Hien Van Vo 1, Quynh Van Nguyen 2, Thu Dang Nguyen 3, Nam Hoai Tran 4
Author affiliation:
Administering anesthesia to pediatric patients with maxillofacial post-burn contractures poses significant challenges, particularly due to anticipated difficulties in airway management. We report two cases involving children with severe perioral adhesive scar contractures that resulted in markedly restricted mouth opening. These cases illustrate the complexity of anesthetic planning in such scenarios and emphasize the need for individualized strategies to ensure safety and effectiveness. In both cases, flexible bronchoscopy-guided intubation was not feasible due to anatomical limitations. Instead, a two-stage anesthetic approach was employed: initial intravenous anesthesia combined with local infiltration for scar release, followed by the placement of a supraglottic airway (ProSeal™ laryngeal mask airway) to establish adequate ventilation. Both patients were managed successfully, with stable intraoperative hemodynamics and uneventful postoperative recovery.
Conclusion: Comprehensive preoperative airway evaluation is critical in pediatric patients with facial and cervical burn contractures. A staged anesthetic technique involving scar release under intravenous and local anesthesia can facilitate effective airway management and improve perioperative outcomes.
Abbreviations: LMA: laryngeal mask airway; ETI: endotracheal intubation; NIBP: non-invasive blood pressure; EtCO2: end-tidal carbon dioxide
Keywords: Airway; Airway Management; Difficult Endotracheal Intubation; Intravenous Anesthesia; Local Anesthesia; Post-Burn Scar Contracture; Surgical Release
Citation: Vo HV, Nguyen QV, Nguyen TD, Nam NH. Airway management in pediatric patients with severe post-burn oral contractures: A report of two cases. Anaesth. pain intensive care 2025;29(4):425-229. DOI: 10.35975/apic.v29i4.2832
Received: March 25, 2025; Revised: May 6, May 12, 2024; Accepted: May 20, 2025
Anesthesia for surgical procedures in patients with maxillofacial contracture scars remains a significant challenge due to the high likelihood of difficult endotracheal intubation (ETI). Selecting an appropriate ventilation and anesthesia strategy for each case is crucial. While flexible bronchoscopy-guided intubation, awake ETI, and emergency tracheostomy are conventional difficult airway management techniques commonly employed in clinical practice, there are no established guidelines for managing airways in burn-related difficult ETI cases.1 We present two cases of pediatric patients with severe post-burn oral stenosis who underwent successful anesthesia for reconstructive surgery at Le Huu Trac National Burn Hospital, Hanoi, Vietnam.
2.1. Case 1:
A 2-years-old female child, weighing 11 kg, was admitted to the hospital in October, 2023, with severe oral stenosis caused by post-burn contractures following a chemical injury. The burn occurred three months earlier due to accidental exposure to an unidentified drain cleaner, affecting the mouth, chest, back, and buttocks. Initial treatment was provided at Da Nang City Obstetrics and Pediatrics Hospital before referral for reconstructive surgery. Upon admission, the patient was conscious, hemodynamically stable, and breathing spontaneously with SpO2 of 99%. Airway examination revealed severe bilateral oral commissure contracture, limiting maximum mouth opening to < 0.5 cm (Mallampati class IV), though neck mobility was preserved. Nasopharyngoscopy confirmed normal airway anatomy from the external nostrils to the vocal cords (Figure 1) Bilateral oral commissure scar release via local flap transfer was planned.

a. Incision and release of oral commissure scar

b. Insertion of the LMA

c.Postoperative view after LMA removal

d. Clinical appearance before discharge
Figure 1: Preoperative appearance of the first patient at admission.
2.1.1. Anesthetic Management:
Phase 1: Oxygen was administered via nasal prongs (2 L/min), and standard monitoring (including ECG, NIBP, SpO2, EtCO2) was initiated. Anesthesia was induced with ketamine 20 mg IV and atropine 0.25 mg IV. After loss of consciousness, local infiltration with 0.5% lidocaine (6 mL) was performed at the surgical site, followed by incision and release of the scar contracture.
Phase 2: Once sufficient mouth opening was achieved, face mask ventilation with 100% oxygen was provided. Intravenous midazolam 1 mg, ketamine 20 mg, and fentanyl 20 µg, were then administered. A size 1.5 ProSeal laryngeal mask airway (LMA® ProsealTM, Teleflex Medical, Dublin, Ireland) was inserted and secured. Mechanical ventilation was initiated in assist-control (A/C) mode, with tidal volume: 110 mL, respiratory rate: 25 breaths/min, and I:E ratio 1:1.5, using the anesthesia machine (CarestationTM 620, GE Healthcare system). Anesthesia was maintained with propofol infusion @100 mg/h, and combined sevoflurane 1–2% (Figure 2). The surgery lasted for 40 min. The patient had an uneventful recovery, was extubated one hour later, and discharged after four days.

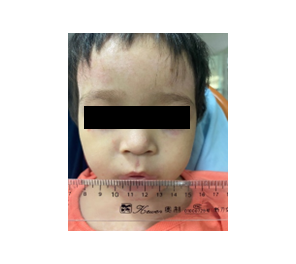
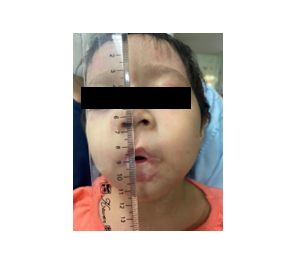
Figure 2: Intraoperative anesthetic and surgical steps with postoperative outcome
2.2. Case 2:
A 7-year-old male patient, weighing 19 kg was admitted on January 4, 2025, with burn injuries involving 21% of the total body surface area caused by a gasoline fire. The affected areas included the face, head, abdomen, and extremities. Following initial burn management, including intensive care, debridement, and skin grafting, severe facial contractures developed, requiring reconstructive surgery.
During the preoperative assessment, the patient was conscious but exhibited severely restricted mouth opening, which impaired his ability to speak. Although neck mobility was preserved, airway evaluation revealed bilateral oral commissure contractures, limiting maximal mouth opening to less than 0.5 cm, corresponding to Mallampati class IV (Figure 3).




Figure 3. Preoperative appearance of the second patient
Flexible bronchoscopy was deemed unfeasible due to extremely narrow nostrils. However, MRI and CT imaging confirmed no airway stenosis, and routine laboratory results were within normal limits. Scar excision with full-thickness Wolf-Krause skin grafting at the forehead was planned by the surgical colleagues.
2.2.1. Anesthetic Management
Phase 1:
Anesthesia was induced with propofol 100 mg IV and fentanyl 50 µg IV, followed by local infiltration of 0.5% lidocaine (10 mL) at the surgical site. Assisted ventilation via face mask was provided during scar release and mouth widening.
Phase 2:
Once mouth opening was sufficient, oxygen was continuously administered via a face mask, followed by propofol 80 mg IV and fentanyl 40 µg IV. A size 2.5-ProSeal LMA (LMA® ProsealTM, Teleflex Medical, Dublin, Ireland) was inserted, confirmed by capnographic waveform, and secured. Ventilation was maintained in Assist Control Volume Controlled Ventilation (A/C VCV) mode (tidal volume: 180 mL, respiratory rate: 22 breaths/min, I:E ratio = 1:2) on the anesthesia machine (CarestationTM 620, GE Healthcare system). Anesthesia was maintained with propofol 200 mg/h IV and additonal fentanyl 100 µg IV.
The surgery lasted for 120 min. Postoperatively, the patient was stable, and LMA was removed one hour later. The patient remained hospitalized for continued scar treatment.
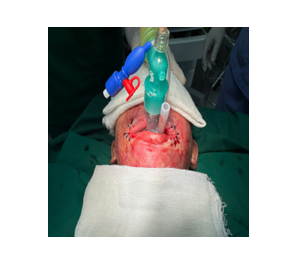
a. Perioperative mechanical ventilation via LMA

b. End of surgery
Figure 4. Airway management and end result
Post-burn scar contractures in the maxillofacial region significantly restrict mouth opening, neck mobility, and anatomical airway integrity, often leading to difficult ETI. In cases of burns, additional airway damage, such as nasopharyngeal and laryngeal stenosis, may occur. Thorough preoperative assessment, including airway imaging and nasopharyngoscopy, is critical for planning anesthesia and ventilation strategies. According to the current guidelines, conventional difficult airway management techniques include awake ETI, flexible bronchoscopy-guided intubation, and emergency tracheostomy. However, in severe cases, surgical release of contractures may be necessary before securing the airway. Tanzer (1964) was the first person to describe pre-intubation scar release to facilitate ETI, a method later validated in multiple studies.2 Kreulen M. (1996) reported 18 cases of difficult ETI among 52 patients undergoing surgery for burn-related scar contractures involving the head and neck region. In 10 of these cases, incision and release of contractures in the neck and oral regions were necessary prior to successful ETI. The authors further emphasized that, in emergency situations, prompt contracture scar release constitutes an effective and expedient method to secure a patent airway. This procedure can be safely performed under local anesthesia combined with mild sedation while the patient breathes spontaneously.3 Several authors have reported that in patients who are conscious and spontaneously breathing, endotracheal intubation may be performed under the guidance of flexible bronchoscopy.4-7
In our clinical cases, the primary factor contributing to difficult ETI was severe mouth opening restriction (Figure 1 and Figure 3) due to bilateral oral commissure adhesion scars resulting from respiratory burns. Consequently, direct placement of an ETT or supraglottic airway (LMA) through the mouth was impossible. However, based on the medical history, both patients were able to eat and drink without choking, speak audibly, and cry loudly. No symptoms of snoring or sleep apnea were observed. In the first case, nasopharyngoscopy was performed to evaluate the patency of the upper airway, from the external nostrils to the larynx and vocal cords. In the second case, flexible bronchoscopy was not feasible due to the extremely narrow nostril size, so we instead assessed the airway using MRI and a chest CT scan. The results confirmed that the upper airway was clear, without adhesions or narrowing caused by burns. Additionally, both patients had excellent neck mobility, allowing for maximum extension, which was a favorable factor for bag-valve-mask ventilation that could be applied for these patients.
However, in the first case, the patient’s young age posed a challenge, as cooperation during flexible bronchoscopy-guided awake intubation was difficult. This precluded the option of performing nasal intubation or using a flexible bronchoscope for guided intubation while the patient was awake and breathing spontaneously. Furthermore, awake ETI in these cases carried the risk of laryngospasm due to inadequate sedation, insufficient pain control, and the inability to completely suppress pharyngeal reflexes. In the second case, as mentioned earlier, flexible bronchoscopy was not an option due to the small nostril size. Given these constraints, we opted for intravenous anesthesia with ketamine combined with local lidocaine infiltration. The patients remained spontaneously breathing and received supplemental oxygen, with manual ventilation via a face mask if needed. This allowed the surgeon to perform an incision to release and widen the mouth before securing the airway with an LMA. The LMA anesthetic technique is perfectly suitable for short-term surgeries like ours and can even be applied to difficult endotracheal intubation situations.8 Anesthesia was then maintained using propofol combined with fentanyl, enabling the surgeon to proceed with the next stages of the procedure.
The most important phase of anesthesia in these cases was the initial release of the oral contracture scar, as this was the period when airway control was most precarious. Any ventilation failure or airway obstruction due to laryngospasm or excessive bleeding at this stage could lead to a life-threatening situation. In both cases, throughout this phase, respiratory and hemodynamic parameters remained stable and within acceptable limits.9
A key factor in the success of these procedures was the close coordination between the anesthesiologist and the surgical team. The surgeon had to operate swiftly to minimize the duration before the airway had been controlled while also being prepared for an emergency tracheostomy if required. In our cases, the time from induction of anesthesia to scar release and successful insertion of the LMA was approximately five minutes.
For pediatric patients with post-burn contracture scars leading to difficult ETI, thorough preoperative airway assessment and strategic anesthetic planning are essential. Surgical scar release before definitive airway management is an effective technique. Intravenous ketamine with local lidocaine anesthesia facilitates safe surgical intervention while preserving spontaneous ventilation. Close collaboration between anesthesiologists and surgeons is crucial for successful outcomes.
5. Ethical consideration
The study fully complies with the Declaration of Helsinki, a formal statement of ethical principles published by the World Medical Association (WMA). The anesthesia procedure applied in the study was approved according to Decision number 324/QD-BVB dated April 1st, 2020, issued by Le Huu Trac National Burn Hospital, Hanoi, Vietnam. Patient’s families were informed and written consent was obtained before the study was commenced. Throughout the entire study period, patient data was protected, and securely stored, and they gave their permission for data and images to be shared for research purposes.
6. Conflict of interest
The authors declare no conflict of interests, and no external or industry funding was involved.
7. Authors’ contribution
HVV: Participated in patient management, conceptualized the study, designed the methodology, collected and analyzed the data, and drafted the manuscript.
QVN: Participated in patient management, contributed to study design, collected and analyzed the data, and drafted the manuscript.
TDN, NHT: Collected and analyzed the data, and contributed to drafting the manuscript.
Author affiliation:
- Hien Van Vo, Department of Anaesthesia, Le Huu Trac National Burn Hospital, Vietnam Military Medical University, Ha Dong District, Ha Noi City, Vietnam; Email: vanhien@vmmu.edu.vn
- Quynh Van Nguyen, Department of Anaesthesia, Le Huu Trac National Burn Hospital, 263 Phung Hung Road, Phuc La Ward, Ha Dong District, Ha Noi City, Vietnam; Email: nguyenvanquynh304@gmail.com
- Thu Dang Nguyen, Department of Anaesthesia, Military Hospital 103, Vietnam Medical University, Hanoi, Vietnam; Email: nguyendangthu@vmmu.edu.vn
- Nam Hoai Tran Department of Anaesthesia, Military Hospital 103, Vietnam Medical University, Hanoi, Vietnam; Email: namb5v103@gmail.com
ABSTRACT
Administering anesthesia to pediatric patients with maxillofacial post-burn contractures poses significant challenges, particularly due to anticipated difficulties in airway management. We report two cases involving children with severe perioral adhesive scar contractures that resulted in markedly restricted mouth opening. These cases illustrate the complexity of anesthetic planning in such scenarios and emphasize the need for individualized strategies to ensure safety and effectiveness. In both cases, flexible bronchoscopy-guided intubation was not feasible due to anatomical limitations. Instead, a two-stage anesthetic approach was employed: initial intravenous anesthesia combined with local infiltration for scar release, followed by the placement of a supraglottic airway (ProSeal™ laryngeal mask airway) to establish adequate ventilation. Both patients were managed successfully, with stable intraoperative hemodynamics and uneventful postoperative recovery.
Conclusion: Comprehensive preoperative airway evaluation is critical in pediatric patients with facial and cervical burn contractures. A staged anesthetic technique involving scar release under intravenous and local anesthesia can facilitate effective airway management and improve perioperative outcomes.
Abbreviations: LMA: laryngeal mask airway; ETI: endotracheal intubation; NIBP: non-invasive blood pressure; EtCO2: end-tidal carbon dioxide
Keywords: Airway; Airway Management; Difficult Endotracheal Intubation; Intravenous Anesthesia; Local Anesthesia; Post-Burn Scar Contracture; Surgical Release
Citation: Vo HV, Nguyen QV, Nguyen TD, Nam NH. Airway management in pediatric patients with severe post-burn oral contractures: A report of two cases. Anaesth. pain intensive care 2025;29(4):425-229. DOI: 10.35975/apic.v29i4.2832
Received: March 25, 2025; Revised: May 6, May 12, 2024; Accepted: May 20, 2025
1. INTRODUCTION
Anesthesia for surgical procedures in patients with maxillofacial contracture scars remains a significant challenge due to the high likelihood of difficult endotracheal intubation (ETI). Selecting an appropriate ventilation and anesthesia strategy for each case is crucial. While flexible bronchoscopy-guided intubation, awake ETI, and emergency tracheostomy are conventional difficult airway management techniques commonly employed in clinical practice, there are no established guidelines for managing airways in burn-related difficult ETI cases.1 We present two cases of pediatric patients with severe post-burn oral stenosis who underwent successful anesthesia for reconstructive surgery at Le Huu Trac National Burn Hospital, Hanoi, Vietnam.
2. CASE REPORTS
2.1. Case 1:
A 2-years-old female child, weighing 11 kg, was admitted to the hospital in October, 2023, with severe oral stenosis caused by post-burn contractures following a chemical injury. The burn occurred three months earlier due to accidental exposure to an unidentified drain cleaner, affecting the mouth, chest, back, and buttocks. Initial treatment was provided at Da Nang City Obstetrics and Pediatrics Hospital before referral for reconstructive surgery. Upon admission, the patient was conscious, hemodynamically stable, and breathing spontaneously with SpO2 of 99%. Airway examination revealed severe bilateral oral commissure contracture, limiting maximum mouth opening to < 0.5 cm (Mallampati class IV), though neck mobility was preserved. Nasopharyngoscopy confirmed normal airway anatomy from the external nostrils to the vocal cords (Figure 1) Bilateral oral commissure scar release via local flap transfer was planned.
a. Incision and release of oral commissure scar
b. Insertion of the LMA
c.Postoperative view after LMA removal
d. Clinical appearance before discharge
Figure 1: Preoperative appearance of the first patient at admission.
2.1.1. Anesthetic Management:
Phase 1: Oxygen was administered via nasal prongs (2 L/min), and standard monitoring (including ECG, NIBP, SpO2, EtCO2) was initiated. Anesthesia was induced with ketamine 20 mg IV and atropine 0.25 mg IV. After loss of consciousness, local infiltration with 0.5% lidocaine (6 mL) was performed at the surgical site, followed by incision and release of the scar contracture.
Phase 2: Once sufficient mouth opening was achieved, face mask ventilation with 100% oxygen was provided. Intravenous midazolam 1 mg, ketamine 20 mg, and fentanyl 20 µg, were then administered. A size 1.5 ProSeal laryngeal mask airway (LMA® ProsealTM, Teleflex Medical, Dublin, Ireland) was inserted and secured. Mechanical ventilation was initiated in assist-control (A/C) mode, with tidal volume: 110 mL, respiratory rate: 25 breaths/min, and I:E ratio 1:1.5, using the anesthesia machine (CarestationTM 620, GE Healthcare system). Anesthesia was maintained with propofol infusion @100 mg/h, and combined sevoflurane 1–2% (Figure 2). The surgery lasted for 40 min. The patient had an uneventful recovery, was extubated one hour later, and discharged after four days.
Figure 2: Intraoperative anesthetic and surgical steps with postoperative outcome
2.2. Case 2:
A 7-year-old male patient, weighing 19 kg was admitted on January 4, 2025, with burn injuries involving 21% of the total body surface area caused by a gasoline fire. The affected areas included the face, head, abdomen, and extremities. Following initial burn management, including intensive care, debridement, and skin grafting, severe facial contractures developed, requiring reconstructive surgery.
During the preoperative assessment, the patient was conscious but exhibited severely restricted mouth opening, which impaired his ability to speak. Although neck mobility was preserved, airway evaluation revealed bilateral oral commissure contractures, limiting maximal mouth opening to less than 0.5 cm, corresponding to Mallampati class IV (Figure 3).
Figure 3. Preoperative appearance of the second patient
Flexible bronchoscopy was deemed unfeasible due to extremely narrow nostrils. However, MRI and CT imaging confirmed no airway stenosis, and routine laboratory results were within normal limits. Scar excision with full-thickness Wolf-Krause skin grafting at the forehead was planned by the surgical colleagues.
2.2.1. Anesthetic Management
Phase 1:
Anesthesia was induced with propofol 100 mg IV and fentanyl 50 µg IV, followed by local infiltration of 0.5% lidocaine (10 mL) at the surgical site. Assisted ventilation via face mask was provided during scar release and mouth widening.
Phase 2:
Once mouth opening was sufficient, oxygen was continuously administered via a face mask, followed by propofol 80 mg IV and fentanyl 40 µg IV. A size 2.5-ProSeal LMA (LMA® ProsealTM, Teleflex Medical, Dublin, Ireland) was inserted, confirmed by capnographic waveform, and secured. Ventilation was maintained in Assist Control Volume Controlled Ventilation (A/C VCV) mode (tidal volume: 180 mL, respiratory rate: 22 breaths/min, I:E ratio = 1:2) on the anesthesia machine (CarestationTM 620, GE Healthcare system). Anesthesia was maintained with propofol 200 mg/h IV and additonal fentanyl 100 µg IV.
The surgery lasted for 120 min. Postoperatively, the patient was stable, and LMA was removed one hour later. The patient remained hospitalized for continued scar treatment.
a. Perioperative mechanical ventilation via LMA
b. End of surgery
Figure 4. Airway management and end result
3. DISCUSSION
Post-burn scar contractures in the maxillofacial region significantly restrict mouth opening, neck mobility, and anatomical airway integrity, often leading to difficult ETI. In cases of burns, additional airway damage, such as nasopharyngeal and laryngeal stenosis, may occur. Thorough preoperative assessment, including airway imaging and nasopharyngoscopy, is critical for planning anesthesia and ventilation strategies. According to the current guidelines, conventional difficult airway management techniques include awake ETI, flexible bronchoscopy-guided intubation, and emergency tracheostomy. However, in severe cases, surgical release of contractures may be necessary before securing the airway. Tanzer (1964) was the first person to describe pre-intubation scar release to facilitate ETI, a method later validated in multiple studies.2 Kreulen M. (1996) reported 18 cases of difficult ETI among 52 patients undergoing surgery for burn-related scar contractures involving the head and neck region. In 10 of these cases, incision and release of contractures in the neck and oral regions were necessary prior to successful ETI. The authors further emphasized that, in emergency situations, prompt contracture scar release constitutes an effective and expedient method to secure a patent airway. This procedure can be safely performed under local anesthesia combined with mild sedation while the patient breathes spontaneously.3 Several authors have reported that in patients who are conscious and spontaneously breathing, endotracheal intubation may be performed under the guidance of flexible bronchoscopy.4-7
In our clinical cases, the primary factor contributing to difficult ETI was severe mouth opening restriction (Figure 1 and Figure 3) due to bilateral oral commissure adhesion scars resulting from respiratory burns. Consequently, direct placement of an ETT or supraglottic airway (LMA) through the mouth was impossible. However, based on the medical history, both patients were able to eat and drink without choking, speak audibly, and cry loudly. No symptoms of snoring or sleep apnea were observed. In the first case, nasopharyngoscopy was performed to evaluate the patency of the upper airway, from the external nostrils to the larynx and vocal cords. In the second case, flexible bronchoscopy was not feasible due to the extremely narrow nostril size, so we instead assessed the airway using MRI and a chest CT scan. The results confirmed that the upper airway was clear, without adhesions or narrowing caused by burns. Additionally, both patients had excellent neck mobility, allowing for maximum extension, which was a favorable factor for bag-valve-mask ventilation that could be applied for these patients.
However, in the first case, the patient’s young age posed a challenge, as cooperation during flexible bronchoscopy-guided awake intubation was difficult. This precluded the option of performing nasal intubation or using a flexible bronchoscope for guided intubation while the patient was awake and breathing spontaneously. Furthermore, awake ETI in these cases carried the risk of laryngospasm due to inadequate sedation, insufficient pain control, and the inability to completely suppress pharyngeal reflexes. In the second case, as mentioned earlier, flexible bronchoscopy was not an option due to the small nostril size. Given these constraints, we opted for intravenous anesthesia with ketamine combined with local lidocaine infiltration. The patients remained spontaneously breathing and received supplemental oxygen, with manual ventilation via a face mask if needed. This allowed the surgeon to perform an incision to release and widen the mouth before securing the airway with an LMA. The LMA anesthetic technique is perfectly suitable for short-term surgeries like ours and can even be applied to difficult endotracheal intubation situations.8 Anesthesia was then maintained using propofol combined with fentanyl, enabling the surgeon to proceed with the next stages of the procedure.
The most important phase of anesthesia in these cases was the initial release of the oral contracture scar, as this was the period when airway control was most precarious. Any ventilation failure or airway obstruction due to laryngospasm or excessive bleeding at this stage could lead to a life-threatening situation. In both cases, throughout this phase, respiratory and hemodynamic parameters remained stable and within acceptable limits.9
A key factor in the success of these procedures was the close coordination between the anesthesiologist and the surgical team. The surgeon had to operate swiftly to minimize the duration before the airway had been controlled while also being prepared for an emergency tracheostomy if required. In our cases, the time from induction of anesthesia to scar release and successful insertion of the LMA was approximately five minutes.
4. CONCLUSION
For pediatric patients with post-burn contracture scars leading to difficult ETI, thorough preoperative airway assessment and strategic anesthetic planning are essential. Surgical scar release before definitive airway management is an effective technique. Intravenous ketamine with local lidocaine anesthesia facilitates safe surgical intervention while preserving spontaneous ventilation. Close collaboration between anesthesiologists and surgeons is crucial for successful outcomes.
5. Ethical consideration
The study fully complies with the Declaration of Helsinki, a formal statement of ethical principles published by the World Medical Association (WMA). The anesthesia procedure applied in the study was approved according to Decision number 324/QD-BVB dated April 1st, 2020, issued by Le Huu Trac National Burn Hospital, Hanoi, Vietnam. Patient’s families were informed and written consent was obtained before the study was commenced. Throughout the entire study period, patient data was protected, and securely stored, and they gave their permission for data and images to be shared for research purposes.
6. Conflict of interest
The authors declare no conflict of interests, and no external or industry funding was involved.
7. Authors’ contribution
HVV: Participated in patient management, conceptualized the study, designed the methodology, collected and analyzed the data, and drafted the manuscript.
QVN: Participated in patient management, contributed to study design, collected and analyzed the data, and drafted the manuscript.
TDN, NHT: Collected and analyzed the data, and contributed to drafting the manuscript.
8. REFERENCES
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022;136(1):31-81. PubMed DOI: 1097/ALN.0000000000004002
- Tanzer RC. Burn contracture of the neck. Plast Reconstr Surg. 1964;33:207-12. PubMed DOI: 1097/00006534-196403000-00001
- Mackie DP, Kreulen M, Kreis RW, Groenevelt F. Surgical release for intubation purposes in postburn contractures of the neck. Burns. 1996;22(4):310-2. PubMed DOI: 1016/0305-4179(95)00138-7
- Sahoo M, Vig S. Managing difficult airway in a post burn neck contracture: a case report. J Clin Images Med Case Rep. 2023;4(11):2669. Full Text
- Mishra D, Chakole V, Dev P. Difficult airway management in a patient with post-burn contracture neck. Cureus. 2022;14(10):e30011. PubMed DOI: 7759/cureus.30011
- Erkalp K, Totoz T, Taskin S, Dalkilinc U, Selcan A. Use of awake flexible fiberoptic bronchoscopic nasal intubation in secure airway management for reconstructive surgery in a pediatric patient with burn contracture of the neck. Case Rep Anesthesiol. 2018;2018:8981561. PubMed DOI: 1155/2018/8981561
- Xue FS, Liao X, Li CW, Xu YC, Yang QY, Liu Y, et al. Clinical experience of airway management and tracheal intubation under general anesthesia in patients with scar contracture of the neck. Chin Med J (Engl). 2018;121(11):989-97. PubMed
- Seo DK, Kim JS, Lee CJ, Jung HS, Kim SS. Difficult intubation using intubating laryngeal mask airway in conjunction with a fiber optic bronchoscope. J Dent Anesth Pain Med. 2015;15(3):167-71. PubMed DOI: 17245/jdapm.2015.15.3.167
- Dang AK, Bali A, Gonzalez DA, Kumar R, Asif S. Clinical uses of ketamine in children: a narrative review. Cureus. 2022;14(7):e27065. PubMed DOI: 7759/cureus.27065