1,3Department of Anesthesiology, Vinayaka Missions Medical College, Karaikal, Puducherry (India)
2Department of Anesthesiology, Indira Gandhi Medical College & Research Centre, Puducherry (India)
Correspondence: Dr Prasanna Vadhanan, MD, Department of Anesthesiology, Vinayaka Missions Medical College, Karaikal, Puducherry 609609 (India); E-mail: vadhanan.prasanna@gmail.com
ABSTRACT
Introduction:
Endotracheal intubation is one of the fundamental skills that should be mastered by the anesthesiologist. One of the important causes of anesthesia related mortality and morbidity is airway related events. Several video laryngoscopes are available in the market to facilitate intubation both in and out of the hospital scenarios. These devices are precluded by their cost and availability especially in developing countries.
In this pilot study we have evaluated a custom made low-cost straight blade video laryngoscope (v-scope) which can be attached to a smartphone, compared to a conventional Miller blade with regards to time taken for intubation, when performed by trainee anesthesiologists. Ours is the first low cost laryngoscope that is based on a straight blade design.
Methodology: Forty adult patients posted for elective surgeries under general anesthesia were randomized into groups of twenty each. Patients of the first group were intubated with the aid of a Millers blade and bougie using a paraglossal technique. The other group was intubated with a low-cost video laryngoscope (v-scope) under similar conditions. All intubations were performed by trainee anesthesiologists. The primary objective was the time taken for intubation. The time taken for visualization of glottis (t1), further time taken for successful passing of endotracheal intubation (t2) were also noted. The ease of intubation, use of additional maneuvers, hemodynamic response and any adverse events were also noted.
Results: The time taken for intubation was similar in both groups (77.25 ± 26.46 vs 74.15 ± 26.3 sec, mean ± SD). The glottis view was better and need for external laryngeal manipulation was lesser with the v-scope. The time taken from visualization of the glottis to intubation was prolonged in the v-scope group (21.1 ± 6.1 sec vs 14.7 ± 3.6 sec, p< 0.001). No significant adverse events were observed
Conclusion: The low-cost video laryngoscope is a useful device in the hands of trainees that can improve the glottic views and achieve similar intubation times as compared to Miller’s blade, similar to other video laryngoscopes.
Key words: Videolaryngoscope; Smart phone: Miller Blade: Intubation
Citation: Vadhanan P, Balakrishnan K, TripatyDK. Evaluation of a low-cost videolaryngoscope – a randomized controlled pilot study. Anaesth Pain & Intensive Care 2017;21(4):406-412
Received: 9 October 2017; Reviewed: 20 October 2017; Corrected: 12 November 2017; Accepted: 22 November 2017
INTRODUCTION
Airway related events are a common cause of anesthesia related mortality and morbidity. One of the basic skills to be learned during anesthesia residency is the ability to perform an endotracheal intubation with different type of laryngoscopes.
A key step in endotracheal intubation is the alignment of the oral, pharyngeal and laryngeal axes. More recently a 2-curve concept has been proposed, involving a primary (oro-pharyngeal curve) and a secondary (pharyngo-glotto-tracheal) curve.1 The need to align the visual axis to these axes is a common reason for poor visualization of the glottis and difficulty encountered during endotracheal intubations. Videolaryngoscopes (VLS) overcome this problem by allowing the viewer to see the glottis through a camera attached to a curved blade. VLSs can be classified as those with a Macintosh blade, angulated blade and one with a channel for tube passage.2 The average cost of a single use VLS can be up to 8000 INR and require batteries and special care. The prohibitive cost precludes their routine use in developing countries. We have designed a low-cost VLS (“v-scope”) based on a straight Miller blade, and compared it to a conventional Miller blade.
The v-scope
Borescope is an instrument used to see through a small hole. Universal Serial Bus (USB) borescopes are commonly used to inspect drainages and inside automobile engines. They are rugged and waterproof. They are illuminated by circumferentially arranged LED bulbs and has a pinhole camera in the middle, and work on trickle power from USB ports of a laptop, computer or, as in this case a smartphone. We attached an USB borescope to a Millers blade by waterproof tapes and connected it to a smartphone (Android OS 4.1 and higher) via an USB-OTG (On the go) cable. The smartphone provides the power supply and processes the image (Figure 1). The resultant image can be viewed in any smartphone by using a variety of free video capture applications available. Recording of still images and video clips is also possible. This makes the device handy and can be used in any emergency easily besides being a useful teaching tool. The auto-detect feature of smartphones allows the image to appear as soon as the USB device is connected, thus requiring minimal time to set up. As the device is waterproof they can be easily sterilized by soap water and glutaraldehyde. The existing bulb of the Millers blade is also kept functional, thereby achieving high degree of illumination and minimal heat generation. The author had uploaded a video demonstrating the use of the v-scope as early as March 2015.3 A similar scope but using a Macintosh blade was later reported by Karippacheril et al4 in February 2016.
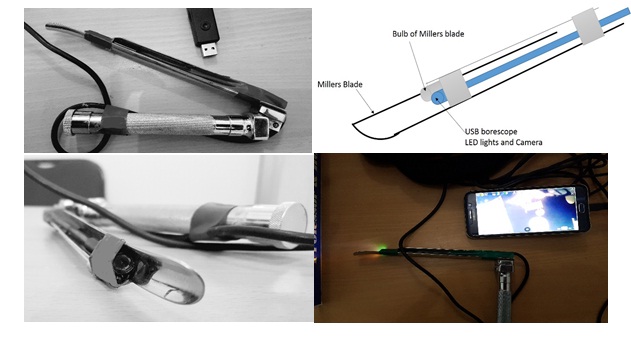
Figures 1: Custom made VLS
METHODOLOGY
The study was conducted in a teaching hospital in southern India over a period of three months from February through April 2016. Forty adult patients of both sexes were recruited for this randomized controlled study after obtaining ethical clearance and informed consent. Inclusion criteria were American Society of Anesthesiologists physical status (ASA) I and II patients posted for elective surgeries under general anesthesia and patients with modified Mallampati scores of 1, 2 and 3.
Patients with risk of aspiration, irregular dentition, oropharyngeal pathology, ASA III and IV, restricted mouth opening or neck movement, Cervical spine instability, Modified Mallampati score of 4, Body mass index (BMI) more than 35 Kg/m2 , neck circumference more than 41cm (male) 39cm (female) and history of difficult airway or sleep apnea were excluded. Suitable patients were randomized into two groups of twenty each by computer generated randomization numbers via sealed opaque envelopes. All patients were premedicated with injection glycopyrrolate 0.2mg intravenously before shifting inside operation room.
Patients were positioned in the sniffing position and preoxygenated. Standard monitors –pulse oximetry, non-invasive blood pressure, 3 lead ECG, end tidal carbon dioxide (EtCO2) and neuromuscular monitor (Inmed, Vadodara) were used. All patients were induced with inj. fentanyl, inj. propofol and inj. vecuronium at appropriate doses. Mask ventilation was confirmed before administering muscle relaxant. After achieving a train-of-four response of zero, intubation was attempted either with a Miller blade (Group 1) through paraglossal approach or the low cost- VLS (v-scope). The time taken for visualization of glottis (t1) was noted. A bougie was used in all cases to aid intubation and glottis view was graded by Cormack-Lehane (CL) score. External laryngeal manipulation was done if necessary. The time taken from visualization of glottis till appearance of EtCO2 (t2) was noted. The time to intubation (time between Introduction of the laryngoscope and appearance of an EtCO2 tracing, t1+t2) and hemodynamic parameters (heart rate and mean arterial pressure) immediately after intubation were noted.
All intubations were performed by two 1st year post graduates alternatively. If there was any difficulty in glottis visualization beyond 120 sec, mask ventilation was resumed and procedure was taken over by the consultant anesthesiologist. The operator was asked to grade the difficulty of intubation on a subjective scale (mild, moderate and severe). Postoperatively the incidences of complications like trauma, sore throat, hoarseness were noted.
Statistical analysis was performed using Microsoft Excel 2016 with real statistics add-on package and IBM SPSS version 23.
Regarding the primary outcome (time taken for intubation), Student’s Unpaired t test was used to calculate the statistical significance after verifying normal distribution by Shapiro-Wilk test and by analyzing Skewness and Kurtosis (0.05,0.63 and -1.46,0.005 respectively). Categorical data were compared with Chi-squared test and Fisher’s Exact test for smaller values (values less than 5) in the contingency tables. Alpha error of 5% was used and a p value of less than 0.05 was considered significant.
RESULTS
Both the groups were similar in terms of age, sex, Mallampati scoring, neck circumference and BMI (Table 1).
Table 1: Demography and Cormack-Lehane grades
The hemodynamic parameters were comparable between both groups at baseline and after intubation (Table 2, Figures 2-5).
Table 2: Heart rate and mean arterial pressures
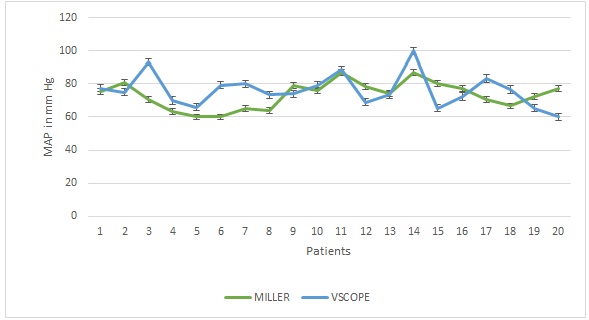
Figure 2: Baseline mean arterial pressures (MAP) in mm Hg. Vertical bars indicate standard error
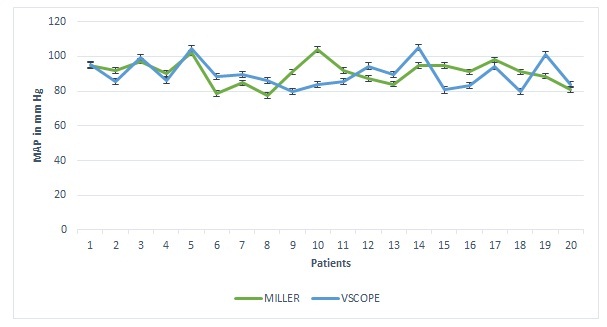
Figure 3: Post intubation mean arterial pressures, vertical bars indicate standard error
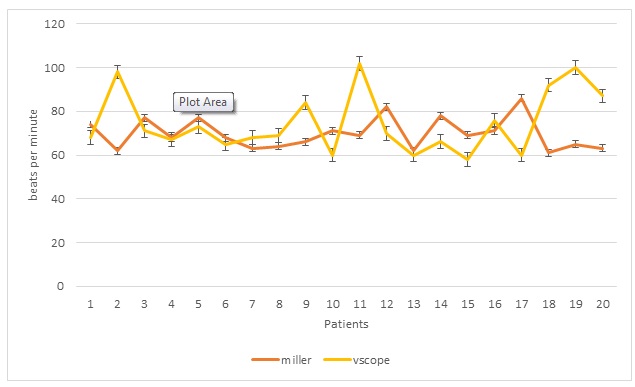
Figure 4: Baseline heart rates, vertical bars indicate standard error
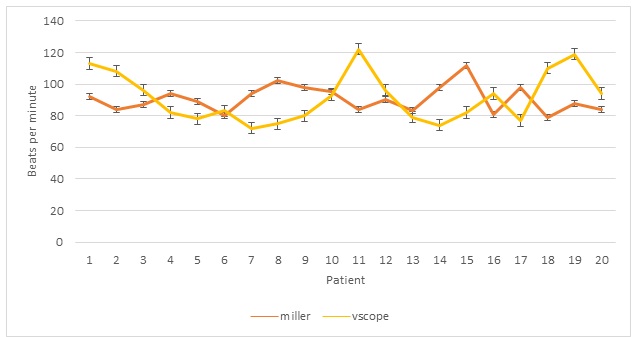
Figure 5: Post intubation heart rates, vertical bars indicate standard error
The mean intubation time was more with v-scope group as compared to the Miller group, (77.25 ± 26.46 vs 74.15 ± 26.3 sec, mean ± SD respectively), but the difference was not statistically significant (p = 0.71). The time for glottis visualization was comparable in both groups (62.2 ± 25.1 and 53.1 ± 24.2 secs, p = 0.22). The time taken from visualization of glottis to appearance of EtCO2 tracing (t2) was more in v-scope group (21.1 ± 6.1 sec) than in Miller group (14.7 ± 3.6 sec, p < 0.001) (Table 3).
Table 3: Glottis visualization time, Intubation time and total times
Regarding the CL grading of laryngoscopic view, 16 patients in v-scope group had a grade 1 view as opposed to 7 patients in Miller group. CL grade 2 was obtained in 9 patients Miller and 3 patients in v-scope group. The difference in distribution was statistically significant. (Chi squared, p = 0.015). External laryngeal manipulation was needed in 10 patients in Miller group and in only 3 patients in v-scope group. The difference was significant (p=0.04, Fisher’s Exact test).
All intubations were successful in the first attempt and none of the patients had significant desaturation, trauma or any other complications. 16/20 intubations in Miller and 14/20 intubations in v-scope group were deemed ‘moderately’ difficult and the remaining (4/20 in Miller and 6/20 in v-scope) were deemed ‘minimally difficult’ by the trainees.
DISCUSSION
The incidences of difficult and failed intubations are 1.8 – 5.8% and 0.13 -0.3% respectively. VLSs like Glidescope have been shown to improve glottis visualization, but the time taken to intubate was prolonged.5 First attempt intubations were more successful by non-expert operators with Glidescope. Griesdale et al noted that the time taken to intubation was shorter by non-experts with Glidescope, a similar effect was not observed with experts. However, there was a substantial heterogeneity for these outcomes.6
In a study comparing Glidescope, C Trach and direct laryngoscopy in morbidly obese patients, time to intubation was faster with Glidescope than C Trach (34 s more) and direct laryngoscopy (14 sec more). 43% and 27% patients required optimization maneuvers as compared to 0% in Glidescope group.7 On the other hand, a study comparing McGrath and C-MAC in potential difficult airways showed mean intubation times shorter with C-MAC than McGrath (50s vs 67s) despite McGrath scope achieving better glottis visualization, number of attempts to intubation was also lesser with C-Mac.8
Most of the VLSs have a curved design to resemble the Macintosh blade. Pediatric straight blade VLSs are available from C-Mac. A straight blade like Miller is very handy in certain conditions like limited mouth opening and a large tongue. The paraglossal approach is useful in cases with large tongue as it improves the view by reducing tongue impression and minimizing the risk of backward displacement of tongue and epiglottis.9
In our study, the total time taken for intubation was similar in both groups - 77.25 ± 26.46 and 74.15 ± 26.31 sec in Millers and v-scope group respectively (Mean ± SD). The difference was not statistically significant (p =0.71). One of the major limitations of VLSs is the difficulty in guiding the endotracheal tube through the glottis despite a better visualization of the glottis. We measured the glottis visualization time (t1, time taken from removal of mask to visualization of the glottis) and ETT time (t2, time from glottis visualization to appearance of an EtCO2 tracing) separately and calculated the total intubation time (t1+t2). The total intubation time and time to glottis visualization were comparable, but the time taken for introduction of endotracheal tube was significantly longer in the v-scope group. The total intubation time (time from introduction of the scope till appearance of EtCO2 tracing) was longer in this study as compared to other studies, where mean intubation times were in the range of 20-30secs.8, 10-12 Several factors might account for this apparent discrepancy. The operators were trainee anesthesiologists who had minimal experience with the paraglossal technique of straight blade introduction. Bougie was used in all patients, and passing the bougie and threading the ETT adds to the total time. Some studies calculate the time when laryngoscope was withdrawn as the end point, however we have used appearance of the EtCO2 tracing as the end point. All these factors might be responsible for the longer intubation times observed in both groups in our study. The author has successfully used the v-scope in several cases of anticipated difficult intubation and limited cervical spine mobility.
Even though the glottis visualization is better with VLSs, guiding the endotracheal tube may be difficult.13 A good glottis view need not translate into easier intubations.14 We have subdivided the intubation times into two, time taken for optimal glottis visualization and further time taken for successful intubation. We have used a flexible bougie in both groups. The time to glottis visualization (t1) was similar in both groups, and the glottis view as judged by the CL grading was better in v-scope group, but the time from glottis visualization to successfully placing the ETT was more in the v-scope group. Lack of depth perception, experience of the operator and fogging of the camera and processing speed of the system (smart phone) also affect intubation times.
The need for external manipulation to optimize the glottis view was more and statistically significant in the Millers group (10/20) when compared to v-scope group (4/20). External manipulation of the larynx would be more efficient with the VLS as the assistant also can view the glottis and perform the manipulation accordingly.
Our findings agree with the study by Liu et al, 2016 comparing McGrath and Macintosh blades by trainee anesthesiologists which showed superior CL grade and better ease of intubation with McGrath but with similar time taken for intubation and success rates.15 All intubations were successfully performed by the trainees and no adverse events were observed in our study.
STRENGTH AND LIMITATIONS
We have analyzed the feasibility of a low cost straight blade bases VLS- v-scope that can be used with a smartphone for the first time in this randomized controlled trial. A sub analysis of intubation times, time taken to view the glottis and time taken to confirm successful intubation has been done, which has shown that better glottis view may not mean easier and quicker intubations, with VLSs. The inclusion and exclusion criteria are robust, and we have considered neck circumference, body mass index apart from Mallampati scoring as predictors of difficult airway. VLSs are ideal teaching tools, and we have analyzed the intubation skills of trainee anesthesiologists in our study.
The major limitation of this study is that blinding cannot be achieved in this design. Also, being a pilot trial, the sample size is small. Using the time to intubation and standard deviation from previous studies, to detect a minimum of 10 sec difference in mean intubation times with an alpha error of 0.05 and power of 80% a sample size of 110 would be needed. The preliminary results from the study warrants larger trials before attempting clinical interpretations. The Percentage of glottis opening (POGO) score has been used in several studies to assess the efficacy of VLSs. This is also a validated tool with high inter observer and intra observer reliability. We have measured the CL grading because the operators were more familiar with it.
CONCLUSION
In conclusion, an ordinary borescope can be used as an effective VLS which is cost effective, easy to assemble and use and can provide acceptable glottis views even in the hands of non-experts. The display can be obtained in any smart phone using Android operating system, hence the device is handy and does not need extra power source which might be advantageous in constrained locations. Large scale studies are needed to demonstrate its effectiveness in difficult airways and any short comings and/or complications associated with its use.
Conflict of interest: All expenses on this project were met solely by the authors
Authors’ contribution:
PV – Concept, study design, Statistics, Manuscript preparation
KB – Procedure, data collection
DKT – Literature review, manuscript revision
REFERENCES
2Department of Anesthesiology, Indira Gandhi Medical College & Research Centre, Puducherry (India)
Correspondence: Dr Prasanna Vadhanan, MD, Department of Anesthesiology, Vinayaka Missions Medical College, Karaikal, Puducherry 609609 (India); E-mail: vadhanan.prasanna@gmail.com
ABSTRACT
Introduction:
Endotracheal intubation is one of the fundamental skills that should be mastered by the anesthesiologist. One of the important causes of anesthesia related mortality and morbidity is airway related events. Several video laryngoscopes are available in the market to facilitate intubation both in and out of the hospital scenarios. These devices are precluded by their cost and availability especially in developing countries.
In this pilot study we have evaluated a custom made low-cost straight blade video laryngoscope (v-scope) which can be attached to a smartphone, compared to a conventional Miller blade with regards to time taken for intubation, when performed by trainee anesthesiologists. Ours is the first low cost laryngoscope that is based on a straight blade design.
Methodology: Forty adult patients posted for elective surgeries under general anesthesia were randomized into groups of twenty each. Patients of the first group were intubated with the aid of a Millers blade and bougie using a paraglossal technique. The other group was intubated with a low-cost video laryngoscope (v-scope) under similar conditions. All intubations were performed by trainee anesthesiologists. The primary objective was the time taken for intubation. The time taken for visualization of glottis (t1), further time taken for successful passing of endotracheal intubation (t2) were also noted. The ease of intubation, use of additional maneuvers, hemodynamic response and any adverse events were also noted.
Results: The time taken for intubation was similar in both groups (77.25 ± 26.46 vs 74.15 ± 26.3 sec, mean ± SD). The glottis view was better and need for external laryngeal manipulation was lesser with the v-scope. The time taken from visualization of the glottis to intubation was prolonged in the v-scope group (21.1 ± 6.1 sec vs 14.7 ± 3.6 sec, p< 0.001). No significant adverse events were observed
Conclusion: The low-cost video laryngoscope is a useful device in the hands of trainees that can improve the glottic views and achieve similar intubation times as compared to Miller’s blade, similar to other video laryngoscopes.
Key words: Videolaryngoscope; Smart phone: Miller Blade: Intubation
Citation: Vadhanan P, Balakrishnan K, TripatyDK. Evaluation of a low-cost videolaryngoscope – a randomized controlled pilot study. Anaesth Pain & Intensive Care 2017;21(4):406-412
Received: 9 October 2017; Reviewed: 20 October 2017; Corrected: 12 November 2017; Accepted: 22 November 2017
INTRODUCTION
Airway related events are a common cause of anesthesia related mortality and morbidity. One of the basic skills to be learned during anesthesia residency is the ability to perform an endotracheal intubation with different type of laryngoscopes.
A key step in endotracheal intubation is the alignment of the oral, pharyngeal and laryngeal axes. More recently a 2-curve concept has been proposed, involving a primary (oro-pharyngeal curve) and a secondary (pharyngo-glotto-tracheal) curve.1 The need to align the visual axis to these axes is a common reason for poor visualization of the glottis and difficulty encountered during endotracheal intubations. Videolaryngoscopes (VLS) overcome this problem by allowing the viewer to see the glottis through a camera attached to a curved blade. VLSs can be classified as those with a Macintosh blade, angulated blade and one with a channel for tube passage.2 The average cost of a single use VLS can be up to 8000 INR and require batteries and special care. The prohibitive cost precludes their routine use in developing countries. We have designed a low-cost VLS (“v-scope”) based on a straight Miller blade, and compared it to a conventional Miller blade.
The v-scope
Borescope is an instrument used to see through a small hole. Universal Serial Bus (USB) borescopes are commonly used to inspect drainages and inside automobile engines. They are rugged and waterproof. They are illuminated by circumferentially arranged LED bulbs and has a pinhole camera in the middle, and work on trickle power from USB ports of a laptop, computer or, as in this case a smartphone. We attached an USB borescope to a Millers blade by waterproof tapes and connected it to a smartphone (Android OS 4.1 and higher) via an USB-OTG (On the go) cable. The smartphone provides the power supply and processes the image (Figure 1). The resultant image can be viewed in any smartphone by using a variety of free video capture applications available. Recording of still images and video clips is also possible. This makes the device handy and can be used in any emergency easily besides being a useful teaching tool. The auto-detect feature of smartphones allows the image to appear as soon as the USB device is connected, thus requiring minimal time to set up. As the device is waterproof they can be easily sterilized by soap water and glutaraldehyde. The existing bulb of the Millers blade is also kept functional, thereby achieving high degree of illumination and minimal heat generation. The author had uploaded a video demonstrating the use of the v-scope as early as March 2015.3 A similar scope but using a Macintosh blade was later reported by Karippacheril et al4 in February 2016.
Figures 1: Custom made VLS
METHODOLOGY
The study was conducted in a teaching hospital in southern India over a period of three months from February through April 2016. Forty adult patients of both sexes were recruited for this randomized controlled study after obtaining ethical clearance and informed consent. Inclusion criteria were American Society of Anesthesiologists physical status (ASA) I and II patients posted for elective surgeries under general anesthesia and patients with modified Mallampati scores of 1, 2 and 3.
Patients with risk of aspiration, irregular dentition, oropharyngeal pathology, ASA III and IV, restricted mouth opening or neck movement, Cervical spine instability, Modified Mallampati score of 4, Body mass index (BMI) more than 35 Kg/m2 , neck circumference more than 41cm (male) 39cm (female) and history of difficult airway or sleep apnea were excluded. Suitable patients were randomized into two groups of twenty each by computer generated randomization numbers via sealed opaque envelopes. All patients were premedicated with injection glycopyrrolate 0.2mg intravenously before shifting inside operation room.
Patients were positioned in the sniffing position and preoxygenated. Standard monitors –pulse oximetry, non-invasive blood pressure, 3 lead ECG, end tidal carbon dioxide (EtCO2) and neuromuscular monitor (Inmed, Vadodara) were used. All patients were induced with inj. fentanyl, inj. propofol and inj. vecuronium at appropriate doses. Mask ventilation was confirmed before administering muscle relaxant. After achieving a train-of-four response of zero, intubation was attempted either with a Miller blade (Group 1) through paraglossal approach or the low cost- VLS (v-scope). The time taken for visualization of glottis (t1) was noted. A bougie was used in all cases to aid intubation and glottis view was graded by Cormack-Lehane (CL) score. External laryngeal manipulation was done if necessary. The time taken from visualization of glottis till appearance of EtCO2 (t2) was noted. The time to intubation (time between Introduction of the laryngoscope and appearance of an EtCO2 tracing, t1+t2) and hemodynamic parameters (heart rate and mean arterial pressure) immediately after intubation were noted.
All intubations were performed by two 1st year post graduates alternatively. If there was any difficulty in glottis visualization beyond 120 sec, mask ventilation was resumed and procedure was taken over by the consultant anesthesiologist. The operator was asked to grade the difficulty of intubation on a subjective scale (mild, moderate and severe). Postoperatively the incidences of complications like trauma, sore throat, hoarseness were noted.
Statistical analysis was performed using Microsoft Excel 2016 with real statistics add-on package and IBM SPSS version 23.
Regarding the primary outcome (time taken for intubation), Student’s Unpaired t test was used to calculate the statistical significance after verifying normal distribution by Shapiro-Wilk test and by analyzing Skewness and Kurtosis (0.05,0.63 and -1.46,0.005 respectively). Categorical data were compared with Chi-squared test and Fisher’s Exact test for smaller values (values less than 5) in the contingency tables. Alpha error of 5% was used and a p value of less than 0.05 was considered significant.
RESULTS
Both the groups were similar in terms of age, sex, Mallampati scoring, neck circumference and BMI (Table 1).
Table 1: Demography and Cormack-Lehane grades
| Parameter | Miller
(n=20) |
v-scope
(n=20) |
p value | |
| Age (years, mean ± SD) | 41.25 ± 12.8 | 40.5 ± 13.4 | 0.85 | |
| Sex (Male: female) | 12:8 | 13:7 | 0.74 | |
| MMP Grade (1,2,3) | 5, 13, 2 | 1, 15, 4 | 0.17 | |
| Neck Circumference (cm, mean ± SD) | 34.2 ± 1.6 | 33.3 ± 2.5 | 0.22 | |
| CL grade (1,2,3) | 7, 9, 4 | 16, 3, 1 | 0.015 | |
The hemodynamic parameters were comparable between both groups at baseline and after intubation (Table 2, Figures 2-5).
Table 2: Heart rate and mean arterial pressures
| Parameter
( Mean ± SD ) |
Miller
(n=20) |
v-scope
(n=20) |
p value |
| Baseline heart rate (beats/minute) | 69.5 ± 1.67 | 74.8 ± 2.92 | 0.14 |
| Baseline MAP (mm Hg) | 73.2 ± 1.89 | 76.01 ± 2.3 | 0.31 |
| Post intubation HR (beats/minute) | 90.6 ± 1.82 | 91.9 ± 2.9 | 0.68 |
| Post intubation MAP mmHg | 90.4 ± 1.6 | 89.7 ± 1.97 | 0.71 |
Figure 2: Baseline mean arterial pressures (MAP) in mm Hg. Vertical bars indicate standard error
Figure 3: Post intubation mean arterial pressures, vertical bars indicate standard error
Figure 4: Baseline heart rates, vertical bars indicate standard error
Figure 5: Post intubation heart rates, vertical bars indicate standard error
The mean intubation time was more with v-scope group as compared to the Miller group, (77.25 ± 26.46 vs 74.15 ± 26.3 sec, mean ± SD respectively), but the difference was not statistically significant (p = 0.71). The time for glottis visualization was comparable in both groups (62.2 ± 25.1 and 53.1 ± 24.2 secs, p = 0.22). The time taken from visualization of glottis to appearance of EtCO2 tracing (t2) was more in v-scope group (21.1 ± 6.1 sec) than in Miller group (14.7 ± 3.6 sec, p < 0.001) (Table 3).
Table 3: Glottis visualization time, Intubation time and total times
| Time in sec
(Mean ± SD) |
Miller | v-scope | p value (Unpaired t) |
| Time to glottis | 62.2 ± 25.1 | 53.1 ± 24.2 | 0.25 |
| Glottis to EtCO2 | 14.7 ± 3.6 | 21.1 ± 6.1 | < 0.001* |
| Total intubation time | 77.25 ± 26.46 | 74.15 ± 26.31 | 0.712 |
All intubations were successful in the first attempt and none of the patients had significant desaturation, trauma or any other complications. 16/20 intubations in Miller and 14/20 intubations in v-scope group were deemed ‘moderately’ difficult and the remaining (4/20 in Miller and 6/20 in v-scope) were deemed ‘minimally difficult’ by the trainees.
DISCUSSION
The incidences of difficult and failed intubations are 1.8 – 5.8% and 0.13 -0.3% respectively. VLSs like Glidescope have been shown to improve glottis visualization, but the time taken to intubate was prolonged.5 First attempt intubations were more successful by non-expert operators with Glidescope. Griesdale et al noted that the time taken to intubation was shorter by non-experts with Glidescope, a similar effect was not observed with experts. However, there was a substantial heterogeneity for these outcomes.6
In a study comparing Glidescope, C Trach and direct laryngoscopy in morbidly obese patients, time to intubation was faster with Glidescope than C Trach (34 s more) and direct laryngoscopy (14 sec more). 43% and 27% patients required optimization maneuvers as compared to 0% in Glidescope group.7 On the other hand, a study comparing McGrath and C-MAC in potential difficult airways showed mean intubation times shorter with C-MAC than McGrath (50s vs 67s) despite McGrath scope achieving better glottis visualization, number of attempts to intubation was also lesser with C-Mac.8
Most of the VLSs have a curved design to resemble the Macintosh blade. Pediatric straight blade VLSs are available from C-Mac. A straight blade like Miller is very handy in certain conditions like limited mouth opening and a large tongue. The paraglossal approach is useful in cases with large tongue as it improves the view by reducing tongue impression and minimizing the risk of backward displacement of tongue and epiglottis.9
In our study, the total time taken for intubation was similar in both groups - 77.25 ± 26.46 and 74.15 ± 26.31 sec in Millers and v-scope group respectively (Mean ± SD). The difference was not statistically significant (p =0.71). One of the major limitations of VLSs is the difficulty in guiding the endotracheal tube through the glottis despite a better visualization of the glottis. We measured the glottis visualization time (t1, time taken from removal of mask to visualization of the glottis) and ETT time (t2, time from glottis visualization to appearance of an EtCO2 tracing) separately and calculated the total intubation time (t1+t2). The total intubation time and time to glottis visualization were comparable, but the time taken for introduction of endotracheal tube was significantly longer in the v-scope group. The total intubation time (time from introduction of the scope till appearance of EtCO2 tracing) was longer in this study as compared to other studies, where mean intubation times were in the range of 20-30secs.8, 10-12 Several factors might account for this apparent discrepancy. The operators were trainee anesthesiologists who had minimal experience with the paraglossal technique of straight blade introduction. Bougie was used in all patients, and passing the bougie and threading the ETT adds to the total time. Some studies calculate the time when laryngoscope was withdrawn as the end point, however we have used appearance of the EtCO2 tracing as the end point. All these factors might be responsible for the longer intubation times observed in both groups in our study. The author has successfully used the v-scope in several cases of anticipated difficult intubation and limited cervical spine mobility.
Even though the glottis visualization is better with VLSs, guiding the endotracheal tube may be difficult.13 A good glottis view need not translate into easier intubations.14 We have subdivided the intubation times into two, time taken for optimal glottis visualization and further time taken for successful intubation. We have used a flexible bougie in both groups. The time to glottis visualization (t1) was similar in both groups, and the glottis view as judged by the CL grading was better in v-scope group, but the time from glottis visualization to successfully placing the ETT was more in the v-scope group. Lack of depth perception, experience of the operator and fogging of the camera and processing speed of the system (smart phone) also affect intubation times.
The need for external manipulation to optimize the glottis view was more and statistically significant in the Millers group (10/20) when compared to v-scope group (4/20). External manipulation of the larynx would be more efficient with the VLS as the assistant also can view the glottis and perform the manipulation accordingly.
Our findings agree with the study by Liu et al, 2016 comparing McGrath and Macintosh blades by trainee anesthesiologists which showed superior CL grade and better ease of intubation with McGrath but with similar time taken for intubation and success rates.15 All intubations were successfully performed by the trainees and no adverse events were observed in our study.
STRENGTH AND LIMITATIONS
We have analyzed the feasibility of a low cost straight blade bases VLS- v-scope that can be used with a smartphone for the first time in this randomized controlled trial. A sub analysis of intubation times, time taken to view the glottis and time taken to confirm successful intubation has been done, which has shown that better glottis view may not mean easier and quicker intubations, with VLSs. The inclusion and exclusion criteria are robust, and we have considered neck circumference, body mass index apart from Mallampati scoring as predictors of difficult airway. VLSs are ideal teaching tools, and we have analyzed the intubation skills of trainee anesthesiologists in our study.
The major limitation of this study is that blinding cannot be achieved in this design. Also, being a pilot trial, the sample size is small. Using the time to intubation and standard deviation from previous studies, to detect a minimum of 10 sec difference in mean intubation times with an alpha error of 0.05 and power of 80% a sample size of 110 would be needed. The preliminary results from the study warrants larger trials before attempting clinical interpretations. The Percentage of glottis opening (POGO) score has been used in several studies to assess the efficacy of VLSs. This is also a validated tool with high inter observer and intra observer reliability. We have measured the CL grading because the operators were more familiar with it.
CONCLUSION
In conclusion, an ordinary borescope can be used as an effective VLS which is cost effective, easy to assemble and use and can provide acceptable glottis views even in the hands of non-experts. The display can be obtained in any smart phone using Android operating system, hence the device is handy and does not need extra power source which might be advantageous in constrained locations. Large scale studies are needed to demonstrate its effectiveness in difficult airways and any short comings and/or complications associated with its use.
Conflict of interest: All expenses on this project were met solely by the authors
Authors’ contribution:
PV – Concept, study design, Statistics, Manuscript preparation
KB – Procedure, data collection
DKT – Literature review, manuscript revision
REFERENCES
- Greenland KB, Edwards MJ, Hutton NJ, Challis VJ, Irwin MG, Sleigh JW. Changes in airway configuration with different head and neck positions using magnetic resonance imaging of normal airways: a new concept with possible clinical applications. Br J Anaesth. 2010 Nov;105(5):683-690. [PubMed] [Free full text]
- Niforopoulou P, Pantazopoulos I, Demestiha T, Koudouna E, Xanthos T. Video-laryngoscopes in the adult airway management: A topical review of the literature. Acta Anaesthesiol Scand. 2010 Oct;54(9):1050–61. [PubMed]
- Prasana V. A Low cost video laryngoscope. [Online] 2015 Mar 19 [Cited 2016 Oct 1st]. Available from:https://youtu.be/NTTD9RwzarM.
- Karippacehril JG, Le Cong M. Videolaryngoscopy using an Android smartphone: A direct digital technique. Ind J Anaesth. 2016 Feb;60(2):143-145. [PubMed] [Free full text]
- Sun DA, Warriner CB, Parsons DG, Klein R, Umedaly HS, Moult M. The GlideScope Video Laryngoscope: randomized clinical trial in 200 patients Br J Anaesth. 2005 Mar;94(3):381-4. [PubMed] [Free full text]
- Griesdale D, Liu D, McKinney J, Choi PT. Glidescope video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis . Can J Anesth. 2012 Jan;59(1):41–52. doi: 10.1007/s12630-011-9620-5 [PubMed] [Free full text]
- Yousef GT, Abdalgalil DA, Ibrahim TH. Orotracheal intubation of morbidly obese patients, comparison of GlideScope® video laryngoscope and the LMA C-TrachTM with direct laryngoscopy. Anesth Essays Res. 2012 Jul-Dec;6(2):174-179. doi:10.4103/0259-1162.108304. [PubMed] [Free full text]
- Ng I, Hill AL, Williams DL, Lee K, Segal R. Randomized controlled trial comparing the McGrath videolaryngoscope with the C-MAC videolaryngoscope in intubating adult patients with potential difficult airways. Br J Anaesth. 2012;109(3):439-443. doi: 10.1093/bja/aes145. [PubMed] [Free full text]
- Henderson JJ. The use of paraglossal straight blade laryngoscopy in difficult tracheal intubation. Anaesthesia. 1997 Jun;52(6):552-60. [PubMed] [Free full text]
- Szarpak L, Truszewski K, Czyzewski L, Gaszynski T, RodriguezNune A. A comparison of the McGrath-MAC and Macintosh laryngoscopes for child tracheal intubation during resuscitation by paramedics. A randomized, crossover, manikin study. Am J Emerg Med. 2016 Aug;34(8):1338-41. doi: 10.1016/j.ajem.2015.11.060 [PubMed]
- Sargin M, Uluer MS. Comparison of McGrath® Series 5 video laryngoscope with Macintosh laryngoscope: A prospective, randomised trial in patients with normal airways. Pak J Med Sci. 2016;32(4):869-874. doi:10.12669/pjms.324.10037. [PubMed] [Free full text]
- Ng I, Sim XL, Williams D, Segal R. A randomised controlled trial comparing the McGrath® videolaryngoscope with the straight blade laryngoscope when used in adult patients with potential difficult airways. 2011;66:709–714.doi: 10.1111/j.1365-2044.2011.06767. [PubMed] [Free full text]
- Healy DW, Picton P, Morris M, Turner C. Comparison of the glidescope, CMAC, storz DCI with the Macintosh laryngoscope during simulated difficult laryngoscopy: a manikin study. BMC Anesthesiol. 2012 Jun 21;12:11. [PubMed] [Free full text]
- Burdett E, Ross-Anderson DJ, Makepeace J, Bassett PA, Clark SG, Mitchel V. Randomized controlled trial of the A.P. Advance, McGrath, and Macintosh laryngoscopes in normal and difficult intubation scenarios: a manikin study. Br J Anaesth. 2011 Dec;107(6):983–988. doi: 10.1093/bja/aer295. [PubMed] [Free full text]