflurane (0.6-0.8%) and long acting muscle relaxant inj. vecuronium 5 mg bolus and 1 mg for top ups every half hourly. Inj. diclofenac sodium was given for analgesia.
The trocars (2 of 10 mm, and 4 of 5 mm) were placed by the surgeon. The ventilator was set to deliver tidal volume of 500 ml at a rate of 12 breaths per min. The peak inspiratory pressure was 16 cmH2O; EtCO2 was 30 mmHg and transabdominal pressure was maintained at 14 cmH2O. Due to presence of multiple large size pedunculated and intramural myomas operative time was prolonged. After approximately 5 hours towards the end of surgery with CO2 insufflation pressure of 14 cmH2O, in an attempt to take out suturing needle, one of the port came out and it took 5 attempts to replace it. It followed in 30 min with a SpO2 decrease to 94% and a rise of EtCO2 to a peak of 62 mmHg. The peak inspiratory pressure rose up to 22 cmH2O. On auscultation chest was clear. The ventilator rate was increased steadily to 21 breaths per min in response to the increasing EtCO2. Maximum ventilator settings eventually were as follows: VT 700 ml, respiratory rate 21, peak inspiratory pressure 25 cmH2O, producing minute ventilation (MV) of 14.7 lit/min, the fraction of inspired oxygen (FiO2) was increased to 1.0 from 0.5. Ventilator setting changes reduced EtCO2 to a minimum of 50 mmHg and SpO2 to 97% during the insufflation period.
At this point of time the patient was noted to have facial swelling, palpation revealed skin crepitus extending from operating site into trunk, chest, neck and face (Figure 1).
Figure 1: Massive swelling of the face

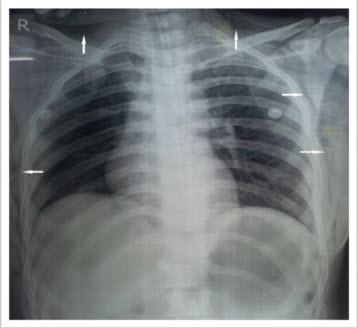
Surgeon was notified of hypercarbia and subcutaneous emphysema and told to hasten the procedure. The arterial blood gas(ABG) measurement was obtained in the operating room; pH 7.299, Po2 111 mmHg, Pco2 60 mmHg, HCO3– 19.8 mmol/lt and SpO2 98% on Fio2 of 1.0. All were consistent with respiratory acidosis. The operation ended in 30 minutes of reaching the peak ETCO2. Patient was shifted to SICU for further observation and monitoring on ventilator on volume control mode. Immediately after shifting to SICU, Chest X ray was taken to rule out pneumothorax and penumomediastinum. CXR showed evidence of massive subcutaneous emphysema but no Pneumothorax or penumomediastinum (Figure 2).
Figure 2: Chest x-ray showing air in subcutaneous tissues (white arrows)
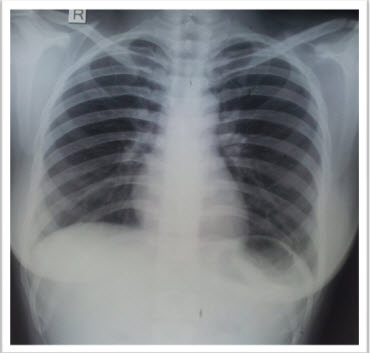
After 6 hours ABG evaluation was done [pH 7.30, PO2 241 mmHg, PCO2 42 mmHg, HCO3– 20mmol/l and SpO2 was 100 % on FiO2 of 0.6.] the patient was electively ventilated for 12 hours. After 12 hours of SICU monitoring ABG evaluation and CXR was done.ABG was showing pH 7.44, PO2 240 mmHg, PCO2 30 mmHg, HCO3 21 mmol/l and SpO2 100% on FiO2 0.6. Subcutaneous emphysema resolved spontaneously. Crepitus had resolved substantially. CXR was normal indicating complete resolution of subcutaneous emphysema (Figure 3).
Figure 3: Chest x-ray showing complete resolution of emphysema
The patient was extubated uneventfully. After 24 hrs of observation patient was shifted to the ward and subsequently discharged after 1 week.
DISCUSSION
Laparoscopic surgery is associated with lower operative morbidity and mortality. Therefore it has been a technique broadly used in the treatment of a variety of intra-abdominal abnormalities that were treated previously with open surgical procedures.¹
There are number of advantages and disadvantages of laparoscopic surgery. The overall recovery time and hospital stay are significantly shorter. Without muscle splinting there is less need for analgesia. All this constitute to lower the cost. However, there is usually a longer operative time compared with an open procedure. The anatomic and physiological changes that occur as a result of pneumoperitoneum with CO2 include the following: reduction in venous return from lower extremities, reduction in cardiac output and index, marked reduction in functional residual capacity, increased peak airway pressure, ventilation perfusion mismatch and increased alveolar/arterial O2 gradient. 6-8 Excess of the CO2 introduced while creating a pneumoperitoneum or pneumoextraperitoneoum must be absorbed from the tissues, across the alveolar membrane and be exhaled into the atmosphere exactly mirroring the body’s physiological process. Without an increase in minute ventilation, hypercarbia will ensue. Maintaining eucarbia may require an increase in minute ventilation by 20 to 30%.
The literature reveals case reports of CO2 diffusing outside the intraperitoneal and extraperitoneal cavities causing subcutaneous emphysema, pneumothorax, pneumomediastinum, pharyngeal emphysema and CO2 embolism.2-4
Hypercarbia contributes to the occurrence of dysrhythmias as a result of enhanced automaticity or an increase in slope of phase 4 depolarisation in the cardiac action potential. A PaCO2 of more than 55 mmHg can result in systolic hypertension, increased central venous pressure, tachycardia and decreased peripheral vascular resistance.1 Persistent hypercarbia will lead to respiratory acidosis. In the unanesthetized patient, compensation takes place in the form of an increase in ventilation, which is mediated by the medullary chemoreceptors, an increase in the plasma concentration of bicarbonate produced by hydration of O2 and renal absorption of bicarbonate into the arterial system. The first two compensatory mechanisms start within seconds of an increase in the serum CO2 level, the renal response requires 48 to 78 hours.6,7
The anesthetized and mechanically ventilated patient has been rendered incapable of the ventilatory response, and if there is not adequate compensation, the serum pH can fall below 7.0 in addition to cardiac dysrrhythmias and significant depression of the central nervous system may also ensue.6,7
An anticipation of hypercarbia requires compensatory ventilator changes. As the EtCO2 increases, other possible causes for this rise should be ruled out. A continued rise in EtCO2 despite the increase in the MV needs to be discussed with the surgeons and temporarily ceasing insufflation until the patients EtCO2 returns to normal limits.8,9
If subcutaneous emphysema is discovered intraoperatively, it should be communicated to the surgeon and extension of the emphysema should be monitored. Possible postoperative problems include prolonged hypercarbia, pharyngeal swelling that may cause airway compromise and facial swelling that may temporarily impair vision. A chest radiograph is done to rule out pneumothorax and/or pneumomediastinum as well as arterial blood gases to evaluate the extent of the hypercarbia.
Another factor that may increase CO2 level is subcutaneous emphysema with increase CO2 absorption. Dissection of the insufflated CO2 from the peritoneal cavity to the subcutaneous tissue may occur at the trocar site or via a defect in the diaphragm. Intra-abdominal CO2 pressure should, therefore, be monitored, since high pressure is associated with higher incidence of subcutaneous emphysema.2,5 Following CO2 absorption into the blood, the gas is stored in visceral and muscle tissue, delaying prompt elimination via the lungs.ᶾ
Our case had multiple risk factors⁵ for the development of subcutaneous emphysema, including maximum end tidal CO2 of 50 mmHg or greater, the use of six or more operative ports and operative time over 200 min. The etiology of subcutaneous emphysema is most likely leakage of insufflated gas into the subcutaneous tissue. An increase in the number of surgical ports also increases the number of points of entry of CO2 gas in subcutaneous tissue.⁵ Subcutaneous emphysema usually develops due to dissection around the trocar site secondary to high insufflation pressure, long surgery duration, at time of port removal and repeated attempts to reinsert the port.
Our patient had hypercarbia and massive subcutaneous emphysema both. There were no signs of pneumothorax or pneumomediastinum, so we immediately informed the surgeon about hypercarbia and massive subcutaneous emphysema and requested to hasten the procedure. Chest x-ray did not show pneumothorax or pneumomediastinum so it was decided not to do any invasive intervention e.g. insertion of subcutaneous catheter or microdrainage with fenestrated catheter and compressive massage etc., and electively ventilate patient till the correction of respiratory acidosis, hypercarbia and resolution of subcutaneous emphysema.10,11
A review of literature shows that pneumothorax and pneumomediastinum may occur due to direct extension of insufflated gas through diaphragmatic rifts into the pleural cavities and develops in 0.03% of patients. The incidence for subcutaneous emphysema during laparoscopy varies from 0.43% to 2.34%.5,9
Length of operative procedure is the most easily identified risk factor for complication related to CO2 insufflation. Long operating time predisposes patients to hypercarbia, subcutaneous emphysema and pneumothorax/pneumomediastinum. The operative time correlates directly with CO2 absorption. Rate of EtCO2 increase appears to be the greatest early in the procedure, but CO2 absorption levels off near the end. Gynecologic surgeons should be aware that patients who have prolonged operative procedures and those with elevated EtCO2, have increased risk of complications. Anesthesiologists must be on look out to identify the risk factors and early intervention.
REFERENCES:
- Worrell JB, Cleary DT. Massive subcutaneous emphysema and hypercarbia: Complications of carbon dioxide absorption during extraperitoneal and intraperitoneal laparoscopic surgery-case studies. AANA J. 2002 Dec;70(6):456-61. [PubMed]
- Kalhan SB, Reancy JA, Collins RL. Pneumomediastinum and subcutaneous emphysema during laparoscopy. Cleve Clin J Med 1990;57: 639-42. [PubMed]
- Karaman S, Akarsu T, Bilgi M, Firat V. Subcutaneous emphysema and hypercarbia during diagnostic laparoscopy. Eng J Med 2005; 44:191-4.
- Bard PA, Chen L. Subcutaneous emphysema associated with laparoscopy. Anaes Analg 1990;71:101-2. [PubMed]
- Murdock EM, Wolff AJ, Van Geem T. Risk factors for hypercarbia, subcutaneous emphysema pneumothorax and pneumomediastinum during laparoscopy. Obstet Gynecol. 2000;95:704-709. [PubMed]
- Wolf JS Jr. Clayman RV. Monk TG, McClennan BL, McDougall EM. Carbon dioxide absorption during laparoscopic pelvic operation. J Am Coll Surg. 1995; 180; 555-560. [PubMed]
- Mullet CE, Viale JP, Sagnard PE, Miellet CC, Ruynat LG, Counioux HC et al. Pulmonary CO2 elimination during surgical procedures using intra- or extraperitoneal CO2 insuffalation. Anesth Analg. 1993; 76:622-626. [PubMed]
- Holzman M, Sharp K, Richards W. Hypercarbia following laparoscopic cholecystectomy. Arch Surg 1991;126,1154-1156 [PubMed]
- Santana A. Crausman RS. Dubin HG. Late onset of subcutaneous emphysema and hypercarbia following laparoscopic cholecystectomy. Chest. 1999; 115:1468-1471. [PubMed]
- Peter o’Reilly,Hua Kiat Chan.Management of extensive subcutaneous emhysema with a subcutaneous drain. Respiratory case reports;1:28-30. [PubMed][Free Full Text]
- Srinivas R, Singh N. Management of extensive subcutaneous emphysema and pneumomediastinum by microdrainage: time for rethink? Singapore Med J 2007;48:e323-6. [PubMed][Free Full Text]
