Pushpavathi Ture, MD1, Madhuri Kurdi, MD2, Sheetal Hiregoudar, DA3, Ganapati Hegde4
1Assistant professor; 2Professor; 3Senior resident; 4Postgraduate Trainee
Department of Anaesthesiology, Karnataka Institute of Medical Sciences, Hubli, Karnataka 580022, (India)
Correspondence: Dr Pushpavathi Ture, Assistant professor, Department of Anesthesiology, Karnataka Institute of Medical Sciences, P B Road, Vidyanagar, Hubli, Karnataka 580022, (India); Phone: 9448251597; E-mail: pushpadrture@rediffmail.com
ABSTRACT
Left atrial myxomas are rare cardiac tumours. When diagnosed, these need to be surgically excised as early as possible as these are known to cause dangerous complications, e.g. intracardiac obstruction and embolism. But when presented as an incidental finding on routine echocardiography in a patient presenting with epigastric hernia it creates a clinical dilemma as to which surgery should be performed first. We present one such case of left atrial myxoma in a 58 year old male patient, who underwent hernioplasty under general anesthesia with thoracic epidural analgesia.
Key words; Atrial myxoma, Asymptomatic, Epidural; Surgical Procedures, Operative; Herniorrhaphy; Intracardiac myxoma
Citation: Ture P, Kurdi M, Hiregoudar S, Hegde G. Anesthetic management of a patient with asymptomatic atrial myxoma for hernia repair. Anaesth Pain & Intensive Care 2016;20(2):246-248
Received: 7 May 2016; Reviewed: 29 May 2016; Corrected: 3 June 2016; Accepted: 6 June 2016
INTRODUCTION
Left atrial myxomas are rare cardiac tumors. When diagnosed, surgical excision should be done as early as possible, as these are known to cause dangerous complications like intra cardiac obstruction and embolism.1 However, these may present as an asymptomatic incidental finding in a patient scheduled for elective non-cardiac surgery. Cardiac surgery is always dreadful and is a very costly affair. It may be impossible to convince an asymptomatic patient to undergo cardiac surgery to get his hernia repaired. This situation poses a clinical dilemma to the anesthesiologist; whether to proceed with hernia surgery or to refuse it. We present here one such case of left atrial myxoma in a 58 year old male patient whom we had to anesthetize for a hernia repair. Most reported cases of myxomas are of patients who were posted for myxoma resection. The anesthetic management of such cases for non-cardiac surgery is seldom reported.
CASE REPORT
A 58 year old male patient, a manual laborer by occupation, presented to our hospital with epigastric hernia for repair. On examination, he was well built male, weighing 73 kg with a height of 173 cm. The pulse rate was 76/min, regular in rhythm. Blood pressure was 132/86 mmHg in right upper limb in supine position. On auscultation, first and second heart sounds were heard and an additional ‘tumor plop’ was heard. A ‘tumor plop’ is a sound that typically occurs during early diastole and is believed to be caused by motion of the tumor striking the wall of the endocardium. Thus, an echocardiogram was advised which revealed a large pedunculated mobile left atrial mass measuring 16x58mm arising from the interatrial septum and prolapsing into the left ventricle during diastole with a mean gradient across the mitral valve of 6 mm Hg. Left ventricular systolic function was normal (Figures 1 & 2). An interatrial septal defect measuring 13 mm was detected on transesophageal echocardiography. A provisional diagnosis of left atrial myxoma was made. The left atrial myxoma was thus an incidental finding and the patient did not have any symptoms or signs related to it. All laboratory investigations were within normal limits.
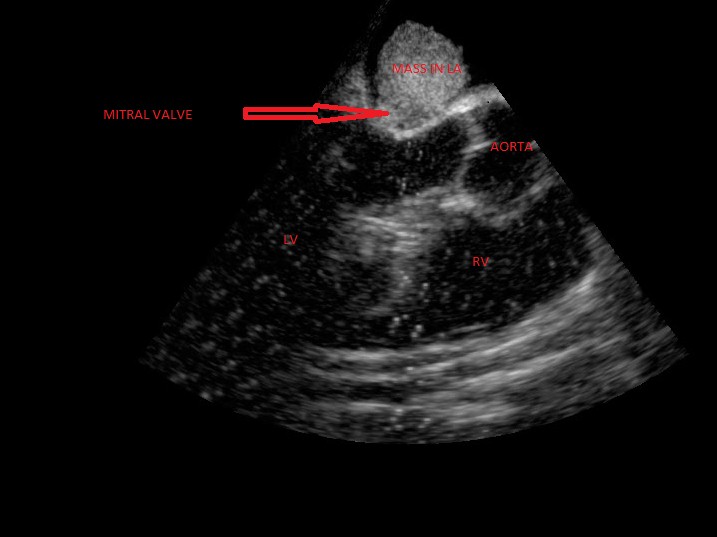
Figure 1: Showing atrial mass above mitral valve
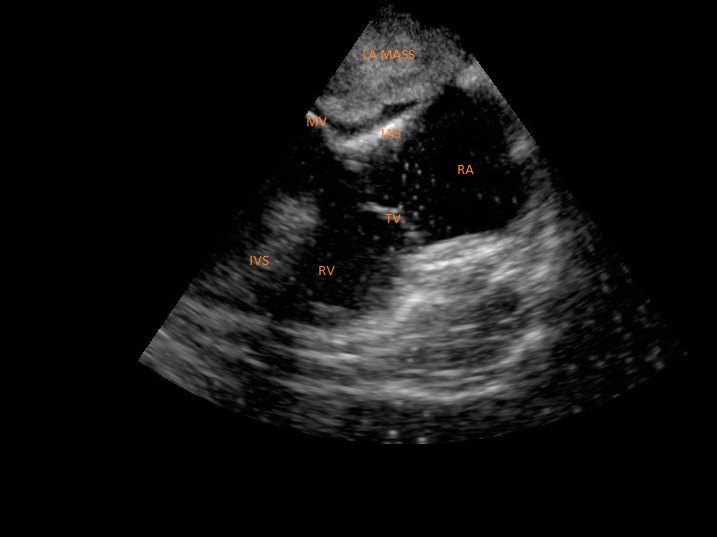
Figure 2: Showing atrial mass above mitral valve
On shifting the patient to the operating room, all routine monitors i.e. 5-lead electrocardiogram, pulse oximeter, noninvasive blood pressure and end tidal CO2 were connected and basal values were noted. Invasive monitoring is not available at our hospital. Antiarrhythmic medications e.g. lignocaine and amiodarone, and the defibrillator were kept ready. In the sitting position, 18G epidural catheter was passed at T8-T9 intervertebral space with loss of resistance technique. A test dose of 3 ml of lignocaine with adrenaline was given and it confirmed epidural placement. In the supine position, patient was premedicated with glycopyrrolate 0.2 mg, fentanyl 150 µg and midazolam 2mg intravenously. After preoxygenation with 100% oxygen for 5 minutes, induction was done with propofol 150 mg intravenously. Patient was intubated orally with succinylcholine 100 mg using 8.5 mm cuffed endotracheal tube.
Patient was put on controlled ventilation with vecuronium 6 mg IV to maintain end tidal CO2 between 30-35 mmHg. Anesthesia was maintained with oxygen, nitrous oxide and sevoflurane. Epidural was activated with 0.5% bupivacaine 6 ml as a bolus. Intraoperatively, hemodynamics were maintained. Heart rate was 65 to 76/min. Blood pressure maintained between 110 to 126 systolic and 76 to 88 mmHg diastolic. The surgery was completed in 90 min with a blood loss of about 200 ml. The patient was reversed with neostigmine 3.5 mg and glycopyrrolate
0.7 mg and extubated.
He was shifted to the surgical intensive care unit for monitoring. Post-operative analgesia was obtained with 8 ml of 0.125% bupivacaine with 150 µg of buprenorphine 3 times a day for 3 days. He was discharged on the 5th postoperative day with an advice to follow up in cardiology outdoor clinic.
DISCUSSION
Primary cardiac tumors are very uncommon, with an annual incidence of 0.5% per million.[2] Although any age can be affected, it predominates in the age group of 30-60 years of age with more than 75% of the affected being women. The occurrence of myxomas in left and right atrium are 75% and 20% respectively.3 Nevertheless our patient was a male and the myxoma was in the left atrium.
Myxomas may manifest with a variety of symptoms, though the classic triad includes embolism, intracardiac obstruction and constitutional symptoms (Goodwin’s triad). Approximately 80% of individuals present with one component of the triad, yet upto 10% may be asymptomatic. Atrial myxomas being discovered on incidental echocardiography examination is a rare phenomenon as seen in our case.3
The presence of a cardiac tumour requires a careful preoperative assessment of cardiac morphology and function. Transthoracic and transesophageal echocardiography, CT and MRI are all used for diagnosis and assessment of treatment options. For the anesthesiologist planning for the appropriate technique these imaging results are essential.4
Most reported cases of myxomas are of patients who were posted for myxoma resection. The anesthetic management of such cases for non-cardiac surgery is seldom reported. We preferred general anesthesia with titrated doses for our patient to prevent sudden hemodynamic changes with epidural catheter in situ for perioperative analgesia. Maddali et al, described the case of a 54-year-old man with no symptoms of a cardiac disease who, in the preoperative assessment for an eye surgery was diagnosed to have a left atrial myxoma coupled with coronary artery disease.5 Nakata et al, presented a case report about a pregnant patient with atrial myxoma in which normal healthy twins were delivered by cesarean section performed under epidural anesthesia at 32 weeks of gestation.6 Zeest K et al, reported acute respiratory distress after knee arthroplasty due to an undiagnosed atrial myxoma.7
To conclude, patients with atrial myxoma may present with embolic events or may be asymptomatic. Embolic events are, however, more common with papillary myxomas Although a myxoma should be excised once detected, this case report depicts the challenging situations faced when anesthetizing these patients for elective non-cardiac surgeries. For optimal outcome, these patients should be managed by a multidisciplinary team including surgeons, cardiologists and anesthesiologists.
Conflict of interest: Nil declared by the authors
Authors’ Contribution: PT & MK - Concept, conduction of the study work and manuscript editing; SH & GH - Conduction of the study work
REFERENCES
1Assistant professor; 2Professor; 3Senior resident; 4Postgraduate Trainee
Department of Anaesthesiology, Karnataka Institute of Medical Sciences, Hubli, Karnataka 580022, (India)
Correspondence: Dr Pushpavathi Ture, Assistant professor, Department of Anesthesiology, Karnataka Institute of Medical Sciences, P B Road, Vidyanagar, Hubli, Karnataka 580022, (India); Phone: 9448251597; E-mail: pushpadrture@rediffmail.com
ABSTRACT
Left atrial myxomas are rare cardiac tumours. When diagnosed, these need to be surgically excised as early as possible as these are known to cause dangerous complications, e.g. intracardiac obstruction and embolism. But when presented as an incidental finding on routine echocardiography in a patient presenting with epigastric hernia it creates a clinical dilemma as to which surgery should be performed first. We present one such case of left atrial myxoma in a 58 year old male patient, who underwent hernioplasty under general anesthesia with thoracic epidural analgesia.
Key words; Atrial myxoma, Asymptomatic, Epidural; Surgical Procedures, Operative; Herniorrhaphy; Intracardiac myxoma
Citation: Ture P, Kurdi M, Hiregoudar S, Hegde G. Anesthetic management of a patient with asymptomatic atrial myxoma for hernia repair. Anaesth Pain & Intensive Care 2016;20(2):246-248
Received: 7 May 2016; Reviewed: 29 May 2016; Corrected: 3 June 2016; Accepted: 6 June 2016
INTRODUCTION
Left atrial myxomas are rare cardiac tumors. When diagnosed, surgical excision should be done as early as possible, as these are known to cause dangerous complications like intra cardiac obstruction and embolism.1 However, these may present as an asymptomatic incidental finding in a patient scheduled for elective non-cardiac surgery. Cardiac surgery is always dreadful and is a very costly affair. It may be impossible to convince an asymptomatic patient to undergo cardiac surgery to get his hernia repaired. This situation poses a clinical dilemma to the anesthesiologist; whether to proceed with hernia surgery or to refuse it. We present here one such case of left atrial myxoma in a 58 year old male patient whom we had to anesthetize for a hernia repair. Most reported cases of myxomas are of patients who were posted for myxoma resection. The anesthetic management of such cases for non-cardiac surgery is seldom reported.
CASE REPORT
A 58 year old male patient, a manual laborer by occupation, presented to our hospital with epigastric hernia for repair. On examination, he was well built male, weighing 73 kg with a height of 173 cm. The pulse rate was 76/min, regular in rhythm. Blood pressure was 132/86 mmHg in right upper limb in supine position. On auscultation, first and second heart sounds were heard and an additional ‘tumor plop’ was heard. A ‘tumor plop’ is a sound that typically occurs during early diastole and is believed to be caused by motion of the tumor striking the wall of the endocardium. Thus, an echocardiogram was advised which revealed a large pedunculated mobile left atrial mass measuring 16x58mm arising from the interatrial septum and prolapsing into the left ventricle during diastole with a mean gradient across the mitral valve of 6 mm Hg. Left ventricular systolic function was normal (Figures 1 & 2). An interatrial septal defect measuring 13 mm was detected on transesophageal echocardiography. A provisional diagnosis of left atrial myxoma was made. The left atrial myxoma was thus an incidental finding and the patient did not have any symptoms or signs related to it. All laboratory investigations were within normal limits.
Figure 1: Showing atrial mass above mitral valve
Figure 2: Showing atrial mass above mitral valve
On shifting the patient to the operating room, all routine monitors i.e. 5-lead electrocardiogram, pulse oximeter, noninvasive blood pressure and end tidal CO2 were connected and basal values were noted. Invasive monitoring is not available at our hospital. Antiarrhythmic medications e.g. lignocaine and amiodarone, and the defibrillator were kept ready. In the sitting position, 18G epidural catheter was passed at T8-T9 intervertebral space with loss of resistance technique. A test dose of 3 ml of lignocaine with adrenaline was given and it confirmed epidural placement. In the supine position, patient was premedicated with glycopyrrolate 0.2 mg, fentanyl 150 µg and midazolam 2mg intravenously. After preoxygenation with 100% oxygen for 5 minutes, induction was done with propofol 150 mg intravenously. Patient was intubated orally with succinylcholine 100 mg using 8.5 mm cuffed endotracheal tube.
Patient was put on controlled ventilation with vecuronium 6 mg IV to maintain end tidal CO2 between 30-35 mmHg. Anesthesia was maintained with oxygen, nitrous oxide and sevoflurane. Epidural was activated with 0.5% bupivacaine 6 ml as a bolus. Intraoperatively, hemodynamics were maintained. Heart rate was 65 to 76/min. Blood pressure maintained between 110 to 126 systolic and 76 to 88 mmHg diastolic. The surgery was completed in 90 min with a blood loss of about 200 ml. The patient was reversed with neostigmine 3.5 mg and glycopyrrolate
0.7 mg and extubated.
He was shifted to the surgical intensive care unit for monitoring. Post-operative analgesia was obtained with 8 ml of 0.125% bupivacaine with 150 µg of buprenorphine 3 times a day for 3 days. He was discharged on the 5th postoperative day with an advice to follow up in cardiology outdoor clinic.
DISCUSSION
Primary cardiac tumors are very uncommon, with an annual incidence of 0.5% per million.[2] Although any age can be affected, it predominates in the age group of 30-60 years of age with more than 75% of the affected being women. The occurrence of myxomas in left and right atrium are 75% and 20% respectively.3 Nevertheless our patient was a male and the myxoma was in the left atrium.
Myxomas may manifest with a variety of symptoms, though the classic triad includes embolism, intracardiac obstruction and constitutional symptoms (Goodwin’s triad). Approximately 80% of individuals present with one component of the triad, yet upto 10% may be asymptomatic. Atrial myxomas being discovered on incidental echocardiography examination is a rare phenomenon as seen in our case.3
The presence of a cardiac tumour requires a careful preoperative assessment of cardiac morphology and function. Transthoracic and transesophageal echocardiography, CT and MRI are all used for diagnosis and assessment of treatment options. For the anesthesiologist planning for the appropriate technique these imaging results are essential.4
Most reported cases of myxomas are of patients who were posted for myxoma resection. The anesthetic management of such cases for non-cardiac surgery is seldom reported. We preferred general anesthesia with titrated doses for our patient to prevent sudden hemodynamic changes with epidural catheter in situ for perioperative analgesia. Maddali et al, described the case of a 54-year-old man with no symptoms of a cardiac disease who, in the preoperative assessment for an eye surgery was diagnosed to have a left atrial myxoma coupled with coronary artery disease.5 Nakata et al, presented a case report about a pregnant patient with atrial myxoma in which normal healthy twins were delivered by cesarean section performed under epidural anesthesia at 32 weeks of gestation.6 Zeest K et al, reported acute respiratory distress after knee arthroplasty due to an undiagnosed atrial myxoma.7
To conclude, patients with atrial myxoma may present with embolic events or may be asymptomatic. Embolic events are, however, more common with papillary myxomas Although a myxoma should be excised once detected, this case report depicts the challenging situations faced when anesthetizing these patients for elective non-cardiac surgeries. For optimal outcome, these patients should be managed by a multidisciplinary team including surgeons, cardiologists and anesthesiologists.
Conflict of interest: Nil declared by the authors
Authors’ Contribution: PT & MK - Concept, conduction of the study work and manuscript editing; SH & GH - Conduction of the study work
REFERENCES
- Arumugam CG, Raju SV, Varma S, Bhaskaran K. Anaesthetic management of a pregnant patient with left atrial myxoma and myxoma excision of lower segment caesarean. Apollo Med. 2008;5(1):71–73.
- Yemul-Golhar S, Shinde S, Kelkar K. Anaesthetic management of a rare variety of cardiac myxoma for emergency decompression laminectomy. South Afr J Anaesth Analg 2013;19(1):71-72.[Free full text]
- Nath M P, Singh B, Chakrabarty A. Left atrial myxoma presenting as stroke-Case report and review of literature. The Indian Anaesthetists’ Forum 2011;1:1-6.
- Mittnacht A, Reich DL, Rhee AJ, Kaplan JA. Cardiac diseases, In: Fleisher LA. Anaesthesia and uncommon diseases, 6th edition, Philadelphia: Elsevier; 2012, 44-45.
- Maddali MM, Abduraz AM, Panduranga P, Kurian E. Left atrial myxoma with coronary artery disease: An unexpected preoperative finding--case report. Middle East J Anaesthesiol 2011;21(3):413-17 [PubMed]
- Nakata S, Nakano S, Mitsuda N, Itou N, Takahashi Y, Matsuda H. Recurrent left atrial myxoma in a patient with a twin fetus pregnancy. Jpn circ J 1996;60(2):130-132. [PubMed] [Free full text]
- Khan Z, Yang B, Mallidi H, Starre PVD. Acute respiratory distress after knee arthroplasty due to undiagnosed atrial myxoma. Open journal of anesthesiology 2012;2:90-92. doi: 10.4236/ojanes.2012.23021.[Free full text]