Ali Asghar1, Madiha Hashmi1, Alia Hussain1
1Dept. of Anaesthesiology, Aga Khan University Hospital, Karachi (Pakistan)
Correspondence: Dr. Ali Asghar, Dept. of Anaesthesiology, Aga Khan University Hospital, Karachi (Pakistan); Phone: 03333306229; E-mail: asghar.ashraf@aku.edu
ABSTRACT
Objective: Raised intracranial pressure (ICP) is a common manifestation of severe brain injury. Rapid diagnosis and timely intervention is required to prevent secondary brain damage and death. Measurement of optic nerve sheath diameter (ONSD) by ultrasound is increasingly used as a marker to detect raised ICP. Knowledge of normal ONSD in a healthy population is essential to interpret this measurement. We aimed to evaluate normal optic nerve sheath diameter in healthy volunteers in Pakistan.
Methodology: It was a prospective, observational study in which one hundred healthy volunteers of Pakistani origin, aged more than 18 years were recruited in the study. The ultrasound probe was placed on the superior and lateral aspect of the orbit against the upper eyelid with the eye closed. For each subject, the primary investigator performed three measurements on each eye. The measurements of each eye were then averaged to yield a mean ONSD.
Results: The median ONSD of right eye was 4.84 mm and 95% of individuals had mean ONSD in the range 4.84–4.97 mm while the median ONSD of left eye was 4.86 mm and 95% of individuals had mean ONSD in the range 4.85–4.96 mm. There was no difference among the 3 repeated measures of ONSD in each eye. There was no relationship between ONSD with age, gender and measurement taken between left and right eyes.
Conclusion: 95% ofstudy sample have an ONSD less than 4.82 mm. ONSD more than 4.82 mm in this population should be considered abnormal and may reflect raised intracranial pressure.
Key words: Optic Nerve;Intracranial Pressure;Ocular Tension; Ocular Tonometry; Ocular ultrasound; Ultrasonography
Citation: AsgharA, HashmiM, HussainA. Optic nerve sheath diameter evaluated by transorbital sonography in healthy volunteers from Pakistan.Anaesth Pain & Intensive Care 2015;19(3)282-286
INTRODUCTION
Raised intracranial pressure (ICP) is a common manifestation of severe brain injury. Rapid diagnosis and timely intervention is required to prevent secondary brain damage and death. In severe traumatic brain injury (TBI) it is recommended to monitor ICP continuously with an aim to keep it less than 20–25 mmHg.1,2 ICP can be definitively measured and monitored through placement of invasive monitoring devices such as an external ventricular drain (EVD).3,4 Other monitoring techniques using either an intra-parenchymal probe or an intra-ventricular catheterare also invasive and associated with risk of hemorrhage and infection.5,6Computed tomography (CT) and magnetic resonance imaging (MRI) suggest raised ICP with signs including effacement of basal cisterns, diffuse sulci effacement and the presence of significant midline shift. These imaging modalities are frequently used to make decisions regarding management of intracranial hypertension, although they have not been validated as accurate predictors. An accurate, reliable, noninvasive, point-of-care monitoring device to identify presence of intracranial hypertension would be helpful in situations where there is clinical suspicion for intracranial hypertension but invasive monitoring and advanced imaging modalities are either unavailable, expensive or associated with unacceptable risk.In centers where facility to monitor ICP using invasive techniques are available, initial non-invasive monitoring could also be used to select the high risk patients.
Bedside ocular ultrasound (US) is an emerging noninvasive technique to measure optic nerve sheath diameter (ONSD). The ultrasonographic measurement of ONSD,a fixed distance from the retina has been evaluated to identify the presence of raised ICP in patients with TBI and intracranial Hemorrhage (ICH).7-10However, there is considerable inter-individual variation in the ONSD, and a consensus regarding cut-off for an abnormal ONSD, indicating raised intracranial pressure is not established.5 mm is most commonly used cut-off in adults but values up to 5.9 mm have been used in some studies.11 Knowledge of the normal range of ONSD in healthy population is essential to interpret this measurement as a marker of raised intracranial pressure in clinical practice. The objective of this study was to evaluate normal optic nerve sheath diameter in healthy volunteers in Pakistan.
METHODOLOGY
After approval from departmental and hospital ethical committees,written informed consent was obtained from all healthy adult volunteers (age > 18 years), employed as staff in the operating rooms of a tertiary care hospital of Pakistan. This was the prospective, observational study in which volunteers of both genders, with no known comorbidities,were recruited for the study from September 2014 to April 2015. Those with preexisting optic nerve pathology or had a history of orbital injury were excluded.Demographic data were collected on a predesigned form and included age, gender, height and weight. All ONSD scans were performed by primary investigatorusing Mindray ultrasound machine with a 7.5 MHz linear array probe with orbital imaging settings and a high resolution optimization setting. The probe wasplaced on the superior and lateral aspect of the orbit against the upper eyelid with the eye closed and angled slightly caudally and medially until the optic nerve wasvisualized as a linear hypo-echoic structure with clearly defined margins posterior to the globe. For each subject, the primary investigator who had one year experience in performing ultrasound, performed three measurements on each eye. The resultantmeasurements of each eye were then averaged to yield a mean ONSD.
Sample Size calculation was based on a previous study.12 A total of 100 healthy individual were included to estimate 95% confidence interval within ±0.10 margin of error. The standard deviation estimate based on the range of data value, which is approximate 0.5.
SD of ONSD= 0.5
CI= 95%
Precision (d) = 0.10
Zα/2 =1.96
= 97
All statistical analysis was performed using statistical package for social science version 19 (SPSS Inc., Chicago, IL). Normality assumption was checked by histogram and Shapiro-Wilk test and median with IQR, mean ± SD, max, min, and 95% percentile were computed for ONSD. Mann Whitney U test was used to compare unpaired ONSD between genders and Wilcoxon matched pairs signed rank test to compare left and right eyes. Friedman’s two ways ANOVA was used to compare the difference of ONSD for repeated observation and intra-class correlation coefficient (ICC) were used to test for differences between the repeated measures of ONSD within individuals. Spearman rank correlation test was used to determine the correlation between the ONSD and other parameters including age, weight, height and BMI. P values of ≤ 0.05 were considered to be statistically significant.
RESULTS
A total of 100 healthy volunteers were enrolled during the study period, consisting of 59 males and 41females.Other demographic characteristics is also shown in Table 1. All patients were of Pakistani origin. The median ONSD of righteye was 4.84 mm and 95% of individuals had mean ONSD in the range 4.84–4.97mm whilethe median ONSD of left eye was 4.86 mm and 95% of individuals had mean ONSD in the range 4.85–4.96 mm (Table 2). There was no difference among the 3 repeated measures of ONSD in each eye (Table3). There was no relationship between ONSD with age, gender and measurement taken between left and right eyes (Table 4, 5 & Figure 1)
Table 1: Demographic data measured
Table 2: Comparison of optic nerve sheath diameter (ONSD) measurement
Median ONSD Right vs. Left eye; p= 0.71, Wilcoxon matched paired rank test
Table 3: Comparison of repeated measured mean ONSD and Intra class correlation the three repeated measurements of ONSD for left and right eye
Friedman’s Two way ANOVA test , ICC= Intra class Correlation
Table 4: Descriptive statistics of optic nerve sheath diameter (ONSD)
Data were presented as median and inter-quartile range
Mann-Whitney U test
Table 5: Correlation between optic nerve sheath diameters with other measures
This table shows the combined results of both eyes (n = 100).
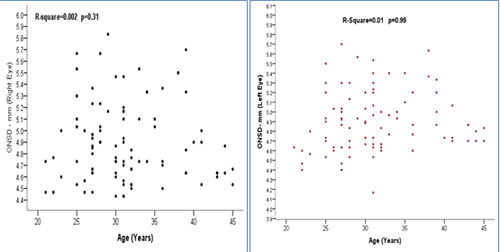
Figure 1: Scatter plot showing the relationship between optic nerve sheath diameter (ONSD) with age for right and left eyes
DISCUSSION
Raised intracranial pressure (ICP) causes secondary brain damage and adversely affects patient outcome.13 Various methods used to assess ICP include clinical examination and fundoscopy, lumbar puncture, radiological imaging and ventriculostomy.14 The gold standard for diagnosis of raised ICP is invasive monitoring 15, but it is not used in developing countries due to unavailability of the monitoring devices, lack of expertise and the associated cost of the procedure. ONSD is an alternative method to measure ICP which is a cost effective, simple, safe and easily available technique. In patients with a raised ICP, optic nerve sheath diameter increases due to its continuation with the meninges and subarachnoid space.16 Over the last few years this evolving technique has been used successfully to monitor and predict ICP in patients with subarachnoid hemorrhage, intracranial hemorrhage and traumatic brain injuries.17
The cutoff point of ONSD has however been a topic of considerable dispute.18-22Even in studies done on healthy volunteers, the range of ONSD measured by ultrasound varies. Results of this study showed that the cutoff for the upper limit of normal ONSD in Pakistani people was 4.82 mm and the range varied from 4.3 mm-5.7 mm.There was no correlation of ONSDwith age, gender, height and weight and it was similar in both eyes. Results of this study were similar to a study conducted in the USA where the median ONSD varied from 4.4 – 4.8 mm in different positions.18 A study with a large sample size, conducted in Bangladeshi population showed that the median ONSD was 4.41 mm with 95 % of subjects in the range of 4.25to 4.75 mm.19 However, there was no age limit for the study subjects and about 12.5% of study population was less than 16 years of age. This might explain the smaller ONSD reported in the Bangladeshi population as compared to the Pakistani population. Vaiman et al. conducted a study in Israeli population using CT or MRI due to better resolution power to determine the normal range of ONSD. They reported that the mean ONSD was 4.94± 1.51 mm in the right eye and 5.17 ± 1.34 mm in left eye.20 Amini et al reported that the mean ONSD in Irani population was 4.6 mm.17 The median ONSD reported by Wang et al in Chinese population was 5.1 mm.21
A few studies showed higher value of ONSD than previously described. Bauerle et al found mean ONSD of 5.4 mm with a range of 4.3 mm- 7.6 mm in German population.22 In this study he used ultrasound to measure ONSD. After a year he conducted another study and used MRI for measurement of ONSD and reported higher value of ONSD 5.69 ± 0.77 in Germans.23 Geeraerts et al also used MRI for ONSD measurement and found that ONSD was 5.08 ± 0.52 mm in healthy volunteersfrom Britain. He also showed that there was a good correlation between ultrasound and MRI measurement of ONSD 3 mm behind the pupils.24
The lowest ONSD of 3.4 mm was reported by Ballantyne et al but he actually measured optic nerve diameter rather than ONSD.25
LIMITATIONS
There are several limitations in this study. All the measurements on each subject were done by the primary investigator which could have introduced observer bias to the subsequent readings. In addition since the primaryinvestigator measured the ONSD in all subjects, the inter-observervariability could not be assessed in this study. The other limitations were that only 100 healthy volunteers were recruited from a single center of Pakistan which does not reflect the whole population of this country and the studywas conducted in adult healthy volunteers so the normal range of ONSD in pediatrics population could not be assessed.
CONCLUSION
95% of study sample have an ONSD less than 4.82 mm,measured by 7.5 MHz linear array ultrasoundprobe in horizontal plane and is independent of age, gender, height, weight and was similar in botheyes. ONSD more than 4.82 mm in this samplecan be considered abnormal and may reflect raised intracranial pressure.But in future larger studies are recommended to reflect the whole population of Pakistan.
Conflict of interest: None declared by the authors
Author responsibility/contribution:
AA: Protocol writing, data collection, analysis, manuscript writing
MH: Protocol reviewing, analysis, manuscript writing
AH: Data collection, manuscript writing
REFERENCES
1Dept. of Anaesthesiology, Aga Khan University Hospital, Karachi (Pakistan)
Correspondence: Dr. Ali Asghar, Dept. of Anaesthesiology, Aga Khan University Hospital, Karachi (Pakistan); Phone: 03333306229; E-mail: asghar.ashraf@aku.edu
ABSTRACT
Objective: Raised intracranial pressure (ICP) is a common manifestation of severe brain injury. Rapid diagnosis and timely intervention is required to prevent secondary brain damage and death. Measurement of optic nerve sheath diameter (ONSD) by ultrasound is increasingly used as a marker to detect raised ICP. Knowledge of normal ONSD in a healthy population is essential to interpret this measurement. We aimed to evaluate normal optic nerve sheath diameter in healthy volunteers in Pakistan.
Methodology: It was a prospective, observational study in which one hundred healthy volunteers of Pakistani origin, aged more than 18 years were recruited in the study. The ultrasound probe was placed on the superior and lateral aspect of the orbit against the upper eyelid with the eye closed. For each subject, the primary investigator performed three measurements on each eye. The measurements of each eye were then averaged to yield a mean ONSD.
Results: The median ONSD of right eye was 4.84 mm and 95% of individuals had mean ONSD in the range 4.84–4.97 mm while the median ONSD of left eye was 4.86 mm and 95% of individuals had mean ONSD in the range 4.85–4.96 mm. There was no difference among the 3 repeated measures of ONSD in each eye. There was no relationship between ONSD with age, gender and measurement taken between left and right eyes.
Conclusion: 95% ofstudy sample have an ONSD less than 4.82 mm. ONSD more than 4.82 mm in this population should be considered abnormal and may reflect raised intracranial pressure.
Key words: Optic Nerve;Intracranial Pressure;Ocular Tension; Ocular Tonometry; Ocular ultrasound; Ultrasonography
Citation: AsgharA, HashmiM, HussainA. Optic nerve sheath diameter evaluated by transorbital sonography in healthy volunteers from Pakistan.Anaesth Pain & Intensive Care 2015;19(3)282-286
INTRODUCTION
Raised intracranial pressure (ICP) is a common manifestation of severe brain injury. Rapid diagnosis and timely intervention is required to prevent secondary brain damage and death. In severe traumatic brain injury (TBI) it is recommended to monitor ICP continuously with an aim to keep it less than 20–25 mmHg.1,2 ICP can be definitively measured and monitored through placement of invasive monitoring devices such as an external ventricular drain (EVD).3,4 Other monitoring techniques using either an intra-parenchymal probe or an intra-ventricular catheterare also invasive and associated with risk of hemorrhage and infection.5,6Computed tomography (CT) and magnetic resonance imaging (MRI) suggest raised ICP with signs including effacement of basal cisterns, diffuse sulci effacement and the presence of significant midline shift. These imaging modalities are frequently used to make decisions regarding management of intracranial hypertension, although they have not been validated as accurate predictors. An accurate, reliable, noninvasive, point-of-care monitoring device to identify presence of intracranial hypertension would be helpful in situations where there is clinical suspicion for intracranial hypertension but invasive monitoring and advanced imaging modalities are either unavailable, expensive or associated with unacceptable risk.In centers where facility to monitor ICP using invasive techniques are available, initial non-invasive monitoring could also be used to select the high risk patients.
Bedside ocular ultrasound (US) is an emerging noninvasive technique to measure optic nerve sheath diameter (ONSD). The ultrasonographic measurement of ONSD,a fixed distance from the retina has been evaluated to identify the presence of raised ICP in patients with TBI and intracranial Hemorrhage (ICH).7-10However, there is considerable inter-individual variation in the ONSD, and a consensus regarding cut-off for an abnormal ONSD, indicating raised intracranial pressure is not established.5 mm is most commonly used cut-off in adults but values up to 5.9 mm have been used in some studies.11 Knowledge of the normal range of ONSD in healthy population is essential to interpret this measurement as a marker of raised intracranial pressure in clinical practice. The objective of this study was to evaluate normal optic nerve sheath diameter in healthy volunteers in Pakistan.
METHODOLOGY
After approval from departmental and hospital ethical committees,written informed consent was obtained from all healthy adult volunteers (age > 18 years), employed as staff in the operating rooms of a tertiary care hospital of Pakistan. This was the prospective, observational study in which volunteers of both genders, with no known comorbidities,were recruited for the study from September 2014 to April 2015. Those with preexisting optic nerve pathology or had a history of orbital injury were excluded.Demographic data were collected on a predesigned form and included age, gender, height and weight. All ONSD scans were performed by primary investigatorusing Mindray ultrasound machine with a 7.5 MHz linear array probe with orbital imaging settings and a high resolution optimization setting. The probe wasplaced on the superior and lateral aspect of the orbit against the upper eyelid with the eye closed and angled slightly caudally and medially until the optic nerve wasvisualized as a linear hypo-echoic structure with clearly defined margins posterior to the globe. For each subject, the primary investigator who had one year experience in performing ultrasound, performed three measurements on each eye. The resultantmeasurements of each eye were then averaged to yield a mean ONSD.
Sample Size calculation was based on a previous study.12 A total of 100 healthy individual were included to estimate 95% confidence interval within ±0.10 margin of error. The standard deviation estimate based on the range of data value, which is approximate 0.5.
SD of ONSD= 0.5
CI= 95%
Precision (d) = 0.10
Zα/2 =1.96
= 97
All statistical analysis was performed using statistical package for social science version 19 (SPSS Inc., Chicago, IL). Normality assumption was checked by histogram and Shapiro-Wilk test and median with IQR, mean ± SD, max, min, and 95% percentile were computed for ONSD. Mann Whitney U test was used to compare unpaired ONSD between genders and Wilcoxon matched pairs signed rank test to compare left and right eyes. Friedman’s two ways ANOVA was used to compare the difference of ONSD for repeated observation and intra-class correlation coefficient (ICC) were used to test for differences between the repeated measures of ONSD within individuals. Spearman rank correlation test was used to determine the correlation between the ONSD and other parameters including age, weight, height and BMI. P values of ≤ 0.05 were considered to be statistically significant.
RESULTS
A total of 100 healthy volunteers were enrolled during the study period, consisting of 59 males and 41females.Other demographic characteristics is also shown in Table 1. All patients were of Pakistani origin. The median ONSD of righteye was 4.84 mm and 95% of individuals had mean ONSD in the range 4.84–4.97mm whilethe median ONSD of left eye was 4.86 mm and 95% of individuals had mean ONSD in the range 4.85–4.96 mm (Table 2). There was no difference among the 3 repeated measures of ONSD in each eye (Table3). There was no relationship between ONSD with age, gender and measurement taken between left and right eyes (Table 4, 5 & Figure 1)
Table 1: Demographic data measured
|
Variables |
Mean±SD |
Median(IQR) |
| Age (Years) |
31.08±5.90 |
30.5 (7) |
| Weight (kg) |
63.5±11.32 |
64 (17) |
| Height (cm) |
160.73±7.31 |
160 (7.31) |
| BMI (kg/m2) |
24.64±4.26 |
24.16 (5.50) |
|
ONSD |
Mean ± SD |
Median (IQR) |
Minimum |
Maximum |
95% Percentile |
| Both Eyes (Combined) |
4.90±0.30 |
4.82 (0.43) |
4.3 |
5.7 |
5.53 |
| Right Eye |
4.90±0.35 |
4.84 (0.47) |
4.43 |
5.83 |
5.5 |
| Left Eye |
4.90±0.31 |
4.86 (0.46) |
4.17 |
5.70 |
5.52 |
Table 3: Comparison of repeated measured mean ONSD and Intra class correlation the three repeated measurements of ONSD for left and right eye
|
Side |
ONSD |
P-Value |
ICC |
95%CI |
||
|
1st Reading |
2ndReading |
3rdReading |
||||
|
Right Eye |
4.9 (0.5) |
4.9 (0.6) |
4.8 (0.5) |
0.46 |
0.88 |
0.83 to 0.92 |
|
Left Eye |
4.9 (0.5) |
4.9 (0.5) |
4.9 (0.4) |
0.97 |
0.86 |
0.81 to 0.90 |
Table 4: Descriptive statistics of optic nerve sheath diameter (ONSD)
|
ONSD |
Males n=59 |
Females n=41 |
P-Value |
| Right Eye |
4.85 (0.53) |
4.83 (0.42) |
0.52 |
| Left Eye |
4.92 (0.47) |
4.83 (0.28) |
0.05 |
| Both Eyes (Combined) |
4.81 (0.52) |
4.83 (0.41) |
0.14 |
Mann-Whitney U test
Table 5: Correlation between optic nerve sheath diameters with other measures
|
Variables |
Spearman’s Rho Correction (ONSD) |
P-Value |
| Age (Years) |
0.05 |
0.61 |
| Weight (kg) |
-0.013 |
0.89 |
| Height (cm) |
0.029 |
0.77 |
| BMI (kg/m2) |
-0.018 |
0.85 |
Figure 1: Scatter plot showing the relationship between optic nerve sheath diameter (ONSD) with age for right and left eyes
DISCUSSION
Raised intracranial pressure (ICP) causes secondary brain damage and adversely affects patient outcome.13 Various methods used to assess ICP include clinical examination and fundoscopy, lumbar puncture, radiological imaging and ventriculostomy.14 The gold standard for diagnosis of raised ICP is invasive monitoring 15, but it is not used in developing countries due to unavailability of the monitoring devices, lack of expertise and the associated cost of the procedure. ONSD is an alternative method to measure ICP which is a cost effective, simple, safe and easily available technique. In patients with a raised ICP, optic nerve sheath diameter increases due to its continuation with the meninges and subarachnoid space.16 Over the last few years this evolving technique has been used successfully to monitor and predict ICP in patients with subarachnoid hemorrhage, intracranial hemorrhage and traumatic brain injuries.17
The cutoff point of ONSD has however been a topic of considerable dispute.18-22Even in studies done on healthy volunteers, the range of ONSD measured by ultrasound varies. Results of this study showed that the cutoff for the upper limit of normal ONSD in Pakistani people was 4.82 mm and the range varied from 4.3 mm-5.7 mm.There was no correlation of ONSDwith age, gender, height and weight and it was similar in both eyes. Results of this study were similar to a study conducted in the USA where the median ONSD varied from 4.4 – 4.8 mm in different positions.18 A study with a large sample size, conducted in Bangladeshi population showed that the median ONSD was 4.41 mm with 95 % of subjects in the range of 4.25to 4.75 mm.19 However, there was no age limit for the study subjects and about 12.5% of study population was less than 16 years of age. This might explain the smaller ONSD reported in the Bangladeshi population as compared to the Pakistani population. Vaiman et al. conducted a study in Israeli population using CT or MRI due to better resolution power to determine the normal range of ONSD. They reported that the mean ONSD was 4.94± 1.51 mm in the right eye and 5.17 ± 1.34 mm in left eye.20 Amini et al reported that the mean ONSD in Irani population was 4.6 mm.17 The median ONSD reported by Wang et al in Chinese population was 5.1 mm.21
A few studies showed higher value of ONSD than previously described. Bauerle et al found mean ONSD of 5.4 mm with a range of 4.3 mm- 7.6 mm in German population.22 In this study he used ultrasound to measure ONSD. After a year he conducted another study and used MRI for measurement of ONSD and reported higher value of ONSD 5.69 ± 0.77 in Germans.23 Geeraerts et al also used MRI for ONSD measurement and found that ONSD was 5.08 ± 0.52 mm in healthy volunteersfrom Britain. He also showed that there was a good correlation between ultrasound and MRI measurement of ONSD 3 mm behind the pupils.24
The lowest ONSD of 3.4 mm was reported by Ballantyne et al but he actually measured optic nerve diameter rather than ONSD.25
LIMITATIONS
There are several limitations in this study. All the measurements on each subject were done by the primary investigator which could have introduced observer bias to the subsequent readings. In addition since the primaryinvestigator measured the ONSD in all subjects, the inter-observervariability could not be assessed in this study. The other limitations were that only 100 healthy volunteers were recruited from a single center of Pakistan which does not reflect the whole population of this country and the studywas conducted in adult healthy volunteers so the normal range of ONSD in pediatrics population could not be assessed.
CONCLUSION
95% of study sample have an ONSD less than 4.82 mm,measured by 7.5 MHz linear array ultrasoundprobe in horizontal plane and is independent of age, gender, height, weight and was similar in botheyes. ONSD more than 4.82 mm in this samplecan be considered abnormal and may reflect raised intracranial pressure.But in future larger studies are recommended to reflect the whole population of Pakistan.
Conflict of interest: None declared by the authors
Author responsibility/contribution:
AA: Protocol writing, data collection, analysis, manuscript writing
MH: Protocol reviewing, analysis, manuscript writing
AH: Data collection, manuscript writing
REFERENCES
- Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons, Joint Section on Neurotrauma, Critical Care, AANS/CNS, Bratton SL,Chestnut RM, et al. Guidelines for the management of severe traumatic brain injury. VI. Indications for intracranial pressure monitoring. J Neurotrauma. 2007;24(Suppl 1):S37–44.[PubMed]
- Morgenstern LB, Hemphill JC III, Anderson C, Becker K, Broderick JP, Connolly ES Jr, Greenberg SM, Huang JN, Mac-Donald RL, Messe´ SR, Mitchell PH, Selim M, Tamargo RJ, American Heart Association Stroke Council and Council on Cardiovascular Nursing. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2010;41:2108–29.[PubMed][Free full text]doi: 10.1161/STR.0b013e3181ec611b
- Helmke K, Hansen HC. Fundamentals of transorbital sonographic evaluation of optic nerve sheath expansion under intracranial hypertension. I. Experimental study. Pediatr Radiol. 1996;26:701–5.[PubMed]
- Mayer S, Chong JY. Critical care management of increased intracranial pressure. J Intensive Care Med. 2002;17:55–67.[Free full text]
- Ngo QN, Ranger A, Singh RN, Kornecki A, Seabrook JA, Fraser DD. External ventricular drains in pediatric patients. Pediatr Crit Care Med. 2009;10:346–51.[PubMed]doi:10.1097/PCC.0b013e3181a320cd.
- Ross IB, Dhillon GS. Ventriculostomy-related cerebral hemorrhages after endovascular aneurysm treatment. AJNR Am J Neuroradiol. 2003;24:1528–31.[PubMed][Free full text]
- The Brain Trauma Foundation. The American Association of Neurological Surgeons. The Joint Section on Neurotrauma and Critical Care. Indications for intracranial pressure monitoring. J Neurotrauma. 2000;17:479–91.[PubMed]
- Geeraerts T, Launey Y, Martin L, Pottecher J, Vigue´ B, Duranteau J, Benhamou D. Ultrasonography of the optic nerve sheath may be useful for detecting raised intracranial pressure after severe brain injury. Intensive Care Med. 2007;33:1704–11.[PubMed]
- Moretti R, Pizzi B. Optic nerve ultrasound for detection of intracranial hypertension in intracranial hemorrhage patients: confirmation of previous findings in a different patient population. J Neurosurg Anesthesiol. 2009;21(1):16–20.[PubMed]doi: 10.1097/ANA.0b013e318185996a.
- Moretti R, Pizzi B, Cassini F, Vivaldi N. Reliability of optic nerve ultrasound for the evaluation of patients with spontaneous intracranial hemorrhage. Neurocrit Care. 2009;11(3):406–10.[PubMed]doi: 10.1007/s12028-009-9250-8.
- Major R, Girling S, Boyle A .Ultrasound measurement of optic nerve sheath diameter in patients with a clinical suspicion of raised intracranial pressure. Emerg Med J. 2009;28:679–81.[PubMed][Free full text]doi: 10.1136/emj.2009.087353.
- Chen H, Ding GS, Zhao YC, Yu RG, Zhou JX. Ultrasound measurement of optic nerve diameter and optic nerve sheath diameter in healthy chinese adults. BMC Neurology 2015;15:106. [PubMed][Free full text] doi: 10.1186/s12883-015-0361-x.
- Vahedi K, Hofmeijer J, Juettler E, Vicaut E,George B, Algra A, et al. Early decompressive surgeryin malignant infarction of the middle cerebral artery: a pooledanalysis of three randomised controlled trials. Lancet Neurol 2007;6:215-22.[PubMed]
- Zhong J, Dujovny M, Park HK, Perez E, Perlin AR, Diaz FG.Advances in ICP monitoring techniques. Neurol Res 2003;25:339-50.[PubMed][Free full text]DOI:http://dx.doi.org/10.1179/016164103101201661
- Raboel PH, Bartak J, Andresen M, Bellander BM, Romner B. Intracranial pressure monitoring : Invasive versus non invasive methods- A review. Crit Care Res Pract.2012;2012:950393.[PubMed][Free full text]doi: 10.1155/2012/950393
- Liu D, Kahn M. Measurement and relationship of subarachnoidpressure of the optic nerve to intracranial pressure in fresh cadavers.Am J Ophthalmol 1993;116:548-56.[PubMed]
- Amini A, Kariman H, Ali Dolatabadi A, Hatamabadi HR, Derakhshanfar H, Mansouri B, et al. Use of the sonographic diameter of optic nerve sheath toestimate intracranial pressure. Am J Emerg Med 2013;31:236–239. [PubMed]doi: 10.1016/j.ajem.2012.06.025.
- Romagnuolo L, Tayal V, Tomaszewski C, Saunders T, Norton HJ. Optic nerve sheath diameter does not change with patient position. Am J Emerg Med. 2005;23:686–8.[PubMed]
- Maude RR, Hossain MA, Hassan MU, Osbourne S, Sayeed KL, Karim MR, et al. Transorbital sonographic evaluation of normal optic nerve sheath diameter in healthy volunteers in Bangladesh. PLoS ONE. 2013;8(12), e81013.[PubMed][Free full text]doi: 10.1371/journal.pone.0081013. eCollection 2013.
- Vaiman M, Gottlieb P, Bekerman I. Quantitative relations between the eyeball, the optic nerve, and the optic canal important for intracranial pressure monitoring. Head Face Med. 2014;10:32. [PubMed][Free full text]doi:10.1186/1746-160X-10-32.
- Wang L, Feng L, Yao Y, Wang Y, Chen Y, Feng J, et al. (2015) Optimal Optic Nerve Sheath Diameter Threshold for the Identification of Elevated Opening Pressure on Lumbar Puncture in a Chinese Population. PLoS ONE 10(2): e0117939. [PubMed][Full free text]doi:10.1371/journal.pone.0117939. eCollection 2015.
- Bauerle J, Lochner P, Kaps M, Nedelmann M. Intra- and interobsever reliability of sonographic assessment of the optic nerve sheath diameter in healthy adults. J Neuroimaging. 2012;22:42–5.[PubMed]doi: 10.1111/j.1552-6569.2010.00546.x.
- Bauerle J, Schuchardt F, Schroeder L, Egger K, Weigel M, Harloff A. Reproducibility and accuracy of optic nerve sheath diameter assessment using ultrasound compared to magnetic resonance imaging. BMC Neurol. 2013;13:187.[PubMed][Full free text]doi: 10.1186/1471-2377-13-187.
- Geeraerts T, Newcombe VF, Coles JP, Abate MG, Perkes IE, Hutchinson PJ, et al. Use of T2-weighted magnetic resonance imaging of the optic nerve sheath to detect raised intracranial pressure. Crit Care. 2008;12:R114.[PubMed][Free Full text]doi: 10.1186/cc7006.
- Ballantyne SA, O’Neill G, Hamilton R, Hollman AS. Observer variation in thesonographic measurement of optic nerve sheath diameter in normal adults.Eur J Ultrasound. 2002;15:45–9.[PubMed]