Ahmed H. Bakeer, MD1, Nasr M. Abdallah, MD2
1Department of Anesthesiology & Pain Management, National Cancer Institute,
Cairo University, Kasr Al Eini,
Street Fom El Khalig, Cairo, (Egypt)
2Department of Anesthesia,
Faculty of Medicine,
Cairo University, Kasr Al Eini, Cairo, (Egypt)
Correspondence: Dr Ahmed H, Bakeer, Department of Anesthesia and Pain Management, National Cancer Institute, Cairo University, Fom EL Khaleeg, Cairo, (Egypt)
Tel: +20233360906
E-mail: mail@mcs-center.com
ABSTRACT
Objective: Endotracheal intubation is associated with hemodynamic response that may be serious in high-risk patients. This study compared oral gabapentin 900 mg alone or with 7.5 mg oral midazolam on the hemodynamic responses to direct laryngoscopy and endotracheal intubation (LETI).
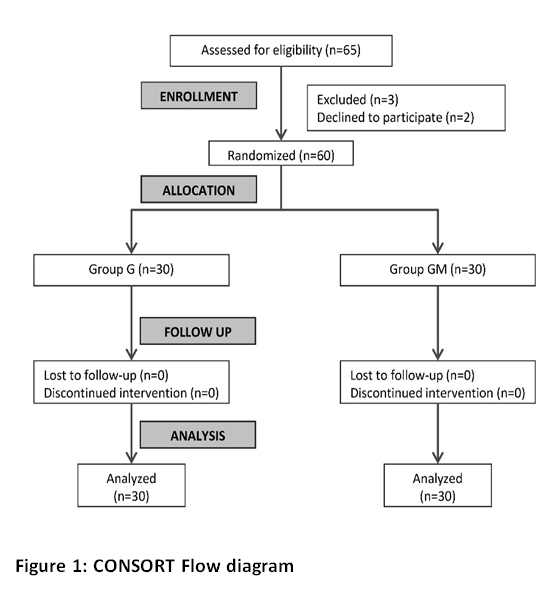
Methodology: This randomized, double-blind clinical trial was conducted in operating room complex, National Cancer Institute, Cairo University, Cairo. The study included 60 normotensive adults scheduled for modified radical mastectomy under general anesthesia. The participants were randomly allocated to two equal groups to receive premedication either with oral gabapentin 900 mg (Group G) or gabapentin 900 mg plus 7.5 mg midazolam (Group GM).
Sedation was monitored up to the time of induction of anesthesia. Heart rate (HR) and systolic and diastolic blood pressures were recorded up to 30 min of laryngoscopy.
Results: In the two groups, systolic and diastolic blood pressure and heart changes were controlled up to 30 min intra-operatively. Systolic and diastolic blood pressure were significantly lower in Group GM compared to Group G. At all times, there was no significant difference in heart rate between the two groups.
Conclusion: Oral gabapentin is effective in attenuation of the hypertensive response to laryngoscopy and endotracheal intubation when administered in a dose of 900 mg 90 min before modified radical mastectomy. It is more effective when combined with oral midazolam 7.5 mg.
Keywords: Stress response; Gabapentoids; Benzodiazepines; Laryngoscopy
Citation:Bakeer AH, Abdallah NM. Attenuation of the hemodynamic response to tracheal intubation with gabapentin and oral midazolam.Anaesth. pain & intensive care 2019;23(1):37-
ISRCTN Registration number: ISRCTN15943548
Received – 8 December 2018; Reviewed – 18 December 2018; Revised –22 January 2019; Reviewed – 28 January, 15 February 2019; Accepted – 20 February 2019
INTRODUCTION
Endotracheal intubation is the definitive method of securing the airway before surgery. However, this procedure is not without adverse effect; it can induce sympathetic nervous system stimulation with ensuing hemodynamic response that may lead to cardiovascular instability and myocardial ischemia in high-risk patients.1 At least in such individuals, there is a necessity to blunt this response. Enduring efforts have been exerted to find the drugs that can safely prevent the exaggerated pressor response during laryngoscopy and endotracheal intubation. Numerous drugs have been tried for this purpose. These include topical2 or intravenous (IV) local anesthetics,3 narcotic analgesics,4 β-adrenergic blockers,5 vasodilators,6 and many others.
Gabapentin is a structural analogue of the neurotransmitter, γ–aminobutyric acid (GABA) that was introduced as an antiepileptic drug.7 It was proved to be effective in controlling neuropathic pain and acute postoperative pain with a reduction of postoperative opioid requirements.8 It has been used to attenuate the pressor response to laryngoscopy and endotracheal intubation.9,10
A drug combination is thought to provide a safer and more balanced effect in anesthesia. Using readily available drugs seems a good idea in situations with limited resources. In the literature, we could not find any study evaluating the combined effect of gabapentin and midazolam, on hemodynamic response to tracheal intubation. Therefore, we conducted this study to compare the effect of a single preoperative oral dose of 900 mg gabapentin alone or in combination with 7.5 mg oral midazolam on the hemodynamic responses to direct laryngoscopy and endotracheal intubation.
METHODOLOGY
Sixty normotensive adults scheduled for modified radical mastectomy under general anesthesia with endotracheal intubation were included in this prospective randomized, double-blind study. The study was carried out from April 2017 to June 2018 after approval of institutional ethical committee. The study implemented the principles of the Declaration of Helsinki (1964) and its following revisions. The study was registered on the ISRCTN registry with study ID ISRCTN15943548.
Inclusion criteria were patients between 18 and 65 years old with American Society of Anesthesiologist (ASA) physical status I or II, undergoing modified radical mastectomy under general anesthesia. Exclusion criteria were allergy to gabapentin or midazolam, body mass index > 35 kg/m2, patients with a history of cardiac, pulmonary, severe liver or renal disease, patients taking sedatives, hypnotics or antihypertensive medications, and patients with anticipated difficult intubation. Patients with duration of laryngoscopy more than 22 sec and those in need of a second attempt of intubation were excluded from the study.
The participants were randomly allocatedto one of the two groups using computerized randomization. Group G (n =30) received oral gabapentin 900 mg (Neurontin 300 mg, 3 x capsules, Pfizer, Egypt) and a vitamin tablet similar to midazolam tablets. Group GM (n = 30) received oral gabapentin 900 mg plus 7.5 mg midazolam (Midathetic® 7.5 mg tablet, Amoun Pharmaceutical Co., Egypt)
Group allocations were done by an anesthesiologist unaware of and not involved in the study. In the pre-medication room, study drugs were given orally with sips of water 90 min before surgery. Patients were monitored in the premedication room to assess the level of sedation using Ramsay Sedation Scale score starting at 15 min after drug intake up to just before induction of anesthesia. After 90min of drug intake, patients were transferred to the operating room and monitors were attached including ECG pulse oximetry and non-invasive blood pressure. Intravenous access was obtained,anda crystalloid infusion was started. Blood pressure and heart rate values were recorded.A standard anesthetic technique was followed in all patients. Pre-oxygenation for 3 min with 100% oxygen was done and then injection of fentanyl 1 µg/kg and propofol 2 mg/kg. Atracurium 0.5 mg/kg IV was used to facilitate tracheal intubation. Laryngoscopy and intubation were done 3 min after atracurium administration by a senior anesthetist. Anesthesia was maintained with isoflurane in 100% oxygen. Patients were mechanically ventilated to maintain end-tidal CO2 between 35-40 mmHg. Muscle relaxation was maintained with intermittent doses of atracurium. At the end of surgery, anesthetic agents were discontinued,and neuromuscular blockade was reversed by injection of neostigmine of 0.05 mg/kg and atropine 0.01 mg/kg after fulfilling the criteria of extubation. The patients then were transferred to post-anesthetic care unit (PACU) and monitored for the next 24 hours for any drug-induced side effects such as nausea, vomiting, headache, dizziness, visual disturbance, and respiratory depression.
The primary outcome measure was the hemodynamic response to laryngoscopy and intubation, e.g., heart rate (HR), and systolic and diastolic blood pressure recorded at baseline (90 min after premedication) before and after induction and at 1, 3, 5, 10, 15, and 30 min of laryngoscopy. The adverse effects were recorded.Secondary outcome measures were level of sedation and adverse effects of the drugs.
Sample size estimation: Assuming that 15% difference in mean arterial pressure is clinically evocative with an estimated standard deviation of 15 to ensure a power of 0.9 with an alpha error of 0.05, a sample size of 22 patients in each group would be sufficient to elicit the difference. Considering a dropout rate of 10%; 30 patients were included in each arm of the study. The sample size was estimated using the online power calculator for continuous outcome superiority trial under Sealed Envelope Ltd. 2012. Available from: https://www.sealedenvelope.com/power/continuous-superiority/
Statistical analysis:
Statistical analysis was done using IBM© SPSS© Statistics version 22 (IBM© Corp., Armonk, NY, USA). Numerical data were expressed as a mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test was used to examine the relationship between qualitative variables. Comparison of repeated measures was made using ANOVA for repeated measures or Friedman test followed by appropriate pairwise comparison. All p-values were corrected due to repeated analyses using Bonferroni correction. A p-value < 0.05 was considered significant.
RESULTS
There was no significant difference in baseline characteristic between the two studied groups (Table 1).In Group G, relative to the baseline reading, SBP decreased significantly after induction. Then it increased significantly up to 3 min after laryngoscopy and endotracheal intubation (LETI) relative to the reading before induction. It started to drop up again 5 min after LETI. The same was observed in Group GM. From 1 to 10 min after LETI, the SBP in Group GM was significantly lower than Group G (Table 2).
Diastolic blood pressure showed similar changes as SBP in Group G. In Group GM, relative to the baseline reading, DBP decreased significantly after induction. Then it increased significantly 1 and 3 min after LETI compared to that after induction, then it started to decline 10 min after LETI. From 1 to 5 min after LETI, the DBP in Group GM was significantly lower than Group G (Table 3).
In Group G, relative to the baseline reading, HR decreased significantly after induction of anesthesia; increasing significantly one minute after LETI, and then dropped till 30 min after LETI. In Group GM, relative to the baseline reading, HR did not show significant change after drug administration, increasing significantly one minute after LETI, and then it dropped till 30 min after LETI. At any given time, there was no significant difference in HR between the two groups (Table 4).
All patients of the two groups were well sedated (Ramsey score 2 or 3) before surgery with significantly higher sedation scores in the combined group after 15 and 30 min (p < 0.001). A limited number of adverse effects were recorded. In Group G, two patients developed nausea, one had vomiting and another one had a headache. In Group GM, one patient had nausea and two had mild headache.
DISCUSSION
In the current study, we evaluated the effect of pretreatment with a single dose of gabapentin 900 mg alone or combined with 7.5 mg of midazolam 90 min before surgery on hemodynamic response to LETI in normotensive women undergoing modified radical mastectomy. The two regimens were found effective for attenuating the pressor response to LETI, but the gabapentin-midazolam combination was associated with significantly lower blood pressure up to 10 min after intubation.
Previous investigators have reported the effectiveness of gabapentin in different dose regimens in attenuation of the hemodynamic response to LETI in normotensive patients. In a randomized, double-blind study, Memis et al.10 reported that gabapentin 800 mg - but not 400 mg - blunted the hemodynamic response to endotracheal intubation during the first 10 min in patients undergoing different types of surgical procedures. Marashi et al.9 found gabapentin 900 mg two hours before surgery was more effective than clonidine in blunting hyperdynamic responses. Bafna et al. reported similar effectiveness of gabapentin in a dose of 1000 mg; the 600 mg dose was not effective.11 In the current study, we selected the 900 mg dose based on the results of these studies.
Fassoulaki et al. adopted a different protocol; they used 1600 mg gabapentin starting the day before surgery in 4 divided doses. Gabapentin decreased systolic and diastolic blood pressure, but it did not affect the tachycardia associated with LETI.12 In this study, gabapentin blunted the tachycardia provoked by LETI. It is known that midazolam may be associated with increased heart rate,13 but this effect was not evident in the combined group, probably due to the influence of gabapentin on heart rate as proved in previous studies.9,10 A recent systematic review of 29 randomized trials has shown that gabapentin attenuates the rise in blood pressure and heart rate one minute after intubation. However, the authors concluded that the included studies were at potential risk of bias.1
Koc and colleagues14examined pretreatment with a combination of gabapentin and dexamethasone one hour before varicocele surgery. The found the HR and MAP values were significantly lower in the combined groups at 1, 3, 5, and 10 min after intubation compared to either drug alone. The hemodynamic effects of gabapentin or dexamethasone alone were comparable. So, gabapentin alone was effective in suppressing the response to tracheal intubation and was more effective when combined with dexamethasone. In the current study, oral midazolam in a dose of 7.5 mg potentiated the effect of gabapentin on hemodynamic response to tracheal intubation. The main difference between the two combinations (dexamethasone/gabapentin and midazolam/gabapentin) is the effect on HR. Midazolam suppressed the blood pressure response but not the heart rate, while dexamethasone suppressed both. We believe that the maintained heart rate with midazolam is better that the suppressed HR with dexamethasone. This can ensure better blood supply to peripheral tissues especially the central nervous system during the critical few min after induction of anesthesia.
In the current study, we investigated another combination of gabapentin with midazolam,a drug that has been introduced into anesthesia 25 years ago. The hemodynamic effects of midazolam in normal humans have been well recognized. It produces a significant reduction in systolic and diastolic blood pressure and increases in heart rate.15 Midazolam is usually used as a pretreatment agent to reduce anxiety and improve patient satisfaction.16
Previous studies reported that midazolam effectively suppresses the sympathetic activations induced by different stimuli.17-20Also, midazolam was associated with a reduction of hemodynamic and cardiac autonomic nervous system responses when added during induction of anesthesia.13,21 Nishiyama and colleagues21 compared a combination of midazolam 0.1 mg/kg followed by 3 mg/kg thiopental sodium with thiopental 5 mg/kg. In both groups, blood pressure and HR increased in response to tracheal intubation, but the increase was significantly lower in the combined group. Regarding heart rate variability, the midazolam-thiopental group showed significantly lower values of increase of low-frequency component/high-frequency component ratio. In another prospective randomized study, midazolam-propofol combination yielded compensated modulatory effects on the cardiovascular system, which were related to significant increases in the LF/HF ratio after induction, and 1, 3, and 5 min after intubation.13
Gabapentin-midazolam combination may exert a synergistic effect on the hemodynamic response to endotracheal intubation as a result of their different mechanisms of action of the two drugs. Like other benzodiazepines, midazolam effects are mediated by its action on the ionotropic GABAA receptors in the central nervous system (CNS) with rapid onset of action and few adverse effects.22 On the other hand, gabapentin exerts little action on GABA receptors despite being developedinitially as a mimetic of this inhibitory neurotransmitter. It has a high affinity to the α2-δ1 subunit of voltage-gated calcium channels located in the CNS.23 Therefore, it acts in a way similar to calcium channel blockers.
CONCLUSION
Based on the results of our study, we conclude that oral gabapentin is effective in attenuation of the hypertensive response to laryngoscopy and endotracheal intubation when administered in a dose of 900 mg 90 min before modified radical mastectomy. However, it is more effective when combined with oral midazolam 7.5 mg.
Financial support: None to declare
Conflicts of Interest: None to declare
Authors’ contribution:
AB: Concept, literature search, conduction of the study work, and manuscript
editing
NA: Conduction of the study work, data analysis, and manuscript editing
REFERENCES
SBP: systolic blood pressure, DBP: diastolic blood pressure
Data are presented as mean ± SD or number (%)
Table 2: Systolic blood pressure rate at baseline, before and after induction of anesthesia and after endotracheal intubation in the two studied groups
Data are presented as mean ± SD
Table 3: Diastolic blood pressure rate at baseline, before and after induction of anesthesia and after endotracheal intubation in the two studied groups
Data are presented as mean ± SD
Table 4: Heart rate at baseline, before and after induction of anesthesia and after endotracheal intubation in the two studied groups
Data are presented as mean ± SD
1Department of Anesthesiology & Pain Management, National Cancer Institute,
Cairo University, Kasr Al Eini,
Street Fom El Khalig, Cairo, (Egypt)
2Department of Anesthesia,
Faculty of Medicine,
Cairo University, Kasr Al Eini, Cairo, (Egypt)
Correspondence: Dr Ahmed H, Bakeer, Department of Anesthesia and Pain Management, National Cancer Institute, Cairo University, Fom EL Khaleeg, Cairo, (Egypt)
Tel: +20233360906
E-mail: mail@mcs-center.com
ABSTRACT
Objective: Endotracheal intubation is associated with hemodynamic response that may be serious in high-risk patients. This study compared oral gabapentin 900 mg alone or with 7.5 mg oral midazolam on the hemodynamic responses to direct laryngoscopy and endotracheal intubation (LETI).
Methodology: This randomized, double-blind clinical trial was conducted in operating room complex, National Cancer Institute, Cairo University, Cairo. The study included 60 normotensive adults scheduled for modified radical mastectomy under general anesthesia. The participants were randomly allocated to two equal groups to receive premedication either with oral gabapentin 900 mg (Group G) or gabapentin 900 mg plus 7.5 mg midazolam (Group GM).
Sedation was monitored up to the time of induction of anesthesia. Heart rate (HR) and systolic and diastolic blood pressures were recorded up to 30 min of laryngoscopy.
Results: In the two groups, systolic and diastolic blood pressure and heart changes were controlled up to 30 min intra-operatively. Systolic and diastolic blood pressure were significantly lower in Group GM compared to Group G. At all times, there was no significant difference in heart rate between the two groups.
Conclusion: Oral gabapentin is effective in attenuation of the hypertensive response to laryngoscopy and endotracheal intubation when administered in a dose of 900 mg 90 min before modified radical mastectomy. It is more effective when combined with oral midazolam 7.5 mg.
Keywords: Stress response; Gabapentoids; Benzodiazepines; Laryngoscopy
Citation:Bakeer AH, Abdallah NM. Attenuation of the hemodynamic response to tracheal intubation with gabapentin and oral midazolam.Anaesth. pain & intensive care 2019;23(1):37-
ISRCTN Registration number: ISRCTN15943548
Received – 8 December 2018; Reviewed – 18 December 2018; Revised –22 January 2019; Reviewed – 28 January, 15 February 2019; Accepted – 20 February 2019
INTRODUCTION
Endotracheal intubation is the definitive method of securing the airway before surgery. However, this procedure is not without adverse effect; it can induce sympathetic nervous system stimulation with ensuing hemodynamic response that may lead to cardiovascular instability and myocardial ischemia in high-risk patients.1 At least in such individuals, there is a necessity to blunt this response. Enduring efforts have been exerted to find the drugs that can safely prevent the exaggerated pressor response during laryngoscopy and endotracheal intubation. Numerous drugs have been tried for this purpose. These include topical2 or intravenous (IV) local anesthetics,3 narcotic analgesics,4 β-adrenergic blockers,5 vasodilators,6 and many others.
Gabapentin is a structural analogue of the neurotransmitter, γ–aminobutyric acid (GABA) that was introduced as an antiepileptic drug.7 It was proved to be effective in controlling neuropathic pain and acute postoperative pain with a reduction of postoperative opioid requirements.8 It has been used to attenuate the pressor response to laryngoscopy and endotracheal intubation.9,10
A drug combination is thought to provide a safer and more balanced effect in anesthesia. Using readily available drugs seems a good idea in situations with limited resources. In the literature, we could not find any study evaluating the combined effect of gabapentin and midazolam, on hemodynamic response to tracheal intubation. Therefore, we conducted this study to compare the effect of a single preoperative oral dose of 900 mg gabapentin alone or in combination with 7.5 mg oral midazolam on the hemodynamic responses to direct laryngoscopy and endotracheal intubation.
METHODOLOGY
Sixty normotensive adults scheduled for modified radical mastectomy under general anesthesia with endotracheal intubation were included in this prospective randomized, double-blind study. The study was carried out from April 2017 to June 2018 after approval of institutional ethical committee. The study implemented the principles of the Declaration of Helsinki (1964) and its following revisions. The study was registered on the ISRCTN registry with study ID ISRCTN15943548.
Inclusion criteria were patients between 18 and 65 years old with American Society of Anesthesiologist (ASA) physical status I or II, undergoing modified radical mastectomy under general anesthesia. Exclusion criteria were allergy to gabapentin or midazolam, body mass index > 35 kg/m2, patients with a history of cardiac, pulmonary, severe liver or renal disease, patients taking sedatives, hypnotics or antihypertensive medications, and patients with anticipated difficult intubation. Patients with duration of laryngoscopy more than 22 sec and those in need of a second attempt of intubation were excluded from the study.
The participants were randomly allocatedto one of the two groups using computerized randomization. Group G (n =30) received oral gabapentin 900 mg (Neurontin 300 mg, 3 x capsules, Pfizer, Egypt) and a vitamin tablet similar to midazolam tablets. Group GM (n = 30) received oral gabapentin 900 mg plus 7.5 mg midazolam (Midathetic® 7.5 mg tablet, Amoun Pharmaceutical Co., Egypt)
Group allocations were done by an anesthesiologist unaware of and not involved in the study. In the pre-medication room, study drugs were given orally with sips of water 90 min before surgery. Patients were monitored in the premedication room to assess the level of sedation using Ramsay Sedation Scale score starting at 15 min after drug intake up to just before induction of anesthesia. After 90min of drug intake, patients were transferred to the operating room and monitors were attached including ECG pulse oximetry and non-invasive blood pressure. Intravenous access was obtained,anda crystalloid infusion was started. Blood pressure and heart rate values were recorded.A standard anesthetic technique was followed in all patients. Pre-oxygenation for 3 min with 100% oxygen was done and then injection of fentanyl 1 µg/kg and propofol 2 mg/kg. Atracurium 0.5 mg/kg IV was used to facilitate tracheal intubation. Laryngoscopy and intubation were done 3 min after atracurium administration by a senior anesthetist. Anesthesia was maintained with isoflurane in 100% oxygen. Patients were mechanically ventilated to maintain end-tidal CO2 between 35-40 mmHg. Muscle relaxation was maintained with intermittent doses of atracurium. At the end of surgery, anesthetic agents were discontinued,and neuromuscular blockade was reversed by injection of neostigmine of 0.05 mg/kg and atropine 0.01 mg/kg after fulfilling the criteria of extubation. The patients then were transferred to post-anesthetic care unit (PACU) and monitored for the next 24 hours for any drug-induced side effects such as nausea, vomiting, headache, dizziness, visual disturbance, and respiratory depression.
The primary outcome measure was the hemodynamic response to laryngoscopy and intubation, e.g., heart rate (HR), and systolic and diastolic blood pressure recorded at baseline (90 min after premedication) before and after induction and at 1, 3, 5, 10, 15, and 30 min of laryngoscopy. The adverse effects were recorded.Secondary outcome measures were level of sedation and adverse effects of the drugs.
Sample size estimation: Assuming that 15% difference in mean arterial pressure is clinically evocative with an estimated standard deviation of 15 to ensure a power of 0.9 with an alpha error of 0.05, a sample size of 22 patients in each group would be sufficient to elicit the difference. Considering a dropout rate of 10%; 30 patients were included in each arm of the study. The sample size was estimated using the online power calculator for continuous outcome superiority trial under Sealed Envelope Ltd. 2012. Available from: https://www.sealedenvelope.com/power/continuous-superiority/
Statistical analysis:
Statistical analysis was done using IBM© SPSS© Statistics version 22 (IBM© Corp., Armonk, NY, USA). Numerical data were expressed as a mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test was used to examine the relationship between qualitative variables. Comparison of repeated measures was made using ANOVA for repeated measures or Friedman test followed by appropriate pairwise comparison. All p-values were corrected due to repeated analyses using Bonferroni correction. A p-value < 0.05 was considered significant.
RESULTS
There was no significant difference in baseline characteristic between the two studied groups (Table 1).In Group G, relative to the baseline reading, SBP decreased significantly after induction. Then it increased significantly up to 3 min after laryngoscopy and endotracheal intubation (LETI) relative to the reading before induction. It started to drop up again 5 min after LETI. The same was observed in Group GM. From 1 to 10 min after LETI, the SBP in Group GM was significantly lower than Group G (Table 2).
Diastolic blood pressure showed similar changes as SBP in Group G. In Group GM, relative to the baseline reading, DBP decreased significantly after induction. Then it increased significantly 1 and 3 min after LETI compared to that after induction, then it started to decline 10 min after LETI. From 1 to 5 min after LETI, the DBP in Group GM was significantly lower than Group G (Table 3).
In Group G, relative to the baseline reading, HR decreased significantly after induction of anesthesia; increasing significantly one minute after LETI, and then dropped till 30 min after LETI. In Group GM, relative to the baseline reading, HR did not show significant change after drug administration, increasing significantly one minute after LETI, and then it dropped till 30 min after LETI. At any given time, there was no significant difference in HR between the two groups (Table 4).
All patients of the two groups were well sedated (Ramsey score 2 or 3) before surgery with significantly higher sedation scores in the combined group after 15 and 30 min (p < 0.001). A limited number of adverse effects were recorded. In Group G, two patients developed nausea, one had vomiting and another one had a headache. In Group GM, one patient had nausea and two had mild headache.
DISCUSSION
In the current study, we evaluated the effect of pretreatment with a single dose of gabapentin 900 mg alone or combined with 7.5 mg of midazolam 90 min before surgery on hemodynamic response to LETI in normotensive women undergoing modified radical mastectomy. The two regimens were found effective for attenuating the pressor response to LETI, but the gabapentin-midazolam combination was associated with significantly lower blood pressure up to 10 min after intubation.
Previous investigators have reported the effectiveness of gabapentin in different dose regimens in attenuation of the hemodynamic response to LETI in normotensive patients. In a randomized, double-blind study, Memis et al.10 reported that gabapentin 800 mg - but not 400 mg - blunted the hemodynamic response to endotracheal intubation during the first 10 min in patients undergoing different types of surgical procedures. Marashi et al.9 found gabapentin 900 mg two hours before surgery was more effective than clonidine in blunting hyperdynamic responses. Bafna et al. reported similar effectiveness of gabapentin in a dose of 1000 mg; the 600 mg dose was not effective.11 In the current study, we selected the 900 mg dose based on the results of these studies.
Fassoulaki et al. adopted a different protocol; they used 1600 mg gabapentin starting the day before surgery in 4 divided doses. Gabapentin decreased systolic and diastolic blood pressure, but it did not affect the tachycardia associated with LETI.12 In this study, gabapentin blunted the tachycardia provoked by LETI. It is known that midazolam may be associated with increased heart rate,13 but this effect was not evident in the combined group, probably due to the influence of gabapentin on heart rate as proved in previous studies.9,10 A recent systematic review of 29 randomized trials has shown that gabapentin attenuates the rise in blood pressure and heart rate one minute after intubation. However, the authors concluded that the included studies were at potential risk of bias.1
Koc and colleagues14examined pretreatment with a combination of gabapentin and dexamethasone one hour before varicocele surgery. The found the HR and MAP values were significantly lower in the combined groups at 1, 3, 5, and 10 min after intubation compared to either drug alone. The hemodynamic effects of gabapentin or dexamethasone alone were comparable. So, gabapentin alone was effective in suppressing the response to tracheal intubation and was more effective when combined with dexamethasone. In the current study, oral midazolam in a dose of 7.5 mg potentiated the effect of gabapentin on hemodynamic response to tracheal intubation. The main difference between the two combinations (dexamethasone/gabapentin and midazolam/gabapentin) is the effect on HR. Midazolam suppressed the blood pressure response but not the heart rate, while dexamethasone suppressed both. We believe that the maintained heart rate with midazolam is better that the suppressed HR with dexamethasone. This can ensure better blood supply to peripheral tissues especially the central nervous system during the critical few min after induction of anesthesia.
In the current study, we investigated another combination of gabapentin with midazolam,a drug that has been introduced into anesthesia 25 years ago. The hemodynamic effects of midazolam in normal humans have been well recognized. It produces a significant reduction in systolic and diastolic blood pressure and increases in heart rate.15 Midazolam is usually used as a pretreatment agent to reduce anxiety and improve patient satisfaction.16
Previous studies reported that midazolam effectively suppresses the sympathetic activations induced by different stimuli.17-20Also, midazolam was associated with a reduction of hemodynamic and cardiac autonomic nervous system responses when added during induction of anesthesia.13,21 Nishiyama and colleagues21 compared a combination of midazolam 0.1 mg/kg followed by 3 mg/kg thiopental sodium with thiopental 5 mg/kg. In both groups, blood pressure and HR increased in response to tracheal intubation, but the increase was significantly lower in the combined group. Regarding heart rate variability, the midazolam-thiopental group showed significantly lower values of increase of low-frequency component/high-frequency component ratio. In another prospective randomized study, midazolam-propofol combination yielded compensated modulatory effects on the cardiovascular system, which were related to significant increases in the LF/HF ratio after induction, and 1, 3, and 5 min after intubation.13
Gabapentin-midazolam combination may exert a synergistic effect on the hemodynamic response to endotracheal intubation as a result of their different mechanisms of action of the two drugs. Like other benzodiazepines, midazolam effects are mediated by its action on the ionotropic GABAA receptors in the central nervous system (CNS) with rapid onset of action and few adverse effects.22 On the other hand, gabapentin exerts little action on GABA receptors despite being developedinitially as a mimetic of this inhibitory neurotransmitter. It has a high affinity to the α2-δ1 subunit of voltage-gated calcium channels located in the CNS.23 Therefore, it acts in a way similar to calcium channel blockers.
CONCLUSION
Based on the results of our study, we conclude that oral gabapentin is effective in attenuation of the hypertensive response to laryngoscopy and endotracheal intubation when administered in a dose of 900 mg 90 min before modified radical mastectomy. However, it is more effective when combined with oral midazolam 7.5 mg.
Financial support: None to declare
Conflicts of Interest: None to declare
Authors’ contribution:
AB: Concept, literature search, conduction of the study work, and manuscript
editing
NA: Conduction of the study work, data analysis, and manuscript editing
REFERENCES
- Doleman B, Sherwin M, Lund JN, Williams JP. Gabapentin for the hemodynamic response to intubation: systematic review and meta-analysis. Can J Anaesth. 2016 Sep;63(9):1042–58 [PubMed]
- Kumar A, Seth A, Prakash S, Deganwa M, Gogia AR. Attenuation of the hemodynamic response to laryngoscopy and tracheal intubation with fentanyl, lignocaine nebulization, and a combination of both: A randomized controlled trial. Anesth Essays Res. 2016 Sep-Dec;10(3):661–6.[PubMed]
- Mendonça FT, de Queiroz LM da GM, Guimarães CCR, Xavier ACD. Effects of lidocaine and magnesium sulfate in attenuating hemodynamic response to tracheal intubation: single-center, prospective, double-blind, randomized study. Rev Bras Anesthesiol. 2017 Jan-Feb;67(1):50–6 [PubMed] [Free Full Text]
- Maruta T, Kodama Y, Tanaka I, Shirasaka T, Tsuneyoshi I. Comparison of the effect of continuous intravenous infusion and two bolus injections of remifentanil on haemodynamic responses during anaesthesia induction: a prospective randomisedsingle-centre study. BMC Anesthesiol. 2016 Nov 14;16(1):110 [PubMed][Free Full Text]
- Singhal SK, Malhotra N, Kaur K, Dhaiya D. Efficacy of esmolol administration at different time intervals in attenuating hemodynamic response to tracheal intubation. Indian J Med Sci. 2010 Oct;64(10):468–75 [PubMed]
- Nishikawa T, Namiki A. Attenuation of the pressor response to laryngoscopy and tracheal intubation with intravenous verapamil. Acta Anaesthesiol Scand. 1989 Apr;33(3):232–5 [PubMed]
- Turan A, Kaya G, Karamanlioglu B, Pamukçu Z, Apfel CC. Effect of oral gabapentin on postoperative epidural analgesia. Br J Anaesth. 2006 Feb;96(2):242–6 [PubMed] [Free Full Text]
- Kinney MAO, Mantilla CB, Carns PE, Passe MA, Brown MJ, Hooten WM, et al. Preoperative gabapentin for acute post-thoracotomy analgesia: a randomized, double-blinded, active placebo-controlled study. Pain Pract. 2012 Mar;12(3):175–83 [PubMed][Free Full Text]
- Marashi SM, Ghafari MH, Saliminia A. Attenuation of hemodynamic responses following laryngoscopy and tracheal intubation -- comparative assessment of clonidine and gabapentin premedication. Middle East J Anaesthesiol. 2009 Jun;20(2):233–7 [PubMed]
- Memiş D, Turan A, Karamanlioğlu B, Seker S, Türe M. Gabapentin reduces cardiovascular responses to laryngoscopy and tracheal intubation. Eur J Anaesthesiol. 2006 Aug;23(8):686–90 [PubMed]
- Bafna U, Goyal VK, Garg A. A Comparison of Different Doses of Gabapentin to Attenuate the Haemodynamic Response to Laryngoscopy and Tracheal Intubation in Normotensive Patients. J Anaesthesiol Clin Pharmacol. 2011 Jan-Mar;27(1):43–6 [PubMed]
- Fassoulaki A, Melemeni A, Paraskeva A, Petropoulos G. Gabapentin attenuates the pressor response to direct laryngoscopy and tracheal intubation. Br J Anaesth. 2006 Jun;96(6):769–73 [PubMed] [Free Full Text]
- Win NN, Kohase H, Yoshikawa F, Wakita R, Takahashi M, Kondo N, et al. Haemodynamic changes and heart rate variability during midazolam-propofol co-induction. Anaesthesia. 2007 Jun;62(6):561–8 [PubMed] [Free Full Text]
- Koç S, Memis D, Sut N. The preoperative use of gabapentin, dexamethasone, and their combination in varicocele surgery: a randomized controlled trial. Anesth Analg. 2007 Oct;105(4):1137–42 [PubMed]
- Gemperle M, Kapp W. Midazolam and anaesthesia. Br J Clin Pharmacol 1983;16 suppl 1:187S-90S [PubMed][Free Full Text]
- Bauer KP, Dom PM, Ramirez AM, O’Flaherty JE. Preoperative intravenous midazolam: benefits beyond anxiolysis. J Clin Anesth. 2004 May;16(3):177–83 [PubMed]
- Sawaguchi K, Matsuura N, Ichinohe T. Comparison of the Effect of Electrical Stimulations on the Chin Skin on Autonomic Nervous Activities During Propofol Sedation With or Without Midazolam. J Oral Maxillofac Surg. 2016 Sep;74(9):1751.e1-6 [PubMed]
- Tsugayasu R, Handa T, Kaneko Y, Ichinohe T. Midazolam more effectively suppresses sympathetic activations and reduces stress feelings during mental arithmetic task than propofol. J Oral Maxillofac Surg. 2010 Mar;68(3):590–6 [PubMed]
- Short TG, Chui PT. Propofol and midazolam act synergistically in combination. Br J Anaesth. 1991 Nov;67(5):539–45 [PubMed] [Free Full Text]
- Wilder-Smith OH, Ravussin PA, Decosterd LA, Despland PA, Bissonnette B. Midazolam premedication reduces propofol dose requirements for multiple anesthetic endpoints. Can J Anaesth. 2001 May;48(5):439–45 [PubMed][Free Full Text]
- Nishiyama T, Misawa K, Yokoyama T, Hanaoka K. Effects of combining midazolam and barbiturate on the response to tracheal intubation: changes in autonomic nervous system. J Clin Anesth 2002;14:344–8 [PubMed]
- Conway A, Rolley J, Sutherland JR. Midazolam for sedation before procedures. Cochrane Database Syst Rev 2016;CD009491 [PubMed] [Free Full Text]
- Taylor CP. Mechanisms of analgesia by gabapentin and pregabalin--calcium channel alpha2-delta [Cavalpha2-delta] ligands. Pain 2009 Mar;142(1-2):13–6 [PubMed]Table 1: Baseline characteristic of the two studied groups
| Group G
(n=30) |
Group GM
(n=30) |
p value | |
| Age (years) | 47.0 ± 6.1 | 49.0 ± 6.2 | 0.213 |
| Sex (male/female) | 21/9 | 19/11 | 0.584 |
| Weight (kg) | 65.0 ± 6.3 | 63.2 ± 6.8 | 0.291 |
| Body mass index (kg/m2) | 30.8 ± 2.7 | 29.5 ± 3.5 | 0.113 |
| ASA Class (I/II) | 20/10 | 18/12 | 0.592 |
| Duration of Laryngoscopy (sec.) | 10.7 ± 2.2 | 10.0 ± 1.4 | 0.142 |
| Duration of surgery (min) | 100.0 ± 9.1 | 103.0 ± 6.6 | 0.093 |
| Baseline Hemodynamics | |||
| SBP (mmHg) | 124 ± 4 | 125 ± 4 | 0.234 |
| DBP (mmHg) | 77 ± 4 | 78 ± 3 | 0.675 |
| Heart Rate (beats/min) | 84 ± 3 | 82 ± 4 | 0.019 |
Data are presented as mean ± SD or number (%)
Table 2: Systolic blood pressure rate at baseline, before and after induction of anesthesia and after endotracheal intubation in the two studied groups
| Systolic blood pressure (mmHg) | Group G
(n=30) |
Group GM
(n=30) |
p-value |
| Baseline | 124 ± 8 | 125 ± 5 | 0.564 |
| Before induction | 118 ± 6 | 116 ± 6 | 0.202 |
| After induction | 120 ± 11 | 118 ± 9 | 0.444 |
| 1 min after intubation | 129 ± 8 | 124 ± 7 | 0.013 |
| 3 min after intubation | 126 ± 7 | 120 ± 9 | 0.006 |
| 5 min after intubation | 118 ± 9 | 112 ± 4 | 0.002 |
| 10 min after intubation | 116 ± 6 | 112 ± 6 | 0.012 |
| 15 min after intubation | 118 ± 9 | 115 ± 5 | 0.116 |
| 30 min after intubation | 120 ± 11 | 118 ± 7 | 0.404 |
Table 3: Diastolic blood pressure rate at baseline, before and after induction of anesthesia and after endotracheal intubation in the two studied groups
| Diastolic blood pressure (mmHg) | Group G
(n=30) |
Group GM
(n=30) |
p-value |
| Baseline | 84 ± 8 | 82 ± 7 | 0.307 |
| Before induction | 78 ± 5 | 76 ± 7 | 0.208 |
| After induction | 72 ± 9 | 70 ± 8 | 0.367 |
| 1 min after intubation | 83 ± 6 | 78 ± 6 | 0.002 |
| 3 min after intubation | 82 ± 9 | 76 ± 10 | 0.018 |
| 5 min after intubation | 80 ± 8 | 76 ± 5 | 0.024 |
| 10 min after intubation | 75 ± 6 | 72 ± 6 | 0.058 |
| 15 min after intubation | 74 ± 7 | 70 ± 9 | 0.060 |
| 30 min after intubation | 73 ± 5 | 70 ± 10 | 0.147 |
Table 4: Heart rate at baseline, before and after induction of anesthesia and after endotracheal intubation in the two studied groups
| Heart Rate (beats/min) | Group G
(n=30) |
Group GM
(n=30) |
p-value |
| Baseline | 84 ± 9 | 85 ± 8 | 0.651 |
| Before induction | 82 ± 10 | 84 ± 8 | 0.093 |
| After induction | 80 ± 8 | 82 ± 6 | 0.586 |
| 1 min after intubation | 85 ± 8 | 87 ± 7 | 0.608 |
| 3 min after intubation | 82 ± 9 | 83 ± 9 | 0.669 |
| 5 min after intubation | 82 ± 11 | 84 ± 8 | 0.424 |
| 10 min after intubation | 81 ± 8 | 82 ± 9 | 0.651 |
| 15 min after intubation | 80 ± 7 | 82 ± 8 | 0.307 |
| 30 min after intubation | 79 ± 6 | 80 ± 7 | 0.555 |