Nguyen Sinh Hien 1 , Ngo Van Thanh 2 , Nguyen Hong Hanh 3 , Dinh Cong Pho 4
Authors affiliations:
Background: Postoperative delirium complicates up to one-quarter of cardiac surgery patients and increases morbidity and mortality. In this study, we determine the incidence and risk factors of postoperative delirium after cardiac surgery and develop and internally validate a multivariable risk prediction model for postoperative delirium.
Methods: In this prospective observational study, 158 adults undergoing cardiac surgery were enrolled. Delirium was assessed daily for five days using CAM-ICU, RASS, and ICDSC. Univariate predictors (P < 0.05) entered multivariate logistic regression. Model discrimination was assessed by ROC analysis; internal validity by 500-sample bootstrapping and ten-fold cross-validation.
Results: The mean of age was 60.4 ± 10.8 years and 53.2% wass female. Delirium occurred in 38 patients (24.1%), peaking on day 1 (15.2%), with hyperactive subtype in 91.7%. Univariate risk factors: female gender (73.7% vs 15.6%, P = 0.004), minimally invasive surgery (44.2% vs 20.0%, P < 0.001), mechanical ventilation (36.7±34.3 vs 28.7±20.9 h, P = 0.002), sedation (32.3±31.7 vs 19.7±16.7 h, P < 0.001), propofol (25.9±20.1 vs 14.2±9.1 h, P < 0.001), infection (42.1% vs 24.2%, P = 0.033), stroke (18.4% vs 5.3%, P = 0.009). Multivariate independent predictors: Female gender (OR 2.68; P = 0.048; AUC 0.635; P = 0.012); Minimally invasive surgery (OR 4.14; P = 0.005; AUC 0.650; P = 0.005); Propofol duration per hour (OR 1.07; P = 0.011; AUC 0.747; P < 0.001); Postoperative infection (OR 3.45; P = 0.046; AUC 0.590; P = 0.096). Apparent model (female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection) AUC was 0.828 (95% CI 0.759–0.897; P < 0.001). Bootstrap mean optimism was 0.038, yielding an optimism-corrected AUC of 0.790. Ten-fold cross-validation produced a mean AUC of 0.79 ± 0.04.
Conclusions: Postoperative delirium affects nearly one-quarter of cardiac surgery patients. A prognostic model including female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection demonstrates robust discrimination (optimism-corrected AUC 0.790) and internal stability. Implementation may enable early risk stratification and optimization of sedation and infection-prevention protocols.
Keywords: Delirium; Cardiac Surgery; Prognostic Model
Citation: Hien NS, Thanh NV, Hanh HH, Pho DC. Prognostic model for delirium after cardiac surgery: insights from a surgical intensive care unit in a tertiary heart center. Anaesth. pain intensive care 2026;30(3):291-300. DOI: 10.35975/apic.v30i3.3163
Received: February 07, 2026; Revised: March 15, 2026; Accepted: March 15, 2026
Postoperative delirium (POD) is a common and serious complication after cardiovascular surgery, with acute neuropsychiatric syndrome marked by fluctuating disturbances in attention, awareness, and cognition. According to The American Psychiatric Association’s fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 1 delirium is defined as a condition with five key features: a disturbance in attention and awareness; this disturbance only occurs from hours to a few days; it represents a change from baseline attention and awareness, and it usually fluctuates in severity depending on the time of the day. Delirium also may express itself as an disturbance in cognition (e.g., memory deficit, disorientation, language, visuospatial ability, or perception). These changes in mental status are not explained by other pre-existing, established, or evolving neurocognitive disorders and do not occur in the context of a severely reduced level of arousal, such as a coma. Also, these do not relate to the side effects of other medical conditions, substance intoxication or withdrawal (i.e., due to drug abuse or a medication), exposure to a toxin, or are due to multiple etiologies.
Postoperative delirium is a frequent and serious complication among adults undergoing cardiac surgery, with reported incidences commonly ranging from about one-fifth to one-quarter of patients in contemporary cohorts. This syndrome is associated with prolonged mechanical ventilation and intensive care unit (ICU) stay, increased hospital length of stay and costs, higher rates of non-home discharge, and both short- and long-term mortality. Beyond its immediate impact on recovery, postoperative delirium is linked to persistent cognitive decline and impaired quality of life, underscoring its importance as a major perioperative brain health issue in cardiac surgical practice. 2.3
The pathophysiology of delirium after cardiac surgery is multifactorial, involving patient vulnerability, perioperative hemodynamic and inflammatory insults, and modifiable factors such as sedation strategies and infection. Numerous clinical and procedural risk factors have been described, including advanced age, pre-existing cognitive or cerebrovascular disease, complex surgery with cardiopulmonary bypass, prolonged mechanical ventilation, and postoperative complications. However, delirium remains under-recognized in routine care, and systematic screening with validated tools is not uniformly implemented in many surgical intensive care units.2,4,5
Several prediction models for postoperative delirium have been proposed, but many were developed in mixed surgical or noncardiac populations, use heterogeneous delirium definitions, or lack robust validation in contemporary cardiac surgery cohorts. Moreover, few models specifically incorporate perioperative factors that are potentially modifiable in the cardiac surgical ICU, such as minimally invasive surgical approaches, depth and duration of sedative exposure, and postoperative infection. A pragmatic, well-calibrated prognostic model tailored to the cardiac surgery population could therefore support early risk stratification, guide preventive bundles, and optimize sedation and infection-prevention protocols in high-risk patients. 6,7
Despite peri-operative advancements, including both surgical and anesthetic, delirium is a frequent post cardiac surgery complication. Delirium is a common menace in the cardiac surgical ICU and outcome consequences of greater number of morbidity and mortality. Recent research has identified possible hazards for the occurrence of delirium and strategies to treat it. However, more studies are required to standardize the risk factors, its occurrence and treatment strategies in post cardiac surgical patients. 8
In this context, the present study aimed to develop and internally validate a multivariable prognostic model for delirium after cardiac surgery, using prospectively collected data from adults admitted to the surgical intensive care unit of a tertiary heart center. The model focuses on readily available preoperative and perioperative variables, including sex, surgical approach, sedative exposure, and postoperative complications, to facilitate bedside application and inform targeted delirium prevention strategies in routine clinical practice.
2.1. Study design
In this prospective observational study, 158 adults undergoing cardiac surgery were enrolled. Delirium was assessed daily for five days using CAM-ICU, RASS, and ICDSC. Univariate predictors (P < 0.05) entered multivariate logistic regression. Model discrimination was assessed by ROC analysis; internal validity by 500-sample bootstrapping and ten-fold cross-validation.
This study was conducted at the Surgical Cardiac Intensive Care Unit at Hanoi Heart Hospital, Vietnam, between May 2025 and August 2025, as an prospective observational study involving adult patients aged 18 y and above, who underwent cardiac surgery with cardiopulmonary bypass. Consent to participate in the study was obtained from each patient before surgery. Details were shown in study flowchart (Figure 1).
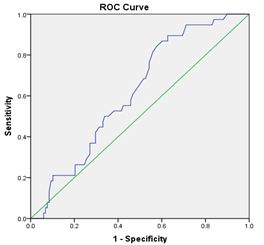
Figure 1: The optimal cut-off value for cardiopulmonary bypass (CPB) time
Exclusion criteria included: Patients with conditions that hindered delirium assessment using the CAM-ICU, such as dementia or deafness, as well as those with severe complications like stroke or who expired during the study, were excluded from the study. The existence of delirium before surgery also excluded the patient from the study.
The sample size was primarily determined using a formula for estimating a single proportion, based on the expected incidence of postoperative delirium in cardiac surgery patients and a predefined margin of error. For the prognostic model, we additionally adhered to the commonly recommended rule of at least 10 events per variable (EPV) to reduce the risk of overfitting. With 38 delirium events, the final multivariable model was therefore restricted to four predictors, maintaining an EPV of approximately 9–10.
2.2. Anesthesia, surgery and intensive care
All the patients received standard care, including an examination one-day before their surgery to take their history and evaluate their physical, mental, and cognitive status. All patients received general anesthesia; induction by midazolam, etomidate, fentanyl and rocuronium, and maintenance of anesthesia with TCI propofol, fentanyl and rocuronium, in combination with sevoflurane or isoflurane inhalation. The depth of anesthesia was maintained using both clinical signs (hemodynamic responses, pupil size, and patient movement) and continuous bispectral index (BIS) monitoring. Anesthetic dosing was adjusted to maintain a target BIS range of 40–60 during surgery. They also received tranexamic acid and prophylactic antibiotics. Heparin was used to stop blood clot formation during cardiopulmonary bypass (CPB), and protamine sulphate was used to reverse the heparin’s effects after CPB stopped. These drugs were used according to ACT guidelines during surgery. The pump flow rate in running CPB was between 2.4 and 2.8 L/min/m2; mean blood pressure was maintained between 60 and 90 mmHg, and mild hypothermia was induced at 33 °C and 35 °C. After surgery, the patient was transferred to the recovery room, sedated with midazolam and fentanyl, and extubated when all criteria were met.
Postoperative analgesia included intravenous using morphine or erector spinae plane (ESP) nerve block using ropivacaine through catheter for the first three days postoperatively, combined with other pain relievers such as paracetamol and nonsteroidal anti-inflammatory drugs.
As part of the study, questionnaires, physical tests, and medical records, were used to get information about the patients. This included demographic information, e.g., age, gender, ASA physical status classification system, and medical histories like hypertension, cerebrovascular accident, diabetes, and history of alcohol abuse. Operative time, CPB time, aortic cross-clamp time, and number of drainages were noted. After surgery, number of days using Propofol, opioids, mechanical ventilation duration, occurrence of acute renal failure and blood transfusion after surgery were recorded.
Postoperative pain was managed according to a standardized analgesic protocol. This included titrated intravenous morphine, combined with scheduled paracetamol with or without nonsteroidal anti‑inflammatory drugs (NSAIDs), as clinically appropriate. Pain intensity was assessed using the Numeric Rating Scale (NRS) every 4 hours, and analgesic doses were adjusted accordingly.
2.3. Delirium assessment
Delirium was assessed once daily for the first five postoperative days in the surgical intensive care unit using validated instruments recommended for critically ill adults. Postoperative delirium was assessed once daily at a fixed time, at 8:00 a.m. ± 1 hour, using a standardized delirium screening protocol. All assessments were performed by trained ICU staff who were familiar with the use of the delirium assessment tool, in order to enhance consistency and reduce interobserver variability. At each assessment, level of consciousness was first evaluated with the Richmond Agitation–Sedation Scale (RASS); patients with deep sedation (RASS −4 or −5) were not evaluated for delirium and were reassessed when arousal improved. Delirium screening was then performed with the Confusion Assessment Method for the Intensive Care Unit (CAM‑ICU), which has high specificity for ICU delirium, and the Intensive Care Delirium Screening Checklist (ICDSC), which captures a spectrum from subsyndromal to full‑syndrome delirium based on symptoms observed over the preceding 24 hours. For each study day, the presence of delirium was defined as a positive CAM‑ICU assessment and/or an ICDSC score at or above the conventional diagnostic threshold (≥4), and delirium subtype (hyperactive, hypoactive, mixed) was categorized according to concurrent RASS scores. All assessments were performed by physicians or nurses who had completed standardized training in the use of RASS, CAM‑ICU, and ICDSC prior to study initiation.
2.4. Statistical analysis
The data were analyzed using SPSS 20.0 software. Quantitative variables were described as mean and standard deviation (X̄, SD). The two mean values were compared using the t-test for standard variables and the Mann-Whitney U test for non-standard variables. Qualitative variables were described as numbers (n) and percentages and tested using the chi-squared test. Odds ratios (ORs) were calculated to show the effect size of perioperative risk factors. Then, the statistically significant risk factors after univariate analysis (P < 0.05) were entered into a logistic multivariable regression model, which was based on the model's fit (Hosmer & Lemeshow Test P > 0.05) to find the most powerful model. The normality of continuous variables was assessed using the Shapiro–Wilk test. Variables that did not follow a normal distribution were compared between groups using the Mann–Whitney U test. The difference was considered statistically significant at P < 0.05.
There were 158 eligible patients enrolled in the study. The incidence of postoperative delirium: There were 38 cases of delirium, accounting for 24.1%.
Table 1 showed the rate of delirium by day. On postoperative day 0, delirium was identified in 8.9% of patients, rising to 15.2% on day 1. The majority of new cases occurred within the first two days. By day 5, the delirium rate declined to 7.7%, and the overall incidence during hospitalization was 24.1%.
Table 2 showed the types of delirium by day. Of the 158 patients, hyperactive delirium was the predominant subtype across all days, peaking at 22 cases on day 1. Hypoactive delirium remained rare, with only 1–2 cases daily, and no mixed-type delirium was observed throughout the study period. The incidence of total delirium was highest on day 1 (24 cases) and decreased thereafter. Table 3 showed the interventions and supportive measures for delirium. Among patients with delirium, intravenous sedation was administered in 57.9%, haloperidol in 92.1%, and oral antipsychotics in 34.2%. Mechanical ventilation was required in 36.8% of cases, and 94.7% underwent physical restraint. The majority of delirium cases resolved within one day (60.5%) as shown in Table 4. Treatment lasted two days in 26.3% of cases and three or more days for the remainder, with just one patient each requiring four to six days for recovery.
Table 5 showed the main patient characteristics and the results of the univariate analysis. Patients who got delirium were much older and more likely to be female than those who didn't get it (P = 0.004). In the delirium group, valvular heart disease and vascular disease were much more common than in the other groups (P = 0.044 and P = 0.050, respectively). There were more patients in the delirium group who had minimally invasive
surgery (p < 0.001). Patients with delirium exhibited significantly prolonged ventilator durations (P = .002) and extended sedative administration periods (p < 0.001), especially with propofol (p < 0.001). Patients who developed delirium also had a higher risk of getting
an infection after surgery (P = 0.033) and having a stroke during or after surgery (P = .009). There were no significant differences between groups in terms of anesthesia duration, cardiopulmonary bypass duration, or comorbidities including hypertension, diabetes, and coronary artery disease. The two patients in Table 5 without cardiopulmonary bypass (CPB) underwent minimally invasive cardiac procedures that did not require extracorporeal circulation but otherwise met all inclusion criteria.
Receiver operating characteristic (ROC) curve showing the area under the curve (AUC) and the best cut-off value for cardiopulmonary bypass (CEC) time in predicting the outcome (Figure 2). The AUC was 0.619, which means it had a small but clinically important ability to tell the difference between groups (P = 0.028). The best cut-off point (Y = 0.268) was a CEC duration of 95 minutes, which gave a sensitivity of 89.5% and a specificity of 62.7%. Receiver operating characteristic (ROC) curve showing the area under the curve (AUC) and the best cut-off point for how long propofol sedation should last to predict the outcome (Figure 2). The AUC was 0.747, which means it was able to tell the difference between the two groups well (P < 0.001). The best cut-off point (Y = 0.38) was 15.5 hours of propofol sedation, which gave a sensitivity of 76.3% and a specificity of 38.3%.
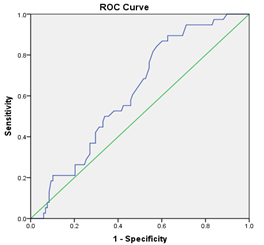
Figure 2 : The optimal cut-off value for propofol sedation duration in predicting the outcome
Table 6 shows that, in the multivariate logistic regression model, female gender (OR 2.68, 95% CI 1.01–7.14, P = 0.048), minimally invasive surgery (OR 4.14, 95% CI 1.54–11.13, P = 0.005), longer propofol sedation duration (OR 1.07 per hour, 95% CI 1.02–1.14, P = 0.011), and postoperative infection (OR 3.45, 95% CI 1.02–11.68, P = 0.046) were independently associated with an increased risk of delirium. In contrast, total sedation duration, mechanical ventilation duration, and perioperative stroke did not remain significantly associated with delirium after adjustment for other covariates (all P-value > 0.05). The apparent model showed in Figure 3 (female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection) demonstrated good discrimination, with an AUC of 0.828 (95% CI 0.759–0.897; P < 0.001). After internal validation using bootstrap resampling, the mean optimism was 0.038, yielding an optimism-corrected AUC of 0.790. Consistent performance was observed with ten-fold cross-validation, which produced a mean AUC of 0.79 ± 0.04.
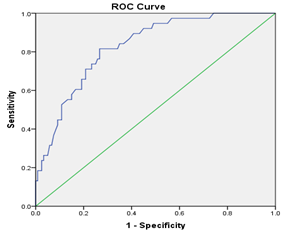
Figure 3: The apparent model (female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection) of prediction
POD is associated with, prolonged ICU stay, long-term cognitive decline, and increased mortality. Monitoring and diagnosis are mainly based on standardized tools such as CAM-ICU, ICDSC. Management, care and treatment are a combination of medication, care and safety measures with significant effectiveness. Patients were prospectively screened from day one to day ten after surgery or until hospital discharge. 9 The duration of mechanical ventilation and ICU length of stay were longer in the group of patients with delirium (10.6 hours (6.6, 19.5) vs 6.4 hours (4.9, 8.6), P < 0.001, and 1.7 days (0.9, 4.2) vs 0.9 days (0.9, 1), P < 0.001). 10 A total of 158 eligible adult patients undergoing cardiac surgery were enrolled in the study. During the index hospitalization, 38 patients developed postoperative delirium, corresponding to an overall incidence of 24.1%, which is within the range reported in contemporary cardiac surgery cohorts
A total of 158 eligible adult patients undergoing cardiac surgery were enrolled in the study. During the index hospitalization, 38 patients developed postoperative delirium, corresponding to an overall incidence of 24.1%, which is within the range reported in contemporary cardiac surgery cohorts. 2 Delirium manifested early in the postoperative period. Delirium was detected in 8.9% of patients on postoperative day (POD) 0, rising to 15.2% on POD 1. Most new cases of delirium happened within the first two days after surgery. This is in line with previous reports that delirium after cardiac surgery most often happens in the first few days in the intensive care unit. The daily rate of delirium peaked on POD 1 and then steadily dropped, reaching 7.7% by POD 5. 4,11 The cumulative incidence of postoperative delirium during the entire hospitalization was 24.1%, suggesting that roughly one in four patients experienced at least one episode of delirium following cardiac surgery. This burden is comparable to that observed in recent cardiac surgery series and underscores delirium as a frequent neuropsychiatric complication in this population. 4,11
Among the 158 patients enrolled, hyperactive delirium was the predominant subtype throughout the postoperative period. This type of delirium reached its highest point on the first day after surgery, with 22 cases. This was the same day that the overall number of delirium cases reached its highest point (24 cases). Conversely, hypoactive delirium was rarely observed, with merely 1–2 cases recorded daily, and no instances of mixed-type delirium were documented throughout the study period. These findings align with previous reports emphasizing the prevalence of hyperactive delirium, particularly in the immediate postoperative phase following cardiac surgery, whereas hypoactive delirium frequently goes unrecognized unless specifically evaluated by seasoned clinicians utilizing standardized instruments. 12,13 The daily rate of total delirium decreased after day 1, reflecting the typical clinical course described in contemporary literature. 14
Table 3 shows a summary of the treatments and support given to patients who had postoperative delirium. Intravenous sedation was utilized in 57.9% of delirious patients, haloperidol in 92.1%, and oral antipsychotic agents in 34.2%, indicating a primarily pharmacological management approach aligned with standard ICU delirium protocols. 15,16 Mechanical ventilation was necessary in 36.8% of delirium cases, and physical restraints were utilized in 94.7% of patients, highlighting that agitation and the risk of self-harm or device removal were prevalent clinical issues in this group. 17
Protocol-based care for delirium was utilized in 86.8% of affected patients, primarily to improve patient safety and standardize management. This protocol was implemented uniformly in patients both with and without mechanical ventilation, indicating that structured delirium care pathways were integrated throughout the range of respiratory support. No additional or alternative protocols beyond the standard delirium management pathway were required during the study period. 15,17,18
Most cases of postoperative delirium went away quickly; 60.5% of the patients who had it were completely better within one day of the onset (Table 4). In 26.3% of cases, delirium needed two days of treatment. Only a small number of patients had it for three or more days; in fact, only one patient needed four, five, or six days to fully recover. This temporal pattern of delirium resolution aligns with prior studies in cardiac surgery cohorts, which show that delirium most often develops early postoperatively and is typically of short duration, especially when timely detection and targeted management strategies are implemented. 19 Rapid recovery rates may reflect both the effectiveness of standard ICU protocols and the predominance of hyperactive delirium, which is usually more responsive to supportive and pharmacological interventions. 15
Table 5 presents the baseline and perioperative characteristics according to delirium status, together with the results of the univariate analysis. Patients who developed postoperative delirium were significantly older and more frequently female than those who did not, consistent with previous work identifying advanced age and female sex as important vulnerability factors for delirium after cardiac surgery. 20 Valvular heart disease and vascular disease were also more prevalent among patients with delirium, suggesting that underlying structural heart disease and systemic vascular pathology may contribute to increased susceptibility. 2,21
Procedural and postoperative factors showed clear differences between groups. Minimally invasive surgery was more common in the delirium group, and patients who developed delirium had significantly longer durations of mechanical ventilation, total sedative exposure, and propofol infusion, in line with prior evidence that prolonged ventilatory support and sedative use are associated with higher delirium risk. In addition, postoperative infection and perioperative stroke occurred more frequently in the delirium group, corroborating reports that inflammatory and neurologic complications are important precipitants of delirium in cardiac surgery populations. By contrast, there were no significant between-group differences in anesthesia time, cardiopulmonary bypass duration, or common comorbidities such as hypertension, diabetes, and coronary artery disease, indicating that, in this cohort, these factors did not independently distinguish patients who developed delirium from those who did not. 21,22
Table 6 summarizes the multivariate logistic regression analysis evaluating independent predictors of postoperative delirium. After adjusting for other factors, being female (OR 2.68, 95% CI 1.01–7.14, P = 0.048), having minimally invasive surgery (OR 4.14, 95% CI 1.54–11.13, P = 0.005), having longer propofol sedation (OR 1.07 per hour, 95% CI 1.02–1.14, P = 0.011), and having an infection after surgery (OR 3.45, 95% CI 1.02–11.68, P = 0.046) were all still linked to a higher risk of delirium. These findings indicate that both patient-related factors (sex) and modifiable perioperative factors (surgical approach, sedative exposure, and infection) contributed meaningfully to delirium risk in this cohort, consistent with contemporary multivariable models in cardiac surgery populations. 4,23,24 Conversely, total sedation duration, mechanical ventilation duration, and perioperative stroke failed to maintain statistical significance in the fully adjusted model (all p > 0.05). This indicates that their associations with delirium, identified in univariate analyses, may be mediated or confounded by other variables included in the study. This pattern is similar to what other studies have found, where some perioperative factors lose significance after taking into account a mix of demographic, surgical, and postoperative complications. This shows how important it is to use multivariable adjustment when looking for independent predictors of delirium. 7,22,25 In our study, longer duration of postoperative propofol sedation was identified as an independent predictor of delirium. However, this association should be interpreted with caution. The duration of propofol exposure likely reflects greater overall illness severity, more complex or prolonged surgery, and a higher need for postoperative mechanical ventilation and sedation, rather than a purely causal effect of propofol itself. Furthermore, reverse causation is possible, as patients who became agitated or delirious often required escalation or prolongation of sedative therapy, which could artificially strengthen the association between propofol duration and delirium. We therefore consider propofol duration to be a marker of high‑risk patients and intensive postoperative care, rather than a modifiable pharmacologic trigger of delirium per se.
The prognostic model combining female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection showed good discriminative performance for predicting postoperative delirium. The apparent model yielded an AUC of 0.828 (95% CI 0.759–0.897; p < 0.001), indicating strong ability to distinguish between patients who did and did not develop delirium, and falling within or above the range reported for other cardiovascular surgery delirium prediction tools. 26,27 After internal validation using bootstrap resampling, the mean optimism in model performance was modest (0.038), yielding an optimism-corrected AUC of 0.790. This indicates good discrimination and suggests limited overfitting, despite the relatively small single-center cohort. Ten-fold cross-validation yielded consistent results, with a mean AUC of 0.79 ± 0.04, demonstrating the model's internal stability and robustness across various data partitions, in accordance with current standards for clinically relevant prediction models in perioperative delirium research. 26,27
Limitations of study
We acknowledge several limitations of our study, including its single‑center design, the relatively modest sample size, the once‑daily assessment of delirium, and the potential for residual confounding.
Postoperative delirium affects nearly one-quarter of cardiac surgery patients. A prognostic model including female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection demonstrates robust discrimination (optimism-corrected AUC 0.790) and internal stability. Implementation may enable early risk stratification and optimization of sedation and infection-prevention protocols.
IRB approval
We conducted this study in compliance with the principles of the Declaration of Helsinki. The study’s protocol was reviewed and approved by the Hanoi Heart Hospital Ethical Review Board (No. 1741/BVT-GCNHĐĐĐ dated on May 8th 2025). Written informed consent was obtained from all patients before surgery.
Data availability
The numerical data generated in the conduct of this study are available with the corresponding author.
Conflict of interest
The authors made no declarations regarding potential conflicts.
Funding
No external or industry funding was involved in this study.
Acknowledgments
We gratefully thank the colleagues and staff in the operating theater and cardiac intensive care unit for their cooperation in data collection.
Authors’ contribution
N.S.H. and N.V.T. conceptualized the study. N.V.T., N.H.H., and D.C.P. collected the data. D.C.P. and N.V.T. performed the formal analysis. N.S.H., D.C.P., and N.V.T. wrote the original draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Authors affiliations:
- Nguyen Sinh Hien, Cardiovascular Surgery Department, Hanoi Heart Hospital, No. 92 Tran Hung Dao Street, Cua Nam Ward, Hanoi, Vietnam; Email: nguyensinhhien@timhanoi.vn
- Ngo Van Thanh, Cardiovascular Surgery Intensive Care Unit, Hanoi Heart Hospital, No. 92 Tran Hung Dao Street, Cua Nam Ward, Hanoi Capital, Vietnam; Email: ngovanthanh@timhanoi.vn
- Nguyen Hong Hanh, Cardiovascular Surgery Intensive Care Unit, Hanoi Heart Hospital, No. 92 Tran Hung Dao Street, Cua Nam Ward, Hanoi, Vietnam; Email: unconditionallove2011@yahoo.com
- Dinh Cong Pho, Department of Cardiology, Heart Institute, 108 Military Central Hospital, No. 1 Tran Hung Dao, Hanoi, Vietnam; Email: dinhcongphohvqy@gmail.com
ABSTRACT
Background: Postoperative delirium complicates up to one-quarter of cardiac surgery patients and increases morbidity and mortality. In this study, we determine the incidence and risk factors of postoperative delirium after cardiac surgery and develop and internally validate a multivariable risk prediction model for postoperative delirium.
Methods: In this prospective observational study, 158 adults undergoing cardiac surgery were enrolled. Delirium was assessed daily for five days using CAM-ICU, RASS, and ICDSC. Univariate predictors (P < 0.05) entered multivariate logistic regression. Model discrimination was assessed by ROC analysis; internal validity by 500-sample bootstrapping and ten-fold cross-validation.
Results: The mean of age was 60.4 ± 10.8 years and 53.2% wass female. Delirium occurred in 38 patients (24.1%), peaking on day 1 (15.2%), with hyperactive subtype in 91.7%. Univariate risk factors: female gender (73.7% vs 15.6%, P = 0.004), minimally invasive surgery (44.2% vs 20.0%, P < 0.001), mechanical ventilation (36.7±34.3 vs 28.7±20.9 h, P = 0.002), sedation (32.3±31.7 vs 19.7±16.7 h, P < 0.001), propofol (25.9±20.1 vs 14.2±9.1 h, P < 0.001), infection (42.1% vs 24.2%, P = 0.033), stroke (18.4% vs 5.3%, P = 0.009). Multivariate independent predictors: Female gender (OR 2.68; P = 0.048; AUC 0.635; P = 0.012); Minimally invasive surgery (OR 4.14; P = 0.005; AUC 0.650; P = 0.005); Propofol duration per hour (OR 1.07; P = 0.011; AUC 0.747; P < 0.001); Postoperative infection (OR 3.45; P = 0.046; AUC 0.590; P = 0.096). Apparent model (female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection) AUC was 0.828 (95% CI 0.759–0.897; P < 0.001). Bootstrap mean optimism was 0.038, yielding an optimism-corrected AUC of 0.790. Ten-fold cross-validation produced a mean AUC of 0.79 ± 0.04.
Conclusions: Postoperative delirium affects nearly one-quarter of cardiac surgery patients. A prognostic model including female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection demonstrates robust discrimination (optimism-corrected AUC 0.790) and internal stability. Implementation may enable early risk stratification and optimization of sedation and infection-prevention protocols.
Keywords: Delirium; Cardiac Surgery; Prognostic Model
Citation: Hien NS, Thanh NV, Hanh HH, Pho DC. Prognostic model for delirium after cardiac surgery: insights from a surgical intensive care unit in a tertiary heart center. Anaesth. pain intensive care 2026;30(3):291-300. DOI: 10.35975/apic.v30i3.3163
Received: February 07, 2026; Revised: March 15, 2026; Accepted: March 15, 2026
1. INTRODUCTION
Postoperative delirium (POD) is a common and serious complication after cardiovascular surgery, with acute neuropsychiatric syndrome marked by fluctuating disturbances in attention, awareness, and cognition. According to The American Psychiatric Association’s fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 1 delirium is defined as a condition with five key features: a disturbance in attention and awareness; this disturbance only occurs from hours to a few days; it represents a change from baseline attention and awareness, and it usually fluctuates in severity depending on the time of the day. Delirium also may express itself as an disturbance in cognition (e.g., memory deficit, disorientation, language, visuospatial ability, or perception). These changes in mental status are not explained by other pre-existing, established, or evolving neurocognitive disorders and do not occur in the context of a severely reduced level of arousal, such as a coma. Also, these do not relate to the side effects of other medical conditions, substance intoxication or withdrawal (i.e., due to drug abuse or a medication), exposure to a toxin, or are due to multiple etiologies.
Postoperative delirium is a frequent and serious complication among adults undergoing cardiac surgery, with reported incidences commonly ranging from about one-fifth to one-quarter of patients in contemporary cohorts. This syndrome is associated with prolonged mechanical ventilation and intensive care unit (ICU) stay, increased hospital length of stay and costs, higher rates of non-home discharge, and both short- and long-term mortality. Beyond its immediate impact on recovery, postoperative delirium is linked to persistent cognitive decline and impaired quality of life, underscoring its importance as a major perioperative brain health issue in cardiac surgical practice. 2.3
The pathophysiology of delirium after cardiac surgery is multifactorial, involving patient vulnerability, perioperative hemodynamic and inflammatory insults, and modifiable factors such as sedation strategies and infection. Numerous clinical and procedural risk factors have been described, including advanced age, pre-existing cognitive or cerebrovascular disease, complex surgery with cardiopulmonary bypass, prolonged mechanical ventilation, and postoperative complications. However, delirium remains under-recognized in routine care, and systematic screening with validated tools is not uniformly implemented in many surgical intensive care units.2,4,5
Several prediction models for postoperative delirium have been proposed, but many were developed in mixed surgical or noncardiac populations, use heterogeneous delirium definitions, or lack robust validation in contemporary cardiac surgery cohorts. Moreover, few models specifically incorporate perioperative factors that are potentially modifiable in the cardiac surgical ICU, such as minimally invasive surgical approaches, depth and duration of sedative exposure, and postoperative infection. A pragmatic, well-calibrated prognostic model tailored to the cardiac surgery population could therefore support early risk stratification, guide preventive bundles, and optimize sedation and infection-prevention protocols in high-risk patients. 6,7
Despite peri-operative advancements, including both surgical and anesthetic, delirium is a frequent post cardiac surgery complication. Delirium is a common menace in the cardiac surgical ICU and outcome consequences of greater number of morbidity and mortality. Recent research has identified possible hazards for the occurrence of delirium and strategies to treat it. However, more studies are required to standardize the risk factors, its occurrence and treatment strategies in post cardiac surgical patients. 8
In this context, the present study aimed to develop and internally validate a multivariable prognostic model for delirium after cardiac surgery, using prospectively collected data from adults admitted to the surgical intensive care unit of a tertiary heart center. The model focuses on readily available preoperative and perioperative variables, including sex, surgical approach, sedative exposure, and postoperative complications, to facilitate bedside application and inform targeted delirium prevention strategies in routine clinical practice.
2. METHODOLOGY
2.1. Study design
In this prospective observational study, 158 adults undergoing cardiac surgery were enrolled. Delirium was assessed daily for five days using CAM-ICU, RASS, and ICDSC. Univariate predictors (P < 0.05) entered multivariate logistic regression. Model discrimination was assessed by ROC analysis; internal validity by 500-sample bootstrapping and ten-fold cross-validation.
This study was conducted at the Surgical Cardiac Intensive Care Unit at Hanoi Heart Hospital, Vietnam, between May 2025 and August 2025, as an prospective observational study involving adult patients aged 18 y and above, who underwent cardiac surgery with cardiopulmonary bypass. Consent to participate in the study was obtained from each patient before surgery. Details were shown in study flowchart (Figure 1).
Figure 1: The optimal cut-off value for cardiopulmonary bypass (CPB) time
Exclusion criteria included: Patients with conditions that hindered delirium assessment using the CAM-ICU, such as dementia or deafness, as well as those with severe complications like stroke or who expired during the study, were excluded from the study. The existence of delirium before surgery also excluded the patient from the study.
The sample size was primarily determined using a formula for estimating a single proportion, based on the expected incidence of postoperative delirium in cardiac surgery patients and a predefined margin of error. For the prognostic model, we additionally adhered to the commonly recommended rule of at least 10 events per variable (EPV) to reduce the risk of overfitting. With 38 delirium events, the final multivariable model was therefore restricted to four predictors, maintaining an EPV of approximately 9–10.
2.2. Anesthesia, surgery and intensive care
All the patients received standard care, including an examination one-day before their surgery to take their history and evaluate their physical, mental, and cognitive status. All patients received general anesthesia; induction by midazolam, etomidate, fentanyl and rocuronium, and maintenance of anesthesia with TCI propofol, fentanyl and rocuronium, in combination with sevoflurane or isoflurane inhalation. The depth of anesthesia was maintained using both clinical signs (hemodynamic responses, pupil size, and patient movement) and continuous bispectral index (BIS) monitoring. Anesthetic dosing was adjusted to maintain a target BIS range of 40–60 during surgery. They also received tranexamic acid and prophylactic antibiotics. Heparin was used to stop blood clot formation during cardiopulmonary bypass (CPB), and protamine sulphate was used to reverse the heparin’s effects after CPB stopped. These drugs were used according to ACT guidelines during surgery. The pump flow rate in running CPB was between 2.4 and 2.8 L/min/m2; mean blood pressure was maintained between 60 and 90 mmHg, and mild hypothermia was induced at 33 °C and 35 °C. After surgery, the patient was transferred to the recovery room, sedated with midazolam and fentanyl, and extubated when all criteria were met.
Postoperative analgesia included intravenous using morphine or erector spinae plane (ESP) nerve block using ropivacaine through catheter for the first three days postoperatively, combined with other pain relievers such as paracetamol and nonsteroidal anti-inflammatory drugs.
As part of the study, questionnaires, physical tests, and medical records, were used to get information about the patients. This included demographic information, e.g., age, gender, ASA physical status classification system, and medical histories like hypertension, cerebrovascular accident, diabetes, and history of alcohol abuse. Operative time, CPB time, aortic cross-clamp time, and number of drainages were noted. After surgery, number of days using Propofol, opioids, mechanical ventilation duration, occurrence of acute renal failure and blood transfusion after surgery were recorded.
Postoperative pain was managed according to a standardized analgesic protocol. This included titrated intravenous morphine, combined with scheduled paracetamol with or without nonsteroidal anti‑inflammatory drugs (NSAIDs), as clinically appropriate. Pain intensity was assessed using the Numeric Rating Scale (NRS) every 4 hours, and analgesic doses were adjusted accordingly.
2.3. Delirium assessment
Delirium was assessed once daily for the first five postoperative days in the surgical intensive care unit using validated instruments recommended for critically ill adults. Postoperative delirium was assessed once daily at a fixed time, at 8:00 a.m. ± 1 hour, using a standardized delirium screening protocol. All assessments were performed by trained ICU staff who were familiar with the use of the delirium assessment tool, in order to enhance consistency and reduce interobserver variability. At each assessment, level of consciousness was first evaluated with the Richmond Agitation–Sedation Scale (RASS); patients with deep sedation (RASS −4 or −5) were not evaluated for delirium and were reassessed when arousal improved. Delirium screening was then performed with the Confusion Assessment Method for the Intensive Care Unit (CAM‑ICU), which has high specificity for ICU delirium, and the Intensive Care Delirium Screening Checklist (ICDSC), which captures a spectrum from subsyndromal to full‑syndrome delirium based on symptoms observed over the preceding 24 hours. For each study day, the presence of delirium was defined as a positive CAM‑ICU assessment and/or an ICDSC score at or above the conventional diagnostic threshold (≥4), and delirium subtype (hyperactive, hypoactive, mixed) was categorized according to concurrent RASS scores. All assessments were performed by physicians or nurses who had completed standardized training in the use of RASS, CAM‑ICU, and ICDSC prior to study initiation.
2.4. Statistical analysis
The data were analyzed using SPSS 20.0 software. Quantitative variables were described as mean and standard deviation (X̄, SD). The two mean values were compared using the t-test for standard variables and the Mann-Whitney U test for non-standard variables. Qualitative variables were described as numbers (n) and percentages and tested using the chi-squared test. Odds ratios (ORs) were calculated to show the effect size of perioperative risk factors. Then, the statistically significant risk factors after univariate analysis (P < 0.05) were entered into a logistic multivariable regression model, which was based on the model's fit (Hosmer & Lemeshow Test P > 0.05) to find the most powerful model. The normality of continuous variables was assessed using the Shapiro–Wilk test. Variables that did not follow a normal distribution were compared between groups using the Mann–Whitney U test. The difference was considered statistically significant at P < 0.05.
3. RESULTS
There were 158 eligible patients enrolled in the study. The incidence of postoperative delirium: There were 38 cases of delirium, accounting for 24.1%.
Table 1 showed the rate of delirium by day. On postoperative day 0, delirium was identified in 8.9% of patients, rising to 15.2% on day 1. The majority of new cases occurred within the first two days. By day 5, the delirium rate declined to 7.7%, and the overall incidence during hospitalization was 24.1%.
| Table 1: The rate of delirium by day | ||||
| Days | Total patients | No delirium | Delirium | New onset delirium |
| N0 | 158 | 144 (91.1) | 14 (8.9) | 14 |
| N1 | 158 | 138 (84.8) | 24 (15.2) | 18 |
| N2 | 156 | 145 (92.9) | 11 (7.1) | 4 |
| N3 | 72 | 66 (91.7) | 6 (8.3) | 1 |
| N4 | 50 | 45 (90) | 5 (10) | 1 |
| N5 | 26 | 24 (92.3) | 2 (7.7) | 0 |
| Total | 158 | 120 (75.9) | 38 (24.1) | 38 |
| Data presented as n (%) | ||||
Table 2 showed the types of delirium by day. Of the 158 patients, hyperactive delirium was the predominant subtype across all days, peaking at 22 cases on day 1. Hypoactive delirium remained rare, with only 1–2 cases daily, and no mixed-type delirium was observed throughout the study period. The incidence of total delirium was highest on day 1 (24 cases) and decreased thereafter. Table 3 showed the interventions and supportive measures for delirium. Among patients with delirium, intravenous sedation was administered in 57.9%, haloperidol in 92.1%, and oral antipsychotics in 34.2%. Mechanical ventilation was required in 36.8% of cases, and 94.7% underwent physical restraint. The majority of delirium cases resolved within one day (60.5%) as shown in Table 4. Treatment lasted two days in 26.3% of cases and three or more days for the remainder, with just one patient each requiring four to six days for recovery.
| Table 2: Types of delirium by day | ||||||
| Types of delirium | N0 | N1 | N2 | N3 | N4 | N5 |
| No delirium | 144 | 158 | 145 | 66 | 45 | 24 |
| Delirium | 14 | 24 | 11 | 6 | 5 | 2 |
| Hyperactive delirium | 12 | 22 | 10 | 5 | 4 | 1 |
| Hypoactive delirium | 2 | 2 | 1 | 1 | 1 | 1 |
| Mixed-type delirium | 0 | 0 | 0 | 0 | 0 | 0 |
| Table 3: Interventions and supportive measures for Delirium (n = 38) | ||
| Characteristics | Number | (%) |
| Therapeutic and supportive interventions | ||
| Intravenous sedation | 22 | 57.89 |
| Haloperidol administration | 35 | 92.1 |
| Oral antipsychotic agents | 13 | 34.21 |
| Reintubation (mechanical ventilation) | 14 | 36.84 |
| Physical restraint (bed confinement) | 36 | 94.73 |
| Table 4: Duration of treatment from delirium onset to resolution (in days) (n = 38) | ||
| No. of days | Number | % |
| 1 | 23 | 60.5 |
| 2 | 10 | 26.3 |
| 3 | 2 | 5.3 |
| 4 | 1 | 2.6 |
| 5 | 1 | 2.6 |
| 6 | 1 | 2.6 |
Table 5 showed the main patient characteristics and the results of the univariate analysis. Patients who got delirium were much older and more likely to be female than those who didn't get it (P = 0.004). In the delirium group, valvular heart disease and vascular disease were much more common than in the other groups (P = 0.044 and P = 0.050, respectively). There were more patients in the delirium group who had minimally invasive
surgery (p < 0.001). Patients with delirium exhibited significantly prolonged ventilator durations (P = .002) and extended sedative administration periods (p < 0.001), especially with propofol (p < 0.001). Patients who developed delirium also had a higher risk of getting
an infection after surgery (P = 0.033) and having a stroke during or after surgery (P = .009). There were no significant differences between groups in terms of anesthesia duration, cardiopulmonary bypass duration, or comorbidities including hypertension, diabetes, and coronary artery disease. The two patients in Table 5 without cardiopulmonary bypass (CPB) underwent minimally invasive cardiac procedures that did not require extracorporeal circulation but otherwise met all inclusion criteria.
| Table 5: Patient characteristics and the results of the univariate analysis. | |||||
| Variables | Non-delirium (n = 120) |
Delirium (n = 38) |
P-value | ||
| Age (years) | < 65 | 7 | 18 | 0.099 | |
| ≥ 65 | 45 | 20 | |||
| Gender | Female | 56 | 28 | 0.004 | |
| Male | 64 | 10 | |||
| Height (cm) | 158.20 ± 7.67 | 156.76 ± 7.470 | 0.990 | ||
| Weight (kg) | 55.11 ± 9.013 | 51.97 ± 8.722 | 0.536 | ||
| BMI (kg/m2) | 21.91 ± 2.641 | 21.05 ± 2.760 | 0.903 | ||
| Medical History | |||||
| Mental disorders, neurological injury | 12 | 4 | 0.925 | ||
| History of respiratory disease | 4 | 2 | 0.951 | ||
| Hypertension | 39 | 7 | 0.096 | ||
| Vascular disease | 11 | 8 | 0.05 | ||
| Valvular heart disease | 43 | 7 | 0.044 | ||
| Coronary artery disease | 29 | 8 | 0.693 | ||
| Type II diabetes mellitus | 19 | 2 | 0.094 | ||
| Thyroid disease | 2 | 1 | |||
| History of substance abuse – alcohol | 6 | 2 | 0.949 | ||
| History of substance use: tobacco – pipe tobacco | 21 | 1 | 0.021 | ||
| Type of surgery | Open surgery | 96 | 19 | < 0.001 | |
| Minimal invasive surgery | 24 | 19 | |||
| CPB | 118 | 38 | 0.423 | ||
| Anesthesia time (mins) | 278.17 ± 61.76 | 287.11 ± 47.24 | 0.090 | ||
| CPB time (mins) | 116.54 ± 51.13 | 129.95 ± 38.71 | 0.212 | ||
| Aortic clamp time (min) | 80.52 ± 37.65 | 83.34 ± 29.05 | 0.113 | ||
| Ventilator time (hours) | 28.73 ± 20.91 | 36.74 ± 34.29 | 0.002 | ||
| Duration of sedative use (hours) | 19.67 ± 16.71 | 32.32 ± 31.73 | 0.000 | ||
| Duration of sedation with midazolam (hours) | 4.60 ± 12.59 | 6.55 ± 21.30 | 0.131 | ||
| Duration of sedation with propofol (hours) | 14.18 ± 9.08 | 25.89 ± 20.05 | 0.000 | ||
| Opioid use (days) | 68.96 ± 20.07 | 71.21 ± 23.56 | 0.332 | ||
| IABP | 1 | 1 | 0.388 | ||
| Dialysis | 0 | 1 | 0.075 | ||
| Post-operative infection | 29 | 16 | 0.033 | ||
| Perioperative stroke | 6 | 7 | 0.009 | ||
Receiver operating characteristic (ROC) curve showing the area under the curve (AUC) and the best cut-off value for cardiopulmonary bypass (CEC) time in predicting the outcome (Figure 2). The AUC was 0.619, which means it had a small but clinically important ability to tell the difference between groups (P = 0.028). The best cut-off point (Y = 0.268) was a CEC duration of 95 minutes, which gave a sensitivity of 89.5% and a specificity of 62.7%. Receiver operating characteristic (ROC) curve showing the area under the curve (AUC) and the best cut-off point for how long propofol sedation should last to predict the outcome (Figure 2). The AUC was 0.747, which means it was able to tell the difference between the two groups well (P < 0.001). The best cut-off point (Y = 0.38) was 15.5 hours of propofol sedation, which gave a sensitivity of 76.3% and a specificity of 38.3%.
Figure 2 : The optimal cut-off value for propofol sedation duration in predicting the outcome
Table 6 shows that, in the multivariate logistic regression model, female gender (OR 2.68, 95% CI 1.01–7.14, P = 0.048), minimally invasive surgery (OR 4.14, 95% CI 1.54–11.13, P = 0.005), longer propofol sedation duration (OR 1.07 per hour, 95% CI 1.02–1.14, P = 0.011), and postoperative infection (OR 3.45, 95% CI 1.02–11.68, P = 0.046) were independently associated with an increased risk of delirium. In contrast, total sedation duration, mechanical ventilation duration, and perioperative stroke did not remain significantly associated with delirium after adjustment for other covariates (all P-value > 0.05). The apparent model showed in Figure 3 (female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection) demonstrated good discrimination, with an AUC of 0.828 (95% CI 0.759–0.897; P < 0.001). After internal validation using bootstrap resampling, the mean optimism was 0.038, yielding an optimism-corrected AUC of 0.790. Consistent performance was observed with ten-fold cross-validation, which produced a mean AUC of 0.79 ± 0.04.
Figure 3: The apparent model (female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection) of prediction
4. DISCUSSION
POD is associated with, prolonged ICU stay, long-term cognitive decline, and increased mortality. Monitoring and diagnosis are mainly based on standardized tools such as CAM-ICU, ICDSC. Management, care and treatment are a combination of medication, care and safety measures with significant effectiveness. Patients were prospectively screened from day one to day ten after surgery or until hospital discharge. 9 The duration of mechanical ventilation and ICU length of stay were longer in the group of patients with delirium (10.6 hours (6.6, 19.5) vs 6.4 hours (4.9, 8.6), P < 0.001, and 1.7 days (0.9, 4.2) vs 0.9 days (0.9, 1), P < 0.001). 10 A total of 158 eligible adult patients undergoing cardiac surgery were enrolled in the study. During the index hospitalization, 38 patients developed postoperative delirium, corresponding to an overall incidence of 24.1%, which is within the range reported in contemporary cardiac surgery cohorts
A total of 158 eligible adult patients undergoing cardiac surgery were enrolled in the study. During the index hospitalization, 38 patients developed postoperative delirium, corresponding to an overall incidence of 24.1%, which is within the range reported in contemporary cardiac surgery cohorts. 2 Delirium manifested early in the postoperative period. Delirium was detected in 8.9% of patients on postoperative day (POD) 0, rising to 15.2% on POD 1. Most new cases of delirium happened within the first two days after surgery. This is in line with previous reports that delirium after cardiac surgery most often happens in the first few days in the intensive care unit. The daily rate of delirium peaked on POD 1 and then steadily dropped, reaching 7.7% by POD 5. 4,11 The cumulative incidence of postoperative delirium during the entire hospitalization was 24.1%, suggesting that roughly one in four patients experienced at least one episode of delirium following cardiac surgery. This burden is comparable to that observed in recent cardiac surgery series and underscores delirium as a frequent neuropsychiatric complication in this population. 4,11
Among the 158 patients enrolled, hyperactive delirium was the predominant subtype throughout the postoperative period. This type of delirium reached its highest point on the first day after surgery, with 22 cases. This was the same day that the overall number of delirium cases reached its highest point (24 cases). Conversely, hypoactive delirium was rarely observed, with merely 1–2 cases recorded daily, and no instances of mixed-type delirium were documented throughout the study period. These findings align with previous reports emphasizing the prevalence of hyperactive delirium, particularly in the immediate postoperative phase following cardiac surgery, whereas hypoactive delirium frequently goes unrecognized unless specifically evaluated by seasoned clinicians utilizing standardized instruments. 12,13 The daily rate of total delirium decreased after day 1, reflecting the typical clinical course described in contemporary literature. 14
Table 3 shows a summary of the treatments and support given to patients who had postoperative delirium. Intravenous sedation was utilized in 57.9% of delirious patients, haloperidol in 92.1%, and oral antipsychotic agents in 34.2%, indicating a primarily pharmacological management approach aligned with standard ICU delirium protocols. 15,16 Mechanical ventilation was necessary in 36.8% of delirium cases, and physical restraints were utilized in 94.7% of patients, highlighting that agitation and the risk of self-harm or device removal were prevalent clinical issues in this group. 17
Protocol-based care for delirium was utilized in 86.8% of affected patients, primarily to improve patient safety and standardize management. This protocol was implemented uniformly in patients both with and without mechanical ventilation, indicating that structured delirium care pathways were integrated throughout the range of respiratory support. No additional or alternative protocols beyond the standard delirium management pathway were required during the study period. 15,17,18
Most cases of postoperative delirium went away quickly; 60.5% of the patients who had it were completely better within one day of the onset (Table 4). In 26.3% of cases, delirium needed two days of treatment. Only a small number of patients had it for three or more days; in fact, only one patient needed four, five, or six days to fully recover. This temporal pattern of delirium resolution aligns with prior studies in cardiac surgery cohorts, which show that delirium most often develops early postoperatively and is typically of short duration, especially when timely detection and targeted management strategies are implemented. 19 Rapid recovery rates may reflect both the effectiveness of standard ICU protocols and the predominance of hyperactive delirium, which is usually more responsive to supportive and pharmacological interventions. 15
Table 5 presents the baseline and perioperative characteristics according to delirium status, together with the results of the univariate analysis. Patients who developed postoperative delirium were significantly older and more frequently female than those who did not, consistent with previous work identifying advanced age and female sex as important vulnerability factors for delirium after cardiac surgery. 20 Valvular heart disease and vascular disease were also more prevalent among patients with delirium, suggesting that underlying structural heart disease and systemic vascular pathology may contribute to increased susceptibility. 2,21
Procedural and postoperative factors showed clear differences between groups. Minimally invasive surgery was more common in the delirium group, and patients who developed delirium had significantly longer durations of mechanical ventilation, total sedative exposure, and propofol infusion, in line with prior evidence that prolonged ventilatory support and sedative use are associated with higher delirium risk. In addition, postoperative infection and perioperative stroke occurred more frequently in the delirium group, corroborating reports that inflammatory and neurologic complications are important precipitants of delirium in cardiac surgery populations. By contrast, there were no significant between-group differences in anesthesia time, cardiopulmonary bypass duration, or common comorbidities such as hypertension, diabetes, and coronary artery disease, indicating that, in this cohort, these factors did not independently distinguish patients who developed delirium from those who did not. 21,22
Table 6 summarizes the multivariate logistic regression analysis evaluating independent predictors of postoperative delirium. After adjusting for other factors, being female (OR 2.68, 95% CI 1.01–7.14, P = 0.048), having minimally invasive surgery (OR 4.14, 95% CI 1.54–11.13, P = 0.005), having longer propofol sedation (OR 1.07 per hour, 95% CI 1.02–1.14, P = 0.011), and having an infection after surgery (OR 3.45, 95% CI 1.02–11.68, P = 0.046) were all still linked to a higher risk of delirium. These findings indicate that both patient-related factors (sex) and modifiable perioperative factors (surgical approach, sedative exposure, and infection) contributed meaningfully to delirium risk in this cohort, consistent with contemporary multivariable models in cardiac surgery populations. 4,23,24 Conversely, total sedation duration, mechanical ventilation duration, and perioperative stroke failed to maintain statistical significance in the fully adjusted model (all p > 0.05). This indicates that their associations with delirium, identified in univariate analyses, may be mediated or confounded by other variables included in the study. This pattern is similar to what other studies have found, where some perioperative factors lose significance after taking into account a mix of demographic, surgical, and postoperative complications. This shows how important it is to use multivariable adjustment when looking for independent predictors of delirium. 7,22,25 In our study, longer duration of postoperative propofol sedation was identified as an independent predictor of delirium. However, this association should be interpreted with caution. The duration of propofol exposure likely reflects greater overall illness severity, more complex or prolonged surgery, and a higher need for postoperative mechanical ventilation and sedation, rather than a purely causal effect of propofol itself. Furthermore, reverse causation is possible, as patients who became agitated or delirious often required escalation or prolongation of sedative therapy, which could artificially strengthen the association between propofol duration and delirium. We therefore consider propofol duration to be a marker of high‑risk patients and intensive postoperative care, rather than a modifiable pharmacologic trigger of delirium per se.
The prognostic model combining female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection showed good discriminative performance for predicting postoperative delirium. The apparent model yielded an AUC of 0.828 (95% CI 0.759–0.897; p < 0.001), indicating strong ability to distinguish between patients who did and did not develop delirium, and falling within or above the range reported for other cardiovascular surgery delirium prediction tools. 26,27 After internal validation using bootstrap resampling, the mean optimism in model performance was modest (0.038), yielding an optimism-corrected AUC of 0.790. This indicates good discrimination and suggests limited overfitting, despite the relatively small single-center cohort. Ten-fold cross-validation yielded consistent results, with a mean AUC of 0.79 ± 0.04, demonstrating the model's internal stability and robustness across various data partitions, in accordance with current standards for clinically relevant prediction models in perioperative delirium research. 26,27
Limitations of study
We acknowledge several limitations of our study, including its single‑center design, the relatively modest sample size, the once‑daily assessment of delirium, and the potential for residual confounding.
5. CONCLUSIONS
Postoperative delirium affects nearly one-quarter of cardiac surgery patients. A prognostic model including female gender, minimally invasive surgery, propofol sedation duration, and postoperative infection demonstrates robust discrimination (optimism-corrected AUC 0.790) and internal stability. Implementation may enable early risk stratification and optimization of sedation and infection-prevention protocols.
IRB approval
We conducted this study in compliance with the principles of the Declaration of Helsinki. The study’s protocol was reviewed and approved by the Hanoi Heart Hospital Ethical Review Board (No. 1741/BVT-GCNHĐĐĐ dated on May 8th 2025). Written informed consent was obtained from all patients before surgery.
Data availability
The numerical data generated in the conduct of this study are available with the corresponding author.
Conflict of interest
The authors made no declarations regarding potential conflicts.
Funding
No external or industry funding was involved in this study.
Acknowledgments
We gratefully thank the colleagues and staff in the operating theater and cardiac intensive care unit for their cooperation in data collection.
Authors’ contribution
N.S.H. and N.V.T. conceptualized the study. N.V.T., N.H.H., and D.C.P. collected the data. D.C.P. and N.V.T. performed the formal analysis. N.S.H., D.C.P., and N.V.T. wrote the original draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
REFERENCES
- Nuckols CC, Nuckols CC. The diagnostic and statistical manual of mental disorders,(DSM-5). Philadelphia: American Psychiatric Association. 2013.
- Mattimore D, Fischl A, Christophides A, Cuenca J, Davidson S, Jin Z, Bergese S. Delirium after Cardiac Surgery-A Narrative Review. Brain Sci. 2023;13(12). [PubMed] DOI: 10.3390/brainsci13121682.
- Lin L, Zhang X, Xu S, Peng Y, Li S, Huang X, et al. Outcomes of postoperative delirium in patients undergoing cardiac surgery: A systematic review and meta-analysis. Frontiers in cardiovascular medicine. 2022;9:884144. [PubMed] DOI: 10.3389/fcvm.2022.884144.
- Nguyen TT, Ho HS, Duong HD. Incidence and risk factors for delirium after open heart surgery with cardiopulmonary bypass. Anaesthesia, Pain & Intensive Care. 2023;27(6):639-45. [FreeText] DOI: 10.35975/apic.v27i6.2354.
- Guo Y, Li C, Mu Y, Wu T, Lin X. Incidence and associated factors of postoperative delirium in adults undergoing cardiac surgery with cardiopulmonary bypass: a prospective cohort study. Journal of Clinical Nursing. 2025;34(9):3811-25. [PubMed] DOI: 10.1111/jocn.17596.
- Shamsi T, Janga SR, Baskaran NU, Rangasamy V, Ramachandran RV, Chen M, et al. Temporal Trends and Severity of Postoperative Delirium in Cardiac Surgery: Insights from A Systematic Review and Meta-Analysis. Journal of Cardiothoracic and Vascular Anesthesia. 2025. [PubMed] DOI: 10.1053/j.jvca.2025.05.020.
- Schumann S, Schön G, Hüners I, Biermann D, Siebel LC, Jess F, et al. Prevalence of and risk factors for postoperative delirium among children after cardiac surgery in a Single-Centre retrospective study. Scientific Reports. 2025;15(1):20140. [PubMed] DOI: 10.1038/s41598-025-04927-z.
- Asghar A, Siddiqui KM, Ahsan K, Chughtai S. Postoperative delirium after cardiac surgery; incidence, management and prevention. Anaesthesia, Pain & Intensive Care. 2017;21(1):109-12. [FreeText]
- Brown CHt, Laflam A, Max L, Lymar D, Neufeld KJ, Tian J, et al. The Impact of Delirium After Cardiac Surgical Procedures on Postoperative Resource Use. Ann Thorac Surg. 2016;101(5):1663-9. [PubMed] DOI: 10.1016/j.athoracsur.2015.12.074.
- Järvelä K, Porkkala H, Karlsson S, Martikainen T, Selander T, Bendel S. Postoperative delirium in cardiac surgery patients. Journal of cardiothoracic and vascular anesthesia. 2018;32(4):1597-602. [PubMed] DOI: 10.1053/j.jvca.2017.12.030.
- Kotfis K, Szylińska A, Listewnik M, Strzelbicka M, Brykczyński M, Rotter I, Żukowski M. Early delirium after cardiac surgery: an analysis of incidence and risk factors in elderly (≥ 65 years) and very elderly (≥ 80 years) patients. Clinical interventions in aging. 2018:1061-70. [PubMed] DOI: 10.2147/CIA.S166909.
- Falk A, Stenman M, Kåhlin J, Hultgren R, Nymark C. Suffering in silence–cardiac surgery patients recalling hypoactive delirium a qualitative descriptive study. Intensive and Critical Care Nursing. 2023;79:103493. [PubMed] DOI: 10.1016/j.iccn.2023.103493.
- Mufti HN, Hirsch GM. Perioperative prediction of agitated (hyperactive) delirium after cardiac surgery in adults–The development of a practical scorecard. Journal of critical care. 2017;42:192-9. [PubMed] DOI: 10.1016/j.jcrc.2017.07.045.
- Pagad S, Somagutta MR, May V, Arnold AA, Nanthakumaran S, Sridharan S, Malik BH. Delirium in cardiac intensive care unit. Cureus. 2020;12(8). [PubMed] DOI: 10.7759/cureus.10096.
- Evans AS, Weiner MM, Arora RC, Chung I, Deshpande R, Varghese R, et al. Current approach to diagnosis and treatment of delirium after cardiac surgery. Ann Card Anaesth. 2016;19(2):328-37. [PubMed] DOI: 10.4103/0971-9784.179634.
- Deininger MM, Schnitzler S, Benstoem C, Simon T-P, Marx G, Panagiotidis D, et al. Standardized pharmacological management of delirium after on-pump cardiac surgery reduces ICU stay and ventilation in a retrospective pre-post study. Scientific Reports. 2023;13(1):3741. [PubMed] DOI: 10.1038/s41598-023-30781-y.
- Neale K, Then KL, Rankin JA. Delirium in the Cardiovascular Surgery Patient: An Overview for Cardiovascular Nurses. Canadian Journal of Cardiovascular Nursing. 2024;35(2). [FreeText] DOI: 10.5737/cjcn-34-2-14.
- Lin H, Dong D, Zheng K, Xu Q. A Comprehensive Intervention Program for Postoperative Delirium Prevention in Elderly Patients Undergoing Cardiac Surgery. Journal of PeriAnesthesia Nursing. 2025;40(2):371-6. [PubMed] DOI: 10.1016/j.jopan.2024.05.018.
- Bilal MS, Khan DIU, Haq IU. Frequency Of Development Of Post-Operative Delirium In Adult Cardiac Surgery Patients In A Single Centre. Pakistan Journal of Medical & Cardiological Review. 2025;4(2):83-110. [FreeText] DOI: 10.5281/zenodo.17780007.
- Labaste F, Porterie J, Bousquet P, Marcheix B, Sanchez-Verlaan P, Frances B, et al. Postoperative delirium is a risk factor of poor evolution three years after cardiac surgery: an observational cohort study. Clinical Interventions in Aging. 2020:2375-81. [PubMed] DOI: 10.2147/CIA.S265797.
- Pei W, Tan H, Dai T, Liu J, Tang Y, Liu J. Risk factors for postoperative delirium in adult patients undergoing cardiopulmonary bypass in cardiac surgery. Am J Transl Res. 2024;16(9):4751-60. [PubMed] DOI: 10.62347/TXAC6999.
- Ding Y, Gao J, Ge Y, Huang T, Zhang Y. Risk factors for postoperative delirium in frail elderly patients undergoing on-pump cardiac surgery and development of a prediction model—a prospective observational study. Frontiers in Cardiovascular Medicine. 2024;11:1425621. [PubMed] DOI: 10.3389/fcvm.2024.1425621.
- Xu MM, Zhou JJ, Han MT, Sun T, Hui KL. Analysis of risk factors and development of a predictive model for postoperative delirium in elderly patients undergoing cardiac surgery with general anesthesia. Medicine (Baltimore). 2025;104(47):e46021. [PubMed] DOI: 10.1097/MD.0000000000046021.
- Gonçalves MCB, Khera T, Otu HH, Narayanan S, Dillon ST, Shanker A, et al. Multivariable Predictive Model of Postoperative Delirium in Cardiac Surgery Patients: Proteomic and Demographic Contributions. Anesth Analg. 2025;140(2):476-87. [PubMed] DOI: 10.1213/ANE.0000000000007293.
- Sabol F, Bily B, Artemiou P, Kolesar A, Torok P, Bilecova-Rabajdova M, et al. Incidence and risk factors of delirium in patients after cardiac surgery: modifiable and non-modifiable factors. Cor et Vasa. 2015;57(3):e168-e75. [FreeText] DOI: 10.1016/j.crvasa.2015.01.004.
- Yang T, Yang H, Liu Y, Liu X, Ding YJ, Li R, et al. Postoperative delirium prediction after cardiac surgery using machine learning models. Comput Biol Med. 2024;169:107818. [PubMed] DOI: 10.1016/j.compbiomed.2023.107818.
- Xu Y, Meng Y, Qian X, Wu H, Liu Y, Ji P, Chen H. Prediction model for delirium in patients with cardiovascular surgery: development and validation. Journal of Cardiothoracic Surgery. 2022;17(1):247. [PubMed] DOI: 10.1186/s13019-022-02005-3.