Muhammad Saleh Khaskheli1, Rafia Tabassum2, Aijaz Hussain Awan3
1Professor & Chairman, Cell: +92 300 321 1417, E-mail: beesaleh@hotmail.com
2Assistant Professor, +92 306 829 4346, E-mail: rafiatabassum2013@gmail.com
3Consultant Anesthesiologist, Cell: +92 302 322 6500, E-mail: draijazhussainawan@gmail.com
Department of Anesthesiology, SICU & Pain Management Center, Peoples University Of Medical & Health Sciences For Women, Shaheed Benazirabad, Sind, (Pakistan)
Correspondence: Professor Muhammad Saleh Khaskheli, Chairman, Department of Anaesthesiology, SICU & Pain Management Center, Peoples University of Medical & Health Sciences For Women, Shaheed Benazirabad, Sind (Pakistan); Cell: 03003211417; E-mail: beesaleh@hotmail.com
ABSTRACT
Objective: The recent interest in intravenous magnesium sulphate for using it in many other indications other than control of eclamptic fits lead the researchers to try it as a smooth muscle relaxant in cases of acute bronchial asthma. The results have largely been controversial, so we conducted this study to determine efficacy of intravenous magnesium sulphate in acute asthma based on its terminal outcome.
Methodology: This retrospective study was conducted at Surgical Intensive Care Unit at Peoples University of Medical and Health Sciences for Women, Nawabshah from January 2014-December 2015. We retrospectively reviewed the medical data sheets of all cases of acute asthma admitted during the study period, and extracted the relevant information. All the patients were initially treated with standard therapy for asthma and then given 4ml of 50% MgSO4 (2g) diluted in 250 ml of normal saline intravenously. Outcomes were presented in percentages and frequencies while patient age is presented as mean ± SD.
Results: The mean age of the population was 45.29 ± 20.1 y. We had a female predominance in our population (60.3%). Successfully cured patients were 32.3% whereas those expired were 57.4%. There was not a significant difference between the genders for the outcome (p > 0.05).
Conclusions: We found that intravenous magnesium sulphate is ineffective in successfully management of patients with acute asthma in terms of enhanced survival rate.
Keywords: Magnesium sulphate; Bronchial asthma; Efficacy; Emergency management.
Citation: Khaskheli MS, Tabassum R, Awan AH. Effectiveness of intravenous magnesium sulphate in acute asthma: a retrospective study. Anaesth Pain & Intensive Care 2017;21(4):458462
Received: 02 Feb 2017; Reviewed: 7 Feb & 21 Jul 2017; Corrected: 8 Feb, 31 Mar, 20 Jul 2017; Accepted: 12 Aug 2017
INTRODUCTION
Asthma is a chronic inflammatory disease of the lower airways characterized by respiratory symptoms and variable airway obstruction. Its clinical manifestations include recurrent symptoms, often involving shortness of breath, wheezing, coughing and chest tightness.1 In developed centuries, asthma is prevalent in 4-5% of the population and almost 27% of patients requiring admission.2 It is extremely prevalent with up to 1:10 adults worldwide.3
In addition to general treatment strategy, standard management of asthma include β2-agonists, inhaled anticholinergic agents, short-acting bronchodilators, and corticosteroids.4,5 For patients unresponsive to these initial therapies, magnesium sulfate (MgSO4) may be a treatment option.1,6 It has also been recommended as an adjunct in treating severe asthma with other mainline drugs.7,8 In patients who do not respond to initial treatments and those with severe, life-threatening acute exacerbations, current guidelines are suggestive of using MgSO4 as an adjunct therapy for reducing hospital stay and improving pulmonary functions, while the evidence for using nebulized magnesium is still inconclusive.4,7,9-11 Results have been mixed for several randomized controlled trials (RCTs) using intravenous MgSO4 in acute patients as some studies demonstrate its benefits,12-14 while others do not.2,15,16 Moreover, the studies reporting positive outcomes have shown a benefit predominantly in severe exacerbations as two recent reviews supported its use as an adjunct in severe asthma.2
Intravenous MgSO4 has a high safety profile17 with commonly reported minor side effects including dry mouth, flushing, malaise pain, and numbness at the site of infusion.1,18 Potential drug interactions include potassium-sparing diuretics and glucagon, which when used simultaneously, increase serum magnesium levels. If concomitant use of both drug groups have to be used, commonly reported problems need to be monitored or the later drug withheld temporarily if possible.1,19 Contraindications to the use of MgSO4 include myasthenia gravis, myocardial conditions, AV block and renal failure (creatinine clearance less than 30 ml/min).1,20
There has not been any study from Pakistan on this topic and there is scarce and conflicting data available on it particularly in Asia.9 Therefore, this study was conducted to investigate the efficacy of intravenous magnesium sulphate in acute asthma based on its outcomes.
METHODOLOGY
The study was approved by the institutional ethical committee. We conducted a retrospective review of all cases of acute severe asthma transferred to Surgical Intensive Care Unit at Peoples University of Medical and Health Sciences for Women, Nawabshah over a period of 2 years (January 2014-December 2015), and extracted the relevant information from the medical records. We excluded the poisoning cases, post-operative cases, post-trauma and patients on ventilatory support from the analysis. Variables under consideration were age and outcome (expired, cured, and referred). We, however, did not obtain any information on post-referral state of the patients. These patients were referred to hospitals with better treatment facilities on the request of their family or due to the orders of their treating physician.
Moreover, all the patients were initially managed at the Department of Medicine and then shifted to Surgical Intensive Care Unit. Before the current admission, most patients had a history of asthma and were received treatment with maintenance and/or rescue medications at home. In addition, patients received standard therapy (including nebulized salbutamol and ipratropium bromide, and systematic hydrocortisone) for an asthma exacerbation before receiving treatment with intravenous magnesium sulfate. All the patients were initially treated with standard therapy for asthma and then given intravenous magnesium sulphate i.e. received 4 ml of 50% MgSO4 (2 g) diluted in 250 ml of normal saline and given slowly over 20 min as per the recent recommendations.21 All the patients, after being stable were shifted to the Department of Medicine.
Statistical analysis: The data was recorded and kept on Microsoft Excel 2007 Spreadsheets. We extracted the relevant information and analyzed it on SPSS version 20. Gender and outcomes were presented in percentages and frequencies while age were presented as mean ± SD. Chi square test was used for comparing the outcome between the genders. The significance level was set at p < 0.05. RESULTS A total of 136 patients were enrolled in the study during the study period. There was a female predominance 82 (60.3%) as compared to males, which were 54 (39.7%). The mean age was 45.29 ± 20.1 y. The cured patients were 32.3% whereas those expired were 57.4%. Table 1 shows the demographic variables while Graph 1 shows outcomes based on the gender of the patients. There was not a significant difference between the genders for the outcome; cure rate for males was 25(18.38%) vs. 19(13.87%) (p > 0.05). A total of 78 (57.4%) patients expired despite the use of MgSO4.
Table 1: Demographic variables and outcomes
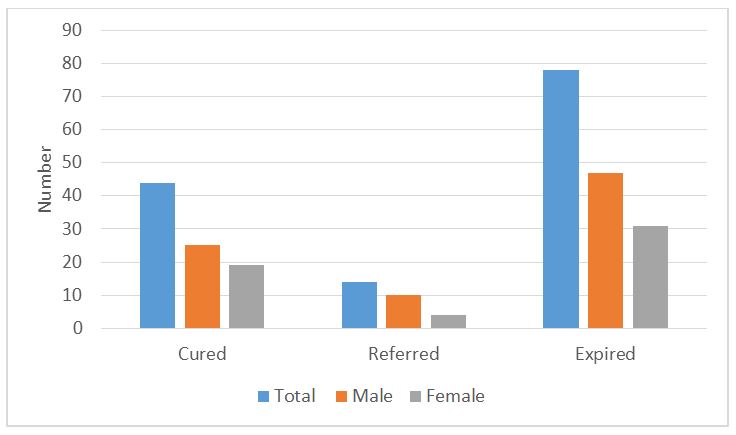
Graph 1: The outcome of the patients based upon gender
DISCUSSION
MgSO4 has been used as an adjunct in managing acute asthma but there is still lack of adequate evidence to support its effectiveness. Most of the studies have been conducted in the West and there is a high gap of research in the Asia-Pacific region.9 The role of MgSO4 in asthma is still unclear, but some studies have helped explain its mode of action. The possible effects of MgSO4 on smooth muscles may include activating sodium-calcium pumps and blocking the entry and release of calcium from the endoplasmic reticulum (ER) which consequently result in decrease in intracellular calcium.22,23 Moreover, MgSO4 inhibits acetylcholine release and depresses excitability of muscle fiber in cholinergic motor nerve terminals, ultimately generating bronchial smooth muscle relaxation.24 Furthermore, calcium and myosin interaction is inhibited by magnesium sulphate resulting into muscle cell relaxation. Magnesium also reduces inflammatory mediators by inhibiting mast cell degranulation and stabilizing T-cells.25 It may also increase the receptor affinity of β2-agonists thereby, increasing their bronchodilator effect.9,26 Lastly, it may directly reduce the severity of asthma by stimulating the synthesis of prostacyclin and nitric oxide.1
We found that 57.4% patients died even after the management of asthma with magnesium sulphate. However, the use of intravenous MgSO4 improved pulmonary function in adults but did not cause any reduction in the rate of hospitalization.27,28 Furthermore, a Cochrane review reported the effectiveness of MgSO4 in the treatment of acute asthma,29 whereas, the recent reviews by Mohammed et al. found that the efficacy of MgSO4 was only marginal on pulmonary function (SMD=0.25, 95% CI= 0.01-0.51).6 Moreover, the most recent review was unable to draw clear conclusions about effectiveness of MgSO4 in adults. However, it was suggested that intravenous MgSO4 seemed to be effective in children.30 This shows that there are mixed results and conclusions about the efficacy of magnesium sulphate in management of acute asthma. We tried a different strategy of finding efficacy of magnesium sulphate as compared to the previous studies; they most often were, randomized controlled trials; but we used an outcome-based retrospective review, concluding that magnesium sulphate was ineffective in asthma management.
Strengths and Limitations: This study is the first one from Pakistan on the role of magnesium sulphate in the management of asthma. However, it has its limitations. The study design for this study was retrospective in which charts of the patients were reviewed. Outcome measures were weak and duration of hospital stay, ventilator support, and post-referral status were not obtained and addressed. Nevertheless, this study expands the previous knowledge base on the use of intravenous magnesium sulphate in asthma management.
CONCLUSION
We found that intravenous magnesium sulphate is ineffective in managing patients with acute asthma. However, there is still need of some larger studies, primarily the randomized trials and prospective studies, to draw definite conclusions about the role of magnesium sulphate in the management of asthma.
Conflict of interest: None declared by the authors
Author contribution: MSK – Manuscript editing
RT – Statistical analysis
AHA – Literature search
REFERENCES
1. Bittar TMB, Guerra SD. Use of intravenous magnesium sulfate for the treatment of severe acute asthma in children in emergency department. Revista Brasileira de terapia intensiva. 2012;24(1):86-90. [Free full text]
2. Kumar SA, Shailendranath G, Raj K. A randomized controlled trial of intravenous magnesium sulphate as an adjunct to standard therapy in acute severe asthma. Iranian Journal of Allergy, Asthma and Immunology. 2008;7(4):221-9. [Free full text]
3. Annesi-Maesano I. Epidemiology of asthma in the world and in France. Rev Prat. 2011 Mar;61(3):329-35.[PubMed]
4. Shan Z, Rong Y, Yang W, Wang D, Yao P, Xie J, et al. Intravenous and nebulized magnesium sulfate for treating acute asthma in adults and children: a systematic review and meta-analysis. Respiratory Medicine. 2013;107(3):321-30. doi: 10.1016/j.rmed.2012.12.001.[PubMed] [Free full text]
5. Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, et al. Global strategy for asthma management and prevention: GINA executive summary. The European respiratory journal. 2008;31(1):143. doi: 10.1183/09031936.00138707. [PubMed] [Free full text]
6. Mohammed S, Goodacre S. Intravenous and nebulised magnesium sulphate for acute asthma: systematic review and meta-analysis. Emerg Med J. 2007 Dec;24(12):823-30. [PubMed] [Free full text]
7. Hossein S, Pegah A, Davood F, Said A, Babak M, Mani M, et al. The effect of nebulized magnesium sulfate in the treatment of moderate to severe asthma attacks: A randomized clinical trial. Am J Emerg Med. 2016 May;34(5):883-6. doi: 10.1016/j.ajem.2016.01.024. [PubMed]
8. Blitz M, Blitz S, Beasely R, Diner B, Hughes R, Knopp J, et al. Inhaled magnesium sulfate in the treatment of acute asthma. The Cochrane database of systematic reviews. 2005(2):CD003898. [PubMed]
9. Song WJ, Chang Y-S. Magnesium sulfate for acute asthma in adults: a systematic literature review. Asia Pacific Allergy. 2012;2(1):76. doi: 10.5415/apallergy.2012.2.1.76. [PubMed] [Free full text]
10. Hughes R, Goldkorn A, Masoli M, Weatherall M, Burgess C, Beasley R. Use of isotonic nebulised magnesium sulphate as an adjuvant to salbutamol in treatment of severe asthma in adults: randomised placebo-controlled trial. The Lancet. 2003;361(9375):2114-7. [PubMed] [Free full text]
11. Jones L, Goodacre S. Magnesium sulphate in the treatment of acute asthma: evaluation of current practice in adult emergency departments. Emergency Medicine Journal. 2009;26(11):783-5. [PubMed] [Free full text]
12. Skobeloff E, Spivey W, McNamara R, Greenspon L. Intravenous magnesium sulfate for the treatment of acute asthma in the emergency department. JAMA. 1989;262(9):1210. [PubMed] [Free full text]
13. Ciarallo L, Sauer AH, Shannon MW. Intravenous magnesium therapy for moderate to severe pediatric asthma: results of a randomized, placebo-controlled trial. J Pediatr. 1996;129(6):809–14. doi: 10.1016/S0022-3476(96)70023-9. [PubMed] [Free full text]
14. Ciarallo L, Brousseau D, Reinert S. Higher-dose intravenous magnesium therapy for children with moderate to severe acute asthma. Arch Pediatr Adolesc Med. 2000;154(10):979–83. doi: 10.1001/archpedi.154.10.979. [PubMed] [Free full text]
15. Green SM, Rothrock SG. Intravenous magnesium for acute asthma: failure to decrease emergency treatment duration or need for hospitalization. Ann Emerg Med. 1992 Mar;21(3):260-5. [PubMed]
16. Tiffany BR, Berk WA, Todd IK, White SR. Magnesium bolus or infusion fails to improve expiratory flow in acute asthma exacerbations. CHEST Journal. 1993;104(3):831-4. [PubMed]
17. Schuh S, Macias C, Freedman SB, Plint AC, Zorc JJ, Bajaj L, et al. North American practice patterns of intravenous magnesium therapy in severe acute asthma in children. Academic Emergency Medicine. 2010;17(11):1189-96. doi: 10.1111/j.1553-2712.2010.00913.x. [PubMed] [Free full text]
18. Scarfone RJ, Loiselle JM, Joffe MD, Mull CC, Stiller S, Thompson K, et al. A randomized trial of magnesium in the emergency department treatment of children with asthma. Annals of emergency medicine. 2000;36(6):572-8. [PubMed]
19. Guerrera M, Volpe S, Mao J. Therapeutic uses of magnesium. American Family Physician. 2009;80(2):157-62. [PubMed] [Free full text]
20. Monem GF, Kissoon N, DeNicola L. Use of magnesium sulfate in asthma in childhood. Pediatric annals. 1996;25(3):136-44. [PubMed]
21. Song WJ, Chang YS. Magnesium sulfate for acute asthma in adults: a systematic literature review. Asia Pac Allergy. 2012;2(1):76-85. doi: 10.5415/apallergy.2012.2.1.76. [PubMed] [Free full text]
22. Spivey WH, Skobeloff EM, Levin RM. Effect of magnesium chloride on rabbit bronchial smooth muscle. Annals of emergency medicine. 1990;19(10):1107-12. [PubMed]
23. Gourgoulianis K, Chatziparasidis G, Chatziefthimiou A, Molyvdas P-A. Magnesium as a relaxing factor of airway smooth muscles. Journal of aerosol medicine. 2001;14(3):301-7. [PubMed] [Free full text]
24. Del Castillo J, Engbaek L. The nature of the neuromuscular block produced by magnesium. The Journal of physiology. 1954;124(2):370-84. [PubMed] [Free full text]
25. Bois P. Effect of magnesium deficiency on mast cells and urinary histamine in rats. British journal of experimental pathology. 1963;44(2):151-5. [PubMed] [Free full text]
26. Classen H, Jacob R, Schimatschek H. Interactions of Magnesium with Direct and Indirect Acting Sympathomimetic Amines. Magnes Bull. 1987;9(2):80-7.
27. Aggarwal P, Sharad S, Handa R, Dwiwedi S, Irshad M. Comparison of nebulised magnesium sulphate and salbutamol combined with salbutamol alone in the treatment of acute bronchial asthma: a randomised study. Emerg Med J. 2006 May;23(5):358-62. [PubMed] [Free full text]
28. Silverman RA, Osborn H, Runge J, Gallagher EJ, Chiang W, Feldman J, et al. IV Magnesium Sulfate in the Treatment of Acute Severe Asthma: A Multicenter Randomized Controlled Trial. Chest. 2002;122(2):489-97. [PubMed]
29. Rowe BH, Bretzlaff J, Bourdon C, Bota G, Camargo Jr C. Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. Cochrane Database Syst Rev. 2000;2(1). [PubMed]
30. Goodacre S, Cohen J, Bradburn M, Gray A, Benger J, Coats T, et al. Intravenous or nebulised magnesium sulphate versus standard therapy for severe acute asthma (3Mg trial): a double-blind, randomised controlled trial. The Lancet Respiratory Medicine. 2013;1(4):293-300. doi: 10.1016/S2213-2600(13)70070-5. doi: 10.1016/S2213-2600(13)70070-5. [PubMed] [Free full text]
1Professor & Chairman, Cell: +92 300 321 1417, E-mail: beesaleh@hotmail.com
2Assistant Professor, +92 306 829 4346, E-mail: rafiatabassum2013@gmail.com
3Consultant Anesthesiologist, Cell: +92 302 322 6500, E-mail: draijazhussainawan@gmail.com
Department of Anesthesiology, SICU & Pain Management Center, Peoples University Of Medical & Health Sciences For Women, Shaheed Benazirabad, Sind, (Pakistan)
Correspondence: Professor Muhammad Saleh Khaskheli, Chairman, Department of Anaesthesiology, SICU & Pain Management Center, Peoples University of Medical & Health Sciences For Women, Shaheed Benazirabad, Sind (Pakistan); Cell: 03003211417; E-mail: beesaleh@hotmail.com
ABSTRACT
Objective: The recent interest in intravenous magnesium sulphate for using it in many other indications other than control of eclamptic fits lead the researchers to try it as a smooth muscle relaxant in cases of acute bronchial asthma. The results have largely been controversial, so we conducted this study to determine efficacy of intravenous magnesium sulphate in acute asthma based on its terminal outcome.
Methodology: This retrospective study was conducted at Surgical Intensive Care Unit at Peoples University of Medical and Health Sciences for Women, Nawabshah from January 2014-December 2015. We retrospectively reviewed the medical data sheets of all cases of acute asthma admitted during the study period, and extracted the relevant information. All the patients were initially treated with standard therapy for asthma and then given 4ml of 50% MgSO4 (2g) diluted in 250 ml of normal saline intravenously. Outcomes were presented in percentages and frequencies while patient age is presented as mean ± SD.
Results: The mean age of the population was 45.29 ± 20.1 y. We had a female predominance in our population (60.3%). Successfully cured patients were 32.3% whereas those expired were 57.4%. There was not a significant difference between the genders for the outcome (p > 0.05).
Conclusions: We found that intravenous magnesium sulphate is ineffective in successfully management of patients with acute asthma in terms of enhanced survival rate.
Keywords: Magnesium sulphate; Bronchial asthma; Efficacy; Emergency management.
Citation: Khaskheli MS, Tabassum R, Awan AH. Effectiveness of intravenous magnesium sulphate in acute asthma: a retrospective study. Anaesth Pain & Intensive Care 2017;21(4):458462
Received: 02 Feb 2017; Reviewed: 7 Feb & 21 Jul 2017; Corrected: 8 Feb, 31 Mar, 20 Jul 2017; Accepted: 12 Aug 2017
INTRODUCTION
Asthma is a chronic inflammatory disease of the lower airways characterized by respiratory symptoms and variable airway obstruction. Its clinical manifestations include recurrent symptoms, often involving shortness of breath, wheezing, coughing and chest tightness.1 In developed centuries, asthma is prevalent in 4-5% of the population and almost 27% of patients requiring admission.2 It is extremely prevalent with up to 1:10 adults worldwide.3
In addition to general treatment strategy, standard management of asthma include β2-agonists, inhaled anticholinergic agents, short-acting bronchodilators, and corticosteroids.4,5 For patients unresponsive to these initial therapies, magnesium sulfate (MgSO4) may be a treatment option.1,6 It has also been recommended as an adjunct in treating severe asthma with other mainline drugs.7,8 In patients who do not respond to initial treatments and those with severe, life-threatening acute exacerbations, current guidelines are suggestive of using MgSO4 as an adjunct therapy for reducing hospital stay and improving pulmonary functions, while the evidence for using nebulized magnesium is still inconclusive.4,7,9-11 Results have been mixed for several randomized controlled trials (RCTs) using intravenous MgSO4 in acute patients as some studies demonstrate its benefits,12-14 while others do not.2,15,16 Moreover, the studies reporting positive outcomes have shown a benefit predominantly in severe exacerbations as two recent reviews supported its use as an adjunct in severe asthma.2
Intravenous MgSO4 has a high safety profile17 with commonly reported minor side effects including dry mouth, flushing, malaise pain, and numbness at the site of infusion.1,18 Potential drug interactions include potassium-sparing diuretics and glucagon, which when used simultaneously, increase serum magnesium levels. If concomitant use of both drug groups have to be used, commonly reported problems need to be monitored or the later drug withheld temporarily if possible.1,19 Contraindications to the use of MgSO4 include myasthenia gravis, myocardial conditions, AV block and renal failure (creatinine clearance less than 30 ml/min).1,20
There has not been any study from Pakistan on this topic and there is scarce and conflicting data available on it particularly in Asia.9 Therefore, this study was conducted to investigate the efficacy of intravenous magnesium sulphate in acute asthma based on its outcomes.
METHODOLOGY
The study was approved by the institutional ethical committee. We conducted a retrospective review of all cases of acute severe asthma transferred to Surgical Intensive Care Unit at Peoples University of Medical and Health Sciences for Women, Nawabshah over a period of 2 years (January 2014-December 2015), and extracted the relevant information from the medical records. We excluded the poisoning cases, post-operative cases, post-trauma and patients on ventilatory support from the analysis. Variables under consideration were age and outcome (expired, cured, and referred). We, however, did not obtain any information on post-referral state of the patients. These patients were referred to hospitals with better treatment facilities on the request of their family or due to the orders of their treating physician.
Moreover, all the patients were initially managed at the Department of Medicine and then shifted to Surgical Intensive Care Unit. Before the current admission, most patients had a history of asthma and were received treatment with maintenance and/or rescue medications at home. In addition, patients received standard therapy (including nebulized salbutamol and ipratropium bromide, and systematic hydrocortisone) for an asthma exacerbation before receiving treatment with intravenous magnesium sulfate. All the patients were initially treated with standard therapy for asthma and then given intravenous magnesium sulphate i.e. received 4 ml of 50% MgSO4 (2 g) diluted in 250 ml of normal saline and given slowly over 20 min as per the recent recommendations.21 All the patients, after being stable were shifted to the Department of Medicine.
Statistical analysis: The data was recorded and kept on Microsoft Excel 2007 Spreadsheets. We extracted the relevant information and analyzed it on SPSS version 20. Gender and outcomes were presented in percentages and frequencies while age were presented as mean ± SD. Chi square test was used for comparing the outcome between the genders. The significance level was set at p < 0.05. RESULTS A total of 136 patients were enrolled in the study during the study period. There was a female predominance 82 (60.3%) as compared to males, which were 54 (39.7%). The mean age was 45.29 ± 20.1 y. The cured patients were 32.3% whereas those expired were 57.4%. Table 1 shows the demographic variables while Graph 1 shows outcomes based on the gender of the patients. There was not a significant difference between the genders for the outcome; cure rate for males was 25(18.38%) vs. 19(13.87%) (p > 0.05). A total of 78 (57.4%) patients expired despite the use of MgSO4.
Table 1: Demographic variables and outcomes
| Variables | Data |
| Age (years) | 45.29 ± 20.1 |
| Gender
· Male · Female |
54 (39.7) 82 (60.3) |
| Outcome
· Cured · Expired · Referred |
44 (32.3%) 78 (57.4%) 14 (10.3%) |
DISCUSSION
MgSO4 has been used as an adjunct in managing acute asthma but there is still lack of adequate evidence to support its effectiveness. Most of the studies have been conducted in the West and there is a high gap of research in the Asia-Pacific region.9 The role of MgSO4 in asthma is still unclear, but some studies have helped explain its mode of action. The possible effects of MgSO4 on smooth muscles may include activating sodium-calcium pumps and blocking the entry and release of calcium from the endoplasmic reticulum (ER) which consequently result in decrease in intracellular calcium.22,23 Moreover, MgSO4 inhibits acetylcholine release and depresses excitability of muscle fiber in cholinergic motor nerve terminals, ultimately generating bronchial smooth muscle relaxation.24 Furthermore, calcium and myosin interaction is inhibited by magnesium sulphate resulting into muscle cell relaxation. Magnesium also reduces inflammatory mediators by inhibiting mast cell degranulation and stabilizing T-cells.25 It may also increase the receptor affinity of β2-agonists thereby, increasing their bronchodilator effect.9,26 Lastly, it may directly reduce the severity of asthma by stimulating the synthesis of prostacyclin and nitric oxide.1
We found that 57.4% patients died even after the management of asthma with magnesium sulphate. However, the use of intravenous MgSO4 improved pulmonary function in adults but did not cause any reduction in the rate of hospitalization.27,28 Furthermore, a Cochrane review reported the effectiveness of MgSO4 in the treatment of acute asthma,29 whereas, the recent reviews by Mohammed et al. found that the efficacy of MgSO4 was only marginal on pulmonary function (SMD=0.25, 95% CI= 0.01-0.51).6 Moreover, the most recent review was unable to draw clear conclusions about effectiveness of MgSO4 in adults. However, it was suggested that intravenous MgSO4 seemed to be effective in children.30 This shows that there are mixed results and conclusions about the efficacy of magnesium sulphate in management of acute asthma. We tried a different strategy of finding efficacy of magnesium sulphate as compared to the previous studies; they most often were, randomized controlled trials; but we used an outcome-based retrospective review, concluding that magnesium sulphate was ineffective in asthma management.
Strengths and Limitations: This study is the first one from Pakistan on the role of magnesium sulphate in the management of asthma. However, it has its limitations. The study design for this study was retrospective in which charts of the patients were reviewed. Outcome measures were weak and duration of hospital stay, ventilator support, and post-referral status were not obtained and addressed. Nevertheless, this study expands the previous knowledge base on the use of intravenous magnesium sulphate in asthma management.
CONCLUSION
We found that intravenous magnesium sulphate is ineffective in managing patients with acute asthma. However, there is still need of some larger studies, primarily the randomized trials and prospective studies, to draw definite conclusions about the role of magnesium sulphate in the management of asthma.
Conflict of interest: None declared by the authors
Author contribution: MSK – Manuscript editing
RT – Statistical analysis
AHA – Literature search
REFERENCES
1. Bittar TMB, Guerra SD. Use of intravenous magnesium sulfate for the treatment of severe acute asthma in children in emergency department. Revista Brasileira de terapia intensiva. 2012;24(1):86-90. [Free full text]
2. Kumar SA, Shailendranath G, Raj K. A randomized controlled trial of intravenous magnesium sulphate as an adjunct to standard therapy in acute severe asthma. Iranian Journal of Allergy, Asthma and Immunology. 2008;7(4):221-9. [Free full text]
3. Annesi-Maesano I. Epidemiology of asthma in the world and in France. Rev Prat. 2011 Mar;61(3):329-35.[PubMed]
4. Shan Z, Rong Y, Yang W, Wang D, Yao P, Xie J, et al. Intravenous and nebulized magnesium sulfate for treating acute asthma in adults and children: a systematic review and meta-analysis. Respiratory Medicine. 2013;107(3):321-30. doi: 10.1016/j.rmed.2012.12.001.[PubMed] [Free full text]
5. Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, et al. Global strategy for asthma management and prevention: GINA executive summary. The European respiratory journal. 2008;31(1):143. doi: 10.1183/09031936.00138707. [PubMed] [Free full text]
6. Mohammed S, Goodacre S. Intravenous and nebulised magnesium sulphate for acute asthma: systematic review and meta-analysis. Emerg Med J. 2007 Dec;24(12):823-30. [PubMed] [Free full text]
7. Hossein S, Pegah A, Davood F, Said A, Babak M, Mani M, et al. The effect of nebulized magnesium sulfate in the treatment of moderate to severe asthma attacks: A randomized clinical trial. Am J Emerg Med. 2016 May;34(5):883-6. doi: 10.1016/j.ajem.2016.01.024. [PubMed]
8. Blitz M, Blitz S, Beasely R, Diner B, Hughes R, Knopp J, et al. Inhaled magnesium sulfate in the treatment of acute asthma. The Cochrane database of systematic reviews. 2005(2):CD003898. [PubMed]
9. Song WJ, Chang Y-S. Magnesium sulfate for acute asthma in adults: a systematic literature review. Asia Pacific Allergy. 2012;2(1):76. doi: 10.5415/apallergy.2012.2.1.76. [PubMed] [Free full text]
10. Hughes R, Goldkorn A, Masoli M, Weatherall M, Burgess C, Beasley R. Use of isotonic nebulised magnesium sulphate as an adjuvant to salbutamol in treatment of severe asthma in adults: randomised placebo-controlled trial. The Lancet. 2003;361(9375):2114-7. [PubMed] [Free full text]
11. Jones L, Goodacre S. Magnesium sulphate in the treatment of acute asthma: evaluation of current practice in adult emergency departments. Emergency Medicine Journal. 2009;26(11):783-5. [PubMed] [Free full text]
12. Skobeloff E, Spivey W, McNamara R, Greenspon L. Intravenous magnesium sulfate for the treatment of acute asthma in the emergency department. JAMA. 1989;262(9):1210. [PubMed] [Free full text]
13. Ciarallo L, Sauer AH, Shannon MW. Intravenous magnesium therapy for moderate to severe pediatric asthma: results of a randomized, placebo-controlled trial. J Pediatr. 1996;129(6):809–14. doi: 10.1016/S0022-3476(96)70023-9. [PubMed] [Free full text]
14. Ciarallo L, Brousseau D, Reinert S. Higher-dose intravenous magnesium therapy for children with moderate to severe acute asthma. Arch Pediatr Adolesc Med. 2000;154(10):979–83. doi: 10.1001/archpedi.154.10.979. [PubMed] [Free full text]
15. Green SM, Rothrock SG. Intravenous magnesium for acute asthma: failure to decrease emergency treatment duration or need for hospitalization. Ann Emerg Med. 1992 Mar;21(3):260-5. [PubMed]
16. Tiffany BR, Berk WA, Todd IK, White SR. Magnesium bolus or infusion fails to improve expiratory flow in acute asthma exacerbations. CHEST Journal. 1993;104(3):831-4. [PubMed]
17. Schuh S, Macias C, Freedman SB, Plint AC, Zorc JJ, Bajaj L, et al. North American practice patterns of intravenous magnesium therapy in severe acute asthma in children. Academic Emergency Medicine. 2010;17(11):1189-96. doi: 10.1111/j.1553-2712.2010.00913.x. [PubMed] [Free full text]
18. Scarfone RJ, Loiselle JM, Joffe MD, Mull CC, Stiller S, Thompson K, et al. A randomized trial of magnesium in the emergency department treatment of children with asthma. Annals of emergency medicine. 2000;36(6):572-8. [PubMed]
19. Guerrera M, Volpe S, Mao J. Therapeutic uses of magnesium. American Family Physician. 2009;80(2):157-62. [PubMed] [Free full text]
20. Monem GF, Kissoon N, DeNicola L. Use of magnesium sulfate in asthma in childhood. Pediatric annals. 1996;25(3):136-44. [PubMed]
21. Song WJ, Chang YS. Magnesium sulfate for acute asthma in adults: a systematic literature review. Asia Pac Allergy. 2012;2(1):76-85. doi: 10.5415/apallergy.2012.2.1.76. [PubMed] [Free full text]
22. Spivey WH, Skobeloff EM, Levin RM. Effect of magnesium chloride on rabbit bronchial smooth muscle. Annals of emergency medicine. 1990;19(10):1107-12. [PubMed]
23. Gourgoulianis K, Chatziparasidis G, Chatziefthimiou A, Molyvdas P-A. Magnesium as a relaxing factor of airway smooth muscles. Journal of aerosol medicine. 2001;14(3):301-7. [PubMed] [Free full text]
24. Del Castillo J, Engbaek L. The nature of the neuromuscular block produced by magnesium. The Journal of physiology. 1954;124(2):370-84. [PubMed] [Free full text]
25. Bois P. Effect of magnesium deficiency on mast cells and urinary histamine in rats. British journal of experimental pathology. 1963;44(2):151-5. [PubMed] [Free full text]
26. Classen H, Jacob R, Schimatschek H. Interactions of Magnesium with Direct and Indirect Acting Sympathomimetic Amines. Magnes Bull. 1987;9(2):80-7.
27. Aggarwal P, Sharad S, Handa R, Dwiwedi S, Irshad M. Comparison of nebulised magnesium sulphate and salbutamol combined with salbutamol alone in the treatment of acute bronchial asthma: a randomised study. Emerg Med J. 2006 May;23(5):358-62. [PubMed] [Free full text]
28. Silverman RA, Osborn H, Runge J, Gallagher EJ, Chiang W, Feldman J, et al. IV Magnesium Sulfate in the Treatment of Acute Severe Asthma: A Multicenter Randomized Controlled Trial. Chest. 2002;122(2):489-97. [PubMed]
29. Rowe BH, Bretzlaff J, Bourdon C, Bota G, Camargo Jr C. Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. Cochrane Database Syst Rev. 2000;2(1). [PubMed]
30. Goodacre S, Cohen J, Bradburn M, Gray A, Benger J, Coats T, et al. Intravenous or nebulised magnesium sulphate versus standard therapy for severe acute asthma (3Mg trial): a double-blind, randomised controlled trial. The Lancet Respiratory Medicine. 2013;1(4):293-300. doi: 10.1016/S2213-2600(13)70070-5. doi: 10.1016/S2213-2600(13)70070-5. [PubMed] [Free full text]