Tasrif Hamdi 1, Elvita R. Daulay 2, Siti Syarifah 3, Raja H. Siregar 4
Authors affiliations:
Background & objective: Thoracic spinal anesthesia (TSA) is less commonly performed compared to other types of spinal anesthesia due to the risk of spinal cord injury, despite the thoracic region having a relatively wider dura-to-cord space. This study aimed to evaluate the distance between the skin, posterior dura mater, and the subarachnoid space at thoracic levels T1, T6, T9, and T12, using magnetic resonance imaging (MRI).
Methodology: A total of 200 patients with medical conditions, subjected to MRI, were evaluated at Adam Malik Hospital, Medan, Indonesia. Investigations were conducted at segments T1, T6, T9 and T12 to identify the distance between skin to the posterior dura mater and subarachnoid space at thoracic levels T1, T6, T9, and T12.
Results: There was no significant relationship of the patients’ age (52.03 ± 15.97 y), weight (58.44 ± 10.46 kg), and height (157.71 ± 7.03 cm) with the measurements of distance of posterior dura mater and spinal cord from the skin. The mean distance from skin to the posterior epidural was greatest at T1 (5.22 ± 1.31 cm), and the mean epidural and subarachnoid space distances were greatest at T6 level (4.21 ± 1.08 cm).
Conclusion: This study identified that the subarachnoid gap is widest at the middle thoracic level, at T6 (6.41 mm) compared to the upper thoracic (T1) level (4.28 mm) and lower thoracic (T9) levels (4.63 mm), at T12 it was 4.60 mm. These anatomical variations have important implications for thoracic spinal anesthesia practice. The findings suggest that targeting the middle thoracic region for spinal injection may be associated with reduced risk of spinal cord injury, offering potential improvement in spinal anesthesia technique.
Abbreviations: DTC: Dura-to-cord, IRB: Institutional Review Board, MRI: Magnetic Resonance Imaging, STROBE: Strengthening the Reporting of Observational Studies in Epidemiology, TSA: Thoracic spinal anesthesia
Keywords: Anatomy; Anesthesia; Magnetic Resonance Imaging; Spinal; Subarachnoid Space
Citation: Hamdi T, Daulay ER, Syarifah S, Siregar RH. The anatomy of subarachnoid space in thoracic spinal anesthesia investigated using magnetic resonance imaging among 200 Indonesian patients. Anaesth. pain intensive care 2025;29(3):514-519. DOI: 10.35975/apic.v29i3.2751
Received: October 01, 2024; Revised: February 18, 2025; Accepted: March 09, 2025
Spinal anesthesia (SA) is an extensively used technique in surgeries at the lower limbs and abdomen, with the application lasting almost 120 years.1 It has several advantages over general anesthesia.2,3 Thoracic spinal anesthesia (TSA) requires administering SA at thoracic vertebral level and has been performed at levels ranging from T10/T11 to T4/T5 intervertebral region. This technique typically uses a long-acting local anaesthetic, such as levobupivacaine, bupivacaine, or ropivacaine, in either hyperbaric or isobaric formulations. It can be administered as a single-shot spinal, continuous TSA, or a combination of both. TSA offers certain advantages over conventional lumbar SA. Using small doses (5 mg) at thoracic puncture site or higher doses (20–40 mg) at a lumbar puncture site, a high thoracic block can be achieved, which is particularly useful for surgical procedures at the upper abdomen or lower thoracic dermatomes.1,2,3
Ahmed et al. discovered that segmental SA at the T5 level for minor breast surgery was both effective and associated with minimal hemodynamic instability, as well as a high level of patient satisfaction. However, there are three primary concerns when administering segmental SA: the potential risk of spinal cord injury, the possibility of the local anesthetic spreading upward and causing a high or complete block, and the risk of hemodynamic or respiratory issues due to the blockade of cardio accelerator fibers or intercostal nerves.7,8,9
Subarachnoid injections are used in patients with cancer pain at thoracic and cervical levels.5 However, spinal anatomical structure affects the spread of subarachnoid anaesthetic solution that moves under the influence of gravity. Neurologists perform myelographic subarachnoid injections at the cervical or thoracic level before introducing magnetic resonance imaging (MRI).6 One crucial component of the neurological damage caused by needle trauma is the distance between dura mater and spinal cord, dura-to-cord (DTC), or subarachnoid space. Since DTC vary depending on the vertebral level, it is crucial to examine the discrepancy in distance based on the level to identify the target level and select a safe strategy. The vertical distance was considerably larger in middle region than at the upper and lower thoracic levels, according to several studies.5,6
A previous case report showed a low risk of spinal cord injury with the segmental SA technique, noting that the spinal cord segments are positioned anteriorly. For this procedure, the sitting position is with the head facing down, which increases the posterior separation of the dura mater and spinal cord, compared to the supine and lateral positions. This helps to reduce the potential risk of spinal cord injury when performing the block at the thoracic level. In addition, we chose the paramedian approach due to the challenging angulation of the thoracic spinous processes, which makes the midline approach to the thoracic epidural space more difficult.10,11
Studies on the anatomy of subarachnoid fissure using MRI provide vast results and continue to expand. Numerous MRI investigations have been carried out to examine subarachnoid space at different thoracic levels and the anatomy of spinal canal but no previous study in this field was conducted in Indonesia. A review of existing literature also revealed a lack of similar studies from neighboring regions or countries, highlighting the scarcity of data on thoracic spinal anatomy in Southeast Asia. Therefore, this study aimed to investigate the anatomy of subarachnoid space to identify the widest distance between skin to the posterior dura mater and the posterior border of spinal cord.12,13
This study received ethical approval from the Ethics Committee of Adam Malik Hospital, Medan. Using a retrospective design, data were collected from hospital records between May and July 2023. This study was determined to be exempted following review by Institutional Review Board (IRB) at Adam Malik Hospital, Medan. IRB waived written informed consent. This protocol adheres to the applicable Strengthening Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study team had full access to all the data and assumed full responsibility for the integrity and accuracy of the analysis.
In this study, measurements were carried out by a final-year radiology resident under the guidance of a board-certified radiology specialist at Adam Malik Hospital, Medan. The resident, with extensive expertise in MRI and spinal imaging, ensured the accuracy and reliability of the data. A 1.5-T Philips MRI scanner was used to assess the subarachnoid space at thoracic levels T1, T6, T9, and T12. Measurements were taken in the supine position, recording distances from the skin to the posterior dura mater and from the dura mater to the spinal cord. The study followed institutional guidelines, with quality control checks performed by the supervising radiologist to ensure precise measurements.14,12
The study included 200 patients, male and female who met the inclusion criteria, which consisted of patients undergoing MRI at Adam Malik Hospital, aged 18 or older, and who provided signed informed consent. This sample size was selected to ensure adequate statistical power, account for anatomical variability, and improve the reliability of the measurements. BMI can affect the distance between the skin and the dura mater, potentially altering the interpretation of anatomical variations. Similarly, variations in patient positioning, such as slight differences in spinal curvature or posture during imaging, may impact the accuracy of measured distances. Additionally, underlying comorbidities like degenerative spinal diseases or previous spinal surgeries could contribute to structural differences that influence the results. Acknowledging and controlling for these confounding factors through stratified analysis or multivariable adjustments would enhance the validity and generalizability of the findings. Exclusion criteria were patients with a history of vertebral surgery, tumors, or fractures at T1, T6, T9, and T12. Measurements were taken from the skin to the posterior dura mater and from the posterior dura mater to the posterior boundary of the subarachnoid space, as shown in Figure 1.15,16
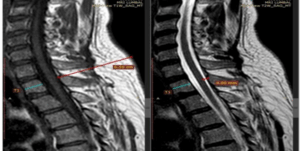
Figure 1: Magnetic Resonance Imaging of the Spinal Column.15
The statistical analysis methods used included descriptive statistics to summarize the data, such as calculating the mean, standard deviation, median, and range for various continuous variables. The normality of the data was assessed using the Kolmogorov-Smirnov test. Based on the normality test results, where a P > 0.05 was considered indicative of normal distribution, parametric or non-parametric statistical methods were selected for further analysis. In addition, univariate analysis was performed using descriptive statistics to determine the frequency distribution of subjects based on their characteristics. Bivariate analysis was also conducted using the chi-square test for categorical variables, and if the chi-square assumptions were not met, Fisher’s exact test was applied. This approach ensured that the selected statistical methods were consistent with the distribution characteristics, allowing for an accurate interpretation of the results.17,12
A total of 74 male and 126 female patients were included in this study as shown in Table 1. Patients demographic characteristics, including age (P < 0.05), weight (P < 0.05), and height (P < 0.05) are given in Table 1.
The widest skin-to-epidural posterior distance was found at T1 (5.22 ± 1.31 cm) compared to T6 (4.21 ± 1.08 cm), T12 (4.16 ± 1.38 cm), and T9 (4.14 ± 1.08 cm) (Table 2) (P > 0.05). The widest distance between the posterior dura mater to the posterior border of subarachnoid space was found at T6 (6.41 ± 1.55 mm) compared to T9 (4.63 ± 1.11 mm), T12 (4.60 ± 1.02 mm), and T1 (4.28 ± 0.84 mm) (Table 3) (P > 0.05).
TSA is an unorthodox technique infrequently used due to the fear of spinal cord injury, cephalad spread of the block, and hemodynamic instability. It can be carried out continuously with a specialized catheter, as a single shot, or in conjunction with an epidural. The sitting position facilitates TSA application because it allows sufficient room for the needle to enter subarachnoid space in thoracic area. Any spinal operation has the potential to cause paresthesia, but needle injections above the lower end of the spinal cord pose the most significant risk of cord injury. The majority of paresthesia (13.6%), manifests in the lumbar area during SA but the clinical importance remains unclear. This procedure has been used for severe patient situations with significant safety. TSA is commonly used for a variety of operations and has numerous benefits over general anesthesia.2,4
The results showed that subarachnoid gap was the widest (6.41 mm) at the mid level (T6 level) compared to the upper (4.28 mm at T1 level) and lower thorax (4.63 mm at T9 level; 4.60 mm at T12). The greater the angle formed, the wider the gap. This study reaffirmed previous results that found the widest subarachnoid gap in middle thorax area (T6) compared to upper and lower thorax.7 The distance between dura mater and spinal cord can be altered by increasing the needle entry angle from skin to subarachnoid space.
A previous study conducted using MRI to examine the anatomy of the thoracic spinal canal in 50 patients, reported a low incidence of neurologic problems during thoracic segmental neuraxial anesthesia. The posterior subarachnoid space was more profound in mid-thoracic than the lumbar and higher levels. This suggests that anesthetic drugs can be administered intrathecally without causing spinal cord contact in thoracic area.12 In this study, the patient was positioned in a supine position; although TSA is generally performed in the lateral decubitus or sitting position. The gap can be widened by positioning the patient in a sitting position as stated in previous studies.13,14 Furthermore, the existence of a gap between dura mater and spinal cord has been explained in previous literature through cadaveric studies. Given the geometry, it was hypothesized that the cord would be found to lie even more anteriorly when the patient is seated or in a lateral posture with an increased back curve. The distance between dura mater and the cord is crucial because it reduces the possibility of a medullary lesion caused by a needle-tip trauma. In thoracic combined spinal epidural anesthesia or cervical and thoracic combined epidural anesthesia, this gap may help prevent lesions from forming in an unintentional dural puncture. The presence of subarachnoid gap can mitigate the risk of injury caused by needle tip injury.19
A retrospective study, conducted on patients who underwent TSA to assess the incidence of neurological and cardiocirculatory complications. The study examined these outcomes across various types of surgeries using different needles (cut and pencil point), with punctures made between T8 and T11 in either the sitting or lateral decubitus position. The study also considered the use of median or paramedian needle insertion and isobaric as well as hyperbaric 0.5% bupivacaine solutions.18
In a study of 104 patients who underwent lumbar puncture with a pencil-point needle (25G Whitacre and 22G Gertie Marx), paresthesia occurred in 14 out of 103 patients (13.6%). All cases of paresthesia were transient. In comparison, the incidence of paresthesia in our study (5.9%) was slightly less than half that observed with lumbar puncture. This difference can be attributed to the presence of the cauda equina in the lumbar region and the larger space between the dura mater and the spinal cord in the thoracic region.18
In a Letter to the Editor, we agreed with Jonnesco's view and concluded that cut-point needles would be safer for chest puncture. Pencil-point needles have a side orifice that starts at 0.8 mm and extends to 1.7 mm, requiring a 2 mm penetration into the subarachnoid space before cerebrospinal fluid (CSF) appears. Upon reviewing the measurements of the pencil-point needle, we found that it indeed requires more than 2 mm to enter the subarachnoid space. In contrast, the cut-point needle (Quincke) does not have this issue, as the needle's opening is already at the point, and CSF appears in the needle hub as soon as the point enters the subarachnoid space.18
In this study involving 1,406 patients, the incidence of paresthesia was the same for both the pencil-point and cut-point needles. Most evaluations in our study, which included Magnetic Resonance Imaging (MRI) of the thoracolumbar spine, showed that the mean distance from the dura mater to the spinal cord was 3.9 mm at T2, 5.8 mm at T5, and 4.1 mm at T10. It is important to note that the needle entry angle at these interspaces ranged from a minimum of 9° to a maximum of 55°, which increases the distance and provides protection to the spinal cord. The study also demonstrated that; despite the pencil-point needle required a maximum of 2 mm penetration into the subarachnoid space and perforating the meningeal layer of the spinal cord, no neurological sequelae occurred, likely due to the protective effect of the pia mater. As for the cut-point needle, which has a terminal orifice, there are no studies on this specific measurement in the literature or on the websites of various manufacturers.18 The key finding of this study was the confirmation of Jonnesco's results from 1909, along with those of several other studies, demonstrating that TSA is a viable procedure with no neurological sequelae. The low incidence of paresthesia supports the conclusion that TSA is safe when using either needle type. This contrasts with a previous study in the lumbar region, which reported neurological damage following spinal or combined spinal-epidural anesthesia using a pencil-point needle.18
When the anesthetist possesses a strong grasp of contemporary anatomy, physiology, and pharmacology, they can provide safe and efficient anesthesia that meets the needs of both the patient and the surgical team.18 Previous studies demonstrated that spinal anatomy undergoes age-related changes, including a reduction in cerebrospinal fluid volume, narrowing of the subarachnoid space, and alterations in vertebral alignment, which may affect needle placement and anesthetic spread.17 In younger individuals, the dura-to-cord distance tends to be larger, offering a greater safety margin for needle insertion, whereas in older adults, degenerative changes; e.g., ligamentum flavum hypertrophy and intervertebral disc narrowing can contribute to a decreased epidural and subarachnoid space.6 A study by Sass et al. using 3D MRI modeling found that aging is associated with a progressive reduction in the ventral subarachnoid space, particularly in the thoracic region, which may increase the risk of unintentional spinal cord contact during anesthesia.16 Conducting a subgroup analysis in this study population could help determine whether these anatomical changes are significant across different age groups and whether adjustments in TSA techniques are necessary for older patients to minimize complications.
The procedure was performed in the head-down sitting position, which increases the posterior separation of the dura mater and spinal cord compared to the supine and lateral positions. This reduces the potential risk of spinal cord injury during the block at the thoracic level. We also opted for the paramedian approach, as the sharp angulation of the thoracic spinous processes makes the midline approach to the thoracic epidural space more challenging.10
Prone positioning is commonly used in spinal procedures that require a posterior approach. However, it is associated with several serious and potentially life-threatening complications, which can lead to permanent disability. These complications include hemodynamic changes causing hypoperfusion, various ophtalmologic issues, central nervous system damage, peripheral nerve compression, compartment syndrome, and pressure ulcers. Additional risks involve airway swelling and peripheral arterial compression. While these complications are uncommon, being aware of them and implementing preventive measures can help minimize morbidity during prone spine surgery.4,5,6
This study has several limitations. The study was conducted at a single institution, so the findings may not be generalizable to broader populations with different anatomical variations. Additionally, all measurements were performed in the supine position, whereas TSA is commonly administered in the sitting or lateral decubitus position, which may influence the observed distances due to posture-related anatomical changes. The study also focused solely on anatomical measurements without direct correlation to clinical outcomes, such as the actual incidence of spinal cord injury or the effectiveness of TSA at diffferent levels. The study included both genders, and no comparison within both is presented. Furthermore, while measurements were conducted by a trained radiology resident under supervision, intra-observer variability remains a potential source of error. Lastly, the study included only Indonesian patients, limiting the applicability of the results to populations with different ethnic and anatomical characteristics.
Multi-center studies involving diverse populations are needed to enhance the generalizability of results. Investigating anatomical variations in different patient positions, such as sitting or lateral decubitus, would provide more clinically relevant insights for TSA practice. Prospective studies correlating imaging findings with clinical outcomes, including the incidence of neurological complications and the efficacy of TSA, would offer valuable practical applications. Additionally, advanced imaging techniques, such as 3D MRI or CT-based reconstructions, could provide more precise assessments of the spinal structures and optimize needle placement strategies. Combining imaging studies with cadaveric dissections or intraoperative observations would further validate anatomical findings and contribute to safer SA techniques.
This study identified that the subarachnoid gap is widest at the middle thoracic level (T6) compared to the upper (T1) and lower thoracic levels (T9 and T12). These anatomical variations have important implications for thoracic spinal anesthesia practice, and suggest that targeting the middle thoracic region for needle injection may reduce the risk of spinal cord injury, offering potential improvements in spinal anesthesia techniques.
8. Data availability
The numerical data generated during this research is available with the authors.
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
TH: Study design, data collection, interpretation of the results, critical revisions of the manuscript.
ERD: Data collection, image analysis and interpretation.
SS, RHS: drafting the manuscript, coordinated the study and ensured adherence to the study protocol.
Authors affiliations:
- Tasrif Hamdi, Department of Anesthesiology and Intensive Care, Adam Malik Hospital, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; Email: hamdi@usu.ac.id; {ORCID:0000-0002-5874-5991}
- Elvita R. Daulay, Department of Radiology, Adam Malik Hospital, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; Email: daulay@usu.ac.id
- Siti Syarifah, Department of Pharmacology, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; Email: syarifah@usu.ac.id; {ORCID:0000-0002-1846-3324}
- Raja H. Siregar, Department of Radiology, Adam Malik Hospital, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; Email: regarskid@gmail.com
ABSTRACT
Background & objective: Thoracic spinal anesthesia (TSA) is less commonly performed compared to other types of spinal anesthesia due to the risk of spinal cord injury, despite the thoracic region having a relatively wider dura-to-cord space. This study aimed to evaluate the distance between the skin, posterior dura mater, and the subarachnoid space at thoracic levels T1, T6, T9, and T12, using magnetic resonance imaging (MRI).
Methodology: A total of 200 patients with medical conditions, subjected to MRI, were evaluated at Adam Malik Hospital, Medan, Indonesia. Investigations were conducted at segments T1, T6, T9 and T12 to identify the distance between skin to the posterior dura mater and subarachnoid space at thoracic levels T1, T6, T9, and T12.
Results: There was no significant relationship of the patients’ age (52.03 ± 15.97 y), weight (58.44 ± 10.46 kg), and height (157.71 ± 7.03 cm) with the measurements of distance of posterior dura mater and spinal cord from the skin. The mean distance from skin to the posterior epidural was greatest at T1 (5.22 ± 1.31 cm), and the mean epidural and subarachnoid space distances were greatest at T6 level (4.21 ± 1.08 cm).
Conclusion: This study identified that the subarachnoid gap is widest at the middle thoracic level, at T6 (6.41 mm) compared to the upper thoracic (T1) level (4.28 mm) and lower thoracic (T9) levels (4.63 mm), at T12 it was 4.60 mm. These anatomical variations have important implications for thoracic spinal anesthesia practice. The findings suggest that targeting the middle thoracic region for spinal injection may be associated with reduced risk of spinal cord injury, offering potential improvement in spinal anesthesia technique.
Abbreviations: DTC: Dura-to-cord, IRB: Institutional Review Board, MRI: Magnetic Resonance Imaging, STROBE: Strengthening the Reporting of Observational Studies in Epidemiology, TSA: Thoracic spinal anesthesia
Keywords: Anatomy; Anesthesia; Magnetic Resonance Imaging; Spinal; Subarachnoid Space
Citation: Hamdi T, Daulay ER, Syarifah S, Siregar RH. The anatomy of subarachnoid space in thoracic spinal anesthesia investigated using magnetic resonance imaging among 200 Indonesian patients. Anaesth. pain intensive care 2025;29(3):514-519. DOI: 10.35975/apic.v29i3.2751
Received: October 01, 2024; Revised: February 18, 2025; Accepted: March 09, 2025
1. INTRODUCTION
Spinal anesthesia (SA) is an extensively used technique in surgeries at the lower limbs and abdomen, with the application lasting almost 120 years.1 It has several advantages over general anesthesia.2,3 Thoracic spinal anesthesia (TSA) requires administering SA at thoracic vertebral level and has been performed at levels ranging from T10/T11 to T4/T5 intervertebral region. This technique typically uses a long-acting local anaesthetic, such as levobupivacaine, bupivacaine, or ropivacaine, in either hyperbaric or isobaric formulations. It can be administered as a single-shot spinal, continuous TSA, or a combination of both. TSA offers certain advantages over conventional lumbar SA. Using small doses (5 mg) at thoracic puncture site or higher doses (20–40 mg) at a lumbar puncture site, a high thoracic block can be achieved, which is particularly useful for surgical procedures at the upper abdomen or lower thoracic dermatomes.1,2,3
Ahmed et al. discovered that segmental SA at the T5 level for minor breast surgery was both effective and associated with minimal hemodynamic instability, as well as a high level of patient satisfaction. However, there are three primary concerns when administering segmental SA: the potential risk of spinal cord injury, the possibility of the local anesthetic spreading upward and causing a high or complete block, and the risk of hemodynamic or respiratory issues due to the blockade of cardio accelerator fibers or intercostal nerves.7,8,9
Subarachnoid injections are used in patients with cancer pain at thoracic and cervical levels.5 However, spinal anatomical structure affects the spread of subarachnoid anaesthetic solution that moves under the influence of gravity. Neurologists perform myelographic subarachnoid injections at the cervical or thoracic level before introducing magnetic resonance imaging (MRI).6 One crucial component of the neurological damage caused by needle trauma is the distance between dura mater and spinal cord, dura-to-cord (DTC), or subarachnoid space. Since DTC vary depending on the vertebral level, it is crucial to examine the discrepancy in distance based on the level to identify the target level and select a safe strategy. The vertical distance was considerably larger in middle region than at the upper and lower thoracic levels, according to several studies.5,6
A previous case report showed a low risk of spinal cord injury with the segmental SA technique, noting that the spinal cord segments are positioned anteriorly. For this procedure, the sitting position is with the head facing down, which increases the posterior separation of the dura mater and spinal cord, compared to the supine and lateral positions. This helps to reduce the potential risk of spinal cord injury when performing the block at the thoracic level. In addition, we chose the paramedian approach due to the challenging angulation of the thoracic spinous processes, which makes the midline approach to the thoracic epidural space more difficult.10,11
Studies on the anatomy of subarachnoid fissure using MRI provide vast results and continue to expand. Numerous MRI investigations have been carried out to examine subarachnoid space at different thoracic levels and the anatomy of spinal canal but no previous study in this field was conducted in Indonesia. A review of existing literature also revealed a lack of similar studies from neighboring regions or countries, highlighting the scarcity of data on thoracic spinal anatomy in Southeast Asia. Therefore, this study aimed to investigate the anatomy of subarachnoid space to identify the widest distance between skin to the posterior dura mater and the posterior border of spinal cord.12,13
2. METHODOLOGY
This study received ethical approval from the Ethics Committee of Adam Malik Hospital, Medan. Using a retrospective design, data were collected from hospital records between May and July 2023. This study was determined to be exempted following review by Institutional Review Board (IRB) at Adam Malik Hospital, Medan. IRB waived written informed consent. This protocol adheres to the applicable Strengthening Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study team had full access to all the data and assumed full responsibility for the integrity and accuracy of the analysis.
In this study, measurements were carried out by a final-year radiology resident under the guidance of a board-certified radiology specialist at Adam Malik Hospital, Medan. The resident, with extensive expertise in MRI and spinal imaging, ensured the accuracy and reliability of the data. A 1.5-T Philips MRI scanner was used to assess the subarachnoid space at thoracic levels T1, T6, T9, and T12. Measurements were taken in the supine position, recording distances from the skin to the posterior dura mater and from the dura mater to the spinal cord. The study followed institutional guidelines, with quality control checks performed by the supervising radiologist to ensure precise measurements.14,12
The study included 200 patients, male and female who met the inclusion criteria, which consisted of patients undergoing MRI at Adam Malik Hospital, aged 18 or older, and who provided signed informed consent. This sample size was selected to ensure adequate statistical power, account for anatomical variability, and improve the reliability of the measurements. BMI can affect the distance between the skin and the dura mater, potentially altering the interpretation of anatomical variations. Similarly, variations in patient positioning, such as slight differences in spinal curvature or posture during imaging, may impact the accuracy of measured distances. Additionally, underlying comorbidities like degenerative spinal diseases or previous spinal surgeries could contribute to structural differences that influence the results. Acknowledging and controlling for these confounding factors through stratified analysis or multivariable adjustments would enhance the validity and generalizability of the findings. Exclusion criteria were patients with a history of vertebral surgery, tumors, or fractures at T1, T6, T9, and T12. Measurements were taken from the skin to the posterior dura mater and from the posterior dura mater to the posterior boundary of the subarachnoid space, as shown in Figure 1.15,16
Figure 1: Magnetic Resonance Imaging of the Spinal Column.15
The statistical analysis methods used included descriptive statistics to summarize the data, such as calculating the mean, standard deviation, median, and range for various continuous variables. The normality of the data was assessed using the Kolmogorov-Smirnov test. Based on the normality test results, where a P > 0.05 was considered indicative of normal distribution, parametric or non-parametric statistical methods were selected for further analysis. In addition, univariate analysis was performed using descriptive statistics to determine the frequency distribution of subjects based on their characteristics. Bivariate analysis was also conducted using the chi-square test for categorical variables, and if the chi-square assumptions were not met, Fisher’s exact test was applied. This approach ensured that the selected statistical methods were consistent with the distribution characteristics, allowing for an accurate interpretation of the results.17,12
3. RESULTS
A total of 74 male and 126 female patients were included in this study as shown in Table 1. Patients demographic characteristics, including age (P < 0.05), weight (P < 0.05), and height (P < 0.05) are given in Table 1.
| Table 1. Baseline Demographic of Study Participants | |||
| Variable | n (%) | Mean ± SD | Median (Min – Max) |
| Gender | |||
| Male | 74 (37.0%) | - | - |
| Female | 126 (63.0%) | - | - |
| Age (y) | 52.03 ± 15.97 | 55.0 (18 – 84) | |
| Weight (kg) | 58.44 ± 10.4 | 58 (37 – 96) | |
| Height (cm) | 157.71 ± 7.03 | 157 (123 – 175) | |
The widest skin-to-epidural posterior distance was found at T1 (5.22 ± 1.31 cm) compared to T6 (4.21 ± 1.08 cm), T12 (4.16 ± 1.38 cm), and T9 (4.14 ± 1.08 cm) (Table 2) (P > 0.05). The widest distance between the posterior dura mater to the posterior border of subarachnoid space was found at T6 (6.41 ± 1.55 mm) compared to T9 (4.63 ± 1.11 mm), T12 (4.60 ± 1.02 mm), and T1 (4.28 ± 0.84 mm) (Table 3) (P > 0.05).
| Table 2. Skin to epidural distance (cm) | ||
| Level | Skin to epidural Distance (cm) | |
| Mean ± SD | Median (Min - Max) | |
| T1 | 5.22 ± 1.31 | 5.21 (1.54 – 8.78) |
| T6 | 4.21 ± 1.08 | 4.26 (1.37 – 7.85) |
| T9 | 4.14 ± 1.08 | 4.20 (1.21 – 8.07) |
| T12 | 4.16 ± 1.38 | 4.06 (0.92 – 9.73) |
| Table 3. Epidural to spinal cord distance (cm) | ||
| Level | Epidural to spinal cord distance (mm) | |
| Mean ± SD | Median (Min - Max) | |
| T1 | 4.28 ± 0.84 | 4.12 (2.66 – 7.40) |
| T6 | 6.41 ± 1.55 | 6.46 (1.05 – 11.30) |
| T9 | 4.63 ± 1.11 | 4.52 (2.01 – 8.84) |
| T12 | 4.60 ± 1.02 | 4.40 (2.03 – 9.38) |
4. DISCUSSION
TSA is an unorthodox technique infrequently used due to the fear of spinal cord injury, cephalad spread of the block, and hemodynamic instability. It can be carried out continuously with a specialized catheter, as a single shot, or in conjunction with an epidural. The sitting position facilitates TSA application because it allows sufficient room for the needle to enter subarachnoid space in thoracic area. Any spinal operation has the potential to cause paresthesia, but needle injections above the lower end of the spinal cord pose the most significant risk of cord injury. The majority of paresthesia (13.6%), manifests in the lumbar area during SA but the clinical importance remains unclear. This procedure has been used for severe patient situations with significant safety. TSA is commonly used for a variety of operations and has numerous benefits over general anesthesia.2,4
The results showed that subarachnoid gap was the widest (6.41 mm) at the mid level (T6 level) compared to the upper (4.28 mm at T1 level) and lower thorax (4.63 mm at T9 level; 4.60 mm at T12). The greater the angle formed, the wider the gap. This study reaffirmed previous results that found the widest subarachnoid gap in middle thorax area (T6) compared to upper and lower thorax.7 The distance between dura mater and spinal cord can be altered by increasing the needle entry angle from skin to subarachnoid space.
A previous study conducted using MRI to examine the anatomy of the thoracic spinal canal in 50 patients, reported a low incidence of neurologic problems during thoracic segmental neuraxial anesthesia. The posterior subarachnoid space was more profound in mid-thoracic than the lumbar and higher levels. This suggests that anesthetic drugs can be administered intrathecally without causing spinal cord contact in thoracic area.12 In this study, the patient was positioned in a supine position; although TSA is generally performed in the lateral decubitus or sitting position. The gap can be widened by positioning the patient in a sitting position as stated in previous studies.13,14 Furthermore, the existence of a gap between dura mater and spinal cord has been explained in previous literature through cadaveric studies. Given the geometry, it was hypothesized that the cord would be found to lie even more anteriorly when the patient is seated or in a lateral posture with an increased back curve. The distance between dura mater and the cord is crucial because it reduces the possibility of a medullary lesion caused by a needle-tip trauma. In thoracic combined spinal epidural anesthesia or cervical and thoracic combined epidural anesthesia, this gap may help prevent lesions from forming in an unintentional dural puncture. The presence of subarachnoid gap can mitigate the risk of injury caused by needle tip injury.19
A retrospective study, conducted on patients who underwent TSA to assess the incidence of neurological and cardiocirculatory complications. The study examined these outcomes across various types of surgeries using different needles (cut and pencil point), with punctures made between T8 and T11 in either the sitting or lateral decubitus position. The study also considered the use of median or paramedian needle insertion and isobaric as well as hyperbaric 0.5% bupivacaine solutions.18
In a study of 104 patients who underwent lumbar puncture with a pencil-point needle (25G Whitacre and 22G Gertie Marx), paresthesia occurred in 14 out of 103 patients (13.6%). All cases of paresthesia were transient. In comparison, the incidence of paresthesia in our study (5.9%) was slightly less than half that observed with lumbar puncture. This difference can be attributed to the presence of the cauda equina in the lumbar region and the larger space between the dura mater and the spinal cord in the thoracic region.18
In a Letter to the Editor, we agreed with Jonnesco's view and concluded that cut-point needles would be safer for chest puncture. Pencil-point needles have a side orifice that starts at 0.8 mm and extends to 1.7 mm, requiring a 2 mm penetration into the subarachnoid space before cerebrospinal fluid (CSF) appears. Upon reviewing the measurements of the pencil-point needle, we found that it indeed requires more than 2 mm to enter the subarachnoid space. In contrast, the cut-point needle (Quincke) does not have this issue, as the needle's opening is already at the point, and CSF appears in the needle hub as soon as the point enters the subarachnoid space.18
In this study involving 1,406 patients, the incidence of paresthesia was the same for both the pencil-point and cut-point needles. Most evaluations in our study, which included Magnetic Resonance Imaging (MRI) of the thoracolumbar spine, showed that the mean distance from the dura mater to the spinal cord was 3.9 mm at T2, 5.8 mm at T5, and 4.1 mm at T10. It is important to note that the needle entry angle at these interspaces ranged from a minimum of 9° to a maximum of 55°, which increases the distance and provides protection to the spinal cord. The study also demonstrated that; despite the pencil-point needle required a maximum of 2 mm penetration into the subarachnoid space and perforating the meningeal layer of the spinal cord, no neurological sequelae occurred, likely due to the protective effect of the pia mater. As for the cut-point needle, which has a terminal orifice, there are no studies on this specific measurement in the literature or on the websites of various manufacturers.18 The key finding of this study was the confirmation of Jonnesco's results from 1909, along with those of several other studies, demonstrating that TSA is a viable procedure with no neurological sequelae. The low incidence of paresthesia supports the conclusion that TSA is safe when using either needle type. This contrasts with a previous study in the lumbar region, which reported neurological damage following spinal or combined spinal-epidural anesthesia using a pencil-point needle.18
When the anesthetist possesses a strong grasp of contemporary anatomy, physiology, and pharmacology, they can provide safe and efficient anesthesia that meets the needs of both the patient and the surgical team.18 Previous studies demonstrated that spinal anatomy undergoes age-related changes, including a reduction in cerebrospinal fluid volume, narrowing of the subarachnoid space, and alterations in vertebral alignment, which may affect needle placement and anesthetic spread.17 In younger individuals, the dura-to-cord distance tends to be larger, offering a greater safety margin for needle insertion, whereas in older adults, degenerative changes; e.g., ligamentum flavum hypertrophy and intervertebral disc narrowing can contribute to a decreased epidural and subarachnoid space.6 A study by Sass et al. using 3D MRI modeling found that aging is associated with a progressive reduction in the ventral subarachnoid space, particularly in the thoracic region, which may increase the risk of unintentional spinal cord contact during anesthesia.16 Conducting a subgroup analysis in this study population could help determine whether these anatomical changes are significant across different age groups and whether adjustments in TSA techniques are necessary for older patients to minimize complications.
The procedure was performed in the head-down sitting position, which increases the posterior separation of the dura mater and spinal cord compared to the supine and lateral positions. This reduces the potential risk of spinal cord injury during the block at the thoracic level. We also opted for the paramedian approach, as the sharp angulation of the thoracic spinous processes makes the midline approach to the thoracic epidural space more challenging.10
Prone positioning is commonly used in spinal procedures that require a posterior approach. However, it is associated with several serious and potentially life-threatening complications, which can lead to permanent disability. These complications include hemodynamic changes causing hypoperfusion, various ophtalmologic issues, central nervous system damage, peripheral nerve compression, compartment syndrome, and pressure ulcers. Additional risks involve airway swelling and peripheral arterial compression. While these complications are uncommon, being aware of them and implementing preventive measures can help minimize morbidity during prone spine surgery.4,5,6
5. LIMITATIONS
This study has several limitations. The study was conducted at a single institution, so the findings may not be generalizable to broader populations with different anatomical variations. Additionally, all measurements were performed in the supine position, whereas TSA is commonly administered in the sitting or lateral decubitus position, which may influence the observed distances due to posture-related anatomical changes. The study also focused solely on anatomical measurements without direct correlation to clinical outcomes, such as the actual incidence of spinal cord injury or the effectiveness of TSA at diffferent levels. The study included both genders, and no comparison within both is presented. Furthermore, while measurements were conducted by a trained radiology resident under supervision, intra-observer variability remains a potential source of error. Lastly, the study included only Indonesian patients, limiting the applicability of the results to populations with different ethnic and anatomical characteristics.
6. FUTURE PROSPECTUS
Multi-center studies involving diverse populations are needed to enhance the generalizability of results. Investigating anatomical variations in different patient positions, such as sitting or lateral decubitus, would provide more clinically relevant insights for TSA practice. Prospective studies correlating imaging findings with clinical outcomes, including the incidence of neurological complications and the efficacy of TSA, would offer valuable practical applications. Additionally, advanced imaging techniques, such as 3D MRI or CT-based reconstructions, could provide more precise assessments of the spinal structures and optimize needle placement strategies. Combining imaging studies with cadaveric dissections or intraoperative observations would further validate anatomical findings and contribute to safer SA techniques.
7. CONCLUSION
This study identified that the subarachnoid gap is widest at the middle thoracic level (T6) compared to the upper (T1) and lower thoracic levels (T9 and T12). These anatomical variations have important implications for thoracic spinal anesthesia practice, and suggest that targeting the middle thoracic region for needle injection may reduce the risk of spinal cord injury, offering potential improvements in spinal anesthesia techniques.
8. Data availability
The numerical data generated during this research is available with the authors.
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
TH: Study design, data collection, interpretation of the results, critical revisions of the manuscript.
ERD: Data collection, image analysis and interpretation.
SS, RHS: drafting the manuscript, coordinated the study and ensured adherence to the study protocol.
11. REFERENCES
- le Roux JJ, Wakabayashi K, Jooma Z. Defining the role of thoracic spinal anaesthesia in the 21st century: a narrative review. Br J Anaesth. 2023;130(1):e56–65. PubMed DOI: 1016/j.bja.2022.03.008
- Ellakany MH. Thoracic spinal anesthesia is safe for patients undergoing abdominal cancer surgery. Anesth Essays Res. 2014;8(2):223–8. PubMed DOI: 4103/0259-1162.134516
- Wang AY, Liu P, Balonov K, Riesenburger R, Kryzanski J. Use of spinal anesthesia in lower thoracic spine surgery: a case series. Oper Neurosurg (Hagerstown). 2022;23(4):298–303. PubMed DOI: 1227/ons.0000000000000325
- DePasse JM, Palumbo MA, Haque M, Eberson CP, Daniels AH. Complications associated with prone positioning in elective spinal surgery. World J Orthop. 2015;6(3):351–9. PubMed DOI: 5312/wjo.v6.i3.351
- Park JW, Bae SK, Huh J. Distance from dura mater to spinal cord at the thoracic vertebral level: an introductory study on local subdural geometry for thoracic epidural block. J Int Med Res. 2016;44(4):950–6. PubMed DOI: 1177/0300060516652751
- Garg H, Kumar S, Hemachandran N, Goel P, Kandasamy D, Bajpai M, et al. Dura-to-spinal cord distance at different vertebral levels in Indian children: a retrospective computerized tomography scan-based study. Anesth Essays Res. 2022;16(1):138–42. PubMed DOI: 4103/aer.aer_26_22
- Ghozali I, Danayati N. Segmental thoracic spinal anesthesia for open reduction with internal fixation surgery in dextra humerus fracture patients. Med Prof J Lampung. 2023;13:1029. Available from: https://www.journalofmedula.com/index.php/medula/article/view/830
- Cramer GD. General characteristics of the spine. In: Cramer GD, Darby SA, editors. Clinical anatomy of the spine, spinal cord, and ANS. 3rd ed. St. Louis: Elsevier; 2014. p. 15–64.
- Alfaras-Melainis K, Fernando RJ, Boisen ML, Hoffman PJ, Rosenkrans DJ, Teeter E, et al. The year in thoracic anesthesia: selected highlights from 2022. J Cardiothorac Vasc Anesth. 2024;38(1):29–56. PubMed DOI: 1053/j.jvca.2023.09.006
- Atmawan DB, Kurniawan HA. Thoracic spinal anaesthesia for modified radical mastectomy. J Anesth Clin Res. 2022;3(1):1–4. DOI: 21776/ub.jap.2022.003.01.01
- Homma T, Doki Y, Yamamoto Y, Ojima T, Shimada Y, Yoshimura N. Risk factors of neuropathic pain after thoracic surgery. J Thorac Dis. 2018;10(5):2898–907. PubMed DOI: 21037/jtd.2018.05.25
- Imbelloni LE, Cardoso BB, Torres CC, de Morais Filho GB, de Lemos Neto SV, Pinho AC. The anatomy of the thoracic spinal canal investigated with magnetic resonance imaging in children aged 0 to 13 years old. J Cancer Prev Curr Res. 2023;14(1):15–22. DOI: 15406/jcpcr.2023.14.00512
- Imbelloni LE. What is the best needle for spinal thoracic anesthesia: pencil point needle or cut point needle? Acta Sci Med Sci. 2020;4(7):33–4. Available from: https://jap.ub.ac.id/index.php/jap/article/download/86/143
- Gala FB, Aswani Y. Imaging in spinal posterior epidural space lesions: a pictorial essay. Indian J Radiol Imaging. 2016;26(3):381–9. PubMed DOI: 4103/0971-3026.190406
- Patel J, Ponnusamy K, Patel A. Thoracic spinal anaesthesia in upper abdominal surgeries. J Clin Diagn Res. 2023;10(85):85–8. DOI: 18231/j.ijca.2023.015
- Sass LR, Khani M, Natividad GC, Tubbs RS, Baledent O, Martin BA. A 3D subject-specific model of the spinal subarachnoid space with anatomically realistic ventral and dorsal spinal cord nerve rootlets. Fluids Barriers CNS. 2017;14(1):1–16. PubMed DOI: 1186/s12987-017-0085-y
- Mehta N, Dar MR, Sharma S, Mehta KS. Thoracic combined spinal epidural anesthesia for laparoscopic cholecystectomy: a feasibility study. J Anaesthesiol Clin Pharmacol. 2016;32(2):224-8. PubMed DOI: 4103/0970-9185.173384
- Imbelloni LE, Fornasari M, Borges G, Filho DM. Thoracic spinal anesthesia is safe and without neurological sequelae: study with 1,406 patients. Int J Anesthetic Anesthesiol. 2022;9(2):148. DOI: 23937/2377-4630/1410148