
Misbah Durrani, MCPS, FCPS*, Mahjabeen Mahmood Kamal, MCPS, FCPS**, Naeem Ahmed, MBBS***, Mobeen Jawad, MCPS, FCPS, FRCR****
*Senior Registrar in Radiology, **Assistant Prof. and Head of Department (Radiology),
Rawalpindi Medical College/DHQ Hospital, Rawalpindi (Pakistan).
***PG. Paediatrics. Holy Family Hospital RWP
****Consultant Radiologist, CMH Rawalpindi
Correspondence: Dr. Mahjabeen Mahmood Kamal, Assistant Professor of Radiology, Rawalpindi Medical College/D.H.Q. Hospital Rawalpindi (Pakistan); E-mail: mahjabeenmahmood@hotmail.com
ABSTRACT
A case of battered baby syndrome of an 11 month old first born baby is reported, which was found to be due to a psychological condition of the mother called acute postpartum depressive psychosis. The child was brought to the emergency with history of fall from the bed. Skull fractures were detected on CT scan but no brain injury. Later on the same baby was brought to the pediatric department with history of fits. CT scan was repeated and based on the CT findings and history the injuries were found out to be due to repeated shaking and beating by the mother.
Key Words: Battered baby syndrome; Computed tomography (CT scan); Skull fractures; Cerebral hemorrhage.
Citation: Durrani M, Kamal MM, Ahmed N, Jawad M. Battered Baby Syndrome: A Case Report. Anaesth Pain & Intensive Care 2009;13(2): 71-74
INTRODUCTION
The term ‘battered baby syndrome’ is defined as a clinical condition, usually in children under 3 years of age, who have suffered non-accidental injury, on one or more occasions, by an adult in the position of trust usually a parent, a guardian or a foster parent1. In addition to the physical injury, there may be deprivation of nutrition, care and affection in circumstances which indicate that such deprivation is not accidental. It is very common to find the discrepancy between the history and clinical findings.1
We received such a case, who reported to us for a repeat CT scan of brain. Initially the condition went unrecognized and on second time the child was found to have severe cerebral damage. Her mother was later diagnosed to have suffered from acute postpartum depressive psychosis after her first delivery.
CASE REPORT
An 11 months old male baby, first born of orphaned young parents, belonging to the low socioeconomic class was brought to the emergency department of DHQ Hospital Rawalpindi, with a history of fall from the bed. An emergency CT scan was done which showed right parietal bone fracture. However, the underlying brain tissue was found normal as shown in Fig. 1 and Fig. 2. Patient was discharged after conservative treatment.
Fig.1. Normal brain tissue .
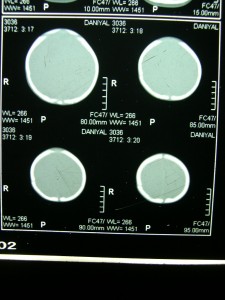
Fig.2. Right parietal bone fracture.
Few days later, the child was brought to the pediatric department of Holy Family Hospital, Rawalpindi, with a history of fits. A repeat CT scan was ordered and the patient was referred to our department (Radiology Department of DHQ hospital Rawalpindi) for the same. On general physical examination of the patient, he was a well fed and properly dressed baby boy. He had an apparently large head with a measured head circumference of 28 cm and an evidence of frontal bossing. He couldn’t hold his head. There was also evidence of bilateral nystagmus.
CT showed the previous skull fracture as well as new fractures involving right parietal and occipital bones. There were cortical parenchymal calcifications in the parietal and occipital lobes bilaterally. Bilateral subdural hygromas and cerebral atrophy was also seen. (Fig. 3 and 4).
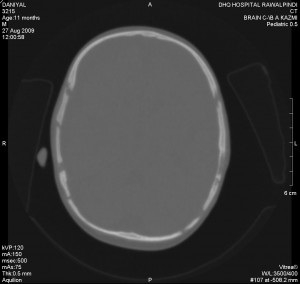 Fig. 3: Multiple skull fractures.
Fig. 3: Multiple skull fractures.
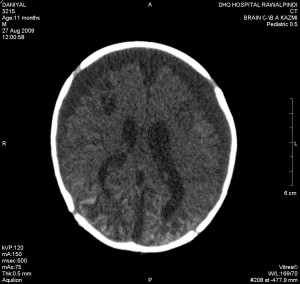
Fig. 4: Bilateral cortical calcification and subdural hygromas.
3D reconstruction images of the skull, show fractures in Fig 5 and 6.
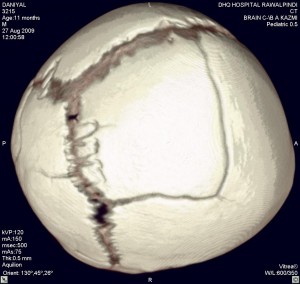
Fig. 5

Fig. 6
No clinical history or radiological evidence of cerebral infection was seen. A contrast enhanced scan was also done, which ruled out abnormal meningeal enhancement. Based on the CT findings and previous history of trauma a suspicion of battered baby syndrome was made. A skeletal survey of the baby, however, did not reveal any other injuries to the bones. A detailed history was taken from the mother and father. The mother got married at the age of only 14 and conceived 2 months later. Her pregnancy went unremarkable and baby was delivered at home with the help of a local ‘Dayi’ (midwife). According to her, she was looking after the baby normally when she conceived again just three months after her first delivery. She started having episodes of depression and became quite irritable. She started beating up the baby, often violently shaking him. These episodes of depression and beatings continued till the second baby boy was born. When the couple came to our department, the mother was carrying her 7 days old baby in her arms.
The patient was sent back to the paediatric department with the diagnosis of battered baby syndrome. After a few days, the patient was again sent to our department for another CT scan as his head circumference was progressively increasing. It was 33 cm at that time. A suspicion of hydrocephalus had been raised and placing a VP shunt was being considered. The CT, however, showed no evidence of hydrocephalus, but significant encephalomalacia was noted (Fig 7).
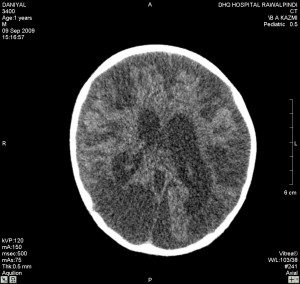
Fig.7. Extensive encephalomalacia.
Baby was managed conservatively and was later discharged. Mother was referred to the Psychiatry Department for psychiatric evaluation, where she was diagnosed as suffering from acute postpartum depressive psychosis. She was admitted for management.
DISCUSSION
In the west, battered bay syndrome is the most common cause of serious injuries in children aged less than 1 year. It is the third most common cause of death in children after sudden infant death syndrome and true accidents. In the United States 1.7 million cases were reported in 1990.2Kempe and his co-workers introduced this term in 1962 to characterize a clinical condition in children, usually younger than 3 years of age, who suffered from serious physical abuse. According to him, this syndrome should be considered in any child exhibiting evidence of fracture of a bone, subdural haematoma, failure to thrive, soft tissue swelling or skin bruises, in any child who dies suddenly, or when the degree and type of injury is at variance with history given3.
In eastern culture, babies are considered as a gift from God and cases of battered baby syndrome are rare. However, instances of ill treatment of young children working as domestic servants are on record, where employers have beaten some children with sticks or burned them with a pair of hot tongs. The crime comes to light only when such children complain to someone who knows their mother tongue4.
Battered baby syndrome should be suspected in all children younger than one year of age, who present with drowsiness, coma, seizures or apnea. A combination of subdural hematomas, retinal haemorrhages with minimal or no trauma and no coagulopathy are pathognomonic of this syndrome. The injuries are caused by shaking with or without impact. Physical signs of violence are often absent and this syndrome may be mistaken for a serious infection or seizure disorder5.
In this syndrome, along with occasional beating, the baby is also held by the thorax and shaken violently. This causes a repetitive acceleration and deceleration trauma which leads to typical intracranial bleeding, eye injuries, skull fractures and rib fractures. Many cases are fatal and lead to seizures and neurological disability including blindness. Cerebral palsy, mental retardation or epilepsy may occur in about 60% of the children.5These intracranial haemorrhages are thought to be caused by the easily torn bridging veins of infant’s head. The infant’s head and blood vessels are particularly vulnerable to vigorous shaking because of the relatively large head and weak neck muscles, the abundance of unmyelinated brain tissue, which permits excessive stretching of the brain and vessels, and the increased pliability of the skull as compared to the rigidly fixed internal structures such as falx cerebri.6
In an infant, anything but a non-widely spaced simple linear fracture of the parietal bone should be viewed with suspicion and regarded as a non-accidental injury until proven otherwise. Such fractures include depressed, stellate, comminuted and other complex fractures7. In children under 2 years of age, a skeletal survey may be done to find other fractures. Skeletal trauma can be seen in 50-80% of cases.2
Ophthalmic examination of children with suspected battered baby syndrome is important for the prognostic as well as diagnostic purposes. Diffuse bleed seen on the optic fundus, vitreous hemorrhage or sub-hyloid haemorrhage are usually associated with worse visual outcome8. Non-reactive pupils and midline shift of the brain structures correlate highly with mortality and more severe neurologic injury. Of the survivors, up to 60% may have neurological sequelae which include seizures, cerebral palsy and blindness.5
Visceral injuries, secondary to abdominal trauma (punch, kick) can be the second leading cause of death in child abuse, usually seen in children more than 2 years of age. Intestinal injuries are the most commonly reported intra-abdominal lesions in battered children. Intramural haemotoma of the duodenum or jejunum is well documented.2
There is a spectrum of the consequences of battered baby syndrome and less severe cases may not be brought to the attention of medical professionals. A victim of sub-lethal shaking or beating may have a history of poor feeding, vomiting, lethargy and/or irritability occurring for days or week. Signs of battered baby syndrome may vary from mild and nonspecific to severe and immediately identifiable clinically. In the most severe cases, which usually result in death or severe neurologic consequences, the child usually becomes immediately unconscious and suffers rapidly escalating life threatening CNS dysfunction.5
A recent WHO estimate shows that 40 million children in the world aged 0-14 years are abused and neglected. These children require both health care and social care.9 The awareness regarding these aspects has recently raised concern among health professionals and enlightened citizens, specially in the advanced countries, where the problem has been reported to have increased to ten folds in the last decade.10 In third world countries with poorer societies, continuous socioeconomic stress induces the parents to abuse their children.11 It is however, imperative that any case, before being labeled as battered baby syndrome, should be thoroughly investigated and all possibilities of accidental injuries should be ruled out.
The role of radiological examination is undeniable in detection of skeletal injuries in these children and must be sought in conjunction with a thorough history to rule out other disease conditions.
REFERENCES
1. Cameron JM. The battered baby syndrome. Practitioner 1972;209:302-309.
2 . Dahnert W. Radiology Review Manual. 6th Edition. Wolters Kluwer Publishers and Distributors; 2007. P52.
3. Kempe CH. Paediatric implications of the battered baby syndrome. Archives of Disease in Childhood.1971;46:28.
4. Parikh CK. Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology. 6th Edition. New Delhi: CBS publishers and Distributers. 2005.p4.188.
5. AmericanAcademy of Paediatrics. Committee on Child Abuse and Neglect, Shaken baby syndrome. Paediatrics.2001;108:206-210.
6. Tobias JD, Rasmussen GE, Yaster M. Multiple trauma in the paediatric patient. In: Mark RC, Ed. Textbook of Paediatric Intensive Care, 3rd edition. Maryland and Williams, 1996:1498.
7. Hobbs CJ. Skull fractures and diagnosis of abuse. Arch Dis Child. 1984;59(3):246-52.
8. Nelson L. Disorders of the eye. In: Behrmen ER,Kliegman RM, Arvin AN Eds. Bangalore, Prism Books Pvt. Ltd 1996;1795.
9. Sharma BR. Medico-legal aspects of child abuse. Physician’s Digest, 2005;14(1):41-48.
10. Chadwick DL, Child abuse In: Textbook of Paediatrics.9thEd. Eds Rudolph AM, Hoffman JLE, Connecticut, Appleton Lange, NortWalk;1991.760-769.
11. Banarjee SR, MehtaMN, Narayan. Child Abuse, Neglect and Child labour. In: IAP Textbook of Paediatrics. 1st Ed. New Delhi: Jaypee Brothers 1999;704-705.
