
L.K. Raiger1, Ravindra Kumar Gehlot2, Vikram Bedi3, Sneha Arun Betkeker4
1Senior Professor, 2Assistant Professor, 3Professor,
Department of Anesthesiology, R.N.T. Medical College, Udaipur, Rajasthan (India).
4Speciality Registrar Anesthetics, Glan Clwyd Hospital, Bodelwyddan (UK).
Correspondence: Dr. Sneha Arun Betkeker,
Address- Flat 61, Staff Residences, Glan Clwyd Hospital, Bodelwyddan, (UK) LL185UJ
E mail: snehabetkekar@hotmail.com
Cell: +447507700071
ABSTRACT
Background and aims: Hip fractures are painful and usually affects elderly patients. If left untreated or under-treated, post-operative pain may increase the length of hospital stay and delayed ambulation. The use of peripheral nerve blocks in this population can significantly reduce the associated mortality and morbidity, without the side effects of systemic analgesics. We conducted this study to compare the use of levobupivacaine with bupivacaine in fascia iliaca compartment block (FICB) for postoperative pain management in surgeries for fractures of neck of femur
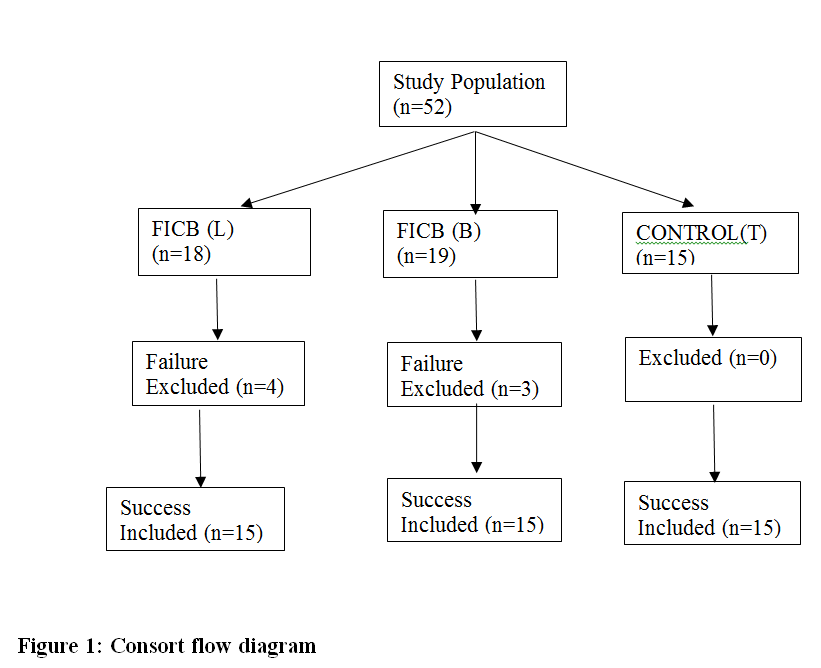
Methodology: This prospective, randomised, double blind study was carried out after approval from the ethical committee and obtaining written informed consent. We enrolled 45 patients undergoing surgery under spinal anesthesia for extracapsular fractures of proximal femur and divided into 3 groups (15 each). Group L: received FICB with 30 ml of levobupivacaine 0.25% (75 mg). Group B: received FICB with 30 ml of bupivacaine 0.25% (75 mg). Group T: no block given. After 30 min patients were shifted to operating room and administered spinal anesthesia in sitting position. Primary outcome was total analgesic consumption in 24 h. Secondary outcomes- patient comfort during positioning for spinal, sensory onset time, postoperative VAS, and time to first analgesic request were registered
Results: Cumulative analgesic consumption was significantly lower in Groups L (93.33 ± 59.362 mg) and B (126.67 ± 45.774 mg) as compared to Group T (273.33 ± 79.881 mg); no significant difference was found between Groups L and B. The time to first analgesic request in Group L was 877.33 ± 355.673 min, Group B was 845.33 ± 379.997 min and Group T was 202.67 ± 142.351 min. Patient comfort on positioning was lowest in Group T.
Conclusion: Administration of FICB in patients undergoing surgery for fractures of proximal femur led to a significant reduction in postoperative pain as compared to systemic analgesics alone. The use of equal concentration of levobupivacaine as compared to bupivacaine provided no added advantage.
Key words: Fascia iliaca compartment block; FICB; Levobupivacaine; Bupivacaine; Hip fractures
Citation: Raiger LK, Gehlot RK, Bedi V, Betkeker SA. Comparison of levobupivacaine and bupivacaine in fascia iliaca compartment block (FICB) for postoperative pain management in surgeries for fractures of neck of femur. Anaesth pain & intensive care 2019;23(3):284-289
Clinical Trial Registery of India (CTRI) Registration Number– CTRI/2018/01/011464
Received: 2 April 2019, Reviewed: 24 September, 13 October 2019, Revised: 22 October, 6 Accepted: 22 October 2019
INTRODUCTION
Hip fractures are always painful, and inadequately controlled pain can have significant psychological and physiological effects. Patients with this injury are usually elderly. It has been shown that patients with higher postoperative pain have an increased length of hospital stay, delayed ambulation, and long term functional impairment.1 Systemic analgesia including both opioids and non-steroidal analgesia can have significant adverse effects especially in the elderly population due to age related changes in pharmacokinetics and pharmacodynamics.2 The use of peripheral nerve blocks for pain management in this population can significantly reduce the morbidity and mortality associated with hip fractures, without the side effects of systemic analgesics.2 Currently bupivacaine is one of the most commonly used local anesthetic for central and peripheral nerve blocks; however, it has the potential to cause serious cardiovascular side effects. Levobupivacaine can prove to be a safe substitute to bupivacaine for management of pain in hip surgery patients receiving fascia iliaca compartment block (FICB). No study directly comparing the two drugs for postoperative pain relief in hip fractures using FICB has been published to date; hence we planned this study to compare the two drugs (bupivacaine and levobupivacaine) in the FICB.
We aimed to compare the clinical efficacy of 0.25% levobupivacaine to 0.25% bupivacaine in fascia iliaca compartment block for postoperative pain management in reducing postoperative pain in patients undergoing surgery for extracapsular fractures of proximal femur under spinal anesthesia.
METHODOLOGY
After taking approval from institutional ethics committee and taking informed written consent from the patients for participation, a prospective randomized double blind unmatched placebo control study was carried out over 6 months from April 2016 to September 2016, in our department of anesthesiology.
Sample size: For the present study to have a power of 80% and an alpha error of < 0.05, 12 patients were required in each of the groups. Hence, we selected a sample of 45 patients, 15 in each group, to compensate for any dropouts.
A total of 45 patients, ≥ 18 y of age, scheduled for elective surgery for extracapsular fractures of proximal femur, ASA physical status class I or II, were enrolled for this study. Exclusion criteria were patient refusal, coagulopathy, infection at puncture site, history of local anesthetic allergy and an uncooperative patient.
After preanesthetic evaluation, which included history, examination, and review of investigation, the enrolled patients were explained the risks and benefits of the procedure and informed consent obtained. Randomization was done into three groups of 15 each, using sealed opaque envelope technique depending on the drug as follows:
Group T (n=15): received no block. [Placebo Group]
Group L (n=15): received 30 ml 0.25% levobupivacaine (75 mg)
Group B (n=15): received 30 ml 0.25% bupivacaine (75 mg)
Blinding: Two anesthesiologists were involved in the study. One prepared the drugs and performed the fascia iliaca compartment block and was not involved in the study further. Another anesthesiologist, who was not aware about the type of drug received by the patient, recorded all data (intra and post-operative) in the proforma. Patient, surgeon and the ward nurse remained unaware of the group allocation.
After a period of overnight fasting the patients were transferred to the pre-induction room where a 20 G cannula was inserted in the dorsum of the non-dominant hand and started on appropriate intravenous fluid. Standard monitoring was applied. After noting baseline blood pressure, oxygen saturation and heart rate the patient was placed in the supine position for performance of the block in L and B groups. In case of the T group, a needle was inserted at the site of insertion of the FICB and withdrawn without injection of any drug. These patients were shifted to the operating room after noting baseline vitals.
Fascia iliaca compartment block technique: The FICB was placed using double pop technique as described by Dalens et al.4 with an 18G, 89 mm long Tuohy needle advanced through the anesthetized site at a 75 degree angle to the skin using a loss of resistance technique. As the needle was advanced, the first loss of resistance was felt as the needle tip passed through the fascia lata. The needle was advanced further till second loss of resistance was felt as the needle passed through the fascia iliaca. This technique is often referred to as a double pop technique. Aspiration was performed to rule out intravascular placement and 30 ml of the study drug was injected. Time of administration of the block was noted. Sensory block was checked using loss of cold sensation in the territory supplied by the femoral nerve, motor block by loss of motor function provided by femoral nerve and pain with VAS scores every 5 min for 30 mins. Patients showing no evidence of femoral nerve block after 30 mins received spinal anesthesia and were excluded from the study. Patients with a successful block were transferred to the operating room and placed in the sitting position for spinal anesthesia with the help of an assistant. The patient comfort level was registered during positioning for spinal. Subarachnoid block was performed using 2 ml (10 mg) of 0.5 % heavy bupivacaine with 0.5 ml tramadol (25 mg) in the L 3 – L4 space using 25G Quinke needle under all aseptic precaution. The table was tilted to the operating side to achieve unilateral effect. After confirmation of successful subarachnoid block surgery was allowed to commence. In the postoperative period, patients in all 3 groups received rescue analgesia with intravenous tramadol (2 mg/kg) when requested or when VAS was more than 3, no other routine analgesic regime was prescribed. Pain was assessed using 10 point VAS, where a score of 0 referred to no pain and a score of 10 referred to worst imaginable pain, at 15 mins, 2 h, 6 h, 12 h and 24 h after completion of surgery. The time for first analgesic request and total analgesic consumption was recorded at 15 mins, 2 h, 6 h, 12 h and 24 h after completion of surgery. Sensory block using loss of cold sensation and motor block using modified bromage scale were recorded at 15 min, 2 h and 6 h after completion of surgery. Any complications that occurred as a result of the block or postoperative pain management regime were noted.
Statistical analysis: Statistical analysis was done with SPSS version 16.0 software. Kruskal Wallace test applied for the non-parametric data, while the parametric data were subjected to ANOVA followed by the Tukey’s HSD to determine the differences between the groups.
RESULTS
The three groups were comparable in terms of demographic characteristics including age, sex and ASA grade (Table 1).
Table 1: Demographic data of the patients
| Variables | Group L (n=15) | Group B (n=15) | Group T (n=15) | p-value |
| Age* (y) | 59.13 ± 15.666 | 56.80 ± 17.608 | 60.07 ± 15.494 | 0.853 |
| M:F n (%) | 10 (66.67%):
5 (33.33%) |
10 (66.67%):
5 (33.33%) |
10 (66.67%):
5 (33.33%) |
1.000 |
| ASA I
ASA II |
9 (60%)
6 (40%) |
9 (60%)
6 (40%) |
9 (60%)
6 (40%) |
1.000 |
* Mean ± SD
The success rate of block placement was 81.09%.The duration of surgery in Group L was 67.33 ± 21.784 min, Group B was 68.67 ± 22.793 min and Group T 68.60 ± 14.569 min. This difference between the groups was not significant statistically.
Table 2: Comparative block characteristics
| Variables | Group L (n=15) | Group B (n=15) | Group T (n=15) | p-value |
| Duration of surgery (min) | 67.33 ± 21.784 | 68.67 ± 22.793 | 68.60 ± 14.569 | 1.000 |
| Onset of sensory block (min) | 11.67 ± 3.067 | 16.67 ± 3.619 | 0 | 1.000 |
| Mean time to first analgesic (min) | 877.33 ± 355.673 | 845.33 ± 379.997 | 202.67 ± 142.35 | |
| Total analgesic consumption | 93.33 ± 59.362
|
126.67 ± 45.774
|
273.33 ± 79.881
|
Onset of sensory of block in Group L was significantly earlier as compared to Group B (Table 2). No motor block was seen in either group.
All patients in Group L were comfortable with the position during subarachnoid block placement whereas one patient in Group B complained of pain and discomfort during positioning. This difference between Group L and B was not significant. However, 9/15 patients i.e. 60% in group T were not satisfied and complained of pain during positioning and the difference with Group L and B was statistically significant.
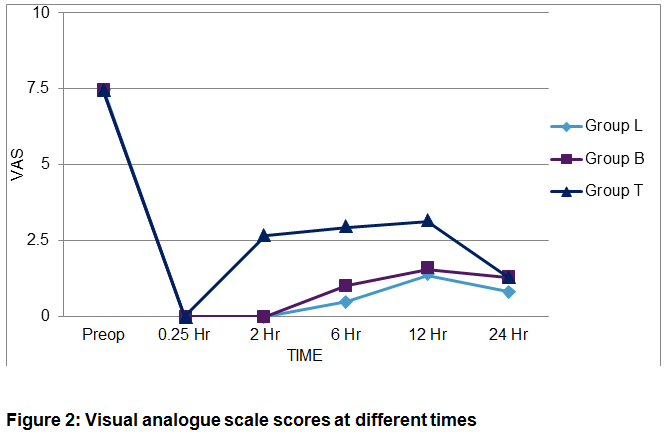
At all time points in the postoperative period (upto 24 h) VAS scores were lower in Group L as compared to the Group B, but the difference was statistically not significant. The VAS was significantly higher in Group T patients at all time points as compared to other two groups (Figure 2).
Mean time to first analgesic request in the Group L was slightly higher than that in the Group B; however, the difference was statistically not significant (Table 2). While in Group T it was significantly earlier compared to other groups (Table 2).
Total analgesic consumption in Group L was less than Group B. It was highest in Group T (Table 2).
No complications related to the block or drugs used in the blocks were noted during our study. Only one patient in the control group who received 400 mg intravenous tramadol (4 doses) developed postoperative nausea and vomiting.
DISCUSSION
In our study the mean age of patients was found to be comparable between the groups. The mean age of the study population was considerably lower in some other studies.3-8 While studies by Foss NB et al. and Mauzopolous G et al. had a higher mean age value than that in our study.9,10
We included patients with extracapsular fractures of proximal femur, which includes intra-trochanteric, sub-trochanteric and cervical neck fractures. The patients with these fractures usually undergo ORIF with DHS, PFN or CC screw. There is no manipulation of the capsule, the posterior part of which is supplied by the sciatic nerve. Hence, pain management in these patients does not require blocking of the sciatic nerve and can be achieved solely by blocking the femoral and lateral femoral cutaneous nerve which can be done by the fascia iliaca compartment block. All groups in our study were comparable in terms of the diagnosis and the types of surgery performed.
In our study spinal anesthesia was the preferred mode of anesthesia and block placement was done preoperatively. Performing the block preoperatively provided the advantage of analgesia during positioning in the sitting position for placement of subarachnoid block. It also allowed the assessment of sensory onset of the FICB without any doubt regarding the residual effect of the subarachnoid block. However, this could affect the effective duration of analgesia so we recorded the duration of the surgery, which was comparable in the three groups.
Different researchers compared the postoperative analgesia provided by the FICB as compared to systemic analgesia at different time points and found that VAS scores were significantly reduced in the FICB group v/s the control group.3,9,10,11 In the FICB group of patients, the mean VAS scores at 10 min and 12 h after the blockade were significantly lower. In addition, postoperative pain was also successfully managed by FICB with mean VAS scores at immediate, 6-h and 12-h time points of 15, 22, and 31 respectively, whereas the corresponding values for the group 2 patients were 62, 49, and 59.The findings of all of these studies was similar to our study group where a highly significant statistical difference was seen between patients receiving block and those not receiving block at 2h, 6 h, 12 h and 24 h.
In a study by Kumie et al.3 the mean time to first analgesic request was at 417 ± 112.10 mins which was less than that seen in our study. There was a significant difference in the mean age of the study population between both studies, our patients being almost double in age. It has been found that there is a significant decrease in pain perception with increasing age due to decline in cognitive function and also an increased sensitivity of peripheral nerves to local anesthetic.12 The time to first analgesic request was 12.28 ± 4.77 h i.e. 748 ± 317 min. Pandya and Jhanwar5 used 35-40 ml of 0.25% bupivacaine as their study drug in both the FICB group and 3-in-1 group. Patients in the FICB group had mean time to first analgesic request 817 ± 186 min. This time to first analgesic request is reflective of the duration of analgesia and was found to be comparable to our study. Only one study has been conducted with levobupivacaine as the analgesic solution in FICB to date, however they did not note the duration of analgesia, so we did not have any reference point for comparison of the Group L. Kumie FT et al3 used both intravenous tramadol and diclofenac sodium as rescue analgesic in their study. The cummulative consumption of diclofenac was significantly less in the FICB group as compared to the control group at 12 h and at 24 h. However, the trend seen with cumulative consumption of tramadol was contrary to this, where no statistical significance was found between the FICB and control group at 12 h and at 24 h. They attributed this finding to the fact that fewer number of patients in the study received tramadol as the primary rescue analgesic postoperatively as compared to diclofenac. The finding by Foss NB et al.9 was similar to our study where the cumulative analgesic consumption between patients who received block and those who did not receive the block was statistically highly significant.
No complications related to the block or drugs used in the block were noted during our study. Only one patient in the control group who received 400 mg intravenous tramadol (4 doses) developed postoperative nausea and vomiting. Foss NB et al.9 noted that patients who required higher dose of morphine were more sedated (6 in control group vs. 1 in FICB group) and had a tendency towards lower oxygen saturation at 60 min and 180 min. There was no difference between groups in nausea and vomiting. No side effects directly attributable to the FICB were noted in contrast to some other studies.10 No incidence of side effects like hematoma, accidental intravascular injection, block failure, or local anesthetic toxicity was noted, which could be directly attributed to the block.
CONCLUSION
We conclude that FICB in patients undergoing surgery for fractures of proximal femur provided adequate analgesia for positioning (sitting) during spinal anesthesia and led to a significant reduction in postoperative pain and in turn analgesic consumption as compared to systemic analgesics alone. The use of equal concentrations of levobupivacaine for FICB and bupivacaine provided similar clinical efficacy and side effect profile.
Conflict of interest: None declared by the authors.
Authors’ contribution:
LKR: Concept, manuscript editing
RKG: Literature search, manuscript editing
VB: Statistical analysis
SAB: Conduct of study, literature search
REFERENCES
- Dulaney-Cripe E, Hadaway S, Bauman R, Trame C, Smith C, Sillaman B, et al. A continuous infusion fascia iliaca compartment block in hip fracture patients: a pilot study. J Clin Med Res. 2012;4(1):45-48. [Pubmed] [Free Full Text]
- Hanna L, Gulati A, Graham A. The role of fascia iliaca blocks in hip fractures: a prospective case-control study and feasibility assessment of a junior-doctor-delivered service. ISRN Ortho. 2014;2014:191306. [Pubmed] [Free Full Text] DOI: 1155/2014/191306
- Kumie FT, Gebremedhn EG, Tawuye HY. Efficacy of fascia iliaca compartment nerve block as part of multimodal analgesia after surgery for femoral bone fracture. World J Emerg Med.2015;6(2):142-146 [Pubmed] [Free Full Text] DOI: 5847/wjem.j.1920-8642.2015.02.010
- Dalens B, Vanneuville G, Tanguy A. Comparison of the fascia iliaca compartment block with the 3-in-1 block in children. AnesthAnalg. 1989;69(6):705–713. [Pubmed]
- Pandya M, Jhanwar S. Comparative study of fascia iliaca compartment block and three in one block for postoperative analgesia in patients undergoing lower limb orthopedic surgeries. Indian J Pain. 2014;28:129-33.
- Hussain R, Nazeer T, Asim A. Unilateral fascia iliaca block (fib) for post-operative analgesia in fracture neck of femur surgery; comparison with standard post-operative analgesia. PJMHS. 2014;8(4):820.4. [Free Full Text]
- Wallace JB, Andrade JA, Christensen JP, Osborne LA, Pellegrini JE. Comparison of fascia iliaca compartment block and 3-in-1 block in adults undergoing knee arthroscopy and meniscal repair. AANA J. 2012;80:37-44. [Pubmed]
- Capdevila X, Biboulet P, Bouregba M, Barthelet Y, Rubenovitch J, d’Athis F. Comparison of the three-in-one and fascia lliaca compartment blocks in adults: clinical and radiographic analysis. AnesthAnalg 1998;86:1039-44. [Pubmed]
- Foss NB, Kristensen BB, Bundgaard M, Bak M, Heiring C, Virkelyst C, et al. Fascia iliaca compartment blockade for acute pain control in hip fracture patients: a randomized, placebo-controlled trial, Anesthesiology. 2007 Apr;106(4):773-8. [Pubmed]
- Mouzopoulos G, Vasiliadis G, Lasanianos N, Nikolaras G, Morakis E, Kaminaris M. Fascia iliaca block prophylaxis for hip fracture patients at risk for delirium: a randomized placebo-controlled study. J Orthop Traumatol. 2009;10(3):127-133. [Pubmed] [Free Full Text]
- Fujihara Y, Fukunishi S, Nishio S, Miura J, Kayanagi S, Yoshiya S,.Fascia iliaca compartment block; its efficacy in pain controle for patients with proximal femoral fracture. J Orthop Sci. 2013;18(5): 793-7 [Pubmed] DOI: 1007/s00776-013-0417-y
- Miller RD. (2015). Miller’s Anesthesia. 8th Philadelphia. Elsevier. p. 2409-20.
