Umair Aftab Baig 1, Saima Rashid 2, Sadique Ali 3, Aiman Saeed Shah 4
Authors affiliations:
Tension pneumocephalus is a life-threatening condition that presents significant challenges for anesthesiologists, particularly in pediatric and adolescent patients. This case report details the perioperative management of a 17-year-old male who developed tension pneumocephalus following a road traffic accident, leading to multiple skull base fractures. In this case, comprehensive preoperative assessment, intraoperative anesthetic management, and postoperative care strategies employed to optimize the patient's outcome. A thorough preoperative evaluation is important in guiding intraoperative and postoperative decisions to avoid unnecessary Intensive Care Unit (ICU) admission.
Interdisciplinary collaboration between the surgical, anesthesiology, and endocrinology team is necessary to manage patient's condition effectively. The case report discusses diagnostic challenges, surgical interventions, and postoperative monitoring that led to the successful resolution of the patient's condition. This case shows the value of coordinated, patient-centered care in achieving favorable outcomes in complex cases of tension pneumocephalus.
Abbreviations: CT: Computed Tomography, GCS: Glasgow Coma Scale, CSF: Cerebrospinal Fluid, WBC: White Blood Count. CVC: Central Venous Catheter, CVP: Central Venous Pressure, CLABSI: Central Line Associated Blood Stream Infections
Keywords: Craniotomy; Interdisciplinary Approach; Pediatric patient; Road traffic accident; Skull base fracture; Tension pneumocephalus
Citation: Baig UA, Rashid S, Ali S, Shah AS. Perioperative anesthesia management of a pediatric patient with unique ‘Mushroom Head’ tension pneumocephalus: A case report. Anaesth. pain intensive care 2025;29(3):703-707. DOI: 10.35975/apic.v29i3.2774
Received: January 14, 2025; Revised: February 05, 2025; Accepted: March 20, 2025
Tension pneumocephalus (TP) is a rare, life-threatening complication often associated with skull base fractures, where air accumulates in the cranial cavity under pressure, compressing brain tissue. It occurs in approximately 0.1% to 0.2% of patients with head trauma and is typically linked to fractures of the anterior cranial fossa.1 The condition poses challenges in pediatric patients, where timely diagnosis and anesthetic management are necessary to prevent neurological damage or death.2
In pediatric cases, where patients may not always present with clear neurological symptoms, prompt identification of tension pneumocephalus becomes even more pivotal. The main diagnostic tool remains the CT scan, which reveals intracranial air and associated midline shifts indicative of increased ICP. The primary mechanism behind tension pneumocephalus is a one-way valve effect, where air enters the intracranial space through fractures in the cranial bones, but cannot escape, leading to rising ICP.3 The primary sources of air entry are fractures of the cranial bones, particularly those involving the paranasal sinuses, mastoid air cells, or the dura mater. This can result in severe complications, including brain herniation, ischemia, and, if left untreated, death.
Children and adolescents with tension pneumocephalus, particularly those following trauma, often present with non-specific symptoms such as severe headaches (44% of cases), nausea, vomiting, and altered mental status. Mental status changes occurred in 44% of tension pneumocephalus cases, with 28% of patients experiencing loss of consciousness at some point during their clinical course.4 As the condition progresses and ICP increases, neurological deficits, such as confusion, ethargy, or motor weakness, may emerge. These overlapping symptoms can complicate diagnosis, especially in pediatric patients who may not communicate symptoms as effectively. A high index of suspicion is therefore critical, especially in patients with skull fractures or cerebrospinal fluid (CSF) leaks. It is mostly found in 20% to 30% of patients with traumatic CSF fistula and can also occur in the patients who have no CSF rhinorrhea.5
The successful management of tension pneumocephalus involves not only surgical intervention but also comprehensive anesthetic care throughout the perioperative period. This case report stresses the role of interdisciplinary collaboration between neurosurgery, anesthesiology, and critical care teams in managing a 17-year-old male patient with tension pneumocephalus following a road traffic accident. The case features the importance of preoperative assessment, intraoperative anesthetic strategies, and postoperative care in preventing complications, minimizing the need for Intensive Care Unit (ICU) admission, and ensuring a favorable outcome.
A 17-year-old male presented to the emergency department with complaints of severe headache and vomiting for two days. One month prior, the patient had sustained multiple skull base fractures due to a road traffic accident (RTA), which were managed conservatively at the time.
On presentation, the patient was fully awake, alert, and oriented. His clinical observations, detailed in Table 1, indicated stable vital signs, and a positive provocation test for CSF rhinorrhea raised the suspicion of a CSF leak.
A computed tomography (CT) scan of the brain revealed the interval development of tension pneumocephalus, with a significant increase in left-sided midline shift from 5 mm to 10 mm (Figure 2).
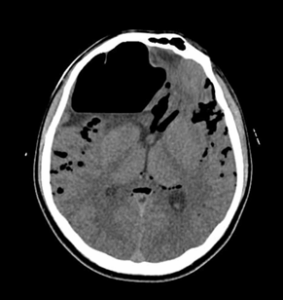
Figure 2: CT scan showing interval progression in “Mushroom Head” pneumocephalus
There is also significant tracking of air identified within the subarachnoid space and basal cisterns anteriorly (Figure 1). Mild cerebral edema is re-demonstrated. Previously seen small right frontal subdural and multifocal contusional hemorrhages are not appreciable on the current scan due to the presence of a large amount of air. The effacement of the frontal horn of the right lateral ventricle is re-demonstrated. The grey-white matter differentiation of the rest of the brain is preserved, and no hydrocephalus is noted. Basal cisterns are patent, and posterior fossa structures are grossly unremarkable. There is interval resolution of the intra-sinus hemorrhage and minimal fluid in the bilateral mastoids. Multiple craniofacial fractures are re-demonstrated. The patient’s laboratory parameters before and after surgery are outlined in Table 2. Preoperatively, the elevated white blood cell (WBC) count and neutrophil percentage indicated a potential inflammatory or infectious process.

Figure 1: CT scan showing pneumocephalus with air-fluid level in the right frontal region.
The patient was taken to the operating room for a modified right frontal craniotomy and repair of an anterior skull base defect. General anesthesia was induced without complications, and the surgical team took appropriate precautions based on the patient’s stable hemodynamic condition. Intraoperative monitoring was carefully chosen to meet the needs of the procedure, with arterial cannulation for blood pressure control and blood gas analysis, while central venous access and inotropic support were deemed unnecessary. Blood transfusion was required during the procedure, but no major complications were noted. The surgery proceeded smoothly, and the patient was successfully extubated in the operating room, following commands in the post-anesthesia care unit (PACU) without requiring intensive care unit (ICU) admission. The intraoperative findings confirmed
multiple fractures of the frontal bone, predominantly on the right side, and a large anterior skull base defect.
Table 3 shows intraoperative management. Postoperatively, the patient was managed with intravenous fluids, antibiotics, analgesics, and antiemetics. A lumbar drain was inserted to reduce the risk of worsening pneumocranium and was removed on postoperative day six. The patient's fluctuating sodium levels and polyuria prompted an endocrinological consultation, leading to a diagnosis of psychogenic polydipsia. His sodium levels were closely monitored, and he was discharged in stable condition on postoperative day 16, with specific instructions for follow-up care.
Despite advancements in neurosurgical techniques and anesthetic management, perioperative care in patients with tension pneumocephalus, particularly in pediatric populations, remains a challenge due to the rarity of the condition and the critical nature of intraoperative and postoperative decisions.6 This case report aims to contribute to the limited literature by outlining the successful anesthesia and surgical management of a 17-year-old patient with tension pneumocephalus.
The incidence of pneumocephalus is less than 1% in patients with head trauma, but it could reach 8% when fractures of either the paranasal sinus or the skull base presents.7 Tension pneumocephalus may develop if the intracranial air creates a mass effect on the brain, resulting in a possibly life-threatening neurosurgical emergency.
Tension pneumocephalus can lead to serious complications, primarily increased ICP, as air accumulation compresses brain tissue and causes midline shift, as in this case where the shift progressed from 5 mm to 10 mm. This can compromise cerebral perfusion, potentially resulting in ischemia, brain herniation, or death. Early surgical intervention, such as decompression, significantly reduces morbidity and mortality, with some studies suggesting that timely intervention can reduce fatality rates to less than 5%.8 Large intracranial air pockets can impair respiratory function, complicating ventilation management during surgery. Careful airway management and minimizing air entry are essential to prevent respiratory complications. CSF leaks, common with skull base fractures, also heighten infection risks, including meningitis and brain abscesses. For instance, in cases involving CSF leaks, the incidence of meningitis can be as high as 20-50% without appropriate surgical repair and antibiotic management.9 In this case, the parietal abscess raised concerns, but antibiotics and skull base repair were effective preventive measures, with close monitoring essential for managing CSF and detecting infections early.
Preoperative management of tension pneumocephalus relies heavily on imaging, with CT scans playing a crucial role in diagnosis. For instance, CT scans are the diagnostic tool of choice in over 90% of pneumocephalus cases, as they are highly effective in detecting intracranial air and guiding surgical intervention. Plain imaging can diagnose pneumocephalus, but CT scan is the diagnostic modality of choice, with an ability to detect as little as 0.5 cm3 of air.4
Studies suggest that early imaging significantly improves outcomes by enabling timely surgical decompression, which can reduce the risk of permanent neurological damage or death. In our case, the CT revealed intracranial air, a midline shift from 5 mm to 10 mm, and mild cerebral edema, confirming the need for surgical intervention. In terms of anesthetic management, the use of agents like Propofol, Cisatracurium, and Fentanyl is common in neurosurgical cases, with research showing that these agents help maintain stable hemodynamics in up to 85% of high-risk neurosurgery patients.10 In the present case, careful endotracheal intubation and ventilation control were essential to avoid further air entry. Continuous monitoring, including arterial line placement for blood pressure and blood gas analysis, ensured stable cerebral perfusion, while unnecessary invasive procedures, such as central venous pressure monitoring, were avoided due to the patient’s stability.
In this case, the intraoperative management involved a modified right frontal craniotomy and repair of the anterior skull base defect to address tension pneumocephalus and craniofacial fractures. Repairing the skull base was crucial to prevent further CSF leaks, a major source of air entry. Postoperatively, a closed lumbar drain was placed for six days to facilitate controlled CSF drainage, reducing air accumulation and ICP. Endocrinological complications, including psychogenic polydipsia, required careful monitoring of fluid intake and sodium levels to avoid further complications. Neurosurgical patients develop some form of fluid or electrolyte imbalance postoperatively. Postoperative fluid or electrolyte imbalances are common in neurosurgical patients, with hyponatremia affecting 16% and hypocalcemia affecting 64% of cases. These disturbances require careful monitoring and prompt intervention.11 In present case, several strategies were employed to prevent complications such as increased ICP, the progression of tension pneumocephalus, and infection. Intraoperative management focused on preventing sudden increases in ICP and ensuring smooth ventilation.
Studies have shown that timely surgical decompression is critical for preventing irreversible brain injury and improving outcomes. The use of a lumbar drain to reduce air accumulation has been well-documented in similar cases, with success in reducing ICP and facilitating recovery. Collaborative management involving multiple specialties can reduce complication rates by 15-30% in neurosurgical patients, as it allows for more comprehensive care.12 However, the interdisciplinary approach in this case, involving both neurosurgical and endocrinological teams, provided a comprehensive strategy that helped manage unexpected complications such as psychogenic polydipsia, a factor not frequently addressed in similar reports.
Timely intervention, guided by thorough imaging and clinical assessment, prevented the progression of potentially fatal complications such as brain herniation or severe neurological deficits. The collaboration between neurosurgery, anesthesia, and endocrinology teams ensured that all aspects of the patient’s condition were addressed, contributing to the favorable outcome.13
Future research should focus on refining diagnostic tools to detect subtle signs of tension pneumocephalus earlier, improving surgical techniques for repairing skull base defects, and optimizing fluid and electrolyte management in complex cases with concurrent endocrinological issues.
The work has been reported to be in line with the SCARE Criteria.14
Effective management of tension pneumocephalus relies on early diagnosis, timely surgical intervention, and comprehensive intraoperative and postoperative care. Prompt imaging and surgical decompression are critical in preventing severe complications, such as increased intracranial pressure and neurological damage. Multidisciplinary collaboration, involving neurosurgery and other specialties as needed, is essential to address complex issues and ensure optimal patient outcomes. Vigilance in the management of post-traumatic cranial injuries, combined with coordinated care, remains the cornerstone of successful tension pneumocephalus treatment.
5. Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available with the authors.
6. Conflict of Interests
All authors declare no conflict of interests.
7. Authors contribution
UAB: Concept and design of the study, searched literature, cquisition of data and analysis, wrote the paper.
SR: Reviewed the manuscript, final approval of the version to be published, monitored the whole study, and agreed to be accountable for all aspects of work.
SA: Interpretation of data
AS: Revision for critically important intellectual content
Authors affiliations:
- Umair Aftab Baig, Department of Anesthesiology, Aga Khan University Hospital, Karachi, Pakistan; Email: umairbaig.ua@gmail.com
- Saima Rashid, Department of Anesthesiology, Aga Khan University Hospital, Karachi, Pakistan; Email: saima.rashid@aku.edu
- Sadique Ali, Department of Anesthesiology, Aga Khan University Hospital, Karachi, Pakistan; Email: sadiquewadho@gmail.com
- Aiman Saeed Shah, Department of Anesthesiology, Aga Khan University Hospital, Karachi, Pakistan; Email: aiman.shah@aku.edu
ABSTRACT
Tension pneumocephalus is a life-threatening condition that presents significant challenges for anesthesiologists, particularly in pediatric and adolescent patients. This case report details the perioperative management of a 17-year-old male who developed tension pneumocephalus following a road traffic accident, leading to multiple skull base fractures. In this case, comprehensive preoperative assessment, intraoperative anesthetic management, and postoperative care strategies employed to optimize the patient's outcome. A thorough preoperative evaluation is important in guiding intraoperative and postoperative decisions to avoid unnecessary Intensive Care Unit (ICU) admission.
Interdisciplinary collaboration between the surgical, anesthesiology, and endocrinology team is necessary to manage patient's condition effectively. The case report discusses diagnostic challenges, surgical interventions, and postoperative monitoring that led to the successful resolution of the patient's condition. This case shows the value of coordinated, patient-centered care in achieving favorable outcomes in complex cases of tension pneumocephalus.
Abbreviations: CT: Computed Tomography, GCS: Glasgow Coma Scale, CSF: Cerebrospinal Fluid, WBC: White Blood Count. CVC: Central Venous Catheter, CVP: Central Venous Pressure, CLABSI: Central Line Associated Blood Stream Infections
Keywords: Craniotomy; Interdisciplinary Approach; Pediatric patient; Road traffic accident; Skull base fracture; Tension pneumocephalus
Citation: Baig UA, Rashid S, Ali S, Shah AS. Perioperative anesthesia management of a pediatric patient with unique ‘Mushroom Head’ tension pneumocephalus: A case report. Anaesth. pain intensive care 2025;29(3):703-707. DOI: 10.35975/apic.v29i3.2774
Received: January 14, 2025; Revised: February 05, 2025; Accepted: March 20, 2025
1. INTRODUCTION
Tension pneumocephalus (TP) is a rare, life-threatening complication often associated with skull base fractures, where air accumulates in the cranial cavity under pressure, compressing brain tissue. It occurs in approximately 0.1% to 0.2% of patients with head trauma and is typically linked to fractures of the anterior cranial fossa.1 The condition poses challenges in pediatric patients, where timely diagnosis and anesthetic management are necessary to prevent neurological damage or death.2
In pediatric cases, where patients may not always present with clear neurological symptoms, prompt identification of tension pneumocephalus becomes even more pivotal. The main diagnostic tool remains the CT scan, which reveals intracranial air and associated midline shifts indicative of increased ICP. The primary mechanism behind tension pneumocephalus is a one-way valve effect, where air enters the intracranial space through fractures in the cranial bones, but cannot escape, leading to rising ICP.3 The primary sources of air entry are fractures of the cranial bones, particularly those involving the paranasal sinuses, mastoid air cells, or the dura mater. This can result in severe complications, including brain herniation, ischemia, and, if left untreated, death.
Children and adolescents with tension pneumocephalus, particularly those following trauma, often present with non-specific symptoms such as severe headaches (44% of cases), nausea, vomiting, and altered mental status. Mental status changes occurred in 44% of tension pneumocephalus cases, with 28% of patients experiencing loss of consciousness at some point during their clinical course.4 As the condition progresses and ICP increases, neurological deficits, such as confusion, ethargy, or motor weakness, may emerge. These overlapping symptoms can complicate diagnosis, especially in pediatric patients who may not communicate symptoms as effectively. A high index of suspicion is therefore critical, especially in patients with skull fractures or cerebrospinal fluid (CSF) leaks. It is mostly found in 20% to 30% of patients with traumatic CSF fistula and can also occur in the patients who have no CSF rhinorrhea.5
The successful management of tension pneumocephalus involves not only surgical intervention but also comprehensive anesthetic care throughout the perioperative period. This case report stresses the role of interdisciplinary collaboration between neurosurgery, anesthesiology, and critical care teams in managing a 17-year-old male patient with tension pneumocephalus following a road traffic accident. The case features the importance of preoperative assessment, intraoperative anesthetic strategies, and postoperative care in preventing complications, minimizing the need for Intensive Care Unit (ICU) admission, and ensuring a favorable outcome.
2. CASE REPORT
A 17-year-old male presented to the emergency department with complaints of severe headache and vomiting for two days. One month prior, the patient had sustained multiple skull base fractures due to a road traffic accident (RTA), which were managed conservatively at the time.
On presentation, the patient was fully awake, alert, and oriented. His clinical observations, detailed in Table 1, indicated stable vital signs, and a positive provocation test for CSF rhinorrhea raised the suspicion of a CSF leak.
| Table 1: Patient’s vital signs and clinical observations | ||
| Parameter | Value | Normal Range |
| Pulse Rate | 86 bpm | 60-100 bpm |
| Blood Pressure | 118/73 mmHg | 90/60-120/80 mmHg |
| Respiratory Rate | 16 breaths/min | 12-16 breaths/min |
| Temperature | 36°C | 36.1°C - 37.2°C |
| Glasgow Coma Scale (GCS) | 15/15 | 15/15 |
| Pupillary Response | Right: 4 mm brisk, Left: 3 mm brisk | Equal and reactive |
A computed tomography (CT) scan of the brain revealed the interval development of tension pneumocephalus, with a significant increase in left-sided midline shift from 5 mm to 10 mm (Figure 2).
Figure 2: CT scan showing interval progression in “Mushroom Head” pneumocephalus
There is also significant tracking of air identified within the subarachnoid space and basal cisterns anteriorly (Figure 1). Mild cerebral edema is re-demonstrated. Previously seen small right frontal subdural and multifocal contusional hemorrhages are not appreciable on the current scan due to the presence of a large amount of air. The effacement of the frontal horn of the right lateral ventricle is re-demonstrated. The grey-white matter differentiation of the rest of the brain is preserved, and no hydrocephalus is noted. Basal cisterns are patent, and posterior fossa structures are grossly unremarkable. There is interval resolution of the intra-sinus hemorrhage and minimal fluid in the bilateral mastoids. Multiple craniofacial fractures are re-demonstrated. The patient’s laboratory parameters before and after surgery are outlined in Table 2. Preoperatively, the elevated white blood cell (WBC) count and neutrophil percentage indicated a potential inflammatory or infectious process.
| Table 2: Laboratory Findings (Preoperative vs. Postoperative) | |||
| Laboratory Test | Preoperative values | Postoperative values | Normal Range |
| Hb (g/dL) | 14.3 | 12.5 | 13.8-17.2 g/dL |
| Hct (%) | 44.5 | 38.3 | 40-54% |
| WBC (x10^9/L) | 14.9 | 18 | 4.0-11.0 x10^9/L |
| Platelet Count (per µL) | - | 150,000 | 150,000-450,000 per µL |
| Total Protein (g/L) | - | 60 | 60-80 g/L |
| Albumin (g/L) | - | 34 | 35-50 g/L |
Figure 1: CT scan showing pneumocephalus with air-fluid level in the right frontal region.
The patient was taken to the operating room for a modified right frontal craniotomy and repair of an anterior skull base defect. General anesthesia was induced without complications, and the surgical team took appropriate precautions based on the patient’s stable hemodynamic condition. Intraoperative monitoring was carefully chosen to meet the needs of the procedure, with arterial cannulation for blood pressure control and blood gas analysis, while central venous access and inotropic support were deemed unnecessary. Blood transfusion was required during the procedure, but no major complications were noted. The surgery proceeded smoothly, and the patient was successfully extubated in the operating room, following commands in the post-anesthesia care unit (PACU) without requiring intensive care unit (ICU) admission. The intraoperative findings confirmed
multiple fractures of the frontal bone, predominantly on the right side, and a large anterior skull base defect.
Table 3 shows intraoperative management. Postoperatively, the patient was managed with intravenous fluids, antibiotics, analgesics, and antiemetics. A lumbar drain was inserted to reduce the risk of worsening pneumocranium and was removed on postoperative day six. The patient's fluctuating sodium levels and polyuria prompted an endocrinological consultation, leading to a diagnosis of psychogenic polydipsia. His sodium levels were closely monitored, and he was discharged in stable condition on postoperative day 16, with specific instructions for follow-up care.
| Table 3: Intraoperative Management | |
| Parameter | Details |
| Anesthetic Agents | Propofol (2 mg/kg), Cisatracurium (0.15 mg/kg), Fentanyl (100 µg) |
| Airway Management | Intubated with size 7.0 endotracheal tube without complications |
| Intraoperative Monitoring | Right radial artery cannulation for blood pressure and arterial blood gas analysis |
| Central Venous Catheter (CVC) | Not placed (patient vitally stable, CVP monitoring not required) |
| Inotropes | Not required |
| Blood Transfusion | 1 unit of packed red blood cells administered |
| Surgical Outcome | Uneventful surgery, patient extubated and obeying commands in PACU |
| ICU Admission | Not required |
| Intraoperative Findings | Multiple fractured fragments of the frontal bone (right side) and a large anterior skull base defect |
3. DISCUSSION
Despite advancements in neurosurgical techniques and anesthetic management, perioperative care in patients with tension pneumocephalus, particularly in pediatric populations, remains a challenge due to the rarity of the condition and the critical nature of intraoperative and postoperative decisions.6 This case report aims to contribute to the limited literature by outlining the successful anesthesia and surgical management of a 17-year-old patient with tension pneumocephalus.
The incidence of pneumocephalus is less than 1% in patients with head trauma, but it could reach 8% when fractures of either the paranasal sinus or the skull base presents.7 Tension pneumocephalus may develop if the intracranial air creates a mass effect on the brain, resulting in a possibly life-threatening neurosurgical emergency.
Tension pneumocephalus can lead to serious complications, primarily increased ICP, as air accumulation compresses brain tissue and causes midline shift, as in this case where the shift progressed from 5 mm to 10 mm. This can compromise cerebral perfusion, potentially resulting in ischemia, brain herniation, or death. Early surgical intervention, such as decompression, significantly reduces morbidity and mortality, with some studies suggesting that timely intervention can reduce fatality rates to less than 5%.8 Large intracranial air pockets can impair respiratory function, complicating ventilation management during surgery. Careful airway management and minimizing air entry are essential to prevent respiratory complications. CSF leaks, common with skull base fractures, also heighten infection risks, including meningitis and brain abscesses. For instance, in cases involving CSF leaks, the incidence of meningitis can be as high as 20-50% without appropriate surgical repair and antibiotic management.9 In this case, the parietal abscess raised concerns, but antibiotics and skull base repair were effective preventive measures, with close monitoring essential for managing CSF and detecting infections early.
Preoperative management of tension pneumocephalus relies heavily on imaging, with CT scans playing a crucial role in diagnosis. For instance, CT scans are the diagnostic tool of choice in over 90% of pneumocephalus cases, as they are highly effective in detecting intracranial air and guiding surgical intervention. Plain imaging can diagnose pneumocephalus, but CT scan is the diagnostic modality of choice, with an ability to detect as little as 0.5 cm3 of air.4
Studies suggest that early imaging significantly improves outcomes by enabling timely surgical decompression, which can reduce the risk of permanent neurological damage or death. In our case, the CT revealed intracranial air, a midline shift from 5 mm to 10 mm, and mild cerebral edema, confirming the need for surgical intervention. In terms of anesthetic management, the use of agents like Propofol, Cisatracurium, and Fentanyl is common in neurosurgical cases, with research showing that these agents help maintain stable hemodynamics in up to 85% of high-risk neurosurgery patients.10 In the present case, careful endotracheal intubation and ventilation control were essential to avoid further air entry. Continuous monitoring, including arterial line placement for blood pressure and blood gas analysis, ensured stable cerebral perfusion, while unnecessary invasive procedures, such as central venous pressure monitoring, were avoided due to the patient’s stability.
In this case, the intraoperative management involved a modified right frontal craniotomy and repair of the anterior skull base defect to address tension pneumocephalus and craniofacial fractures. Repairing the skull base was crucial to prevent further CSF leaks, a major source of air entry. Postoperatively, a closed lumbar drain was placed for six days to facilitate controlled CSF drainage, reducing air accumulation and ICP. Endocrinological complications, including psychogenic polydipsia, required careful monitoring of fluid intake and sodium levels to avoid further complications. Neurosurgical patients develop some form of fluid or electrolyte imbalance postoperatively. Postoperative fluid or electrolyte imbalances are common in neurosurgical patients, with hyponatremia affecting 16% and hypocalcemia affecting 64% of cases. These disturbances require careful monitoring and prompt intervention.11 In present case, several strategies were employed to prevent complications such as increased ICP, the progression of tension pneumocephalus, and infection. Intraoperative management focused on preventing sudden increases in ICP and ensuring smooth ventilation.
Studies have shown that timely surgical decompression is critical for preventing irreversible brain injury and improving outcomes. The use of a lumbar drain to reduce air accumulation has been well-documented in similar cases, with success in reducing ICP and facilitating recovery. Collaborative management involving multiple specialties can reduce complication rates by 15-30% in neurosurgical patients, as it allows for more comprehensive care.12 However, the interdisciplinary approach in this case, involving both neurosurgical and endocrinological teams, provided a comprehensive strategy that helped manage unexpected complications such as psychogenic polydipsia, a factor not frequently addressed in similar reports.
Timely intervention, guided by thorough imaging and clinical assessment, prevented the progression of potentially fatal complications such as brain herniation or severe neurological deficits. The collaboration between neurosurgery, anesthesia, and endocrinology teams ensured that all aspects of the patient’s condition were addressed, contributing to the favorable outcome.13
Future research should focus on refining diagnostic tools to detect subtle signs of tension pneumocephalus earlier, improving surgical techniques for repairing skull base defects, and optimizing fluid and electrolyte management in complex cases with concurrent endocrinological issues.
The work has been reported to be in line with the SCARE Criteria.14
4. CONCLUSION
Effective management of tension pneumocephalus relies on early diagnosis, timely surgical intervention, and comprehensive intraoperative and postoperative care. Prompt imaging and surgical decompression are critical in preventing severe complications, such as increased intracranial pressure and neurological damage. Multidisciplinary collaboration, involving neurosurgery and other specialties as needed, is essential to address complex issues and ensure optimal patient outcomes. Vigilance in the management of post-traumatic cranial injuries, combined with coordinated care, remains the cornerstone of successful tension pneumocephalus treatment.
5. Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available with the authors.
6. Conflict of Interests
All authors declare no conflict of interests.
7. Authors contribution
UAB: Concept and design of the study, searched literature, cquisition of data and analysis, wrote the paper.
SR: Reviewed the manuscript, final approval of the version to be published, monitored the whole study, and agreed to be accountable for all aspects of work.
SA: Interpretation of data
AS: Revision for critically important intellectual content
8. REFERENCES
- Healy J, Grant M, Melnyk S, Boldt B. Tension pneumocephalus – a rare complication of cerebrospinal fluid leak. Radiol Case Rep. 2019;14:365–7. PubMed DOI: 1016/j.radcr.2018.10.030
- Simmons J, Luks AM. Tension pneumocephalus: an uncommon cause of altered mental status. J Emerg Med. 2013;44:340–3. PubMed DOI: 1016/j.jemermed.2012.01.055
- Clement AR, Palaniappan D, Panigrahi RK. Tension pneumocephalus. Anesthesiology. 2017;127:710. PubMed DOI: 1097/ALN.0000000000001703
- Pillai P, Sharma R, MacKenzie L, Reilly EF, Beery PR, Papadimos TJ, et al. Traumatic tension pneumocephalus – two cases and comprehensive review of literature. Int J Crit Illn Inj Sci. 2017;7:58–64. PubMed DOI: 4103/IJCIIS.IJCIIS_8_17
- Kwon J, Rha HK, Park HK, Chough CK, Joo WI, Cho SH, et al. Proper management of posttraumatic tension pneumocephalus. Korean J Neurotrauma. 2017;13:158–61. PubMed DOI: 13004/kjnt.2017.13.2.158
- Heinrich S, Birkholz T, Ihmsen H, Irouschek A, Ackermann A, Schmidt J. Incidence and predictors of difficult laryngoscopy in 11,219 pediatric anesthesia procedures. Paediatr Anaesth. 2012;22:729–36. PubMed DOI: 1111/j.1460-9592.2012.03813.x
- Al-Aieb A, Peralta R, Ellabib M, El-Menyar A, Al-Thani H. Traumatic tension pneumocephalus: two case reports. Int J Surg Case Rep. 2017;31:145–9. PubMed DOI: 1016/j.ijscr.2017.01.038
- Azab MA, Hazem A, Lucke-Wold B. Tension pneumocephalus as a complication of surgical evacuation of chronic subdural hematoma: case report and literature review. Explor Neuroprot Ther. 2023;3:177–85. DOI: 37349/ent.2023.00046
- Steiert C, Kraus LM, Roelz R, Urbach H, Beck J, Meckel S, et al. Surgical repair of skull base CSF leaks after cisternography diagnosis: analysis of validity and surgical outcome and impact on future treatment strategies. Biomed Res Int. 2022;2022:1–13. PubMed DOI: 1155/2022/8740352
- Choi JW, Joo JD, Kim DW, In JH, Kwon SY, Seo K, et al. Comparison of an intraoperative infusion of dexmedetomidine, fentanyl, and remifentanil on perioperative hemodynamics, sedation quality, and postoperative pain control. J Korean Med Sci. 2016;31:1485–95. PubMed DOI: 3346/jkms.2016.31.9.1485
- Săcărescu A, Turliuc MD. Electrolyte imbalance in acute traumatic brain injury: insights from the first 24 h. Clin Pract. 2024;14:1767–78. PubMed DOI: 3390/clinpract14050141
- Marchán-López Á, Lora-Tamayo J, de la Calle C, Jiménez Roldán L, Moreno Gómez LM, Sáez de la Fuente I, et al. Impact of a hospitalist co-management program on medical complications and length of stay in neurosurgical patients. Jt Comm J Qual Patient Saf. 2024;50:318–25. PubMed DOI: 1016/j.jcjq.2024.01.003
- Taberna M, Gil Moncayo F, Jané-Salas E, Antonio M, Arribas L, Vilajosana E, et al. The multidisciplinary team (MDT) approach and quality of care. Front Oncol. 2020;10:85. PubMed DOI: 3389/fonc.2020.00085
- Sohrabi C, Mathew G, Maria N, Kerwan A, Franchi T, Agha RA. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg. 2023;109(5):1136. PubMed DOI: 1097/JS9.0000000000000373