
Thorat Pravin Shivajirao, MBBS, DA, DNB*, Nageshkumar P Wasmatkar, MBBS**, Pratibha Govindrao Gore, MBBS***, J. N. Lakhe, MBBS, B.Sc., MD****, Shidhaye Ramchandra Vinayak, MD, DA*****
*Assistant Professor; **Postgraduate Resident; **** Associate Professor; *****Professor
Department of Anesthesiology and Critical Care
Rural Medical College, Pravara Institute of Medical Sciences, Loni 413736 (India)
***Postgraduate Resident
Department of Oral Pathology and Microbiology
Rural Dental College, Pravara Institute of Medical Sciences, Loni 413736 (India)
Correspondence: Dr. R. V. Shidhaye, Shraddha Clinic, Babhaleshwar, Tal. Rahata, Distt. Ahmednagar- 413737 (India); Phone: 02422 253459; Cell: 091 9822034601; E-mail: rvshidhaye@yahoo.com
ABSTRACT
Anesthetic challenges in Morquio syndrome include the respiratory problems due to restrictive defect in the thoracic cage, upper airway obstruction during head flexion, atlantoaxial instability and compression of the cervical spinal cord due to hypoplasia of the dens, complicating intubation. After pre-anesthetic check up and informed written consent, the patient was premedicated with glycopyrrolate 0.08 mg and fentanyl 10 mcg. Induction was done with inhalational anesthetic agent sevoflurane along with Oxygen (O2) and Nitrous oxide (N2O) maintaining the spontaneous respiration. Intubation was done with Flexo metallic tube (FMT) no. 24 through right nostril avoiding forceful movements at atlantoaxial joint and cervical spine. Maintenance and recovery was uneventful. Paramount in the anaesthetic care of such patients is a thorough preoperative evaluation of airway in addition to cardiac, respiratory, neurological function. Inhalational induction technique may be useful in difficult intubation.
Key words: Morquio syndrome; Inhalation induction; Difficult intubation.
Citation: Shivajirao TP, Wasmatkar NP, Gore PG, Lakhe JN, Vinayak SR. Anesthetic considerations in Morquio syndrome: A case report. Anaesth Pain & Intensive Care 2013;17(1):75-78
INTRODUCTION
Mucopolysaccharidoses are a heterogeneous group of metabolic disorders usually inherited in autosomal recessive fashion, characterized by a lack of glycosaminoglycans. Mucopolysaccharidosis type IV is an autosomal recessive disorder caused by deficiency of n- acetylgalactosamine-6-sulphate and is also called as Morquio syndrome.1 It is characterized by a defect in the degradation of keratan sulfate resulting in the accumulation of mucopolysaccharides. The disorder results in short stature, spinal deformity, odontoid hypoplasia, macroglossia, corneal opacities, short neck, pectus carinatum, kyphoscoliosis, dwarfism, cardiac abnormalities, hepatomegaly, acoustic deafness, and dental abnormalities.2 Atlantoaxial subluxation and cervical myelopathy are usual clinical findings. Anaesthetic challenges in such cases include the respiratory problems due to, restrictive defect in the thoracic cage, upper airway obstruction during head flexion, atlantoaxial instability and compression of the cervical spinal cord due to hypoplasia of the dens; complicating intubation procedures.
CASE REPORT
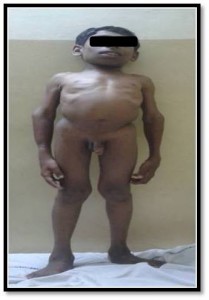
A male patient, 17 years, weighing 18 kg, presented to the pedodontics department with dental caries for full mouth rehabilitation. He was born of consanguineous marriage with full term normal vaginal delivery with birth weight of 1.75 kg and history of birth asphyxia. He had delayed speech and had been very hyperactive. Clinical examination revealed a short stature, microcephaly, short neck, cervical scoliosis, slanting forehead, barrel chest deformity, dorsolumbar kyphosis, increased anteroposterior diameter of chest, pectus excarinatum, waddling gait, pot belly, valgus deformity of both upper and lower limbs and hoarse voice (Figures 1 and 2).
Figure 1: Side view of the child

Figure 2: Front view of the child
Oral cavity examination revealed bulky soft tissue, large tongue, caries teeth, poor oral hygiene, large uvula and restricted neck anteroposterior movements, Mallampati grade– II. Systemic examination showed normal cardiovascular and respiratory systems. Liver was palpable by 1½ cm below right costal margin. Preoperative investigations, including hemogram, urine examination, liver function tests, renal function tests and echocardiography were within normal limits. X-ray neck and cervical spine AP view( Figure 3) showed ‘thickening of calvarium, hypoplasia of odontoid process of C2 vertebra, atlanto-occipital subluxation (lateral atlanto-dental distance: on left side-2.6mm and on right side- 1.25mm; Predental distance: anteriorly-2.58mm and posteriorly-4.30mm). Chest x-ray PA view and lateral view with skull (Figures 3 and 4) showed ‘mild flaring and widening of ribs, platyspondyly ( flattening of vertebral bodies) and anterior beaking of all vertebrae, short thick clavicles, pectus carinatum (increase in AP distance of thoracic cage), focal narrowing of airway seen at the level of hypopharynx just posterior to epiglottis measuring 5mm at this level, 10mm above it and 15mm below it in AP diameter and hypoplastic maxilla with prominent mandible.
Figure 3: Chest x-ray PA view

Figure 4: Lateral view of the skull and cervical spine

Lumbosacral spine x-rays on AP and lateral views (Figures 5 and 6) showed ‘ not clearly visualized femoral capital epiphyses (progressive disappearance is characteristic), flaring of iliac wings, increased obliquity of acetabular roof, interpeduncular distance increasing caudally in lumbosacral spine.
Figure 5: Lumbosacral spine lateral view showing poorly visualized femoral capital epiphyses, increased interpeduncular distance, flattening of the vertebral bodies anteriorly

Figure 6: Lumbosacral spine AP view

Wrist joint AP view (Figure 7) showed mild widening of metacarpals and slanting distal articular surfaces of radius and ulna. Constellations of all these radiological findings favored the clinical suspicion of mucopolysaccharidosis and possibility of difficult intubation.
Figure 7: Wrist joints AP view showed mild widening of metacarpals and slanting distal articular surfaces of radius and ulna

Anaesthetic management: General anaesthesia was planned with sevoflurane in oxygen and nitrous oxide. Glycopyrrolate was given, but no heavy sedation, as premedication. Considering the anticipated difficult intubation inhalational induction with spontaneous respiration was planned. Due to a possibility of atlantoaxial subluxation and cervical myelopathy intubation was planned with neck stabilization. Nasal intubation was planned with a flexometallic tube, as the dental surgeon had to share airway and oral cavity. Use of flexible bronchoscope for intubation was the good option but it was not available. Extubation was planned to be done when patient was full conscious and awake, considering the possibility of respiratory depression and difficult intubation if reintubation was required. Postoperatively intensive monitoring for airway patency and adequacy of respiration and hemodynamic stability was planned.
After pre anaesthetic check up and informed written consent, patient was premedicated with glycopyrrolate 0.08 mg and fentanyl 10 mcg. Induction was done with inhalational anaesthetic agent sevoflurane in oxygen and nitrous oxide. Sevoflurane was increased in incremental doses from 2% to 8%. After achieving adequate depth of anaesthesia with sevoflurane patient was intubated with flexometallic endotracheal tube No. 24 through right nostril, avoiding forceful movements at atlantoaxial joint and cervical spine and maintaining spontaneous respiration. Patient was maintained on sevoflurane in oxygen and nitrous oxide. Analgesia was provided with incremental doses of inj. fentanyl. Monitoring included heart rate, electrocardiogram, non invasive blood pressure, oxygen saturation (SpO2) and endtidal carbon dioxide. After completion of the surgical procedure the patient was extubated when fully awake and with all airway reflexes recovered. Patient was shifted to recovery room where he was monitored for the vital parameters. Recovery was uneventful and patient was shifted to pediatric ward after gaining full consciousness.
DISCUSSION
Morquio syndrome also known as mucopolysaccharidosis type IV is an autosomal recessive disorder caused by deficiency of n-acetylgalactosamine-6-sulphate. Morquio in Uruguay and Brailsford in England simultaneously described this syndrome in 1929.1 The incidence is unknown but is estimated to be between 1 in 75 000 population in Northern Ireland to 1 in 200 000 population in British Columbia.3,4 Morquio syndrome is characterised by a defect in the degradation of keratin sulphate resulting in the accumulation of mucopolysaccharides. At birth, a patient with Morquio syndrome may appear healthy; however, as the child grows into adulthood, various manifestations of this syndrome begin to emerge.The airway issues in these patients are frequently complicated by cervical spine instability and the risk of subluxation.5 Respiratory function can be compromised by chronic respiratory disease, recurrent pulmonary infections, obstructive sleep apnea and kyphoscoliosis leading to restrictive lung disease. The most important problems concerning the airway management are based on intracellular accumulation of mucopolysaccharides resulting in macroglossia, limited mouth opening due to involvement of temporo-mandibular joints and short neck. The trachea is often narrow and flattened.6 The unique anatomy and extremely sensitive airway may result in failed intubation and bronchospasm even after successful intubation.7 These elements may lead to ‘cannot intubate, cannot ventilate’ situation. Cardiac involvement is usual. Valve involvement may cause incompetent or stenotic lesions especially of the aortic valve,8,9 whilst myocardial deposits cause reduced compliance.8 Systemic and pulmonary hypertension may occur and death is often due to cardiac or respiratory failure.10 In our patient, we noticed coarse facial features like frontal slanting, narrowed nasal opening, macroglossia, reduced oropharyngeal space, dental caries, restricted neck movements and the skeletal abnormalities like kyphoscoliosis contributing to difficult ventilation and intubation. Cardiac abnormalities, e.g. aortic regurgitation and other valvular lesions, were not present in our case. Premedicants are best avoided because of dangers of upper airway obstruction, respiratory depression, hypercarbia and cardiorespiratory arrest. An antisialogogue is an essential component of preanaesthetic medication in view of the copious upper airway secretions, and antibiotic prophylaxis is advised in view of the high incidence of cardiac valvular lesions.11 We used glycopyrrolate as an antisialogogue and avoided sedative agents. We gave titrated doses of fentanyl under strict respiratory monitoring. An inhalational induction with sevoflurane provides a controlled situation with maintenance of spontaneous ventilation until laryngoscopy is performed. Depth of anaesthesia can be titrated by adjusting concentration of inhalational agent. The main advantage of using inhalational induction is that it keeps the returning doors open in ‘cannot intubate, cannot ventilate’ situation. We took care of the cervical spine by limiting the neck movements and stabilizing it during induction and intubation throughout the procedure. Sevoflurane was chosen as inhalational agent because it is non-irritant, tolerated well by children and gives fast induction and recovery. If muscle relaxation is felt necessary, provided the lungs can be ventilated adequately, suxamethonium provides the best intubating conditions.10 The controversy regarding the appropriate mode of induction still exists. Some anesthesiologists prefer the use of intravenous agents, while others choose inhalational agents (especially in children), but most of the authors suggest avoiding muscle relaxants. The relaxation of the supraglottic tissue may preclude effective bag-mask ventilation.12 Endotracheal intubation using fiberoptic technique, being minimally invasive and allowing neutral head position is strongly recommended in these patients.13 Oral fiberoptic technique might be difficult due to large, heavy, anteriorly placed, ‘hanging epiglottis’ (sometimes resting on the tongue base) making the passage of the fiberscope impossible. Nasal fiberoptic technique may also be difficult related to mucopolysaccharoid infiltration in the nasopharynx, with the increased risk of bleeding.14 Fiberoptic bronchoscope may not be available at most canters and it also requires special skills.
CONCLUSION
Understanding the Morquio syndrome and careful planning of the anesthetic technique enables us to manage such patients successfully. A thorough preoperative evaluation of the airways, careful assessment of cervical spine, cardiac, respiratory and neurological functions are paramount in the anesthetic care of such patients. Inhalational induction may be useful to overcome the problem of difficult intubation when fiberoptic intubation is not possible.
REFERENCES
- Morquio L. Sur une forme de dystrophie osseuse familiale. Arch Med Enfants 1929; 32:129-140.
- Holzgreve W, Gröbe H, von Figura K, Kresse H, Beck H, Mattei JF. Morquio syndrome: clinical findings in 11 patients with MPS IVA and two patients with MPSIVB. Hum Genet1981;57:360–5. [Medline]
- Lowry RB, Renwick DH. Relevant frequency of the Hurler and Hunter syndromes.N Engl J Med1971;284:221-222. [Medline]
- Nelson J. Incidence of the mucopolysaccharidoses in Northern Ireland.Hum Genet1997;101(3):355-8. [Medline]
- Gösele S, Dithmar S, Holz FG, Völcker HE. Late diagnosis of Morquio syndrome. Clinical histopathological findings in a rare mucopolysaccharidosis. Klin Monbl Augenheilkd 2000;217(2):114-117. [Medline]
- Walker RW, Darowski M, Morris P, Wraith JE. Anaesthesia and mucopolysaccharidoses. Anaesthesia1994;49:1078-84. [Medline]
- Man TT, Tsai PS, Rau RH, Cheng CR, Ko YP, Wu KH. Children with mucopolysaccharidoses– three cases report. Acta Anaesthesiol Sin 1999;37:93-96. [Medline]
- Renteria VG, Ferrans VJ, Roberts WC. The heart in the Hurler syndrome. Am J Cardiol1976;38:487-501. [Medline]
- Ireland MA, Rowlands DB. Mucopolysaccharidosis type 4 as a cause of mitral stenosis in an adult. Br Heart J 1981;46:113-15. [Medline] [Free PMC Article]
- King DH, Jones RM, Barnett MB. Anaesthetic considerations in the Mucopolysaccharidoses. Anaesthesia1984;39:126-31. [Medline]
- Diaz JH, Belani KG. Perioperative management of children with mucopolysaccharidosis. Anesth Analg1993;77:1261-70. [Medline]
- Tobias JD. Anesthetic care for the child with Morquio syndrome: general versus regional anesthesia. J Clin Anesth 1999;11(3):242-246. [Medline]
- McLaughlin AM, Farooq M, Donnelly MB, Foley K. Anaesthetic considerations of adults with Morquio syndrome – a case report. BMC Anesthesiol 2010 Feb 26;0:2. doi: 10.1186/1471-2253-10-2. [Medline] [Free PMC Article]
- Kadic L, Driessen JJ. Driessen:General anaesthesia in an adult patient with Morquio syndrome with emphasis on airway issues. Bosn J Basic Med Sci 2012;12(2):132-133. [Medline]
