
To the Editor,
Central venous catheterization (CVC) is routinely being practised in wards and emergency departments for central venous pressure monitoring, administration of ionotropes, hyperosmolar drugs, parenteral nutrition and chemotherapy. Ultrasonographic (USG) guidance and therapeutic beds for achieving Trendelenburg position provide valuable help in vessel access and performing this procedure safely. But at many locations and institutions these facilities may not be available, and use of the blind technique in supine position becomes mandatory. Blind technique is associated with significantly higher complication rate and a lower success rate. On the basis of normal human physiology, we opine that in such situations, the use of Valsalva maneuver (VM) to aid CVC increases the success rate. We illustrate this by two cases, where expected difficult CVC was simplified using VM.
Case 1: A 15 years old male, diagnosed with aplastic anemia, required CVC for antithymocyte globulin administration. He had a cyst on left side of the neck and right sided skin excoriation due to a previously placed CVC in the right internal jugular vein (IJV). A platelet count of 20,000/mm3 in the patient prevented us from trying the blind subclavian approach. IJV cannulation on the right side was not attempted due to previous scar. USG machine and therapeutic bed were not available. After aseptic preparation and local anesthetic infiltration, the patient was asked to perform VM which made the external jugular vein (EJV) prominent. While the patient maintained VM, the EJV was punctured and the guidewire was threaded effortlessly through the EJV. A repeat VM helped guide the CVC over the guidewire.
Case 2: A 48 years old, obese, female patient of enterocutaneous fistula, with short neck required CVC for parenteral nutrition. In the absence of USG, a therapeutic bed and prominent anatomical landmarks, we anticipated difficulty. After aseptic preparation and local anesthetic infiltration, the patient was asked to perform VM. After a test puncture with a pilot needle, the needle for passage of guidewire was inserted into right IJV just lateral to carotid pulsation, followed by successful guide wire placement. The central catheter was then placed following a repeat VM.
IJV cannulation is a common technique for blind external landmark guided CVC, wherein inadvertent carotid artery puncture, nerve injury and airway compromise are frequently encountered complications. Trendelenburg position, hepatic compression, positive intra thoracic pressure and VM1,2 increase the cross sectional area of central veins significantly (>20% ) and reduce their collapsibility in spontaneously breathing patients3 as shown in Figure 1 and 2. Moreover, VM opens the valves in the larger veins (especially EJV) by distending them. Increased diameter of IJV and EJV combined with opening of the venous valves makes needle placement, passage of guidewire and catheter easier,4 thereby reducing the complications. Feasibility of performing VM in both intubated and ventilated patients (passive VM), as well as in spontaneously breathing patients (active VM) allows this technique to be used in a wide range of patients. Clinicians should thus be aware of this simple technique to enhance the success rates of CVC in wards and emergency settings.
References:
1. Lobato EB, Florete OG Jr, Paige GB, Morey TE. Cross sectional area and intravascular pressure of the right internal jugular vein during anesthesia.effect of Trendelenburg position, positive intrathoracic pressure, and hepatic compression. J Clin Anesth 1998; 10:1-5.
[Medline]
2. P. Cowlishaw, P. Ballard. Valsalva Manoeuvre For Central Venous Cannulation Anesthesia 2007;62:640
3. Bellazzini MA, Rankin PM, Gangnon RE, Bjoernsen LP. Ultrasound validation of maneuvers to increased internal jugular vein cross section area and decreased compressibility. Am J Emerg Med. 2009 May;27(4):454-9. doi: 10.1016/j.ajem.2008.03.034.
[Medline]
4. Suzuki T, Takeyama K, Hasegawa J, Nishiyama J, Takiguchi M. Valsalva maneuver prevents guide wire trouble associated with 22-g safe guide. Tokai J Exp Clin Med. 2001;26(3):113-8.
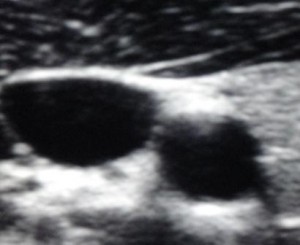
Figure 1: IJV cross section before VM.
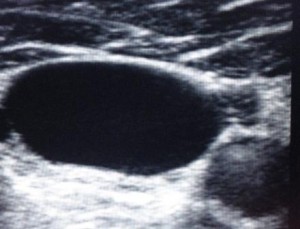
Figure 2: IJV cross section after VM.
Sukhen Samanta, MD* andRudrashish Haldar, MD, PDCC**
*Department of Critical Care Medicine, **Department of Anesthesiology
Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India, 226014
Correspondence: Dr. Rudrashish Haldar, Old PG Hostel, Room No. 2, SGPGI, Lucknow, India, 226014; Email: rudrashish@yahoo.com; Mobile: 08004904625
Citation: Samanta S, Haldar R. Valsalva maneuver aids blind central venous catheterization. Anaesth Pain & Intensive Care 2013;17(1):—
