
Yasunari Matsuki, MD*, Yuka Matsuki, MD**, Yoshikazu Yasuda, MD*, Maki Mizogami, MD**, Ko Takakura, MD**, Kenji Shigemi, MD**
*Department of Intensive Care Unit, **Department of Anesthesiology & Reanimatology,
University of Fukui, Faculty of Medicine Sciences, Fukui (Japan)
Correspondence: Yasunari Matsuki, MD, Department of Intensive Care Unit, University of Fukui, Faculty of Medicine Sciences, 23-3 Shimoaizuki, Matsuoka, Eiheijicho, Yoshidagun, Fukui 910-1193 (Japan); Tel: +81-776-61-8391; Fax: +81-776-61-8116; E-mail: tainobu@u-fukui.ac.jp
ABSTRACT
Legionella pneumonia is often complicated by multiple organ failure. Although acute kidney injury is relatively rare in the context of Legionella pneumonia, it is associated with an increase in mortality rate. This report describes a case of a patient with Legionella pneumonia and acute kidney injury who was successfully treated with polymyxin B-immobilized fiber column direct hemoperfusion (PMX-DHP). We conclude that PMX-DHP may be a useful therapeutic modality in patients with Legionella infection and acute kidney injury.
Key words: Legionella pneumonia; Polymyxin B-immobilized fiber column direct hemoperfusion; Acute kidney injury
Citation: Matsuki Y, Matsuki Y, Yasuda Y, Mizogami M, Takakura K, Shigemi K. Successful treatment of severe Legionella pneumonia and acute kidney injury with polymyxin B-immobilized fiber column direct hemoperfusion. Anaesth Pain & Intensive Care 2013;17(1):88-90
INTRODUCTION
Legionella pneumonia was first described following an outbreak of pneumonia among army veterans attending an American Legion convention in Philadelphia in 1976.1 This pneumonia is often complicated by multiple organ failure, including acute kidney injury and hepatic dysfunction, that is associated with an increase in mortality rate.2-3 Polymyxin B-immobilized fiber column direct hemoperfusion (PMX-DHP) is a useful treatment modality for patients with organ dysfunction due to severe sepsis.4 We describe a case of a patient with severe Legionella pneumonia and acute kidney injury who was successfully treated with PMX-DHP.
CASE REPORT
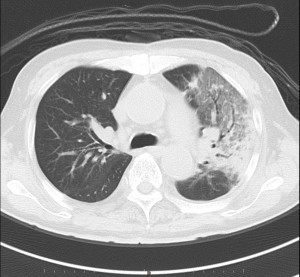
A 70 years old man was admitted to our hospital with diarrhea, high-grade fever and dyspnea. He had been on treatment for malignant lymphoma, and had mitral valvuloplasty in the past. Physical examination on admission to our hospital revealed a temperature of 38.8°C, blood pressure of 65/40mmHg, heart rate of 89/min, SpO2 of 80% (on 15 L/min of O2 via reservoir mask) and a respiratory rate of 35/min. Glasgow coma scale was 9/15. Fine crackles were audible in the upper lung fields bilaterally. Laboratory tests showed elevations in leukocytes and C-reactive protein at 13,100/μl and 35.20mg/100 ml respectively. BUN (28 mg/100 ml), Creatinine (1.64 mg/100 ml), AST (1019iu/L), ALT (677iu/L) and LDH (1756iu/L) were also elevated, and the Na level (127 mEq/L) was low. Arterial blood gas analysis (taken while O2 was being administered at 15 L/min via reservoir mask) showed severe hypoxemia, and metabolic acidosis (pH of 7.06, PaCO2 of 54 mmHg, PaO2 of 52 mmHg, HCO3– of 14.5 mmol/L). Chest x-ray film showed infiltrative shadows in the left upper lung fields, and a chest CT revealed consolidation and ground-glass opacity in the left upper lung field (Fig 1-A&B).
Fig 1-A: Chest radiograph on admission. There is an infiltrative shadow in the left upper lung field.
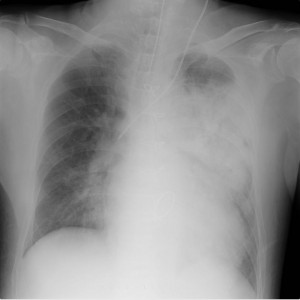
Fig 1-B: Chest computed tomography on admission showing consolidation with ground-glass opacities in the left lung field
The patient’s clinical course is summarized in Fig 2. He was admitted to the intensive care unit (ICU) with a blood pressure of 78/42 mmHg despite administration of 5 μg/kg/min of dopamine hydrochloride and 0.1 μg/kg/min of noradrenaline. He was immediately intubated and ventilated with 100% oxygen and was treated with sivelestat sodium hydrate, intravenous fluids of volume and antibiotics (tazobactam/piperacillin, pazufloxacin). A diagnosis of legionellosis was made on the basis of positive specific urinary antigen. Antibiotics were switched to erythromycin, but blood pressure and the PaO2/FiO2 (P/F) ratio continued to decrease. He became anuric, and continuous hemodiafiltration (CHDF) (CH-1.0®; Toray Medical Co., Tokyo, Japan) was started to maintain body water balance. In addition, PMX-DHP (Toraymyxin 20R®; Toray Medical Co., Tokyo, Japan) was performed for 4 hours on days 1 and 2 to adsorb endotoxin. After the introduction of PMX-DHP, blood pressure and urinary output were gradually increased, and catecholamines were tapered off. The P/F ratio improved from 173 to 386 on day 3, and CHDF was terminated on day 8. The patient was extubated on day 9 after careful weaning from mechanical ventilation.
Fig 2: Clinical course after initiation of PMX-DHP. Catecholamines (noradrenaline and dopamine) were tapered off, and blood pressure and the PaO2/FiO2 (P/F) ratio gradually improved.
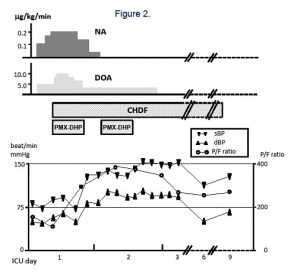
(Legend: NA: noradrenaline, DOA: dopamine, CHDF: continuous hemodiafiltration, PMX-DHP: polymyxin B-immobilized fiber column direct hemoperfusion, sBP: systolic blood pressure, dBP: diastolic blood pressure)
DISCUSSION
The bacterium, Legionella, got its name after a 1976 outbreak, when many people who went to a Philadelphia convention of the American Legion suffered from this disease, a type of pneumonia (lung infection). Although this type of bacterium was around before 1976, more illness from Legionnaires’ disease is being detected now. The report describes the case of a patient with Legionella pneumonia and acute kidney injury who was successfully treated with PMX-DHP. Legionella pneumophila is one of the three most common causes of severe community-acquired acute pneumonia and comprises 3-6% of all cases of community-acquired pneumonias.5,6 Although radiologic and clinical findings alone are not sufficient to establish a diagnosis of Legionella pneumonia, if these are accompanied by diarrhea, neurological signs, a temperature >39°C, hyponatremia and hepatic dysfunction, these are strongly suggestive of legionellosis.7-9 Diarrhea, hyponatremia and hepatic dysfunction were noted in our present case. The patient was ultimately diagnosed with legionellosis on the basis of positive specific urinary antigen.
Although Legionella pneumonia complicated by acute kidney injury is a rare disease, it is associated with a mortality rate greater than 50%.2,3 In our case, rhabdomyolysis was not observed, and we speculated that direct microbial toxicity,10 endotoxemia, inflammatory cytokines11 and/or hypotension was the cause of acute kidney injury. L. pneumophila is a Gram-negative aerobic bacterium that is an intracellular parasite, and produces beta-lactamase and many other potential endotoxins.
PMX-DHP can lower the plasma level of endotoxin and inflammatory cytokines,12,13 and can significantly improve hemodynamics and organ function in patients with severe sepsis and/or septic shock arising from Gram-negative bacterial infections.4,14 In the present case, early use of PMX-DHP resulted in improved hemodynamics and kidney function. PMX-DHP exerts a therapeutic effect in patients with pneumonia by absorbing cytokines (e.g. IL-8) and neutrophil elastase produced by activated neutrophils PMX-DHP,15,16 and this was the likely mechanism of therapeutic action in our patient.
CONCLUSION
We conclude that PMX-DHP may be a useful therapeutic modality in patients with Legionella infection and acute kidney injury.
REFERENCES
- Fraser DW, Tsai TR, Orenstein W, Parkin WE, Beecham HJ, Sharrar RG, et al. Legionnaires’ disease. Description of an epidemic of pneumonia. N Engl J Med. 1977;297(22):1189-97. [PubMed]
- Harvey M, Quirke P, Warren D. Acute renal failure complicating Legionnaires’ disease. Postgrad Med J. 1980 Sep;56(659):672-4. [PubMed] [Free full article]
- Lin SL, Chen HS, Yu CJ, Yen TS. Legionnaires’ disease with acute renal failure: report of two cases. J Formos Med Assoc. 1995 Mar;94(3):123-6. [PubMed]
- Cruz DN, Antonelli M, Fumagalli R, Foltran F, Brienza N, Donati A, et al. Early use of polymyxin B hemoperfusion in abdominal septic shock: the EUPHAS randomized controlled trial. JAMA. 2009 Jun 17;301(23):2445-52. doi: 10.1001/jama.2009.856. [PubMed] [Free full article]
- Mundy LM, Auwaerter PG, Oldach D, Warner ML, Burton A, Vance E, et al. Community-acquired pneumonia: impact of immune status. Am J Respir Crit Care Med. 1995 Oct;152(4 Pt 1):1309-15. [PubMed]
- Marston BJ, Plouffe JF, File TM Jr, Hackman BA, Salstrom SJ, Lipman HB, et al. Incidence of community-acquired pneumonia requiring hospitalization. Results of a population-based active surveillance Study in Ohio. The Community-Based Pneumonia Incidence Study Group. Arch Intern Med. 1997 Aug 11-25;157(15):1709-18. [PubMed]
- Stout JE, Yu VL. Legionellosis. N Engl J Med. 1997 Sep 4;337(10):682-7. [PubMed]
- Katz DS, Leung AN. Radiology of pneumonia. Clin Chest Med. 1999 Sep;20(3):549-62. [PubMed]
- Mulazimoglu L, Yu VL. Can Legionnaires disease be diagnosed by clinical criteria? A critical review. Chest. 2001 Oct;120(4):1049-53. [PubMed]
- Wong KH, Moss CW, Hochstein DH, Arko RJ, Schalla WO. “Endotoxicity” of the Legionnaires’ disease bacterium. Ann Intern Med 1979; 90: 624-627. [PubMed]
- Remick DG, Kunkel SL. Toxic effects of cytokines in vivo. Lab Invest. 1989 Mar;60(3):317-9. [PubMed]
- Kushi H, Miki T, Okamaoto K, Nakahara J, Saito T, Tanjoh K. Early hemoperfusion with an immobilized polymyxin B fiber column eliminates humoral mediators and improves pulmonary oxygenation. Crit Care 2005; 9: 653-661. [PubMed] [Free full article]
- Seo Y, Abe S, Kurahara M, Okada D, Saito Y, Usuki J, et al. Beneficial effect of polymyxin B-immobilized fiber column (PMX) hemoperfusion treatment on acute exacerbation of idiopathic pulmonary fibrosis. Intern Med. 2006;45(18):1033-8. Epub 2006 Oct 16. [PubMed] [Free full article]
- Cruz DN, Antonelli M, Fumagalli R, Foltran F, Brienza N, Donati A, et al. Early use of polymyxin B hemoperfusion in abdominal septic shock: the EUPHAS randomized controlled trial. JAMA. 2009 ;301:2445-2452. [PubMed] [Free full article]
- Abe S, Seo Y, Hayashi H. Neutrophil adsorption by polymyxin B-immobilized fiber column(PMX) for acute exacerbation in patients with interstitial pneumonia: a pilot study. Blood Purif. 2010;29(4):321-6. doi: 10.1159/000287232. Epub 2010 Feb 24. [PubMed] [Free full article]
- Kawagishi N, Ohkohchi N, Fujimori K, Orii T, Koyamada N, Kikuchi H, Satomi S. The effect of continuous veno-venous hemofiltration or direct hemoperfusion with polymyxin B-immobilized fiber on neutrophil respiratory oxidative burst in patients with sepsis and septic shock. Ther Apher. 2001 Feb;5(1):7-11. [PubMed]
