Rajesh Kumar 1 , Nasir Ali Rahim Najjad 2 , Maha Batool 3 , Saqib Ali Syed 4 , Hiranand 5 , Muhammad Arslan Zahid 6
Authors affiliations:
Background & objective: Every patient who undergoes some sort of surgery, whether under general, spinal, epidural or local anesthesia needs vascular access and fluid replacement. The choice of fluid is determined by many factors and may vary according to the center and the anesthetist. We evaluated perioperative fluid therapy practices among anesthetists managing pediatric surgical patients in tertiary care hospitals of Karachi (Pakistan) and assessed the influence of demographic and institutional factors on fluid selection.
Methodology: A cross-sectional study conducted between July 2021 - January 2022 in various tertiary care hospitals in Karachi, Pakistan. A total of 150 qualified FCPS and MCPS anesthetists were surveyed using a structured REDCap-based questionnaire. The SPSS version 26.0 was used to conduct the statistical analysis with the significance set at P < 0.05.
Results: Half strength dextrose saline (0.45 NaCl/5% glucose) was the most frequently used maintenance fluid in newborns (50.7%), whereas Ringer’s lactate (Hartmann's) was the most frequently used maintenance fluid in children >2 months (96.7-98%). Ringer’s Lactate (Hartmann's) was the preferred fluid for blood loss replacement across all age groups. The availability of a standardized fluid guidelines was reported by only 33.3% of anesthetists; 77.3% of them selected fluids according to the availability, instead of any protocol. Significant association between the fluid choice and variables such as gender (P = 0.039) and anesthetists’ qualification (P = 0.033), and years of experience (P = 0.040), as well as the institute type (P = 0.049) existed.
Conclusion: The nature of perioperative fluid practices for pediatric surgical patients between the anesthetists displays a significant difference depending on the pediatric age group and is affected by practitioner background and institutional setting. The persistent use of hypotonic fluids in neonates and poor guideline adherence highlight the urgent need for standardized protocols and targeted training in pediatric fluid management.
Keywords: Anesthetist practices; Cross-sectional study; Hypotonic solutions; Isotonic fluids; Guideline adherence; Pediatric anesthesia; Perioperative fluid therapy.
Citation: Kumar R, Najjad NAR, Batool M, Syed SA, Hiranand, Zahid MA. Perioperative fluid choice in pediatric anesthesia: a cross-sectional study of current practices in tertiary care hospitals of Karachi. Anaesth. pain intensive care 2026;30(2):240-247. DOI: 10.35975/apic.v30i2.3133
Received: May 09, 2025; Revised: October 26, 2025; Accepted: January 01, 2026
Pediatric anesthesia involves perioperative fluid therapy, which is a crucial aspect of achieving hemodynamic stability, tissue perfusion and electrolyte balance. Meticulous choice of intravenous (IV) fluids in children is a complicated issue that is contingent on age-specific physiology, surgery setting and changing clinical standards. The renal and endocrine systems of the pediatric patient are immature, especially in the neonates and infants, which makes them more vulnerable to fluid and electrolyte imbalances than adults..1 Over 300 million surgical procedures are undertaken every year all over the world and of this number about 11% are done to children below the age of 15.2 Pediatric surgical care in low- and middle-income countries (LMICs) is growing at a fast pace but the standardized perioperative procedures, particularly those related to the fluid therapy, are not followed uniformly.3 Non-specialist anesthetists often have limited pediatric-specific training, leading to inconsistent fluid management practices.
Historically, maintenance fluids for pediatric patients were based on hypotonic solutions like 1/2 strength Dextrose saline in the early years by theoretical calculations of electrolyte and caloric requirements.4 Literature has demonstrated that hypotonic solutions are linked to a high likelihood of hospital-acquired hyponatremia and this is linked to negative outcomes such as seizures, cerebral oedema as well as mortality.5,6 This has led to the review of recommendations by international organizations like the National Institute for Health and Care Excellence (NICE) and the American Academy of Pediatrics (AAP) recommended the use of isotonic crystalloids such as 0.9% Normal Saline and Ringer’s Lactate, in the daily practice on children.7,8 Even with these recommendations, there is still a lot of variation in practice, especially in the neonatal population, where sodium load, glucose requirement and fluid volume sensitivity make decision-making more complicated. According to a systematic review, more than 40% of practitioners still employed hypotonic fluids in neonates even in tertiary care facilities.9 LMIC studies point out that fluid selection by anesthetists is frequently determined by constraints of availability or price or individual preferences instead of standardized protocols.10 The discrepancy between evidence-based guidelines and bedside practice has led to concerns regarding patient safety as well as the necessity to use local data to influence policy and education.
There are no national pediatric anesthesia guidelines in Pakistan and although institutions might have their own protocols, usually the implementation of these protocols is not always followed. The published information on fluid therapy trends among anesthetists in the process of dealing with pediatric cases is limited. The knowledge of the current practice patterns is important to identify knowledge gaps, resource constraints and areas in need of specific intervention.11,12 The aim of the study is to assess the fluid therapy preferences of the anesthetists working with the pediatric surgical patients in Pakistan during perioperative care. The study aims to present evidence that can be used in standardizing, safe and contextually appropriate fluid therapy by analyzing fluid use trends across different pediatric age groups and the role of the practitioner qualification, institutional environment and the availability of guidelines in the aspect of fluid therapy.
This was a descriptive cross-sectional study that was carried out in a period of six months between 21st July 2021 and 31st January 2022. The study was conducted in 13 tertiary care teaching hospitals in Karachi, Pakistan. Participating institutions were The Indus Hospital, The Aga Khan University Hospital, Civil Hospital Karachi, Jinnah Postgraduate Medical Centre (JPMC), National Institute of Child Health (NICH), Sindh Institute of Urology and Transplantation (SIUT), Abbasi Shaheed Hospital, Liaquat National Hospital, Ziauddin Hospital, SMBB Trauma Center, PNS Shifa, Patel Hospital and the National Institute of Cardiovascular Diseases (NICVD). These centers include both public and private sector setups which helps in ensuring a varied anesthesiology workforce.
The target population was the qualified anesthetists already engaged in the perioperative management of surgical patients in the children category. The participants were recruited through a non-probability consecutive sampling method. Sample size was calculated with the OpenEpi software, where we anticipated proportions of fluid preferences at 52.7% of 1/2 strength of Dextrose saline, 41.8% of Ringer’s Lactate and 5.5% of Normal Saline. The minimum sample size that was required was 150 anesthetists at 95% level of confidence and an 8% margin of error.
The target population was anesthesiologists that had passed the FCPS or MCPS examinations, were aged between 28 and 80 years and who were currently working in a tertiary care hospital in Karachi and were willing to give informed consent. Those anesthetists who refused to participate or were not actively working in a tertiary care facility were not involved in the study.
Ethical permission was taken by the college of physicians and surgeons Pakistan (CPSP) and the Institutional Review Board (IRB) of The Indus Hospital before initiation of study. The heads of anesthesia departments of all the participating hospitals were also given permission. A list of practicing anesthetists was created and the potential participants contacted either by phone or email. The data were gathered in a pre-validated questionnaire that was given out in a structured form through the REDCap platform. The questionnaire focused on the type of fluids that were preferred as a form of maintenance, bolus and blood loss substitute in pediatric patients across various age groups. It also collected demographic information, professional experience, how often it handles pediatric cases and whether it has any institutional guidelines or not. The participation was voluntary and anonymity was ensured. It took the respondents between 15-20 minutes to complete the survey.
The main variable of interest was the selection of perioperative fluids by the anesthetists based on the age category of the child: newborn (0 48 hours), term newborn, children aged 2 months to 5 years and children older than 5 years. Fluid choices were isotonic crystalloids (e.g. Normal Saline, Ringer’s Lactate), hypotonic solutions (e.g. 1/2 strength Dextrose saline), colloids and blood products. Three clinical settings to assess the fluid preference were based on the maintenance therapy, fluid bolus and blood loss replacement. Fluid selection was measured against the accepted international standards such as American Academy of Pediatrics, NICE and the Association of Paediatric Anaesthetists.
Data was analyzed and entered into the IBM SPSS Statistics 26.0. Numerical variables (age, years of experience) were described as the means with standard deviations or medians and interquartile ranges (IQR) based on data distributions. Categorical data such as gender, qualification, type of institution, frequency of pediatric sessions and fluid preferences were indicated as frequencies and percentages. The relationship between independent variables (e.g, gender, experience, institute type) and fluid choice was determined by using the Chi-square test or Fisher Exact test in its place. The p-value < 0.05 was taken as statistically significant.
Across all age groups, fluid preference varied notably. In neonates (both newborns and term), as a maintenance fluid, 50.7% and 43.3% of the respondents used 1/2 strength Dextrose saline. Comparatively, Ringer’s Lactate (R/L) has become the most popular maintenance fluid in children aged 2 months old and above 5 years, with a preference of 96.7 and 98% respectively. The same trend was noted in the use of bolus fluid, although R/L was the most common in all ages, there was still significant use of 1/2 strength Dextrose in the neonates, 40% of the newborns and 34.7% of the term neonates. In the case of blood loss replacement, Ringer’s Lactate in 3:1 ratio was the most favored fluid in all groups with a high preference in children above 2 months. Colloids were applied more commonly in the neonatal age group (39.3%) compared to other children (Table 2).
In terms of the institutional practice, 33.3% of anesthetists responded that standardized fluid therapy guidelines were present at their work place. Guideline availability varied according to institute type: 25 institutes each in government and the private sector had guidelines but 70 of 95 private practitioners had no guidelines indicating a greater disparity in protocol use in the private setting (Figure 1). With regards to fluid selection rationale, 77.3% of anesthetists chose their fluid because it was readily available, whereas 22% chose because it is a personal preference. 0.7% checked institutional or published guidelines.
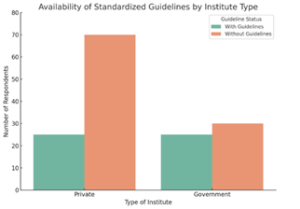
Figure 1: Availability of standardized perioperative fluid guidelines across institute types
Important associations were found using statistical testing. Bolus fluid selection in newborns and maintenance fluid in term neonates had a significant relationship with gender (P = 0.039 and P = 0.039 respectively). The level of qualification was significantly associated with the choice of bolus fluid in newborns (P = 0.033), institute type had a significant correlation with the choice of maintenance fluid in newborns (P = 0.049). The more professionally experienced anesthetists had a significant association when it comes to the choice of the bolus fluid used on term neonates (P = 0.040). Access to guidelines (P = 0.623) and the number of pediatric sessions weekly (P = 0.122) were not found to be statistically significant in relation to fluid choice (Table 3).
The study evaluated the perioperative fluid therapy practices of anesthetists attending pediatric surgical patients of various ages. The results indicate a significant range of preferences to fluids, which greatly depends on the demographics of practitioners, institutional setting and resources. Such discoveries point to the constant disparities between best practice guidelines and clinical practice in the management of fluids, particularly in neonatal care.
Despite the recommendations, hypotonic fluids, especially 1/2 strength Dextrose saline in the maintenance and bolus dose of neonates was still being administered. Although there is increasing international opposition to the widespread administration of hypotonic solution to children, based on the established conditions of hyponatremia, cerebral edema and seizures, more than half of the participants in the survey used such fluids in newborns. Immaturity of the renal system and impaired sodium control in neonatal patients also makes them particularly susceptible to water intoxication and electrolyte imbalance.1,2 Recent recommendations on fluid management in children by several countries in the high-income category support the use of isotonic fluids, either 0.9% saline or Ringer’s Lactate, as the ideal fluid to be used in children of all ages including neonates in the maintenance phase (Appendix 1).3-5
Older pediatric populations had more concerted evidence-based fluid practices. Ringer’s Lactate (R/L) became the most popular option in maintenance and bolus therapy in children over the age of two months with preference rating of more than 95% in each of the therapies. This corresponds to the evidence of clinical trials and recommendations of guidelines that recommend using balanced isotonic crystalloids to manage patients perioperatively in children due to their ability to maintain intravascular volume without disturbing electrolyte levels.6,7 The trend towards R/L in this generation is promising and can be attributed to the increasing compliance with the principles of safe fluid prescriptions, especially in the older and more physiologically stable pediatric patients.8
Ringer’s Lactate in a 3:1 proportion was the fluid of choice in the replacement of blood loss in all age groups. It is a practice in agreement with the guidelines of resuscitation standards in pediatrics, especially in a surgical environment where the formulation of rapid volume expansion is necessary.9 A significant percentage of respondents (39.3%) used colloids, particularly in neonates. The use of colloid (albumin or synthetic starches) in special clinical cases may have theoretical advantages but no evidence that would recommend their use in all cases instead of crystalloids in pediatric surgical patients.10 Large adult trials such as SAFE and CRISTAL, there was no survival benefit seen with colloids and issues of renal safety and cost-effectiveness were also raised.11,12 Pediatric specific literature also suggests the use of crystalloids as first-line resuscitation fluids with the use of colloids in selective indications, as in hypoalbuminemia or third-spacing as a result of burns.13 FThere was a significant institutional finding of lack of the availability of standardized fluid therapy guidelines with the respondents reporting only 33.3%. 70% of anesthetists in the private hospitals reported the lack of such protocols. This difference indicates that the fluid management procedures tend to be determined by personal choice or by supply limitations as opposed to a coherent clinical policy. These are in line with previous low- and middle-income country surveys, which point to protocol adoption and inconsistent adherence as the most frequent obstacles to safe perioperative care.14
The factors affecting the choice of fluids also showed evidence-based practice lapses. The most mentioned determinant was presence of fluid in the operating theatre (77.3%), followed by personal preference (22%). and only 0.7% of the respondents said they had chosen fluids according to formal guidelines, indicating a gap between the available evidence and everyday clinical practice. Such a dependence on availability instead of protocolization of care creates a considerable risk of variation in care and avoidable complications. The other similar studies have highlighted the role of institutional protocols and continuing education in enhancing safe pediatric fluid practices adherence.15
The demographic variables were significantly associated with the fluid preferences. All of the gender, qualification level, type of institute and years of experience were found to have statistically significant correlations with fluid choices in neonates and infants. Gender, in particular, was also shown to be significantly related to bolus and maintenance fluid choices in case of neonates (P = 0.039) whereas the level of qualification had an effect on the choice of bolus fluid (P = 0.033).
The implications of these associations are that clinical decision-making could be guided by non-clinical factors without their knowledge. Such tendencies are observed in the studies of pediatric anesthetic practice within similar health systems where personal training background and exposure tend to dominate over practice-based guidelines.16
The presence of guidelines (P = 0.623) and the number of pediatric patients per week (P = 0.122) did not have any significant statistical relation to fluid preference. This implies that protocols alone might not guarantee adherence since they need to be actively disseminated, trained and enforced institutionally.3,15
The study was limited by its cross-sectional nature and self-reported information that can be biased in its response. There was possible limitation on generalizability as the sample included only anesthetists in selected institutions. Also, the clinical outcomes regarding the fluid choices were not measured.
This study reveals notable variability in perioperative fluid practices among anesthetists, despite the known risks of hyponatremia and cerebral edema. Isotonic fluids are appropriately favored in older pediatric patients. These findings highlight the need for standardized guidelines and targeted educational initiatives to ensure safe, evidence-based fluid management across all pediatric age groups.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
RJ: Main concept
NARN: Conduction of the study work
MB: Manuscript editing
SSA: Literature search
HD: Proof reading
MAZ: Final review
Authors affiliations:
- Rajesh Kumar, Sindh Institute of Urology and Transplantation, Karachi, Pakistan; Email: kewalanirajesh@gmail.com, ORCID: 0009-0000-1398-1504
- Nasir Ali Rahim Najjad, Sindh Institute of Urology and Transplantation, Karachi, Pakistan; Email: nasiralirahimnajjad@gmail.com; https://orcid.org/0009-0005-0394-2030
- Maha Batool, Sindh Institute of Urology and Transplantation, Karachi, Pakistan; Email: 519syeda@gmail.com; https://orcid.org/0000-0001-7405-6363
- Saqib Ali Syed, Sindh Institute of Urology and Transplantation, Karachi, Pakistan; Email: drsyedsaqibali@gmail.com; https://orcid.org/0009-0006-0022-9106
- Hiranand, Sindh Institute of Urology and Transplantation, Karachi, Pakistan; Email: heranand75@gmail.com; https://orcid.org/0000-0003-4760-3418
- Muhammad Arslan Zahid, National Medical Centre, Karachi, Pakistan; Email: dr.arslanzahid@gmail.com; https://orcid.org/0009-0003-4707-0786
ABSTRACT
Background & objective: Every patient who undergoes some sort of surgery, whether under general, spinal, epidural or local anesthesia needs vascular access and fluid replacement. The choice of fluid is determined by many factors and may vary according to the center and the anesthetist. We evaluated perioperative fluid therapy practices among anesthetists managing pediatric surgical patients in tertiary care hospitals of Karachi (Pakistan) and assessed the influence of demographic and institutional factors on fluid selection.
Methodology: A cross-sectional study conducted between July 2021 - January 2022 in various tertiary care hospitals in Karachi, Pakistan. A total of 150 qualified FCPS and MCPS anesthetists were surveyed using a structured REDCap-based questionnaire. The SPSS version 26.0 was used to conduct the statistical analysis with the significance set at P < 0.05.
Results: Half strength dextrose saline (0.45 NaCl/5% glucose) was the most frequently used maintenance fluid in newborns (50.7%), whereas Ringer’s lactate (Hartmann's) was the most frequently used maintenance fluid in children >2 months (96.7-98%). Ringer’s Lactate (Hartmann's) was the preferred fluid for blood loss replacement across all age groups. The availability of a standardized fluid guidelines was reported by only 33.3% of anesthetists; 77.3% of them selected fluids according to the availability, instead of any protocol. Significant association between the fluid choice and variables such as gender (P = 0.039) and anesthetists’ qualification (P = 0.033), and years of experience (P = 0.040), as well as the institute type (P = 0.049) existed.
Conclusion: The nature of perioperative fluid practices for pediatric surgical patients between the anesthetists displays a significant difference depending on the pediatric age group and is affected by practitioner background and institutional setting. The persistent use of hypotonic fluids in neonates and poor guideline adherence highlight the urgent need for standardized protocols and targeted training in pediatric fluid management.
Keywords: Anesthetist practices; Cross-sectional study; Hypotonic solutions; Isotonic fluids; Guideline adherence; Pediatric anesthesia; Perioperative fluid therapy.
Citation: Kumar R, Najjad NAR, Batool M, Syed SA, Hiranand, Zahid MA. Perioperative fluid choice in pediatric anesthesia: a cross-sectional study of current practices in tertiary care hospitals of Karachi. Anaesth. pain intensive care 2026;30(2):240-247. DOI: 10.35975/apic.v30i2.3133
Received: May 09, 2025; Revised: October 26, 2025; Accepted: January 01, 2026
1. INTRODUCTION
Pediatric anesthesia involves perioperative fluid therapy, which is a crucial aspect of achieving hemodynamic stability, tissue perfusion and electrolyte balance. Meticulous choice of intravenous (IV) fluids in children is a complicated issue that is contingent on age-specific physiology, surgery setting and changing clinical standards. The renal and endocrine systems of the pediatric patient are immature, especially in the neonates and infants, which makes them more vulnerable to fluid and electrolyte imbalances than adults..1 Over 300 million surgical procedures are undertaken every year all over the world and of this number about 11% are done to children below the age of 15.2 Pediatric surgical care in low- and middle-income countries (LMICs) is growing at a fast pace but the standardized perioperative procedures, particularly those related to the fluid therapy, are not followed uniformly.3 Non-specialist anesthetists often have limited pediatric-specific training, leading to inconsistent fluid management practices.
Historically, maintenance fluids for pediatric patients were based on hypotonic solutions like 1/2 strength Dextrose saline in the early years by theoretical calculations of electrolyte and caloric requirements.4 Literature has demonstrated that hypotonic solutions are linked to a high likelihood of hospital-acquired hyponatremia and this is linked to negative outcomes such as seizures, cerebral oedema as well as mortality.5,6 This has led to the review of recommendations by international organizations like the National Institute for Health and Care Excellence (NICE) and the American Academy of Pediatrics (AAP) recommended the use of isotonic crystalloids such as 0.9% Normal Saline and Ringer’s Lactate, in the daily practice on children.7,8 Even with these recommendations, there is still a lot of variation in practice, especially in the neonatal population, where sodium load, glucose requirement and fluid volume sensitivity make decision-making more complicated. According to a systematic review, more than 40% of practitioners still employed hypotonic fluids in neonates even in tertiary care facilities.9 LMIC studies point out that fluid selection by anesthetists is frequently determined by constraints of availability or price or individual preferences instead of standardized protocols.10 The discrepancy between evidence-based guidelines and bedside practice has led to concerns regarding patient safety as well as the necessity to use local data to influence policy and education.
There are no national pediatric anesthesia guidelines in Pakistan and although institutions might have their own protocols, usually the implementation of these protocols is not always followed. The published information on fluid therapy trends among anesthetists in the process of dealing with pediatric cases is limited. The knowledge of the current practice patterns is important to identify knowledge gaps, resource constraints and areas in need of specific intervention.11,12 The aim of the study is to assess the fluid therapy preferences of the anesthetists working with the pediatric surgical patients in Pakistan during perioperative care. The study aims to present evidence that can be used in standardizing, safe and contextually appropriate fluid therapy by analyzing fluid use trends across different pediatric age groups and the role of the practitioner qualification, institutional environment and the availability of guidelines in the aspect of fluid therapy.
2. METHODOLOGY
This was a descriptive cross-sectional study that was carried out in a period of six months between 21st July 2021 and 31st January 2022. The study was conducted in 13 tertiary care teaching hospitals in Karachi, Pakistan. Participating institutions were The Indus Hospital, The Aga Khan University Hospital, Civil Hospital Karachi, Jinnah Postgraduate Medical Centre (JPMC), National Institute of Child Health (NICH), Sindh Institute of Urology and Transplantation (SIUT), Abbasi Shaheed Hospital, Liaquat National Hospital, Ziauddin Hospital, SMBB Trauma Center, PNS Shifa, Patel Hospital and the National Institute of Cardiovascular Diseases (NICVD). These centers include both public and private sector setups which helps in ensuring a varied anesthesiology workforce.
The target population was the qualified anesthetists already engaged in the perioperative management of surgical patients in the children category. The participants were recruited through a non-probability consecutive sampling method. Sample size was calculated with the OpenEpi software, where we anticipated proportions of fluid preferences at 52.7% of 1/2 strength of Dextrose saline, 41.8% of Ringer’s Lactate and 5.5% of Normal Saline. The minimum sample size that was required was 150 anesthetists at 95% level of confidence and an 8% margin of error.
The target population was anesthesiologists that had passed the FCPS or MCPS examinations, were aged between 28 and 80 years and who were currently working in a tertiary care hospital in Karachi and were willing to give informed consent. Those anesthetists who refused to participate or were not actively working in a tertiary care facility were not involved in the study.
Ethical permission was taken by the college of physicians and surgeons Pakistan (CPSP) and the Institutional Review Board (IRB) of The Indus Hospital before initiation of study. The heads of anesthesia departments of all the participating hospitals were also given permission. A list of practicing anesthetists was created and the potential participants contacted either by phone or email. The data were gathered in a pre-validated questionnaire that was given out in a structured form through the REDCap platform. The questionnaire focused on the type of fluids that were preferred as a form of maintenance, bolus and blood loss substitute in pediatric patients across various age groups. It also collected demographic information, professional experience, how often it handles pediatric cases and whether it has any institutional guidelines or not. The participation was voluntary and anonymity was ensured. It took the respondents between 15-20 minutes to complete the survey.
The main variable of interest was the selection of perioperative fluids by the anesthetists based on the age category of the child: newborn (0 48 hours), term newborn, children aged 2 months to 5 years and children older than 5 years. Fluid choices were isotonic crystalloids (e.g. Normal Saline, Ringer’s Lactate), hypotonic solutions (e.g. 1/2 strength Dextrose saline), colloids and blood products. Three clinical settings to assess the fluid preference were based on the maintenance therapy, fluid bolus and blood loss replacement. Fluid selection was measured against the accepted international standards such as American Academy of Pediatrics, NICE and the Association of Paediatric Anaesthetists.
Data was analyzed and entered into the IBM SPSS Statistics 26.0. Numerical variables (age, years of experience) were described as the means with standard deviations or medians and interquartile ranges (IQR) based on data distributions. Categorical data such as gender, qualification, type of institution, frequency of pediatric sessions and fluid preferences were indicated as frequencies and percentages. The relationship between independent variables (e.g, gender, experience, institute type) and fluid choice was determined by using the Chi-square test or Fisher Exact test in its place. The p-value < 0.05 was taken as statistically significant.
3. RESULTS
The number of anesthetists who were evaluated was 180. Of the 180, 30 were excluded for not meeting the inclusion criteria or declining participation and 150 were included in the final analysis. Majority were male (74.7%), with 60.7% being FCPS-qualified consultants and 39.3% had an MCPS qualification. The majority of participants (63.3%) operated in the private sector hospitals and 36.7% belonged to the government establishments. Concerning the anesthesia exposure in children, 64.7% of them handle 1-2 sessions per week and 26.7% handle 3+ sessions. A smaller number (8.7%) lacked regular pediatric cases. The mean age of the respondents was 43.1 ± 8.3 years and the mean experience was 10.7 ± 7.5 years (Table 1).| Table 1: Demographics and practice patterns of anesthetists (n = 150) | ||
| Variable | Categories | N (%) |
| Gender | Male | 112 (74.7) |
| Female | 38 (25.3) | |
| Qualification | FCPS Consultant | 91 (60.7) |
| MCPS Consultant | 59 (39.3) | |
| Type of Institute | Private | 95 (63.3) |
| Government | 55 (36.7) | |
| Pediatric Sessions/Week | No regular | 13 (8.7) |
| 1–2 sessions | 97 (64.7) | |
| ≥3 sessions | 40 (26.7) | |
| Standardized Guidelines Present | Yes | 50 (33.3) |
| No | 100 (66.7) | |
| Bad Experience with unrecommended Fluids | Yes | 116 (77.3) |
| No | 34 (22.7) | |
| Age (years) | Mean ± SD | 43.1 ± 8.3 |
| Experience (years) | Mean ± SD | 10.7 ± 7.5 |
Across all age groups, fluid preference varied notably. In neonates (both newborns and term), as a maintenance fluid, 50.7% and 43.3% of the respondents used 1/2 strength Dextrose saline. Comparatively, Ringer’s Lactate (R/L) has become the most popular maintenance fluid in children aged 2 months old and above 5 years, with a preference of 96.7 and 98% respectively. The same trend was noted in the use of bolus fluid, although R/L was the most common in all ages, there was still significant use of 1/2 strength Dextrose in the neonates, 40% of the newborns and 34.7% of the term neonates. In the case of blood loss replacement, Ringer’s Lactate in 3:1 ratio was the most favored fluid in all groups with a high preference in children above 2 months. Colloids were applied more commonly in the neonatal age group (39.3%) compared to other children (Table 2).
| Table 2: Perioperative fluid preferences by pediatric age group and clinical indication (n = 150) | ||||||
| Age Group | Indication | Normal Saline (%) | Ringer’s Lactate (%) | ½ Strength Dextrose (%) | Other Fluids (%) | Most Preferred Fluid |
| Newborn (0–48 h) | Maintenance | 14.3 | 32.7 | 50.7 | 1/5 DS: 1.3, D5%: 0.7 | ½ Strength Dextrose Saline |
| Bolus | 17.3 | 41.3 | 40.0 | 1/3 DS: 0.7, 1/5 DS: 0.7 | Ringer’s Lactate | |
| Blood Loss Replacement | — | 50.7 | — | Colloid: 39.3, NS 3:1: 8.7, FFP: 1.3 | Ringer’s Lactate (3:1) | |
| Term Neonate | Maintenance | 13.3 | 42.0 | 43.3 | 1/5 DS: 0.7, D5%: 0.7 | ½ Strength Dextrose Saline |
| Bolus | 16.0 | 48.7 | 34.7 | 1/3 DS: 0.7 | Ringer’s Lactate | |
| Blood Loss Replacement | — | 50.7 | — | Colloid: 39.3, NS 3:1: 8.7, FFP: 1.3 | Ringer’s Lactate (3:1) | |
| 2 months– 5 yrs | Maintenance | 2.0 | 96.7 | 0.0 | 1/5 DS: 1.3 | Ringer’s Lactate |
| Bolus | 12.0 | 86.0 | 0.7 | 1/5 DS: 1.3 | Ringer’s Lactate | |
| Blood Loss Replacement | — | 78.7 | — | Colloid: 16.7, NS 3:1: 4.0, FFP: 0.7 | Ringer’s Lactate (3:1) | |
| Over 5 yrs | Maintenance | 1.3 | 98.0 | 0.0 | 1/5 DS: 0.7 | Ringer’s Lactate |
| Bolus | 6.7 | 92.0 | 1.3 | — | Ringer’s Lactate | |
| Blood Loss Replacement | — | 83.3 | — | Colloid: 13.3, NS 3:1: 3.3 | Ringer’s Lactate (3:1) | |
In terms of the institutional practice, 33.3% of anesthetists responded that standardized fluid therapy guidelines were present at their work place. Guideline availability varied according to institute type: 25 institutes each in government and the private sector had guidelines but 70 of 95 private practitioners had no guidelines indicating a greater disparity in protocol use in the private setting (Figure 1). With regards to fluid selection rationale, 77.3% of anesthetists chose their fluid because it was readily available, whereas 22% chose because it is a personal preference. 0.7% checked institutional or published guidelines.
Figure 1: Availability of standardized perioperative fluid guidelines across institute types
Important associations were found using statistical testing. Bolus fluid selection in newborns and maintenance fluid in term neonates had a significant relationship with gender (P = 0.039 and P = 0.039 respectively). The level of qualification was significantly associated with the choice of bolus fluid in newborns (P = 0.033), institute type had a significant correlation with the choice of maintenance fluid in newborns (P = 0.049). The more professionally experienced anesthetists had a significant association when it comes to the choice of the bolus fluid used on term neonates (P = 0.040). Access to guidelines (P = 0.623) and the number of pediatric sessions weekly (P = 0.122) were not found to be statistically significant in relation to fluid choice (Table 3).
| Table 3: Statistical associations between demographic/practice variables and fluid preferences | |
| Variable Tested | P-value |
| Gender vs. Bolus fluid for newborns | 0.039* |
| Gender vs. Maintenance fluid for term neonates | 0.039* |
| Qualification vs. Bolus fluid for newborns | 0.033* |
| Institute Type vs. Maintenance fluid for newborns | 0.049* |
| Experience vs. Bolus fluid for term neonates | 0.040* |
| Guideline Availability vs. Fluid preference (any age) | 0.623 |
| Pediatric Sessions per Week vs. Fluid preference (any age) | 0.122 |
| *Significant P < 0.05 | |
4. DISCUSSION
The study evaluated the perioperative fluid therapy practices of anesthetists attending pediatric surgical patients of various ages. The results indicate a significant range of preferences to fluids, which greatly depends on the demographics of practitioners, institutional setting and resources. Such discoveries point to the constant disparities between best practice guidelines and clinical practice in the management of fluids, particularly in neonatal care.
Despite the recommendations, hypotonic fluids, especially 1/2 strength Dextrose saline in the maintenance and bolus dose of neonates was still being administered. Although there is increasing international opposition to the widespread administration of hypotonic solution to children, based on the established conditions of hyponatremia, cerebral edema and seizures, more than half of the participants in the survey used such fluids in newborns. Immaturity of the renal system and impaired sodium control in neonatal patients also makes them particularly susceptible to water intoxication and electrolyte imbalance.1,2 Recent recommendations on fluid management in children by several countries in the high-income category support the use of isotonic fluids, either 0.9% saline or Ringer’s Lactate, as the ideal fluid to be used in children of all ages including neonates in the maintenance phase (Appendix 1).3-5
Older pediatric populations had more concerted evidence-based fluid practices. Ringer’s Lactate (R/L) became the most popular option in maintenance and bolus therapy in children over the age of two months with preference rating of more than 95% in each of the therapies. This corresponds to the evidence of clinical trials and recommendations of guidelines that recommend using balanced isotonic crystalloids to manage patients perioperatively in children due to their ability to maintain intravascular volume without disturbing electrolyte levels.6,7 The trend towards R/L in this generation is promising and can be attributed to the increasing compliance with the principles of safe fluid prescriptions, especially in the older and more physiologically stable pediatric patients.8
Ringer’s Lactate in a 3:1 proportion was the fluid of choice in the replacement of blood loss in all age groups. It is a practice in agreement with the guidelines of resuscitation standards in pediatrics, especially in a surgical environment where the formulation of rapid volume expansion is necessary.9 A significant percentage of respondents (39.3%) used colloids, particularly in neonates. The use of colloid (albumin or synthetic starches) in special clinical cases may have theoretical advantages but no evidence that would recommend their use in all cases instead of crystalloids in pediatric surgical patients.10 Large adult trials such as SAFE and CRISTAL, there was no survival benefit seen with colloids and issues of renal safety and cost-effectiveness were also raised.11,12 Pediatric specific literature also suggests the use of crystalloids as first-line resuscitation fluids with the use of colloids in selective indications, as in hypoalbuminemia or third-spacing as a result of burns.13 FThere was a significant institutional finding of lack of the availability of standardized fluid therapy guidelines with the respondents reporting only 33.3%. 70% of anesthetists in the private hospitals reported the lack of such protocols. This difference indicates that the fluid management procedures tend to be determined by personal choice or by supply limitations as opposed to a coherent clinical policy. These are in line with previous low- and middle-income country surveys, which point to protocol adoption and inconsistent adherence as the most frequent obstacles to safe perioperative care.14
The factors affecting the choice of fluids also showed evidence-based practice lapses. The most mentioned determinant was presence of fluid in the operating theatre (77.3%), followed by personal preference (22%). and only 0.7% of the respondents said they had chosen fluids according to formal guidelines, indicating a gap between the available evidence and everyday clinical practice. Such a dependence on availability instead of protocolization of care creates a considerable risk of variation in care and avoidable complications. The other similar studies have highlighted the role of institutional protocols and continuing education in enhancing safe pediatric fluid practices adherence.15
The demographic variables were significantly associated with the fluid preferences. All of the gender, qualification level, type of institute and years of experience were found to have statistically significant correlations with fluid choices in neonates and infants. Gender, in particular, was also shown to be significantly related to bolus and maintenance fluid choices in case of neonates (P = 0.039) whereas the level of qualification had an effect on the choice of bolus fluid (P = 0.033).
The implications of these associations are that clinical decision-making could be guided by non-clinical factors without their knowledge. Such tendencies are observed in the studies of pediatric anesthetic practice within similar health systems where personal training background and exposure tend to dominate over practice-based guidelines.16
The presence of guidelines (P = 0.623) and the number of pediatric patients per week (P = 0.122) did not have any significant statistical relation to fluid preference. This implies that protocols alone might not guarantee adherence since they need to be actively disseminated, trained and enforced institutionally.3,15
| Appendix 1: Composition of common intravenous solutions used in children | |||||||
| IV fluid | Composition | ||||||
| Na+ | K+ | Cl− | Ca++ | Lactate | Glucose | Calories | |
| mmol/l | mmol/l | mmol/l | mmol/l | mmol/l | g/L | cal/L | |
| Ringer's lactate (Hartmann's) | 130 | 5.4 | 112 | 1.8 | 27 | – | – |
| Normal saline (0.9% NaCl) | 154 | – | 154 | – | – | – | – |
| 10% glucose | – | – | – | – | – | 100 | 400 |
| 0.45 NaCl/5% glucose | 77 | – | 77 | – | – | 50 | 200 |
| Darrow's solution | 121 | 35 | 103 | – | 53 | – | – |
| Half-strength Darrow with 5% glucose | 61 | 17 | 52 | – | 27 | 50 | 200 |
| Half-strength Ringer's lactate with 5% glucose | 65 | 2.7 | 56 | 1 | 14 | 50 | 200 |
| 0.18% NaCl/4% glucose | 31 | – | 31 | – | – | 40 | 160 |
| 5% glucoseb | – | – | – | – | – | 50 | 200 |
5. LIMITATIONS
The study was limited by its cross-sectional nature and self-reported information that can be biased in its response. There was possible limitation on generalizability as the sample included only anesthetists in selected institutions. Also, the clinical outcomes regarding the fluid choices were not measured.
6. CONCLUSION
This study reveals notable variability in perioperative fluid practices among anesthetists, despite the known risks of hyponatremia and cerebral edema. Isotonic fluids are appropriately favored in older pediatric patients. These findings highlight the need for standardized guidelines and targeted educational initiatives to ensure safe, evidence-based fluid management across all pediatric age groups.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
RJ: Main concept
NARN: Conduction of the study work
MB: Manuscript editing
SSA: Literature search
HD: Proof reading
MAZ: Final review
11. REFERENCES
- Yin GM, Chen JH, Xu W. Knowledge, Attitudes and Practices of Patients from the Anesthesia Clinic in Jinshan District, Shanghai, Regarding Visiting the Anesthesia Clinic. Patient Prefer Adherence. 2025 Feb 18; 19:363-372. DOI: https://doi.org/10.2147/PPA.S496835 . PMCID: PMC11846519.
- Tütüncü AÇ, Hatipoğlu Z, Cebeci H, Çopuroğlu E, Altun D, Ustalar Özgen SZ. Perioperative Anaesthetic Approaches to Paediatric Patients: A National Survey. Turk J Anaesthesiol Reanim. 2025 May 30;53(3):98-106. doi: https://doi.org/10.4274/TJAR.2025.252053 . Epub 2025 May 27. PMID: 40423561; PMCID: PMC12123655.
- Lee H, Kim JT. Pediatric perioperative fluid management. Korean J Anesthesiol. 2023 Dec;76(6):519-530. doi: https://doi.org/10.4097/kja.23128. Epub 2023 Apr 19. PMID: 37073521; PMCID: PMC10718623.
- Mathew A, Rai E. Pediatric perioperative fluid management. Saudi J Anaesth. 2021 Oct-Dec;15(4):435-440. doi: https://doi.org/10.4103/sja.sja_140_21 . Epub 2021 Sep 2. PMCID: PMC8477784.
- Beels M, Stevens S, Saldien V. Perioperative fluid management in children: an updated review. Acta anaesthesiologica belgica/Belgische Vereniging voor Anesthesie en Reanimatie; Society for Anesthesia and Resuscitation of Belgium. -Brussel, 1950, currens. 2022;73(3):179-89.
- Sakkanan NV, Swaminathan S, Bidkar PU, Vairappan B, Sathiaprabhu A, Dey A. Comparison of the efficacy of 0.9% normal saline with balanced crystalloid (Plasmalyte) in maintaining the metabolic profile in head injury patients undergoing evacuation of acute subdural haematoma - A randomised controlled trial. Indian J Anaesth. 2024 Jun;68(6):553-559. doi: https://doi.org/10.4103/ija.ija_1160_23 . Epub 2024 May 8. PMCID: PMC11186531.
- Voet M, Cornelissen EAM, van der Jagt MFP, Lemson J, Malagon I. Perioperative anesthesia care for the pediatric patient undergoing a kidney transplantation: An educational review. Paediatr Anaesth. 2021 Nov;31(11):1150-1160. doi: https://doi.org/10.1111/pan.14271 . Epub 2021 Aug 20. PMCID: PMC9292670.
- Beckman EJ, Hovey S, Bondi DS, Patel G, Parrish RH 2nd. Pediatric Perioperative Clinical Pharmacy Practice: Clinical Considerations and Management: An Opinion of the Pediatrics and Perioperative Care Practice and Research Networks of the American College of Clinical Pharmacy. J Pediatr Pharmacol Ther. 2022;27(6):490-505. doi: https://doi.org/10.5863/1551-6776-27.6.490 . Epub 2022 Aug 19. PMCID: PMC9400189.
- Sbaraglia F, Cuomo C, Della Sala F, Festa R, Garra R, Maiellare F, Micci DM, Posa D, Pizzo CM, Pusateri A, Spano MM, Lucente M, Rossi M. State of the Art in Pediatric Anesthesia: A Narrative Review about the Use of Preoperative Time. J Pers Med. 2024 Feb 6;14(2):182. doi: https://doi.org/10.3390/jpm14020182 . PMCID: PMC10890671.
- Colomina MJ, Galán Menéndez P, Ripollés-Melchor J. Use of fluid therapy in perioperative adult patients: A narrative review. Rev Esp Anestesiol Reanim (Engl Ed). 2024 Dec;71(10):748-759. doi: https://doi.org/10.1016/j.redare.2024.09.003 . Epub 2024 Sep 5. PMID: 39243813.
- Karim R, Afridi JK, Afaq S, Zaman MB, Naeem S, Zaman MA. Comparison of sodium abnormalities associated with hypotonic versus isotonic maintenance infusions in hospitalized children. Journal of Medical Sciences. 2023 Nov 14;31(4):337-41. https://doi.org/10.52764/jms.23.31.4.16 .
- Shahbaz S, Zakar R, Howard N. Anaesthesia provision challenges in public hospitals of Pakistan's Punjab province: a qualitative study of expert perspectives. BMJ Open. 2023 Dec 21;13(12): e075108. doi: https://doi.org/10.1136/bmjopen-2023-075108 . PMCID: PMC10748997.
- Ciccozzi A, Pizzi B, Vittori A, Piroli A, Marrocco G, Della Vecchia F, Cascella M, Petrucci E, Marinangeli F. The Perioperative Anesthetic Management of the Pediatric Patient with Special Needs: An Overview of Literature. Children (Basel). 2022 Sep 21;9(10):1438. doi: https://doi.org/10.3390/children9101438. PMCID: PMC9600107.
- Puri S, Bandyopadhyay A, Ashok V. Supplemental intraoperative crystalloids for pediatric postoperative nausea and vomiting-A systematic review and meta-analysis. Paediatr Anaesth. 2023 Jan;33(1):38-45. doi: https://doi.org/10.1111/pan.14566 . Epub 2022 Oct 8. PMID: 36178763.
- Rasool Q, Nazir A, Batool F, Zahir J, Malik A, Aziz T. Effect of intravenous fluid therapy on postoperative vomiting in children undergoing tonsillectomy. Journal of Islamic International Medical College (JIIMC). 2022 Mar 28;17(1):19-24.
- Mahboba JH, Mohammed ZF. Recovery from Sevoflurane Anesthesia: A Comparism with Isoflurane Anesthesia in pediatric undergo tonsillectomy with or without adenoidectomy under general anesthesia. Pakistan Journal of Life & Social Sciences. 2024 Jan 1;22(1). https://doi.org/10.57239/PJLSS-2024-22.1.00250