
Muhammad Rafiq, PhD
Institute of Clinical Psychology, University of Management and Technology, Johar Town, Lahore, (Pakistan)
Correspondence: Dr Muhammad Rafiq, PhD,
Institute of Clinical Psychology, University of Management and Technology, C-II, Johar Town, Lahore, Punjab 54770, (Pakistan);
Phone: +92 3213330471; E-mail: rafiqdar@hotmail.com
ABSTRACT
Recent findings have indicated that hypnotic interventions produce significant decrease in pain intensity. This current case studies are focused to highlight significant impact on pain management including headache. All the patients underwent a complete observation and clinical interview and only patients with psychological pain were included in the study group. For the management of headache, a novel hypnotic intervention – Circle Therapy (CT), was applied on a group of ten patients indicating their pain intensity in the range of 8-10 on subjective pain rating scale. According to rating scale, headache above 8 was considered as severe, 5-8 moderate and < 5 as mild. CT is a brief hypnotic technique limited to about 10 min. Post hypnosis ratings were also measured. The pre and post hypnosis data were recorded and analyzed by paired samples t test. Use of CT showed significant results between pre and post rating e.g. 9 ± 0.25 vs. 1 ± 0.21 (p < 0.001). This brief CT intervention provided an immediate relief from headache, however, this is limited to few case studies focusing on just headache. So, we recommend large sample studies to document the effects of CT in different types of pain.
Key words: Pain management; Circle therapy; Headache; Suggestibility; Hypnosis, Brief psychotherapy
Citation: Rafiq M. Circle therapy for headache management: case studies. Anaesth pain intensive care 2020;24(1):__
DOI: https://doi.org/10.35975/apic.v24i1.
Received – 28 December 2019; Reviewed – 10 January 2020; Accepted – 10 January 2020
INTRODUCTION
Pain of any type is considered as serious healthcare problem and according to WHO, headache has a high prevalence of 47% and is among major causes of disability. Headache is the commonest neurological condition presenting to primary care with 3% of adults consulting for headache.1 So its management is important and different pharmacological and non-pharmacological interventions have been used to treat it. Studies have also shown beneficial effect of hypnosis in reducing the pain of medical and psychological origin.2 Research on the effects of psychological interventions including hypnosis has proved a reduction in pain.3,4 Literature has also shown that the art of hypnotherapy is useful in a variety of pains either of biomedical or psychological origin, i.e. migraine, cancer induced pain, stress induced headache, and arthritis etc.5-10
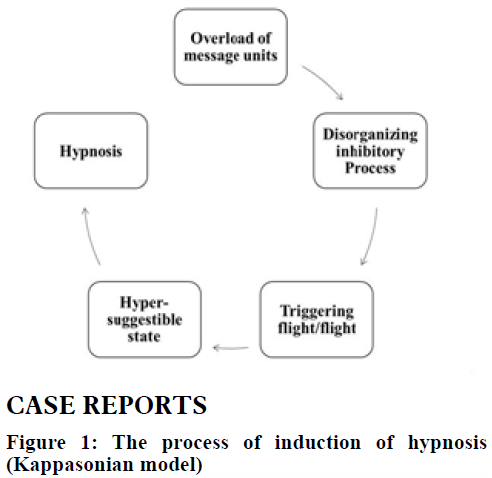
Hypnosis has been induced through different approaches and there are different models of hypnosis. One of the models of hypnosis is the Kappasonian model, which states that hypnosis is induced by an overload of messages from the environment to conscious and subconscious mind of the patient. This overload of messages work by blocking the critical faculty of the mind, creating fight/flight reactions of the body leading to the sub-conscious mind that is hyper-suggestible state, called hypnosis.11 The Kappasonian model of hypnosis’s process is shown in Figure 1.
The important part during hypnosis is ‘suggestion’; and the most important aspect of suggestion is the way it is given. This particular way of giving suggestion is called suggestibility. According to Kappasonian model, suggestibility is mainly of two types i.e. emotional suggestible and physical suggestible. Emotional suggestible people are more suggestible if they are given inferred suggestions, while physical suggestible are those who are more suggestible to indirect or inferred suggestions.11
CASE REPORTS
Participants: Ten patients of both the genders were studied to explore the effect of hypnotic technique, circle therapy (CT) for the reduction of headache. The patients were selected from the referred cases by the medical physician for assessment and management of headache due to any psychological stressors. The patients were observed and clinically interviewed to assess factors of the pain. Almost all the patients were suffering from severe headache off and on since few weeks. The patients were taking analgesic medication since days and they reported a temporary effect but no permanent effect.
On the basis of patients’ history and clinical interview, it was assumed that the headache might be due to psychological stressors. The patients were selected whose headache was assessed to be without any medical reason or any chronic disease. For all the patients, pre-hypnosis pain intensity was assessed on a rating scale. As it is important to assess the suggestibility of the patient for better suggestions during hypnosis, all the patients were assessed for suggestibility through handwriting analysis and finger spreading technique and also assessed to be emotional suggestible.
Procedure: Before the induction of therapy, all the patients were in agreement to finish the headache. The patients were briefed about the hypnotic process and its steps. The whole process of hypnosis and CT induction included these steps:
First step: all patients were relaxed through deep breathing on a recliner in a peaceful room with moderate temperature. In undisturbed and calm state, brain waves are usually theta, which can be helpful in attaining hypnotic state more easily.12
Second step: hypnotic state was created by asking each patient to concentrate on central point of a circle on a desktop of a computer and they were suggested to close their eyes as they feel tired. Average eyes closing time for the patients was around 2-3 min.
Third step: all the patients were given a plain paper and black pen and when they were in hypnotic state, they were suggested: “Please draw a circle clockwise as you start to relieve and keep drawing circle till fully relaxed and calm”. After drawing few circles, they were feeling very less or no pain and they were relaxed and confident. One of the copies of the picture of the circles drawn by them is shown in Figure 2.
RESULTS
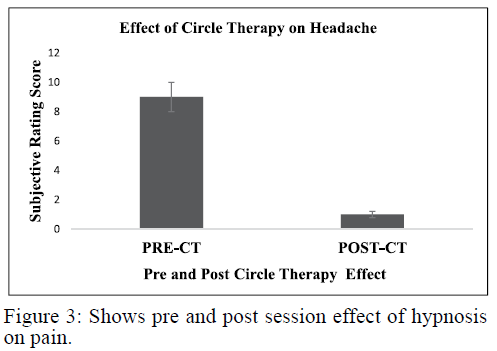
One way repeated measures ANOVA showed a significant effect of CT on headache, F (1, 9) = 2880, p = 0.000, ηp2 = .997. Post-hoc analysis showed that there was a significant difference between pre- and post-hypnosis for headache, (9 ± 0.25 vs. 1 ± 0.21 (p < 0.001). Results obtained after one way repeated measures ANOVA are also shown in Table 1 and significant effect of CT show in Figure 3.
Table 1: One-way repeated measures ANOVA for the pre and post CT (N=10)
| Measurements | M | SD | L. Bound | U Bound | F | p |
| Pre-therapy rating | 9.00 | .25 | 8.41 | 9.58 | 2880.00 | 0.001*** |
| Post-therapy rating | 1.00 | .21 | .52 | 1.47 |
DISCUSSION
Our results on the current case studies explored the effect of CT, a novel hypnotic technique for reduction of headache. There was significant effect of CT post hypnosis and patients felt an immediate relief from headache through hypnotic suggestions. This CT is based on Kappasonian model of hypnosis which states that subconscious mind is hyper suggestible. The subconscious mind can be assessed by overload of message units leading to inhibition of critical faculty of mind as shown in the Figure 1.11 Message units can be of various types, including authority/credentials of the therapist, clinic venue, persuasive communication of the therapist, rapport building, suggestibility style, etc. In this case series, physical and psychological types of message units were used to disorganize the critical minds of the patients. Physical message units were included: peaceful room, comfortable chair, deep breathing and psychological: referral (as they were referred by the medical doctor to have hypnotic intervention for the headache), credentials and certifications of the therapist, so a strong belief on the therapist. These message units have not created only a psychological impact but also rationale for induction of hypnotic state, especially physical message units. We used deep relaxation in these cases, which has an impact not only on pain relief but a relaxed state is more prone to induce trance.13 As the patients were in hypnotic state (procedure described above), therapist gave a suggestion, “Please do start drawing a circle clockwise as you start to relieve and keep drawing circle till fully relaxed”. It is recommended to suggest the patient by giving positive alternatives during subconscious mind, as subconscious mind responds well to the positive suggestions. The therapist repeated the suggestion with low tone, “Keep drawing the circle clockwise till no pain”. As the patients stop drawing circle when they feel zero pain, the author named the therapy as CT. Giving suggestion in low tone is way of emotional suggestibility, as patients were observed emotional suggestible through handwriting analysis and finger spreading technique. Physical suggestible people spread their fingers more quickly if they are suggested with loud voice tone. Emotional people spread their fingers more quickly if they are asked to do that in low tone of voice.11 This concept of suggestibility might use the concept of perceptual and cognitive distraction in minimizing pain perception.14 This is again dependent on subconscious mind as cognitive distraction is best achieved by assessing the subconscious mind, as subconscious mind is hyper-suggestible.15
Literature has indicated that our mind is implicated in perception of headache. Studies have also shown that psychological stressors influence pain perception. However, studies have also indicated that hypnosis is helpful in inducing the state of anesthesia.16 So, the state of hypnosis may be helpful altering the state of mind and this may reduce the pain perception. Biomedical studies have also indicated that the pain pathways may be activated by different psychological factors including negative emotions, stress and empathy.17 Studies have indicated that hypnosis can be used for the management of psychological issues18 and this will help in the management of psychogenic pain.
Our results cannot be generalized to suggest the use of hypnosis for physiological pain and/or other kinds of pain including migraine. However, studies have revealed that pain can be of physiological or psychological origin and studies have suggested that pain, whether physical or psychological, shares the same underlying neurological mechanisms.19 So, the state of hypnosis might be helpful in the management of physiological pain as well. The brain areas that are found to be implicated in either type of pain are anterior cingulate cortex and prefrontal cortex and may extend to other regions as well. As similar brain areas are involved in both physical and psychological pain, we should see pain as a continuum that ranges from purely physical to purely psychological.20 With such interesting and novel results, there are certain limitations, as our data on the effect of hypnosis on headache of psychological origin, we can’t conclude for any physical, medical type of pain and/or pain associated with any chronic disease like arthritis, hepatitis, migraine etc. Our case series involved patients with emotional suggestibility, so results might have been different had we used physical suggestibility. We recommend that an intensive research may be conducted to investigate above mentioned variables.
CONCLUSION
Our study shows an effective strategy for management of the headache. The advantages of using circle therapy are; management of the headache of psychological origin without any side effects and unnecessary use of analgesics. There is a need to apply this technique on other types of pain and to conduct large scale studies to compare the effects with other treatment modalities.
Conflict of interest: The author declares no conflict of interest
Author’s contribution: The author was the sole responsible for the concept, data analysis, manuscript writing and review.
Consent: Written informed consent was obtained from the patients for communication of his/her case report with accompanying image.
REFERENCES
- R Latinovic, M Gulliford, L Ridsdale. Headache and migraine in primary care: consultation, prescription, and referral rates in a large population. J Neurol Neurosurg Psychiatry. 2006;77(3):385–7. [PubMed] DOI: 1136/jnnp.2005.073221
- Lang EV, Benotsch EG, Fick LJ, Lutgendorf S, Berbaum ML, Berbaum KS, et al. Adjunctive non-pharmacological analgesia for invasive medical procedures: a randomised trial. Lancet. 2000;355(9214):1486-90. [PubMed] DOI: 1016/S0140-6736(00)02162-0
- Jensen M, Patterson DR. Hypnotic treatment of chronic pain. J Behav Med. 2006 Feb;29(1):95-124. [PubMed] DOI: 1007/s10865-005-9031-6
- Montgomery GH, DuHamel KN, Redd WH. A meta-analysis of hypnotically induced analgesia: how effective is hypnosis? Int J Clin Exp Hypn. 2000 Apr;48(2):138-53. [PubMed] DOI: 1080/00207140008410045
- Haanen HC, Hoenderdos HT, van Romunde LK, Hop WC, Mallee C, Terwiel JP, et al. Controlled trial of hypnotherapy in the treatment of refractory fibromyalgia. J Rheumatol. 1991 Jan;18(1):72-5. [PubMed]
- Appel PR, Bleiberg J. Pain reduction is related to hypnotizability but not to relaxation or to reduction in suffering: a preliminary investigation. Am J Clin Hypn. 2005 Oct-2006 Jan;48(2-3):153-61. [PubMed] DOI: 1080/00029157.2005.10401512
- Jensen MP, Hanley MA, Engel JM, Romano JM, Barber J, Cardenas DD, et al. Hypnotic analgesia for chronic pain in persons with disabilities: A case series abstract. Int J Clin Exp Hypn. 2005 Apr;53(2):198-228. [PubMed] DOI: 1080/00207140590927545
- Gay MC, Philippot P, Luminet O. Differential effectiveness of psychological interventions for reducing osteoarthritis pain: a comparison of Erickson hypnosis and Jacobson relaxation. Euro J Pain. 2002;6(1):1-16.
- Elkins G, et al. Hypnosis to reduce pain in cancer survivors with advanced disease: a prospective study. Psycho-oncology. 2005;14:S63.
- Rafiq M. Headache management through hypnosis: a case report. Anaesth Pain Intensive Care. 2018:22(2):227-30. [Free full text]
- Kappas JG. Professional Hypnotism manual: introducing physical and emotional suggestibility and sexuality. Panorama Publishing Company; 1987.
- Jensen MP, Adachi T, Hakimian S. Brain oscillations, hypnosis, and hypnotizability. Am J Clin Hypn. 2015;57(3):230-53. [PubMed] DOI: 1080/00029157.2014.976786
- Vickers A, Zollman C, Payne DK. Hypnosis and relaxation therapies. West J Med. 2001 Oct;175(4):269-72. [PubMed] DOI: 1136/ewjm.175.4.269
- Spiegel H, Spiegel D. Trance and treatment: Clinical uses of hypnosis. American Psychiatric Pub; 2008.
- Lynn SJ, Shindler K, Meyer E. Hypnotic suggestibility, psychopathology, and treatment outcome. Sleep Hypnosis. 2003;5(1):17-25. [Free Full Text]
- Facco E. Hypnosis and anesthesia: back to the future. Minerva Anestesiol. 2016;82(12):1343-56. [PubMed]
- Villemure C, Bushnell CM. Cognitive modulation of pain: how do attention and emotion influence pain processing? Pain. 2002;95(3):195-9. [PubMed] DOI: 1016/s0304-3959(02)00007-6
- Fisch S, Brinkhaus B, Teut M. Hypnosis in patients with perceived stress–a systematic review. BMC Complement Altern Med. 2017;17(1):323. DOI: 1186/s12906-017-1806-0
- Meerwijk EL, Ford JM, Weiss SJ. Brain regions associated with psychological pain: implications for a neural network and its relationship to physical pain. Brain Imaging Behav. 2013;7(1):1-14. [PubMed] DOI: 1007/s11682-012-9179-y
- Biro D. Is there such a thing as psychological pain? And why it matters. Cult Med Psychiatry. 2010;34(4):658-67. [PubMed] DOI: 1007/s11013-010-9190-y
