Martien Silviandy Setiawan 1 , Erwin Mulyawan 2 , Hori Hariyanto 3
Authors affiliations:
Adhesive capsulitis, commonly known as frozen shoulder, is a progressive painful condition characterized by limited active and passive range of motion (ROM) in all planes of glenohumeral joint movement due to inflammation, fibrosis, and capsular contracture. Frozen shoulder is divided into 3 main phases: freezing, frozen, and thawing. Conventional management of frozen shoulder often yields suboptimal results. Severe pain intensity can hinder the patient's rehabilitation process, necessitating innovative analgesic methods. A 50-year-old male with a history of frozen shoulder phase adhesive capsulitis for one month, experiencing rest pain VAS 6/10 and active movement pain VAS 9/10, had received conventional therapy including intra-articular steroid injections and nerve blocks with PRF. The patient experienced severe pain during rehabilitation, so a Continuous Interscalene Brachial Plexus Block (CISB) guided by ultrasound, connected to patient controlled analgesia (PCA) as an analgesic modality, was performed. Rehabilitation continued with passive and active shoulder manipulation. CISB with PCA represents a valuable analgesic strategy in adhesive capsulitis, allowing early physiotherapy and functional recovery when conventional therapies fail.
Abbreviations: AC: Adhesive capsulitis, CISB: Continuous Interscalene Block, PCA: patient controlled analgesia, ROM: range of motion,
Keywords : Adhesive Capsulitis, Continuous Interscalene Block (CISB), Frozen Shoulder, Pain Management, Patient Controlled Analgesia (PCA),
Citation: Setiawan MS, Mulyawan E, Hariyanto H. Frozen no more: conquering painful rehabilitation in refractory adhesive capsulitis through continuous interscalene block with PCA. Anaesth. pain intensive care 2026;30(3):380-383. DOI: 10.35975/apic.v30i3.3181
Received: December 2, 2025; Revised: January 11, 2026; Accepted: February 21, 2026
Adhesive capsulitis (AC), commonly known as frozen shoulder, is a musculoskeletal disorder characterised by progressive pain and restriction of both active and passive range of motion (ROM) in all planes of the glenohumeral joint, resulting from inflammation, fibrosis, and capsular contracture. The global prevalence is approximately 2–5% in the general population, with a female predominance (1.6:1) and a peak incidence between 40–60 years of age.1
Classically, AC progresses through three clinical stages: the freezing phase (2–9 months), dominated by progressive pain and gradual loss of motion; the frozen phase (4–12 months), where pain decreases but stiffness becomes predominant; and the thawing phase (12–42 months), characterised by gradual recovery of movement. The overall disease course may extend up to three years, and a subset of patients experience persistent functional deficits.1,2
Conventional management aims to relieve pain and restore function through physiotherapy and pharmacological therapy. However, severe pain, particularly in the freezing and early frozen phases, frequently hampers rehabilitation and delays recovery. Although oral analgesics, intra-articular corticosteroid injections, single-shot nerve blocks, and neuromodulation techniques such as pulsed radiofrequency have been employed, their analgesic effects on movement-related pain are often transient or inadequate. This perpetuates a pain–spasm–immobility cycle that limits participation in physiotherapy and contributes to chronic disability.2
Continuous interscalene block (CISB) combined with patient-controlled analgesia (PCA) represents an innovative analgesic approach in the management of pain in AC. By placing a perineural catheter around the C5–C7 roots of the brachial plexus, continuous local anaesthetic infusion can achieve sustained sensory blockade with minimal motor impairment.
Integration with PCA allows patients to titrate analgesia according to individual pain perception, promoting active participation and confidence during rehabilitation. This case report aims to evaluate the safety and efficacy of CISB-PCA through continuous catheter placement to facilitate effective rehabilitation for frozen shoulder.
A 50-year-old man with uncontrolled type 2 diabetes presented with progressive right shoulder pain and complete stiffness in all planes of motion for one year. He denied any history of trauma, fever, unexplained weight loss, or constitutional symptoms. No erythema, warmth, or swelling was noted. He denied any lumps in the joint. He has never had surgery before. Resting pain intensity was rated VAS 6/10, worsening to VAS 9/10 with movement. The pain did not improve with oral pharmacotherapy, leading to disruption of daily activities and a decrease in quality of life.
On physical examination, there was marked restriction of both active and passive movements: 15° flexion, 10° extension, 5° abduction, 10° external rotation, and 15° internal rotation. Special examination showed positive results for Neer's sign, Hawkins-Kennedy sign, and Empty Can test, while Yergason's and Speed's test were negative. Magnetic resonance imaging (MRI) of the right glenoid revealed thickening of the glenohumeral joint's axillary recess and inflammatory changed around the internal rotator cuff with glenohumeral joint effusion, while other structures are within normal limits. Therefore, a clinical and radiological diagnosis of right-sided AC in the frozen phase was made.
The patient had previously undergone suprascapular nerve pulsed radiofrequency (PRF) at 40°C, 45 V, 1 Hz, 40 ms for 120 seconds (two cycles), followed by ultrasound-guided intra-articular corticosteroid injections (triamcinolone acetonide 40 mg with 5 mL of 1% lidocaine into the glenohumeral joint, and 20 mg triamcinolone acetonide with 2 mL of 1% lidocaine into the subacromial bursa). Despite these interventions and a structured physiotherapy program, he experienced only partial relief of resting pain and persistent severe pain during movement, rendering rehabilitation ineffective. Strong oral pharmacodynamic combinations like tramadol remained unable to reduce the patient's extreme pain intensity during the medical rehabilitation process.
To facilitate effective medical rehabilitation, the Continuous Interscalene Block (CISB) technique with Patient Controlled Analgesia (PCA) was performed under ultrasound guidance. After the patient was positioned, anatomical landmarks, including the sternocleidomastoid, anterior scalene, and middle scalene muscles were identified. The brachial plexus roots appeared as a “cluster of grapes” on ultrasound (Figure I).
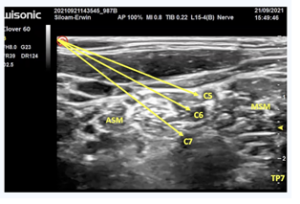
Figure I: Visualization of brachial plexus roots with "cluster of grapes" findings
A Contiplex catheter was inserted through an interscalene approach into the right brachial plexus, and confirmed by deltoid muscle contraction upon nerve stimulation at 0.4 mA (Figure 2).
An initial bolus of 10 mL of 0.25% bupivacaine was administered, followed by connection of the catheter to a PCA pump containing 0.125% bupivacaine (100 mL). The infusion settings included a basal rate of 2 mL/hour, a bolus of 2 mL, a lockout interval of 20 minutes, and a maximum dose of 10 mg/hour. Continuous monitoring was performed for potential complications such as phrenic nerve palsy and Horner syndrome.
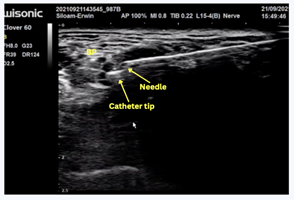
Figure 2: Placement of a CISB catheter tip using ultrasound
Following initiation of CISB with PCA, the patient experienced rapid and significant pain relief, enabling immediate initiation of active and passive shoulder mobilisations. During the first physiotherapy session, audible crepitus was noted during manipulation. Over ten days of therapy, the patient achieved remarkable improvement in ROM: flexion increased to 180°, extension to 60°, abduction to 90°, and both internal and external rotations to 90°, with minimal residual pain (VAS 2/10).
PCA use averaged 4–6 bolus demands daily, indicating sufficient efficacy for basal continuous infusion. The catheter was removed without complications and the patient continued physiotherapy with minimal analgesic requirements.
Effective physiotherapy is the cornerstone of AC management, but its success is contingent upon adequate pain control and patient compliance.¹ In the frozen phase, pain and stiffness significantly restrict shoulder movement, impeding rehabilitation and predisposing patients to persistent joint contractures.1,2
Therefore, regional anaesthesia techniques can serve as valuable adjuncts in such scenarios. Continuous interscalene brachial plexus block provides sustained analgesia to the shoulder region by continuous local anaesthetic infusion around the brachial plexus. Studies have demonstrated significant improvements in ROM, reduced pain scores, and decreased opioid requirements following CISB. This approach disrupts the pain–spasm–immobility cycle, mitigates central sensitisation, and facilitates early, pain-free mobilisation.3,4
CISB combined with PCA offers distinct advantages over single-injection or systemic analgesic methods. The continuous infusion ensures consistent analgesia, while the PCA component empowers patients to manage breakthrough pain autonomously.1 Low-concentration bupivacaine provides selective sensory blockade with minimal motor impairment, enabling intensive physiotherapy and early functional recovery.2
The use of CISB for frozen shoulder represents an innovative approach that opens a new paradigm by adapting postoperative analgesia techniques to facilitate non-surgical musculoskeletal rehabilitation. Recent studies support the application of CISB in refractory frozen shoulder. Ilango et al. and Ilfeld et al. reported enhanced postoperative ROM and superior analgesia with continuous interscalene infusion compared to single-shot blocks.3,4 Similarly, Malhotra et al. demonstrated that mobilisation under CISB achieved greater ROM gains than intra-articular corticosteroid injection, with mean flexion up to 150° and abduction up to 100°, while VAS pain scores dropped from 10 to between 0 and 2.5 Miyazaki et al. further confirmed that CISB accelerates postoperative recovery of shoulder mobility following capsulotomy.6
Beyond the analgesic effect, the integration of PCA promotes patient engagement and confidence in movement, both critical to the success of rehabilitation.7 By enabling patient-driven titration, CISB–PCA optimises comfort and psychological readiness for mobilisation. The present case exemplifies how adapting a perioperative analgesic strategy to a chronic musculoskeletal context can yield transformative functional outcomes in otherwise refractory AC.
4. CONCLUSION
Continuous interscalene brachial plexus block with patient-controlled analgesia represents an effective and safe analgesic strategy for refractory AC. It facilitates intensive physiotherapy and restores functional range of motion unattainable through conventional therapies, offering a promising adjunct in comprehensive pain management and rehabilitation.
Appreciation is also extended to the clinical and nursing teams involved in the perioperative care of the patient, whose collaboration contributed to the successful management and reporting of this case.
Authors affiliations:
- Martien Silviandy Setiawan, Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Pelita Harapan, Tangerang; Email; martiensetiawan09@gmail.com
- Erwin Mulyawan, Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Pelita Harapan, Tangerang; Email; erwin_mulys@yahoo.co.id
- Hori Hariyanto, Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Pelita Harapan, Tangerang; Email; horimd@yahoo.com
ABSTRACT
Adhesive capsulitis, commonly known as frozen shoulder, is a progressive painful condition characterized by limited active and passive range of motion (ROM) in all planes of glenohumeral joint movement due to inflammation, fibrosis, and capsular contracture. Frozen shoulder is divided into 3 main phases: freezing, frozen, and thawing. Conventional management of frozen shoulder often yields suboptimal results. Severe pain intensity can hinder the patient's rehabilitation process, necessitating innovative analgesic methods. A 50-year-old male with a history of frozen shoulder phase adhesive capsulitis for one month, experiencing rest pain VAS 6/10 and active movement pain VAS 9/10, had received conventional therapy including intra-articular steroid injections and nerve blocks with PRF. The patient experienced severe pain during rehabilitation, so a Continuous Interscalene Brachial Plexus Block (CISB) guided by ultrasound, connected to patient controlled analgesia (PCA) as an analgesic modality, was performed. Rehabilitation continued with passive and active shoulder manipulation. CISB with PCA represents a valuable analgesic strategy in adhesive capsulitis, allowing early physiotherapy and functional recovery when conventional therapies fail.
Abbreviations: AC: Adhesive capsulitis, CISB: Continuous Interscalene Block, PCA: patient controlled analgesia, ROM: range of motion,
Keywords : Adhesive Capsulitis, Continuous Interscalene Block (CISB), Frozen Shoulder, Pain Management, Patient Controlled Analgesia (PCA),
Citation: Setiawan MS, Mulyawan E, Hariyanto H. Frozen no more: conquering painful rehabilitation in refractory adhesive capsulitis through continuous interscalene block with PCA. Anaesth. pain intensive care 2026;30(3):380-383. DOI: 10.35975/apic.v30i3.3181
Received: December 2, 2025; Revised: January 11, 2026; Accepted: February 21, 2026
1. INTRODUCTION
Adhesive capsulitis (AC), commonly known as frozen shoulder, is a musculoskeletal disorder characterised by progressive pain and restriction of both active and passive range of motion (ROM) in all planes of the glenohumeral joint, resulting from inflammation, fibrosis, and capsular contracture. The global prevalence is approximately 2–5% in the general population, with a female predominance (1.6:1) and a peak incidence between 40–60 years of age.1
Classically, AC progresses through three clinical stages: the freezing phase (2–9 months), dominated by progressive pain and gradual loss of motion; the frozen phase (4–12 months), where pain decreases but stiffness becomes predominant; and the thawing phase (12–42 months), characterised by gradual recovery of movement. The overall disease course may extend up to three years, and a subset of patients experience persistent functional deficits.1,2
Conventional management aims to relieve pain and restore function through physiotherapy and pharmacological therapy. However, severe pain, particularly in the freezing and early frozen phases, frequently hampers rehabilitation and delays recovery. Although oral analgesics, intra-articular corticosteroid injections, single-shot nerve blocks, and neuromodulation techniques such as pulsed radiofrequency have been employed, their analgesic effects on movement-related pain are often transient or inadequate. This perpetuates a pain–spasm–immobility cycle that limits participation in physiotherapy and contributes to chronic disability.2
Continuous interscalene block (CISB) combined with patient-controlled analgesia (PCA) represents an innovative analgesic approach in the management of pain in AC. By placing a perineural catheter around the C5–C7 roots of the brachial plexus, continuous local anaesthetic infusion can achieve sustained sensory blockade with minimal motor impairment.
Integration with PCA allows patients to titrate analgesia according to individual pain perception, promoting active participation and confidence during rehabilitation. This case report aims to evaluate the safety and efficacy of CISB-PCA through continuous catheter placement to facilitate effective rehabilitation for frozen shoulder.
2. CASE REPORT
A 50-year-old man with uncontrolled type 2 diabetes presented with progressive right shoulder pain and complete stiffness in all planes of motion for one year. He denied any history of trauma, fever, unexplained weight loss, or constitutional symptoms. No erythema, warmth, or swelling was noted. He denied any lumps in the joint. He has never had surgery before. Resting pain intensity was rated VAS 6/10, worsening to VAS 9/10 with movement. The pain did not improve with oral pharmacotherapy, leading to disruption of daily activities and a decrease in quality of life.
On physical examination, there was marked restriction of both active and passive movements: 15° flexion, 10° extension, 5° abduction, 10° external rotation, and 15° internal rotation. Special examination showed positive results for Neer's sign, Hawkins-Kennedy sign, and Empty Can test, while Yergason's and Speed's test were negative. Magnetic resonance imaging (MRI) of the right glenoid revealed thickening of the glenohumeral joint's axillary recess and inflammatory changed around the internal rotator cuff with glenohumeral joint effusion, while other structures are within normal limits. Therefore, a clinical and radiological diagnosis of right-sided AC in the frozen phase was made.
The patient had previously undergone suprascapular nerve pulsed radiofrequency (PRF) at 40°C, 45 V, 1 Hz, 40 ms for 120 seconds (two cycles), followed by ultrasound-guided intra-articular corticosteroid injections (triamcinolone acetonide 40 mg with 5 mL of 1% lidocaine into the glenohumeral joint, and 20 mg triamcinolone acetonide with 2 mL of 1% lidocaine into the subacromial bursa). Despite these interventions and a structured physiotherapy program, he experienced only partial relief of resting pain and persistent severe pain during movement, rendering rehabilitation ineffective. Strong oral pharmacodynamic combinations like tramadol remained unable to reduce the patient's extreme pain intensity during the medical rehabilitation process.
To facilitate effective medical rehabilitation, the Continuous Interscalene Block (CISB) technique with Patient Controlled Analgesia (PCA) was performed under ultrasound guidance. After the patient was positioned, anatomical landmarks, including the sternocleidomastoid, anterior scalene, and middle scalene muscles were identified. The brachial plexus roots appeared as a “cluster of grapes” on ultrasound (Figure I).
Figure I: Visualization of brachial plexus roots with "cluster of grapes" findings
A Contiplex catheter was inserted through an interscalene approach into the right brachial plexus, and confirmed by deltoid muscle contraction upon nerve stimulation at 0.4 mA (Figure 2).
An initial bolus of 10 mL of 0.25% bupivacaine was administered, followed by connection of the catheter to a PCA pump containing 0.125% bupivacaine (100 mL). The infusion settings included a basal rate of 2 mL/hour, a bolus of 2 mL, a lockout interval of 20 minutes, and a maximum dose of 10 mg/hour. Continuous monitoring was performed for potential complications such as phrenic nerve palsy and Horner syndrome.
Figure 2: Placement of a CISB catheter tip using ultrasound
Following initiation of CISB with PCA, the patient experienced rapid and significant pain relief, enabling immediate initiation of active and passive shoulder mobilisations. During the first physiotherapy session, audible crepitus was noted during manipulation. Over ten days of therapy, the patient achieved remarkable improvement in ROM: flexion increased to 180°, extension to 60°, abduction to 90°, and both internal and external rotations to 90°, with minimal residual pain (VAS 2/10).
PCA use averaged 4–6 bolus demands daily, indicating sufficient efficacy for basal continuous infusion. The catheter was removed without complications and the patient continued physiotherapy with minimal analgesic requirements.
3. DISCUSSION
Effective physiotherapy is the cornerstone of AC management, but its success is contingent upon adequate pain control and patient compliance.¹ In the frozen phase, pain and stiffness significantly restrict shoulder movement, impeding rehabilitation and predisposing patients to persistent joint contractures.1,2
Therefore, regional anaesthesia techniques can serve as valuable adjuncts in such scenarios. Continuous interscalene brachial plexus block provides sustained analgesia to the shoulder region by continuous local anaesthetic infusion around the brachial plexus. Studies have demonstrated significant improvements in ROM, reduced pain scores, and decreased opioid requirements following CISB. This approach disrupts the pain–spasm–immobility cycle, mitigates central sensitisation, and facilitates early, pain-free mobilisation.3,4
CISB combined with PCA offers distinct advantages over single-injection or systemic analgesic methods. The continuous infusion ensures consistent analgesia, while the PCA component empowers patients to manage breakthrough pain autonomously.1 Low-concentration bupivacaine provides selective sensory blockade with minimal motor impairment, enabling intensive physiotherapy and early functional recovery.2
The use of CISB for frozen shoulder represents an innovative approach that opens a new paradigm by adapting postoperative analgesia techniques to facilitate non-surgical musculoskeletal rehabilitation. Recent studies support the application of CISB in refractory frozen shoulder. Ilango et al. and Ilfeld et al. reported enhanced postoperative ROM and superior analgesia with continuous interscalene infusion compared to single-shot blocks.3,4 Similarly, Malhotra et al. demonstrated that mobilisation under CISB achieved greater ROM gains than intra-articular corticosteroid injection, with mean flexion up to 150° and abduction up to 100°, while VAS pain scores dropped from 10 to between 0 and 2.5 Miyazaki et al. further confirmed that CISB accelerates postoperative recovery of shoulder mobility following capsulotomy.6
Beyond the analgesic effect, the integration of PCA promotes patient engagement and confidence in movement, both critical to the success of rehabilitation.7 By enabling patient-driven titration, CISB–PCA optimises comfort and psychological readiness for mobilisation. The present case exemplifies how adapting a perioperative analgesic strategy to a chronic musculoskeletal context can yield transformative functional outcomes in otherwise refractory AC.
4. CONCLUSION
Continuous interscalene brachial plexus block with patient-controlled analgesia represents an effective and safe analgesic strategy for refractory AC. It facilitates intensive physiotherapy and restores functional range of motion unattainable through conventional therapies, offering a promising adjunct in comprehensive pain management and rehabilitation.- Acknowledgement
Appreciation is also extended to the clinical and nursing teams involved in the perioperative care of the patient, whose collaboration contributed to the successful management and reporting of this case.
- Declaration of Consent
- Conflict of Interest
- Authors’ Contributions
9. REFERENCES
- Mariano ER, Loland VJ, Sandhu NS, Bishop ML, Bellars RH, Schwartz AJ, et al. Continuous interscalene brachial plexus block via an ultrasound-guided posterior approach: a randomized, triple-masked, placebo-controlled study. Anesth Analg. 2009;108(5):1688–94. PMCID: PMC2745838 DOI: 1213/ane.0b013e318199dc86
- Genc C, Tulgar S, Unal M, Genc AS, Kehribar L, Erdivanli B, et al. The minimum effective concentration (MEC90) of bupivacaine for an ultrasound-guided suprainguinal fascia iliaca compartment block for analgesia in knee surgery: a dose-finding study. Korean J Anesthesiol. 2024;77(3):364–73. PMCID: PMC11150113 DOI: 4097/kja.23710
- Ilango B, Subramanian V, Kumar A, Prasad J. Arthroscopic capsular release and continuous upper arm brachial block in resistant frozen shoulder. J Orthop. 2020;23:123–9. PMCID: PMC7494934 DOI: 1016/j.jor.2020.08.033
- Malhotra N, Garg B, Sahu D, Mehta N, Kotwal P. Continuous interscalene nerve block following adhesive capsulitis manipulation. Reg Anesth Pain Med. 2013;38(2):125–9. PMCID: PMC3578220 DOI: 1097/AAP.0b013e318283475b
- Ilfeld BM, Moeller LK, Mariano ER. Outcomes of mobilization under continuous interscalene block versus mobilization and intraarticular steroid injection in frozen shoulder. J Clin Orthop Trauma. 2022;25:101680.
- Miyazaki AN, Fregoneze M, Santos PD, Doneux PS, Silva LA, Andrade AL, et al. Clinical results of shoulder manipulation under ultrasound-guided cervical nerve root block in frozen shoulder. J Shoulder Elbow Surg. 2016;25(12):1937–43. DOI:1007/s40122-018-0109-6
- Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth. 2001;87(1):36–46. DOI: 10.1093/bja/87.1.36