
Pranav Bansal*, Jagdish Dureja**, Gunjan Chaudhry***
*Associate Professor; **Professor & HoD, ***Assistant Professor
Dept of Anesthesiology & Critical Care, Bhagat Phool Singh Government Medical College for Women, Khanpur Kalan, Sonepat, Haryana (India)
Correspondence: Dr. Pranav Bansal, BPS Govt. Medical College, Khanpur Kalan, Sonepat, Haryana (India); Phone: +91-8607466555; E-mail: drpranav_bansal@yahoo.com
ABSTRACT
Maxillofacial trauma is one of the causes of anticipated difficult airway management and difficult intubation due to distortion of the facial and laryngopharyngeal anatomy. Firecrackers are widely used around the globe in local or national level festivals, and these rarely cause maxillofacial trauma which may lead to difficulties in management of airway. This case report presents a similar case.
Key words: Maxillofacial trauma; Difficult airway management; Difficult intubation
Citation:Bansal P, Dureja J, Chaudhry G. Fire cracker blast in a child’s mouth. Anaesth Pain & Intensive Care 2014;18(2):192-194
INTRODUCTION
Firecrackers are used during various religious or national festivals and ceremonies all over the world, where these form an essential part of the celebrations. Firecracker injuries are also reported during these festivals. A few examples include annual festival of ‘Chaharshanbeh Soori’ in Iran, ‘Tihar’ in Nepal, ‘Hari Raya’ in Malaysia, ‘Guy Fawkes Night’ in United Kingdom, ‘Independence Day’ in USA, ‘Bastille Day’ in France, ‘Diwali’ in India & ‘Shab-e-braat’ in India and Pakistan.1,2
Pediatric population is the commonest target of firecracker injuries due to lack of parental guidance and supervision. It usually leads to burns of skin, damage of myofascial planes and fractures of phalanges in upper extremities.If exploded near the face, firecrackers can cause irreparable damage to facial structures including eyes and/or hearing apparatus apart from varying degrees of burns.2 Fortunately facial trauma is a rare presentation following firecracker injury in pediatric or adult population. Apart from causing functional and aesthetic impact on the growth, facial trauma leads long lasting emotional and psychological effects on the mental development of child.3
Management of severe trauma of facial structures is a real challenge for medical personnel. Distortion of the airway from trauma and coexisting injuries complicates the airway management in pediatric patients. Major concerns about airway management include;
(a) Disrupted anatomy, edema, and blood, damaged tissues and debris in the airway;
(b) Inability to obtain the adequate seal with face mask to facilitate mask ventilation;
(c) Inability to effectively ventilate the lungs;
(d) Difficulty in the visualization of the vocal cords due to blood, secretions, debris, soft tissue, and bone fractures and
(e) The patient being full stomach with risk of aspiration.4 We here present a case report of fire cracker injury during a major festival.
CASE REPORT
A 3 years old baby girl, weighing 10 kg, presented to emergency department with her facial tissues spread apart in ‘cauliflower like’ pattern. The child was watching fire works with neighborhood children without parental supervision, when some of them placed a fire cracker in her mouth in mischief or ignorance, and set it on fire. The sudden explosion led to massive damage of soft tissues of her lower face. There was no history of unconsciousness or ear / nose bleed following the incident. On examination the child was conscious and silent. The right side of her cheek, part of tongue and parts of mouth were torn apart with massive edema, distorting the anatomy beyond identification (Figure 1). The premolars of right upper jaw were damaged while the dentition of lower jaw was preserved. The patient was taken for emergent repair of soft tissues of the face by the maxillofacial surgeon.

Figure 1: Lacerated tissues of the right side of mouth with partially bisected tongue (arrow)
In the operating room intravenous line was secured with a 20G cannula and the monitors attached. Patient was given inj. glycopyrrolate 5 µg/kg and ketamine 1 mg/kg IV. It was planned to perform inhalational induction without use of a muscle relaxant. An appropriate size face mask (No. 1), connected to pediatric circuit, was applied to the face and lacerated tissues were carefully enclosed within the mask (Figure 2). A proper size nasophayngeal airway was passed through left nostril. As a backup plan, an ENT surgeon was stand-by in the operating room to perform tracheostomy if needed.

Figure 2: Enclosure of tissues within the mask with areas of potential air leak
As substantial air leak was present from the side of the mask, a larger mask (No. 2) was instituted to enclose the avulsed tissues. A high flow of oxygen (10 L/min), halothane 3-4% and assisted ventilation was started. When the eyelash reflex was abolished nasal intubation was performed using uncuffed endotracheal tube (ETT) size 4.0 mm. On direct laryngoscopy the laryngeal structures seemed to be preserved because the impact of cracker was limited to oral cavity (Figure 3). Trachea was secured with ETT and pharyngeal packing was done. Anesthesia was maintained with 1-2% halothane in O2 andN2O, and atracurium in intermittent doses. Hydrocortisone and dexamethasone were administered intravenously to reduce upper airway edema and nausea/vomiting . Subsequent anesthetic management was uneventful. After 2 hours of surgery, the approximation of tongue and facial tissues was achieved and a stay suture was passed through the tongue and secured on chin to prevent upper airway obstruction postoperatively, from the swollen tongue. Reversal of anesthesia was achieved with glycopyrrolate +neostigmine in prescribed doses and patient was extubated after adequate recovery. A nasopharyngeal airway was placed to maintain airway patency in the postoperative period. Supplemental oxygen and analgesics were administered that ensured a smooth recovery in the postoperative period. The incident left permanent scars in the mind of the patient, family members and the operating room staff.
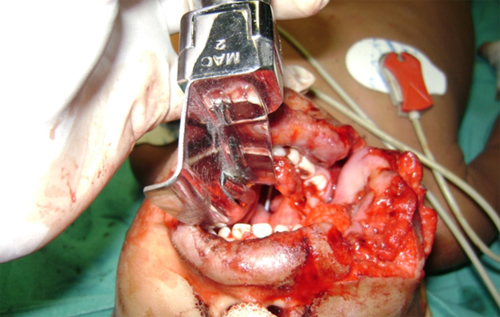
Figure 3: Endotracheal tube visible on direct laryngoscopy
DISCUSSION
The attraction amongst children and youth with fire crackers is because of their sparkle, burst of colors, frightening sounds and noises produced through explosion of flammable materials. On close encounter, fire crackers are no less dangerous or destructive than explosive materials, especially for children. They may turn the traditional festivals into a source of an unwarranted parental anxiety and may result in unforeseen accidents which may permanently handicap exposed children. 2
Lack of knowledge and non-compliance of safety measures is the major reason for fire cracker eventualities. Absence of parental supervision, injury to passersby in streets and unexpected explosion due to fire cracker malfunction may also contribute to fire work injuries.
The anesthetic focus in management of pediatric patients with facial trauma revolves around securing of airway, maintaining hemodynamic status with adequate fluid and blood replacement, pain management and to prevent airway related complications, e.g. edema, spasm, desaturation, etc. in the postoperative period.5
Disrupted airway anatomy, tissue edema, and bleeding following maxillofacial trauma leave few options to secure an intact airway. Airway obstruction can set in at any time once the child is anesthetized. Awake intubation following airway topicalization is the gold standard in such cases in adult patients, though often impossible in pediatric patients. Fiberoptic-guided intubation is impossible to perform in cases of intraoral bleed, while tracheostomy is usually reserved for emergency access to airway or in severe facial injuries.6 We chose a plan of inhalational induction with spontaneous respiration under general anesthesia as the most suitable alternative in this situation.
Postoperatively, airway obstruction is common in these cases due to increasing tissue edema, tongue fall and blood and tissue debris. It is best prevented by placing a nasopharyngeal airway prior to extubation and passing a surgical tie across the tongue to prevent pharyngeal obstruction by back fall of edematous tongue. Airway edema may be decreased by administering warm humidified oxygen and parenteral steroids.6
In our case, the deeper tissues of neck i.e. the pharynx and larynx were spared as the impact of fire cracker spared these tissues, probably due to a low intensity explosion. Moreover, the cracker must have been placed superficially and obliquely in the mouth so that the explosive jet was directed externally towards the cheek. A deeper placement of cracker could have damaged the midline pharyngeal and laryngeal architecture beyond the point of recognition.
Close cooperation between the anesthesiologist and the fasciomaxillary surgeon is essential for optimum results in these cases, as both of them have to work in the same field. Moreover, the anesthesiologist may need frequent airway manipulations even during surgery. The tracheal tube may be secured by stitching to the tissues by the surgeon. Similarly, he or she may well be requested to pass a stitch through the tongue pulling it out to secure open airway passage postoperatively.
In most of the countries of Southeast Asia, there are no regulations/legislations for preventing or regulating the use of fireworks by public.7 Publication of such multi-centre studies, case series or reports by medical fraternity can increase the awareness amongst our government bodies, which may then formulate strict guidelines for the prevention of fire cracker injuries amongst civilians in future.
Financial Support: Self
Conflict of Interest: Nil
REFERENCES
- Hatamabadi HR, Tabatabaey A, Heidari K, Khoramian MK. Firecracker Injuries During Chaharshanbeh Soori Festival In Iran: a Case Series Study. Arch Trauma Res 2013;2:46-9. [PubMed][Free Full Text]
- Upadhyaya DN, Khanna V. Diwali burns: An overview. Indian Journal of Burns 2012;20:46-7. [Free Full Text]
- Mukherjee CG, Mukherjee U. Maxillofacial trauma in children. Indian J of Clinical Pediatric Dentistry 2012;5:231-6. [Free Full Text]
- Krishna HM, Kundu R. Adult face mask for inhalational induction in a child with maxillofacial injury. Anesth Essays Res 2012;6:215-7. [Free Full Text]
- Ivashkov Y, Bhananker SM. Perioperative management of pediatric trauma patients. Int J Crit Illn Inj Sci 2012;2:143-8. [PubMed][Free Full Text]
- Rao BK, Singh VK, Ray S, Mehra M. Airway management in trauma. Indian J of Critical Care Med 2004;8:98-105. [Free Full Text]
- Tandon R, Agrawal K, Narayan R P, Tiwari V K, Prakash V, Kumar S, Sharma S. Firecracker injuries during Diwali festival: The epidemiology and impact of legislation in Delhi. Indian J Plast Surg 2012;45:97-101. [PubMed][Free Full Text]
