Chee Kean Chen 1* , Nizar Abd Jalil 2 , Vui Eng Phui 3
Authors affiliations:
Background & objectives: Lumbar discogenic pain is a common cause of low back pain and remains difficult to treat. This study aims to evaluate the clinical outcome in terms of changes in pain intensity, functional improvement, and the safety profile of intradiscal bipolar radiofrequency (RF) annuloplasty in the treatment of lumbar discogenic pain.
Methodology: Between January 2019 and December 2021, medical records of all patients with lumbar discogenic pain who underwent intradiscal bipolar RF annuloplasty were retrospectively reviewed and analyzed. Outcomes on pain reduction were measured using a numerical rating scale (NRS), and functional status was measured using the Oswestry Disability Index (ODI) at baseline and at 1, 6, and 12 months. Differences in the NRS and ODI during subsequent follow-up visits with baseline measurements were calculated with repeated-measure analysis of variance (ANOVA).
Results: A total of 103 patients were included in the analysis. The average patient’s age was 42.51 ± 10.81 years, and there were 71.8% females. The proportion of patients who reported ≥50% reduction in the NRS was 82.5%, 86.4%, and 75.7% at 1, 6, and 12-month follow-up periods, respectively. The NRS was reduced from 7.39 ± 0.94 at baseline to 3.46 ± 1.30 at 12 months after treatment (P < 0.001). The ODI improved from 56.91 ± 8.61 to 32.04 ± 9.28 at 12 months after treatment (P < 0.001). No procedure-related complications were reported.
Conclusion: The high ratio of patients who showed considerable pain relief with the treatment of lumbar discogenic pain with intradiscal bipolar RF annuloplasty proves that this interventional procedure is effective and safe. This procedure can be another treatment option for patients who fail conservative medical treatment.
Abbreviations: IDET: intradiscal electrothermal therapy, RF: radiofrequency, NRS: Numeric Rating Scale, HIZ: high-intensity zone, ODI: Oswestry Disability Index, SPSS: Statistical Package for Social Sciences, ANOVA: analysis of variance, BMI: body mass index
Keywords: Annulus fibrosus; Intervertebral disc degeneration; Low back pain; Radiofrequency ablation; Safety; Treatment outcome
Citation: Chen CK, Jalil NA, Phui VE. Efficacy and safety of intradiscal bipolar radiofrequency annuloplasty in patients diagnosed with lumbar discogenic pain. Anaesth. pain intensive care 2025;29(8):841-849.
DOI: 10.35975/apic.v29i6.3005
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
Lumbar discogenic pain is a multifactorial pain syndrome that involves mechanical low back pain with or without radicular symptoms, in conjunction with radiological findings of degenerative disc disease. It has been shown that this condition is the most common source of low back pain. As high as 40% of chronic low back pain cases are reported as discogenic in etiology.1
The initial treatment of lumbar discogenic pain generally consists of conservative methods, such as rest, lifestyle and activity modification, analgesics, and physiotherapy. However, there is a big portion of lumbar discogenic pain patients who fail to respond to conservative treatments. This group of patients may benefit from various percutaneous intradiscal treatments that have been introduced in recent years. Being the center of discussion, the posterior annulus has attracted various treatment modalities and approaches. The mechanism of intradiscal treatments is to alter internal disc structure and mechanics, as well as ablate the nerve supply of the disc. The intradiscal treatments include intradiscal electrothermal therapy (IDET), cooled radiofrequency (RF) biacusplaty, radiofrequency nucleo-annuloplasty with Disc-Fx, intradiscal RF annuloplasty, either pulsed or conventional, monopolar or bipolar configurations. All these modalities have shown various degrees of success in treating discogenic low back pain.2,3
Compared with monopolar thermocoagulation, bipolar RF annuloplasty is a more recent technique in treating lumbar discogenic pain. The lesions created by bipolar RF annuloplasty are larger than those created by monopolar thermocoagulation, and thus, it is expected to increase the efficacy of treatment.4 Results from a small case series, as well as a cohort study comparing intradiscal monopolar and bipolar RF thermocoagulation, showed that intradiscal bipolar RF thermocoagulation could be an efficacious long-term treatment option in those with discogenic low back pain.5
This retrospective study aims to report the one-year outcomes, efficacy, and safety of bipolar RF annuloplasty procedure for the treatment of discogenic low back pain.
Using a retrospective observational study design, the medical records of all patients with lumbar discogenic pain undergoing bipolar intradiscal RF annuloplasty at KPJ Kuching Specialist Hospital and KPJ Sentosa Specialist Hospital, Malaysia, between January 2019 and December 2021 were reviewed. This retrospective study was approved by Clinical Research Center Kuching with research identification number: RSCH ID-22-04216-WFQ. Written informed consent was not required, as all data were retrospectively collected from patients’ records.
The inclusion criteria were: 1) axial low back pain greater than leg pain for a period longer than six months, that might be aggravated by prolonged sitting, coughing, or sneezing; 2) baseline Numeric Rating Scale (NRS) score of at least 4; 3) failure of conservative measures (medication and physical therapy) within the previous four to six weeks; 4) affected disc height of at least 50% of the adjacent disc; 5) tenderness upon palpation of the relevant level spinous processes; 6) disc with high-intensity zone (HIZ) on lumbar magnetic resonance imaging; 7) positive response to provocative discogram; and 8) single-level disc disease.
The exclusion criteria were: 1) radicular pain, leg pain more than low back pain; 2) spondylolisthesis greater than grade I; 3) spinal stenosis with canal anteroposterior diameter less than 8 mm; 4) significant neurological deficit; 5) pain due to spinal infection, fracture, or malignancy; and 6) bleeding tendency.
During provocative discography, the two adjacent levels (control discs) were stimulated first, while the suspicious level was stimulated last. Under fluoroscopy, the final location of the needle was verified in the center of the discs, and 1.5 to 2.5 mL of Iohexol was injected into the nucleus at a rate of 0.05 mL/s. Patients were assessed for pain response during the injection. Only patients with concordant pain (with NSR score of at least 6) at the suspicious level, and with no pain or discordant pain at the adjacent levels, were offered bipolar RF annuloplasty.
For patients eligible for treatment, informed consent was obtained after explaining the benefits and potential adverse effects of bipolar intradiscal radiofrequency (RF) annuloplasty, including infection (discitis), allergic reactions, transient radicular pain, and bleeding.
2.1. Bipolar Intradiscal Radiofrequency Annuloplasty
Resuscitation medications and equipment were prepared prior to the procedure. The patient’s hemodynamic status (ie, blood pressure, oxygen saturation, and electrocardiogram) was monitored closely throughout the procedure. The procedure was performed under an aseptic technique throughout. The patient was in the prone position on a radiolucent table with a pillow underneath the abdomen to reduce lumbar lordosis. Cefuroxime 1.5 g, Fentanyl 50 mcg, and Midazolam 2 mg were given intravenously. The C-arm of the fluoroscope was positioned in the axial plane to identify the targeted intervertebral space. The C-arm was then turned cephalo-caudal to square the end plates of the vertebrae. Subsequently, the C-arm was turned laterally
(obliquely) so that the superior articular process was positioned at the junction of the lateral and middle thirds of the vertebral body. The needle entry site was lateral to the superior articular process, in between the two vertebral endplates. The skin entry site was anesthetized with 0.5–1.0 ml of 1% lidocaine superficially. A 20-gauge, 10-cm or 15-cm, sharp and curved RF-insulated cannula with an active tip of 10 mm was inserted and advanced in a tunnel view method until increased resistance was felt, which signified an annular puncture. The C-arm was then positioned to obtain a lateral view, and the cannula was further advanced until the tip of the cannula was at the junction of the posterior and middle thirds of the vertebral body. In the axial view, the tip of the cannula should be close to the center of the vertebral body. A second similar RF cannula was similarly inserted on the contralateral side to the first RF cannula. Final cannula placement was confirmed in both the lateral and axial views, with the distance between both cannula tips being around 10 mm apart in the axial view, as shown in Figure 1.
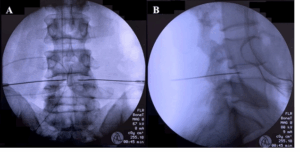
Figure 1: Intradiscal bipolar RF annuloplasty procedure. Anteroposterior and lateral views show that the RF cannulas are positioned in the L4/5 intervertebral disc.
Sensory stimulation was carried out at 100 Hz and 0.5 V, while motor stimulation was carried out at 2 Hz and 1.0 V to exclude segmental nerve root stimulation. The impedance measurement was lower than 400 ohms. Bipolar intradiscal RF annuloplasty was performed at 80°C with the two electrodes heated simultaneously for 90 seconds using a G4 Radiofrequency Generator (Cosman Medical, Burlington, USA). A second lesion at 80°C for 90 seconds was made after both cannulas were withdrawn by 3 mm. Both the cannulas were withdrawn once the tip temperature decreased to 40°C, and a sterile dressing was applied. The patient was transferred to the recovery bay for 15 minutes of hemodynamic monitoring. The patient was discharged home with oral celecoxib 400 mg daily, pantoprazole 40 mg daily, and paracetamol 1 g, three times daily for five days to relieve post-procedural needle soreness.
2.2. Data Collection
After the identification of eligible cases using a computerized clinic registry, medical records, procedure charts, and follow-up questionnaires of all patients were reviewed. Confidential and de-identified data collected included patient demographics such as age, gender, body mass index, and occupation; and clinical data such as diagnosis, duration of pain, disc level treated, previous treatment, other associated treatments, adverse effects, and complications from the procedure.
The objective of the study was to evaluate the analgesic efficacy of intradiscal bipolar RF annuloplasty using NRS, which measures pain from no pain to worst possible pain on a 0–10 scale, and the functional improvement using the Oswestry Disability Index (ODI) with scores ranging from 0 to 100, with the higher index reflecting the person’s greater disability from pain. The primary outcome was the proportion of patients who achieved successful outcomes after treatment. Successful outcomes were defined as a reduction in NRS of ≥ 50% or an ODI reduction of ≥ 40% during each follow-up interval. NRS and ODI were recorded in the form of questionnaires during clinic visits before treatment (baseline), at 3 months, 6 months, and 1 year after treatment.
Although data were analyzed at approximately 1, 6, and 12-month time frames, follow-up time points were not precise due to patient and clinic scheduling constraints.
The data were analyzed using Statistical Package for Social Sciences (SPSS) software version 25.0. Descriptive statistics of the data were presented as a mean and standard deviation. Frequency and descriptive statistics were calculated to check all relevant data characteristics. Differences in NRS and ODI during subsequent follow-up visits with baseline measurements were measured with repeated-measure analysis of variance (ANOVA) followed by post hoc analysis with Bonferroni’s multiple comparison test. P < 0.05 was considered statistically significant.
Between January 2019 and December 2021, a total of 157 patients underwent intradiscal bipolar radiofrequency (RF) annuloplasty for lumbar discogenic pain. As both institutions were referral pain centers, and many patients traveled long distances, a number of them were lost to follow-up. Patients who were lost to follow-up or had incomplete data were excluded from the study. Patients with other causes of low back pain who received interventional pain treatments, such as RF ablation of the lumbar medial branch for facet joint pain or RF sacral lateralis for sacroiliac joint pain, during the follow-up period were also excluded. Consequently, the findings presented in this study were derived from the complete data of 103 patients (Figure 2).

Figure 2: Flow chart of the study
There were 29 male and 74 female patients with a mean age of 43 ± 10.8 years in this study. The mean body mass index (BMI) of patients was 26.28 kg/m2. The mean duration of pain was 13.5 ± 5.6 months. During the period of observation, none of the patients required repeat bipolar RF annuloplasty. Demographic data and clinical presentation of patients are summarized in Table 1.
Table 2 summarizes the outcome of our series. The percentages of patients who achieved ≥ 50% reduction in NRS were 82.5%, 86.4%, and 75.7% of the total sample at 1, 6, and 12 months, respectively.
As for functional status, the proportions of patients who achieved ≥ 40% reduction in ODI were 76.7%, 73.8%, and 70.9% of the total sample at 1, 6, and 12 months after treatment, respectively.
Pain relief and functional status improved significantly at every follow-up interval. Baseline NRS decreased from 7.39 ± 0.94 to 3.13 ± 1.12 at 1 month, 2.96 ± 1.18 at 6 months, and 3.46 ± 1.30 at 12 months post-treatment, P < 0.001. Functionally, mean ODI decreased from 56.91 ± 8.613 at baseline to 31.01 ± 8.354 at 1 month, 31.17 ± 8.343 at 6 months, and 32.04 ± 9.276 at 12 months post-treatment, P < 0.001 (Table 3 and Figure 3). In this study, we did not encounter any procedural-related complications such as infection, discitis, hematoma formation, nerve root trauma, or spinal cord injury.
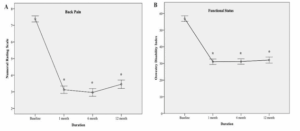
Figure 3: Numerical rating scale (NRS), and Oswestry disability index (ODI) at baseline 1, 6, and 12 months after the intradiscal bipolar RF annuloplasty. * P < 0.001 vs. baseline. The data are presented as the estimated mean ± 95% confidence interval.
Currently available evidence shows that discogenic pain is due to internal disc disruption. This is characterized by nuclear matrix degradation and radial fissures within the disc. The degraded matrix activates surrounding nociceptors6 and the radial fissures enhance the growth of new nerves.7 Disrupted disc exhibits an abnormal physical stress profile, with significantly increased stress being found in the posterior annulus fibrosis, which could be the source of mechanical pain.8 Thus, any modality's efficacy in treating discogenic pain depends on two important factors: the needle's location and the lesion's size.
It is rational that any technique to disrupt the transmission of pain signals in the management of discogenic pain should be targeted at the posterior annulus fibrosis. Previous literature has consistently supported these findings; earlier studies in which the final needle placement was at the center of the nucleus pulposus demonstrated lower efficacy9 and shorter duration of pain relief 10 in comparison with later studies in which the neurotomy was targeted at the posterior part of the intervertebral disc.5,11,12
Intradiscal electrothermal therapy (IDET) is a treatment modality where a navigable catheter is inserted into the disc so that thermocoagulation takes place at the inner posterior annulus. However, meta-analyses of the available studies on the efficacy and complications of IDET yield controversial conclusions.13 Difficulty in maneuverability and procedure-related complications, which include catheter breakage, nerve root injury, disc herniation, cauda equina syndrome, infection, epidural abscess, and spinal cord damage, resulted in IDET falling out of favor in current practice.14
Radiofrequency technology has been used as a method of nociceptive transmission modulation in the management of various chronic pain conditions, either non-ablative (pulsed radiofrequency) or ablative (conventional or cooled radiofrequency) methods.15
The non-destructive neural modulation effect of pulsed RF has been utilized in treating discogenic pain, but the results could have been more impressive and conclusive. For efficacy assessment of six months, a comparison study by Fukui et al. showed that intradiscal pulsed RF was as effective as IDET in treating lumbar discogenic pain.16 However, in a prospective study of 26 participants, Jung et al. at 12 months showed a modest effect with only 42% of the treated group having a successful clinical outcome, which was defined as more
than a 2-point reduction in pain score at the end of the study.17 Rohof also reported on the use of pulsed RF for the treatment of discogenic pain in 76 patients. After secondary sources of pain were treated accordingly, only 56% of all the patients had more than 50% pain relief 12 months after treatment.18 In a more recent study by Park et al. investigating the duration effect of pulsed RF on chronic lumbar discogenic pain, both 7 and 15 minutes of pulsed RF were effective up to a 6-month follow-up.19 All four studies utilized monopolar pulsed RF.
DiscTrode is another treatment modality utilizing conventional RF in which a navigable electrode is placed at the posterior annulus. In a case-control study reported by Finch et al., patients who received RF annuloplasty with DicsTrode showed a significant decrease in VAS and ODI compared to the control group, even up to 12 months post-treatment.20 However, similar findings were not reproducible in a subsequent randomized controlled trial. DiscTrode was found to have no beneficial effect in terms of pain score and functional improvement compared to the placebo group.21
Besides placing the radiofrequency needle accurately, the size of the neurotomy lesion also has to be reasonably large to accommodate the uncertain distribution of nerve endings in the posterior segment of the disc. This is in contrast to neurotomy of the medial branch of the dorsal rami in facet joint disease, where proximity to the targeted nerve can be confirmed by motor stimulation, which elicits contraction of paravertebral muscles.22 These shortcomings could be overcome by increasing the size of the RF neurotomy lesion with bipolar RF configuration, as the coverage area of two bipolar RF needles is larger compared to the single-needle monopolar RF technique.4,23,24 Bipolar RF configuration could be achieved using either cooled RF or conventional RF.
Intradiscal cooled RF, better known as biacuplasty, places two cooled RF probes at the posterior annulus in a bipolar configuration. In a randomized controlled trial by Desai et al., the combination of intradiscal biacuplasty and conservative medical management showed significant long-term effectiveness in pain reduction and functional improvement, compared with conservative medical management alone in patients with discogenic low back pain.12 However, more and more recent comparative studies show that conventional RF, which is simpler and easier to handle, is not inferior in treatment efficacy compared to a more complicated and costly cooled RF system.25
As for bipolar configuration with a conventional RF system, Zeng et al. in a randomized controlled trial showed that bipolar RF had significantly higher efficacy than monopolar RF in terms of pain score and modified Macnab criteria 6 months after treatment.5 Another prospective case series of 23 patients by Zhang et al. also showed that conventional bipolar RF annuloplasty was effective in treating discogenic pain, with 87% of patients having more than 50% pain reduction at 12 months post-treatment.11 The needle entry via the medial border of the facet joint approach was used in both studies, where dural puncture and penetration into the subarachnoid space were unavoidable to reach the disc.5,11 Three out of 23 patients suffered from post-dural puncture headaches in the later study.11
Unlike previous studies,5,11 the current study is the first case series reporting only a bilateral posterolateral needle approach to achieve bipolar configuration and utilizing a conventional RF system. The pain intensity scores (NRS) and functional capacity (ODI) showed significant improvement starting at 1 month after treatment, and the effect persisted until 12 months. At the 12-month follow-up, 78 patients (75.7%) had more than 50% pain relief. The results are comparable to the outcomes previously reported with bipolar RF annuloplasty in patients with discogenic pain. No procedural-related complications were reported in this study.
This study highlights the clinical application of conventional radiofrequency systems, a tool that is commonly available in most institutions managing chronic pain patients. In contemporary pain practice, patients with chronic low back pain usually have more than one pain generator, which might include facet joint disease, sacroiliac joint pain, lumbar radicular pain, and myofascial pain syndrome of the low back muscle. Conventional radiofrequency neurotomy is a well-established treatment modality for many pain conditions, such as facet joint disease and sacroiliac joint pain. Utilizing the same modality for different etiologies of pain might be more economical and time-saving. Patients who did not achieve significant pain reduction from this treatment were mainly those who had discogenic pain at the L5/S1 level, in which the iliac crest prevented satisfactory needle placement. The needle tips were placed too anteriorly and laterally in situ, hence an optimal strip of neurotomy lesioning was not achieved.
It is retrospective in design, with a relatively small sample size and no control group. We could not control and evaluate the use of analgesics during the follow-up periods, which might have affected the results of the current study. Only data from 103 out of 157 patients were complete and available for analysis, which introduces a risk of selection bias. The considerable number of patients lost to follow-up could have caused our results to show worse outcomes than presented, as those who did not turn up during follow-up might have had good pain relief effects after intradiscal bipolar RF annuloplasty. On the contrary, some patients might have turned to other specialties, especially to the spine team, when they did not achieve satisfactory pain relief after intradiscal bipolar RF annuloplasty. The findings of this study are still significant, as managing lumbar discogenic pain remains a challenge despite many modalities of treatment that have been tested in the last two decades.
The findings of the study indicate that bipolar intradiscal RF annuloplasty could lead to significant pain relief and functional improvement up to at least 12 months in patients with discogenic low back pain, and could be a useful alternative to overcome the limitations of other percutaneous treatments.
NAJ: study concept, data interpretation, manuscript preparation
VEP: data collection and analysis, manuscript writing, proofreading
13. REFERENCES
Authors affiliations:
- Chee Kean Chen, KPJ Kuching Specialist Hospital, Kuching, Malaysia; Email: chenck@hotmail.my; {ORCID:0000-0002-3522-5774}
- Nizar Abd Jalil, KPJ Kuching Specialist Hospital, Kuching, Malaysia; Email: nizaraj@gmail.com; {ORCID:0009-0008-1689-3276}
- Vui Eng Phui, KPJ Kuching Specialist Hospital, Kuching, Malaysia; Email: vephui@gmail.com; {ORCID:0009-0009-0648-3844}
ABSTRACT
Background & objectives: Lumbar discogenic pain is a common cause of low back pain and remains difficult to treat. This study aims to evaluate the clinical outcome in terms of changes in pain intensity, functional improvement, and the safety profile of intradiscal bipolar radiofrequency (RF) annuloplasty in the treatment of lumbar discogenic pain.
Methodology: Between January 2019 and December 2021, medical records of all patients with lumbar discogenic pain who underwent intradiscal bipolar RF annuloplasty were retrospectively reviewed and analyzed. Outcomes on pain reduction were measured using a numerical rating scale (NRS), and functional status was measured using the Oswestry Disability Index (ODI) at baseline and at 1, 6, and 12 months. Differences in the NRS and ODI during subsequent follow-up visits with baseline measurements were calculated with repeated-measure analysis of variance (ANOVA).
Results: A total of 103 patients were included in the analysis. The average patient’s age was 42.51 ± 10.81 years, and there were 71.8% females. The proportion of patients who reported ≥50% reduction in the NRS was 82.5%, 86.4%, and 75.7% at 1, 6, and 12-month follow-up periods, respectively. The NRS was reduced from 7.39 ± 0.94 at baseline to 3.46 ± 1.30 at 12 months after treatment (P < 0.001). The ODI improved from 56.91 ± 8.61 to 32.04 ± 9.28 at 12 months after treatment (P < 0.001). No procedure-related complications were reported.
Conclusion: The high ratio of patients who showed considerable pain relief with the treatment of lumbar discogenic pain with intradiscal bipolar RF annuloplasty proves that this interventional procedure is effective and safe. This procedure can be another treatment option for patients who fail conservative medical treatment.
Abbreviations: IDET: intradiscal electrothermal therapy, RF: radiofrequency, NRS: Numeric Rating Scale, HIZ: high-intensity zone, ODI: Oswestry Disability Index, SPSS: Statistical Package for Social Sciences, ANOVA: analysis of variance, BMI: body mass index
Keywords: Annulus fibrosus; Intervertebral disc degeneration; Low back pain; Radiofrequency ablation; Safety; Treatment outcome
Citation: Chen CK, Jalil NA, Phui VE. Efficacy and safety of intradiscal bipolar radiofrequency annuloplasty in patients diagnosed with lumbar discogenic pain. Anaesth. pain intensive care 2025;29(8):841-849.
DOI: 10.35975/apic.v29i6.3005
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Lumbar discogenic pain is a multifactorial pain syndrome that involves mechanical low back pain with or without radicular symptoms, in conjunction with radiological findings of degenerative disc disease. It has been shown that this condition is the most common source of low back pain. As high as 40% of chronic low back pain cases are reported as discogenic in etiology.1
The initial treatment of lumbar discogenic pain generally consists of conservative methods, such as rest, lifestyle and activity modification, analgesics, and physiotherapy. However, there is a big portion of lumbar discogenic pain patients who fail to respond to conservative treatments. This group of patients may benefit from various percutaneous intradiscal treatments that have been introduced in recent years. Being the center of discussion, the posterior annulus has attracted various treatment modalities and approaches. The mechanism of intradiscal treatments is to alter internal disc structure and mechanics, as well as ablate the nerve supply of the disc. The intradiscal treatments include intradiscal electrothermal therapy (IDET), cooled radiofrequency (RF) biacusplaty, radiofrequency nucleo-annuloplasty with Disc-Fx, intradiscal RF annuloplasty, either pulsed or conventional, monopolar or bipolar configurations. All these modalities have shown various degrees of success in treating discogenic low back pain.2,3
Compared with monopolar thermocoagulation, bipolar RF annuloplasty is a more recent technique in treating lumbar discogenic pain. The lesions created by bipolar RF annuloplasty are larger than those created by monopolar thermocoagulation, and thus, it is expected to increase the efficacy of treatment.4 Results from a small case series, as well as a cohort study comparing intradiscal monopolar and bipolar RF thermocoagulation, showed that intradiscal bipolar RF thermocoagulation could be an efficacious long-term treatment option in those with discogenic low back pain.5
This retrospective study aims to report the one-year outcomes, efficacy, and safety of bipolar RF annuloplasty procedure for the treatment of discogenic low back pain.
2. METHODOLOGY
Using a retrospective observational study design, the medical records of all patients with lumbar discogenic pain undergoing bipolar intradiscal RF annuloplasty at KPJ Kuching Specialist Hospital and KPJ Sentosa Specialist Hospital, Malaysia, between January 2019 and December 2021 were reviewed. This retrospective study was approved by Clinical Research Center Kuching with research identification number: RSCH ID-22-04216-WFQ. Written informed consent was not required, as all data were retrospectively collected from patients’ records.
The inclusion criteria were: 1) axial low back pain greater than leg pain for a period longer than six months, that might be aggravated by prolonged sitting, coughing, or sneezing; 2) baseline Numeric Rating Scale (NRS) score of at least 4; 3) failure of conservative measures (medication and physical therapy) within the previous four to six weeks; 4) affected disc height of at least 50% of the adjacent disc; 5) tenderness upon palpation of the relevant level spinous processes; 6) disc with high-intensity zone (HIZ) on lumbar magnetic resonance imaging; 7) positive response to provocative discogram; and 8) single-level disc disease.
The exclusion criteria were: 1) radicular pain, leg pain more than low back pain; 2) spondylolisthesis greater than grade I; 3) spinal stenosis with canal anteroposterior diameter less than 8 mm; 4) significant neurological deficit; 5) pain due to spinal infection, fracture, or malignancy; and 6) bleeding tendency.
During provocative discography, the two adjacent levels (control discs) were stimulated first, while the suspicious level was stimulated last. Under fluoroscopy, the final location of the needle was verified in the center of the discs, and 1.5 to 2.5 mL of Iohexol was injected into the nucleus at a rate of 0.05 mL/s. Patients were assessed for pain response during the injection. Only patients with concordant pain (with NSR score of at least 6) at the suspicious level, and with no pain or discordant pain at the adjacent levels, were offered bipolar RF annuloplasty.
For patients eligible for treatment, informed consent was obtained after explaining the benefits and potential adverse effects of bipolar intradiscal radiofrequency (RF) annuloplasty, including infection (discitis), allergic reactions, transient radicular pain, and bleeding.
2.1. Bipolar Intradiscal Radiofrequency Annuloplasty
Resuscitation medications and equipment were prepared prior to the procedure. The patient’s hemodynamic status (ie, blood pressure, oxygen saturation, and electrocardiogram) was monitored closely throughout the procedure. The procedure was performed under an aseptic technique throughout. The patient was in the prone position on a radiolucent table with a pillow underneath the abdomen to reduce lumbar lordosis. Cefuroxime 1.5 g, Fentanyl 50 mcg, and Midazolam 2 mg were given intravenously. The C-arm of the fluoroscope was positioned in the axial plane to identify the targeted intervertebral space. The C-arm was then turned cephalo-caudal to square the end plates of the vertebrae. Subsequently, the C-arm was turned laterally
(obliquely) so that the superior articular process was positioned at the junction of the lateral and middle thirds of the vertebral body. The needle entry site was lateral to the superior articular process, in between the two vertebral endplates. The skin entry site was anesthetized with 0.5–1.0 ml of 1% lidocaine superficially. A 20-gauge, 10-cm or 15-cm, sharp and curved RF-insulated cannula with an active tip of 10 mm was inserted and advanced in a tunnel view method until increased resistance was felt, which signified an annular puncture. The C-arm was then positioned to obtain a lateral view, and the cannula was further advanced until the tip of the cannula was at the junction of the posterior and middle thirds of the vertebral body. In the axial view, the tip of the cannula should be close to the center of the vertebral body. A second similar RF cannula was similarly inserted on the contralateral side to the first RF cannula. Final cannula placement was confirmed in both the lateral and axial views, with the distance between both cannula tips being around 10 mm apart in the axial view, as shown in Figure 1.
Figure 1: Intradiscal bipolar RF annuloplasty procedure. Anteroposterior and lateral views show that the RF cannulas are positioned in the L4/5 intervertebral disc.
Sensory stimulation was carried out at 100 Hz and 0.5 V, while motor stimulation was carried out at 2 Hz and 1.0 V to exclude segmental nerve root stimulation. The impedance measurement was lower than 400 ohms. Bipolar intradiscal RF annuloplasty was performed at 80°C with the two electrodes heated simultaneously for 90 seconds using a G4 Radiofrequency Generator (Cosman Medical, Burlington, USA). A second lesion at 80°C for 90 seconds was made after both cannulas were withdrawn by 3 mm. Both the cannulas were withdrawn once the tip temperature decreased to 40°C, and a sterile dressing was applied. The patient was transferred to the recovery bay for 15 minutes of hemodynamic monitoring. The patient was discharged home with oral celecoxib 400 mg daily, pantoprazole 40 mg daily, and paracetamol 1 g, three times daily for five days to relieve post-procedural needle soreness.
2.2. Data Collection
After the identification of eligible cases using a computerized clinic registry, medical records, procedure charts, and follow-up questionnaires of all patients were reviewed. Confidential and de-identified data collected included patient demographics such as age, gender, body mass index, and occupation; and clinical data such as diagnosis, duration of pain, disc level treated, previous treatment, other associated treatments, adverse effects, and complications from the procedure.
The objective of the study was to evaluate the analgesic efficacy of intradiscal bipolar RF annuloplasty using NRS, which measures pain from no pain to worst possible pain on a 0–10 scale, and the functional improvement using the Oswestry Disability Index (ODI) with scores ranging from 0 to 100, with the higher index reflecting the person’s greater disability from pain. The primary outcome was the proportion of patients who achieved successful outcomes after treatment. Successful outcomes were defined as a reduction in NRS of ≥ 50% or an ODI reduction of ≥ 40% during each follow-up interval. NRS and ODI were recorded in the form of questionnaires during clinic visits before treatment (baseline), at 3 months, 6 months, and 1 year after treatment.
Although data were analyzed at approximately 1, 6, and 12-month time frames, follow-up time points were not precise due to patient and clinic scheduling constraints.
The data were analyzed using Statistical Package for Social Sciences (SPSS) software version 25.0. Descriptive statistics of the data were presented as a mean and standard deviation. Frequency and descriptive statistics were calculated to check all relevant data characteristics. Differences in NRS and ODI during subsequent follow-up visits with baseline measurements were measured with repeated-measure analysis of variance (ANOVA) followed by post hoc analysis with Bonferroni’s multiple comparison test. P < 0.05 was considered statistically significant.
3. RESULTS
Between January 2019 and December 2021, a total of 157 patients underwent intradiscal bipolar radiofrequency (RF) annuloplasty for lumbar discogenic pain. As both institutions were referral pain centers, and many patients traveled long distances, a number of them were lost to follow-up. Patients who were lost to follow-up or had incomplete data were excluded from the study. Patients with other causes of low back pain who received interventional pain treatments, such as RF ablation of the lumbar medial branch for facet joint pain or RF sacral lateralis for sacroiliac joint pain, during the follow-up period were also excluded. Consequently, the findings presented in this study were derived from the complete data of 103 patients (Figure 2).
Figure 2: Flow chart of the study
There were 29 male and 74 female patients with a mean age of 43 ± 10.8 years in this study. The mean body mass index (BMI) of patients was 26.28 kg/m2. The mean duration of pain was 13.5 ± 5.6 months. During the period of observation, none of the patients required repeat bipolar RF annuloplasty. Demographic data and clinical presentation of patients are summarized in Table 1.
| Table 1: Baseline demographic characteristics and clinical presentation of patients | ||
| Variable | n = 103 | |
| Gender | Male | 29 (28.2) |
| Female | 74 (71.8) | |
| Age (year) | 42.51 ± 10.81 | |
| Height (m) | 1.62 ± 7.56 | |
| Weight (kg) | 68.93 ± 9.80 | |
| BMI | 26.28 ± 3.19 | |
| Occupation | Office | 55 (53.4) |
| Manual | 24 (23.3) | |
| Homemaker | 24 (23.3) | |
| Duration of pain (month) | 13.53 ± 5.65 | |
| Treated lumbar spine level | L2/3 | 2 (1.9) |
| L3/4 | 10 (9.7) | |
| L4/5 | 51 (49.5) | |
| L5/S1 | 40 (38.8) | |
| Data are expressed as mean ± standard deviation or numbers (%), n = number of patients, BMI: body mass index | ||
Table 2 summarizes the outcome of our series. The percentages of patients who achieved ≥ 50% reduction in NRS were 82.5%, 86.4%, and 75.7% of the total sample at 1, 6, and 12 months, respectively.
| Table 2: Primary outcome measures | ||
| Intervals | ≥ 50% reduction in NRS | ≥ 40% reduction in ODI |
| 1-month | 85 (82.5) | 79 (76.7) |
| 6-month | 89 (86.4) | 76 (73.8) |
| 12-month | 78 (75.7) | 73 (70.9) |
| Data are expressed as numbers (percentages), NRS: Numeric Rating Scale; ODI: Oswestry Disability Index | ||
As for functional status, the proportions of patients who achieved ≥ 40% reduction in ODI were 76.7%, 73.8%, and 70.9% of the total sample at 1, 6, and 12 months after treatment, respectively.
Pain relief and functional status improved significantly at every follow-up interval. Baseline NRS decreased from 7.39 ± 0.94 to 3.13 ± 1.12 at 1 month, 2.96 ± 1.18 at 6 months, and 3.46 ± 1.30 at 12 months post-treatment, P < 0.001. Functionally, mean ODI decreased from 56.91 ± 8.613 at baseline to 31.01 ± 8.354 at 1 month, 31.17 ± 8.343 at 6 months, and 32.04 ± 9.276 at 12 months post-treatment, P < 0.001 (Table 3 and Figure 3). In this study, we did not encounter any procedural-related complications such as infection, discitis, hematoma formation, nerve root trauma, or spinal cord injury.
Figure 3: Numerical rating scale (NRS), and Oswestry disability index (ODI) at baseline 1, 6, and 12 months after the intradiscal bipolar RF annuloplasty. * P < 0.001 vs. baseline. The data are presented as the estimated mean ± 95% confidence interval.
| Table 3: Mean pain and Oswestry Disability Index (ODI) outcomes of patients at different time points | |||||
| Outcome | Baseline | 1 month | 6 months | 12 months | P-value |
| NRS | 7.39 ± 0.94 | 3.13 ± 1.12 | 2.96 ± 1.18 | 3.46 ± 1.30 | < 0.001* |
| ODI | 56.91 ± 8.613 | 31.01± 8.354 | 31.17 ± 8.343 | 32.04 ± 9.276 | < 0.001* |
| Values are the mean ± standard deviation. Repeated-measure analysis of variance (ANOVA) was used to compare the means. Bonferroni correction was applied for differences at 1, 6, and 12 months versus baseline.*indicates a significant difference. NRS pain: Numeric Rating Scale for pain; ODI: Oswestry Disability Index. | |||||
4. DISCUSSION
Currently available evidence shows that discogenic pain is due to internal disc disruption. This is characterized by nuclear matrix degradation and radial fissures within the disc. The degraded matrix activates surrounding nociceptors6 and the radial fissures enhance the growth of new nerves.7 Disrupted disc exhibits an abnormal physical stress profile, with significantly increased stress being found in the posterior annulus fibrosis, which could be the source of mechanical pain.8 Thus, any modality's efficacy in treating discogenic pain depends on two important factors: the needle's location and the lesion's size.
It is rational that any technique to disrupt the transmission of pain signals in the management of discogenic pain should be targeted at the posterior annulus fibrosis. Previous literature has consistently supported these findings; earlier studies in which the final needle placement was at the center of the nucleus pulposus demonstrated lower efficacy9 and shorter duration of pain relief 10 in comparison with later studies in which the neurotomy was targeted at the posterior part of the intervertebral disc.5,11,12
Intradiscal electrothermal therapy (IDET) is a treatment modality where a navigable catheter is inserted into the disc so that thermocoagulation takes place at the inner posterior annulus. However, meta-analyses of the available studies on the efficacy and complications of IDET yield controversial conclusions.13 Difficulty in maneuverability and procedure-related complications, which include catheter breakage, nerve root injury, disc herniation, cauda equina syndrome, infection, epidural abscess, and spinal cord damage, resulted in IDET falling out of favor in current practice.14
Radiofrequency technology has been used as a method of nociceptive transmission modulation in the management of various chronic pain conditions, either non-ablative (pulsed radiofrequency) or ablative (conventional or cooled radiofrequency) methods.15
The non-destructive neural modulation effect of pulsed RF has been utilized in treating discogenic pain, but the results could have been more impressive and conclusive. For efficacy assessment of six months, a comparison study by Fukui et al. showed that intradiscal pulsed RF was as effective as IDET in treating lumbar discogenic pain.16 However, in a prospective study of 26 participants, Jung et al. at 12 months showed a modest effect with only 42% of the treated group having a successful clinical outcome, which was defined as more
than a 2-point reduction in pain score at the end of the study.17 Rohof also reported on the use of pulsed RF for the treatment of discogenic pain in 76 patients. After secondary sources of pain were treated accordingly, only 56% of all the patients had more than 50% pain relief 12 months after treatment.18 In a more recent study by Park et al. investigating the duration effect of pulsed RF on chronic lumbar discogenic pain, both 7 and 15 minutes of pulsed RF were effective up to a 6-month follow-up.19 All four studies utilized monopolar pulsed RF.
DiscTrode is another treatment modality utilizing conventional RF in which a navigable electrode is placed at the posterior annulus. In a case-control study reported by Finch et al., patients who received RF annuloplasty with DicsTrode showed a significant decrease in VAS and ODI compared to the control group, even up to 12 months post-treatment.20 However, similar findings were not reproducible in a subsequent randomized controlled trial. DiscTrode was found to have no beneficial effect in terms of pain score and functional improvement compared to the placebo group.21
Besides placing the radiofrequency needle accurately, the size of the neurotomy lesion also has to be reasonably large to accommodate the uncertain distribution of nerve endings in the posterior segment of the disc. This is in contrast to neurotomy of the medial branch of the dorsal rami in facet joint disease, where proximity to the targeted nerve can be confirmed by motor stimulation, which elicits contraction of paravertebral muscles.22 These shortcomings could be overcome by increasing the size of the RF neurotomy lesion with bipolar RF configuration, as the coverage area of two bipolar RF needles is larger compared to the single-needle monopolar RF technique.4,23,24 Bipolar RF configuration could be achieved using either cooled RF or conventional RF.
Intradiscal cooled RF, better known as biacuplasty, places two cooled RF probes at the posterior annulus in a bipolar configuration. In a randomized controlled trial by Desai et al., the combination of intradiscal biacuplasty and conservative medical management showed significant long-term effectiveness in pain reduction and functional improvement, compared with conservative medical management alone in patients with discogenic low back pain.12 However, more and more recent comparative studies show that conventional RF, which is simpler and easier to handle, is not inferior in treatment efficacy compared to a more complicated and costly cooled RF system.25
As for bipolar configuration with a conventional RF system, Zeng et al. in a randomized controlled trial showed that bipolar RF had significantly higher efficacy than monopolar RF in terms of pain score and modified Macnab criteria 6 months after treatment.5 Another prospective case series of 23 patients by Zhang et al. also showed that conventional bipolar RF annuloplasty was effective in treating discogenic pain, with 87% of patients having more than 50% pain reduction at 12 months post-treatment.11 The needle entry via the medial border of the facet joint approach was used in both studies, where dural puncture and penetration into the subarachnoid space were unavoidable to reach the disc.5,11 Three out of 23 patients suffered from post-dural puncture headaches in the later study.11
Unlike previous studies,5,11 the current study is the first case series reporting only a bilateral posterolateral needle approach to achieve bipolar configuration and utilizing a conventional RF system. The pain intensity scores (NRS) and functional capacity (ODI) showed significant improvement starting at 1 month after treatment, and the effect persisted until 12 months. At the 12-month follow-up, 78 patients (75.7%) had more than 50% pain relief. The results are comparable to the outcomes previously reported with bipolar RF annuloplasty in patients with discogenic pain. No procedural-related complications were reported in this study.
This study highlights the clinical application of conventional radiofrequency systems, a tool that is commonly available in most institutions managing chronic pain patients. In contemporary pain practice, patients with chronic low back pain usually have more than one pain generator, which might include facet joint disease, sacroiliac joint pain, lumbar radicular pain, and myofascial pain syndrome of the low back muscle. Conventional radiofrequency neurotomy is a well-established treatment modality for many pain conditions, such as facet joint disease and sacroiliac joint pain. Utilizing the same modality for different etiologies of pain might be more economical and time-saving. Patients who did not achieve significant pain reduction from this treatment were mainly those who had discogenic pain at the L5/S1 level, in which the iliac crest prevented satisfactory needle placement. The needle tips were placed too anteriorly and laterally in situ, hence an optimal strip of neurotomy lesioning was not achieved.
5. LIMITATIONS
It is retrospective in design, with a relatively small sample size and no control group. We could not control and evaluate the use of analgesics during the follow-up periods, which might have affected the results of the current study. Only data from 103 out of 157 patients were complete and available for analysis, which introduces a risk of selection bias. The considerable number of patients lost to follow-up could have caused our results to show worse outcomes than presented, as those who did not turn up during follow-up might have had good pain relief effects after intradiscal bipolar RF annuloplasty. On the contrary, some patients might have turned to other specialties, especially to the spine team, when they did not achieve satisfactory pain relief after intradiscal bipolar RF annuloplasty. The findings of this study are still significant, as managing lumbar discogenic pain remains a challenge despite many modalities of treatment that have been tested in the last two decades.
6. CONCLUSION
The findings of the study indicate that bipolar intradiscal RF annuloplasty could lead to significant pain relief and functional improvement up to at least 12 months in patients with discogenic low back pain, and could be a useful alternative to overcome the limitations of other percutaneous treatments.
- Further research
- Data availability
- Conflict of interest
- Funding
- Acknowledgements
- Authors’ contribution
NAJ: study concept, data interpretation, manuscript preparation
VEP: data collection and analysis, manuscript writing, proofreading
13. REFERENCES
- Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine 1995;20:1878-83. [PubMed] DOI: 1097/00007632-199509000-00008
- Manchikanti L, Hirsch JA. An update on the management of chronic lumbar discogenic pain. Pain Manag 2015;5:373-86. [PubMed] DOI: 2217/pmt.15.33
- Malik KM, Cohen SP, Walega DR, Benzon HT. Diagnostic criteria and treatment of discogenic pain: a systematic review of recent clinical literature. Spine J 2013;13:1675-89. [PubMed] DOI:1016/j.spinee.2013.06.063
- Cosman ER Jr, Gonzalez CD. Bipolar radiofrequency lesion geometry: implications for palisade treatment of sacroiliac joint pain. Pain Pract 2011;11:3-22.
[PubMed] DOI: 1111/j.1533-2500.2010.00400.x - Zeng Z, Yan M, Dai Y, Qiu W, Deng S, Gu X. Percutaneous bipolar radiofrequency thermocoagulation for the treatment of lumbar disc herniation. J Clin Neurosci. 2016;30:39–43. [PubMed] DOI: 1016/j.jocn.2015.10.050
- Hadjipavlou AG, Tzermiadianos MN, Bogduk N, Zindrick MR. The pathophysiology of disc degeneration: A critical review. J Bone Joint Surg. 2008;90:1261–70.
[PubMed] DOI: 1302/0301-620X.90B10.20910 - Peng B, Hao J, Hou S, Wu W, Jiang D, Fu X, et al. Possible pathogenesis of painful intervertebral disc degeneration. Spine. 2006;31:560–6.
[PubMed] DOI: 1097/01.brs.0000201324.45537.46 - Hansson TH, Keller TS, Spengler DM. Mechanical behaviour of the human lumbar spine. II. Fatigue strength during dynamic compressive loading. J Orthop Res. 1987;5:479–87.
[PubMed] DOI: 1002/jor.1100050403 - Barendse GA, van den Berg SG, Kessels AH, Weber WE, van Kleef M. Randomised controlled trial of percutaneous intradiscal radio-frequency thermo-coagulation for chronic discogenic back pain: lack of effect from a 90-second 70°C lesion. Spine. 2001;26:287–92.
[PubMed] DOI: 1097/00007632-200102010-00014 - Erçelen Ö, Bulutçu E, Öktenoglu T, Bozkus H, Özer F. Radiofrequency lesioning using two different time modalities for the treatment of lumbar discogenic low back pain: a randomized trial. Spine. 2003;28:1922–7.
[PubMed] DOI: 1097/01.BRS.0000083326.39944.73 - Zhang L, Ding XL, Zhao XL, Wang JN, Li YP, Tian M. Fluoroscopy-guided bipolar radiofrequency thermocoagulation treatment for discogenic low back pain. Chinese Med J. 2016;129:2313–8.
[PubMed] DOI: 4103/0366-6999.190682 - Desai MJ, Kapural L, Petersohn JD, Vallejo R, Menzies R, Creamer M, Gofeld M. Twelve-month follow-up of a randomized clinical trial comparing intradiscal biacuplasty to conventional medical management for discogenic lumbar back pain. Pain Med. 2017;18:751–63.
[PubMed] DOI: 1093/pm/pnw184 - Freeman BJ. IDET: a critical appraisal of the evidence. Eur Spine J. 2006;15(Suppl 3):S448–S457. [PubMed] DOI: 1007/s00586-006-0156-2
- Rathmell J, Saal JS, Saal J. Discography, IDET, percutaneous discectomy, and nucleoplasty: complications and their prevention. Pain Med. 2008;9(Suppl 1):S73–S81. Full Text.
- Chappell ME, Lakshman R, Trotter P, Abrahams M, Lee M. Radiofrequency denervation for chronic back pain: a systematic review and meta-analysis. BMJ Open. 2020;10:e035540.
[PubMed] DOI: 1136/bmjopen-2019-035540 - Fukui S, Nitta K, Iwashita N, Tomie H, Nosaka S, Rohof O. Results of intradiscal pulsed radiofrequency for lumbar discogenic pain: comparison with intradiscal electrothermal therapy. Korean J Pain. 2012;25:155–60.
[PubMed] DOI: 3344/kjp.2012.25.3.155 - Jung YJ, Lee DG, Cho YW, Ahn SH. Effect of intradiscal monopolar pulsed radiofrequency on chronic discogenic back pain diagnosed by pressure-controlled provocative discography: a one year prospective study. Ann Rehabil Med. 2012;36:648–56.
[PubMed] DOI: 5535/arm.2012.36.5.648 - ohof O. Intradiscal pulsed radiofrequency application following provocative discography for the management of degenerative disc disease and concordant pain: a pilot study. Pain Pract. 2012;12:342–9.
[PubMed] DOI: 1111/j.1533-2500.2011.00512.x - Park CH, Lee SH, Lee PB. Intradiscal pulsed radiofrequency application duration effect on lumbar discogenic low back pain. Pain Physician. 2020;23(5):E535–40.
[PubMed] PMID: 32967404 - Finch PM, Price LM, Drummond PD. Radiofrequency heating of painful annular disruptions: one-year outcomes. Clin Spine Surg. 2005;18:6–13.
[PubMed] DOI: 1097/01.bsd.0000143312.08303.5d - Kvarstein G, Måwe L, Indahl A, Hol PK, Tennøe B, Digernes R, et al. A randomized double-blind controlled trial of intra-annular radiofrequency thermal disc therapy–a 12-month follow-up. Pain. 2009;145:279–86.
[PubMed] DOI: 1016/j.pain.2009.05.001 - Koh JC, Lee YW, Choi JB, Ha DH, An JW. Relationship between paravertebral muscle twitching and long-term effects of radiofrequency medial branch neurotomy. Korean J Pain. 2017;30:296–303.
[PubMed] DOI:3344/kjp.2017.30.4.296 - Vallejo R, Benyamin R, Tilley DM, Kelley CA, Cedeño DL. An ex vivo comparison of cooled-radiofrequency and bipolar-radiofrequency lesion size and the effect of injected fluids. Reg Anesth Pain Med. 2014;39:312–21.
[PubMed] DOI:1097/AAP.0000000000000090 - Rohof O, Chen CK. The response to radiofrequency neurotomy of medial branches including a bipolar system for thoracic facet joints. Scand J Pain. 2018;18:747–53.
[PubMed] DOI: 1515/sjpain-2018-0048 - McCormick ZL, Choi H, Reddy R, Syed RH, Bhave M, Kendall MC, et al. Randomized prospective trial of cooled versus traditional radiofrequency ablation of the medial branch nerves for the treatment of lumbar facet joint pain. Reg Anesth Pain Med. 2019;44:389–97. [PubMed] DOI: 1136/rapm-2018-000035