Nobuyasu Komasawa, MD, PhD
Author affiliation:
Nobuyasu Komasawa, MD, PhD, Community Medicine Education Promotion Office, Kagawa Medical University, 1750-1 Ikenobe, Miki-cho, Kita-gun, Kagawa, 761-0793, Japan.
Correspondence: Nobuyasu Komasawa, E-mail: komasawa.nobuyasu@kagawa-u.ac.jp; Phone: +81-87-891-2442; Fax: +81-87-891-2442.
Airway management evidence has primarily been gathered within the operating room, particularly during the induction of anesthesia. The introduction of newly developed supraglottic devices and videolaryngoscopes have significantly impacted the guidelines for managing difficult airways, prompting the need for new evaluation criteria. Moreover, airway complications such as accidental extubation may occur during surgery, while aspiration or respiratory suppression can manifest during the recovery period following extubation. In this review, I will explore the potential future standards for airway management and potential indications for its application. Additionally, I will underscore the significance of emergency airway management during both the surgical procedure and the recovery phase. It is imperative that we not only accumulate knowledge related to managing difficult airways but also focus on emergency airway management in the future. This calls for interprofessional airway management training for all members of the perioperative team.
Key words: Airway Management; Videolaryngoscope; Supraglottic Device; Future Direction
Abbreviations: DAM - Difficult Airway Management; DAS - Difficult Airway Society; OR - operating room; SGD - Supraglottic Device; VLS – videolaryngoscope
Citation: Komasawa N. Advancing airway management for enhanced patient outcomes: a narrative review. Anaesth. pain intensive care 2024;28(1):171−176; DOI: 10.35975/apic.v28i1.2391
Received: December 12, 2023; Reviewed: December 16, 2023; Accepted: December 16, 2023
Airway management is an art, and the anesthesiologists are considered masters of this art. In fact, some senior anesthesiologists use to say that “Anesthesia is nothing but airway management” (Professor M. Salim, Pakistan). It is the primary skill learnt by the trainees in anesthesiology, and they will always be called throughout their future careers, whenever colleagues from other specialties will face difficulty with airway. However, airway management is not specific to the anesthesiologists, and emergency medicine specialists and intensive care specialists must also be proficient in this skill.
All anesthetic drugs, including sedatives, analgesics, and muscle relaxants, have an impact on airway maintenance to some extent.1,2 Therefore, ensuring the safe management of a patient's airway is the primary responsibility of all anesthesiologists. Worldwide, various airway management guidelines have been established to enhance the safety of patients undergoing general anesthesia. The bulk of evidence related to airway management has been accumulated primarily in the operating room (OR), particularly during the induction of anesthesia.3,4
The advent of newly developed videolaryngoscopes (VLS) and supraglottic devices, has brought about significant changes and opened up new horizons in difficult airway management guidelines. In this review, I will initially address the necessity of tracheal tube passage in the era of VLS and discuss the ventilation scale for supraglottic devices, as well as specific modifications for special situations. Subsequently, I will underscore the expansion of evidence-based airway management to encompass intraoperative and perioperative recovery periods
2. VLS in airway management
Sufficient laryngoscopy does not ensure successful tracheal intubation
The Difficult Airway Management (DAM) Algorithms / Guidelines from the American Society of Anesthesiologists (ASA) delineate five distinct challenging airway scenarios. These include:
1. Challenging mask ventilation;
2. Challenging laryngoscopy;
3. Challenging tracheal intubation;
4. Challenging placement of supraglottic devices (SGD); and
5. Challenging invasive airway management.5
The ASA-DAM recommends anesthesiologists to prepare for airway management based on these guidelines. The most commonly utilized system for anticipating difficult airways is the Mallampati classification, which proves valuable in predicting challenges with mask ventilation and intubation.6 Recent advancements have introduced various types of VLS capable of indirect laryngoscopy.7 These devices simplify the laryngoscopy procedure significantly, and certain guidelines propose them as the preferred choice in specific scenarios.8 However, in some cases, while the glottis may be clearly visible, advancing the tube into the trachea can pose challenges due to factors such as a mismatch between the trachea and tube alignment, anatomical issues like subglottic narrowing, or laryngeal deviation.
Given that the ASA-DAM guidelines differentiate between challenging laryngoscopy and challenging intubation, it is essential to evaluate each on a distinct scale. Although the Cormack-Lehane system is commonly employed for assessing laryngoscopy, there is no equivalent system for grading challenging intubations, i.e., the passage of the tracheal tube through the glottis. A previously proposed alternative evaluation system is the "tracheal tube passage through glottis (TTPG) grade," consisting of four distinct grades: "no resistance," "minor resistance," "major resistance," and "impossible passage" (Box 1).9 Implementing such a novel system would facilitate the evaluation of challenging intubations and allow for correlations with predictive factors for difficult airway management. Furthermore, such tube passage grading can link to difficult airway management to subglottic regions in which clear evidence has not been validated sufficiently yet.
3. Classification of SGDs for emergency airway management
In addition to VLS, a range of new SGDs with varying features have been developed. The guidelines from the Difficult Airway Society (DAS) and the ASA recommend the early use of SGDs for airway rescue in cases where ventilation is insufficient or impossible, aiming to prevent hypoxia-induced cardiac arrest.10 For airway management during resuscitation, both the American Heart Association (AHA) and the European Resuscitation Council (ERC) Cardiopulmonary Resuscitation guidelines recommend SGDs that can be inserted without interrupting chest compressions.11,12 Consequently, SGDs play a critical role in emergent airway management not only in the OR but also in the general wards and prehospital resuscitations.
Various types of SGDs are now available, including the traditional laryngeal mask, anatomically-shaped SGDs like the LMA-ProSeal, cuffless soft gel SGDs such as the i-gel, and esophagus-blocking SGDs like the laryngeal tube and Combitube. These airway management devices are collectively referred to as 'SGDs' because they do not require tracheal intubation and provide a seal within the pharyngeal anatomy.
Several randomized clinical and simulation studies have demonstrated that the rigid curved tube structure of SGDs facilitates easy placement, with added stomach tube passage to prevent aspiration.13 Although these devices have distinct functionalities, the difficulty of SGD insertion can be reduced in various ways, warranting a shift in evaluation focus from 'insertion' to 'ventilation.' To enhance effective emergency airway management with SGDs, there is a compelling need to gather and analyze data, classifying which SGDs are suitable for different scenarios.
While the ASA-DAM defines five patterns of difficult airway management as previously described,13 it is important to note that challenging mask ventilation and challenging tracheal intubation are classified separately.14,15 However, there are currently no equivalent systems for assessing the effectiveness of ventilation with SGDs. Since the primary goal of SGD insertion in ventilation rescue is to secure the airway and provide oxygen to the lungs, the evaluation scale for successful airway rescue with SGDs should differ from that used in general anesthesia, where high-sealing pressure is essential during mechanical ventilation.
The author previously suggested a new evaluation scale, the “ventilation efficacy with SGD (V-SGD) scale,” comprising the following three grades: “insufficient ventilation with SGD and decreased SpO2,” “insufficient ventilation with SGD but with maintained SpO2 (insufficient sealing pressure)” and “sufficient ventilation and maintained SpO2 (sufficient sealing pressure)” (Box 2).16 The V-SGD evaluation scale, which allows for the evaluation of SGD, may be useful not only for evaluating the ventilation status with conventional SGD during general anesthesia but also for decision-making during rescue application of various SGDs in difficult or ‘can’t ventilate, can’t intubate’ emergency situations.
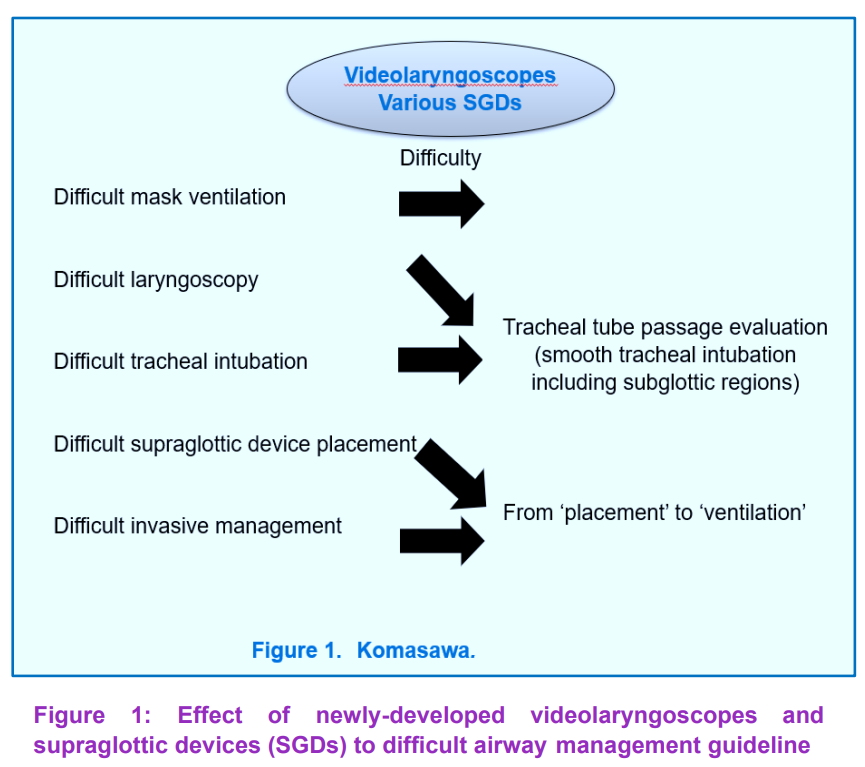
In summary, newly developed VLSs or SGDs significantly affected the difficult airway management (Figure 1). In other words, VLS have reduced the frequency of difficult laryngoscopy and clarified the needs of tracheal tube passages, while SGD variations have alleviated insertion difficulty and offered an at-hand means of rescue ventilation.
4. Application and Expansion for DAS Guidelines in Special Situations
Various airway management guidelines have been published worldwide. However, most of the guidelines were established by evidence in adult cases and not in pediatric ones. One major reason of this is that various clinical studies and data accumulation was performed in adult population. As unanticipated DAM often occurs in pediatric or obstetric patients, which show specific anatomic or physiologic characteristics, the establishment or modification of DAM guideline is essential according to the age variations.17,18
When establishing pediatric DAM guidelines, it is crucial to consider specific factors unique to pediatric patients. The children generally have a shorter tolerance time for hypoxia compared to the adults. Additionally, many SGDs, originally designed for adults, are often utilized in pediatric cases, making it imperative to conduct comprehensive evaluations of their suitability for pediatric applications.19 Invasive airway management is typically discouraged in pediatrics due to the inherent challenges associated with identifying the cricothyroid membrane and the relatively extended time required. Furthermore, pediatric patients may present with various congenital syndromes, each posing specific challenges in airway management. Therefore, it is essential to accumulate and analyze data to gain a better understanding of these complexities. In cases involving pediatric patients with congenital cardiac diseases, careful consideration of controlling the pulmonary/systemic blood flow ratio is of utmost importance. The pediatric airway management, especially in unanticipated difficult airway cases, rapid and definitive airway management is needed. Thus, perioperative team training including nurses and medical engineers are essential.20 Based on DAM evidence and database in specific clinical characteristics, a DAM guideline development for special situation is warranted for the future.
5. Need for trouble management guidelines during anesthesia
Although evidence accumulation is not easy and unpractical in emergency response, there are various case reports on the airway management trouble during the maintenance of anesthesia.21, 22, 23 Sudden airway loss in the prone position is a high risk, especially during robot-assisted surgery.24 Pneumothorax or asthma attack is also a high-risk complication during mechanical ventilation. While there is insufficient evidence of successful use of VLS or SGDs for emergency airway management in positions other than supine position, some consensus is still required.
Furthermore, there are several possible mechanisms for impossible ventilation such as anaphylactic reaction, severe asthma attack, or airway fire.25 As these airway troubles need specific resolutions, some basic management flow is warranted in the future. Such guideline should be practiced by all OR members because the airway crisis during operation often needs collaboration of the surgeon and the nurses. Interprofessional training as perioperative team is warranted for airway crises during surgery.
The OR environment stands distinct from other hospital settings due to several key factors. Within the OR, patients receive continuous monitoring, and essential medical information such as body weight and relevant medical history is readily available to the management team during crisis situations. Additionally, the causes of airway crises are often identifiable, such as instances of airway fires or accidental tracheal tube extubation.
Personnel involved in crisis management typically have defined roles, with a clear distinction between those engaged in the operative field (e.g., surgeons, scrub nurses) and those involved in non-operative field activities (e.g., anesthesiologists, circulating nurses, and paramedical staff (medical engineers).26 During crises, personnel in the operative and non-operative fields maintain their designated roles and collaborate within their professional and spatially designated working areas.27 For instance, the surgeons and scrub nurses focus on managing airway fires in the operative field, while others concentrate on resuscitation strategies, such as re-inserting airway devices or ensuring oxygenation.
Incorporating assessments of interaction and collaboration between operative and non-operative field personnel is imperative for effective OR crisis management and teamwork.28 Potential modifications might encompass enhancing "shared situational awareness between the operative and non-operative fields" and ensuring "effective verbal communication between the operative and non-operative fields." Formative assessments of these factors can further enhance the effectiveness of simulation training for perioperative team management during emergency airway resuscitation in the OR.
6. Postoperative airway management guidelines
There is also a need for evidence accumulation and interprofessional guideline for postoperative airway management guideline. One national study showed non-negligible number of airway trouble after recovery of anesthesia.29 As there is no clear evidence on the duration of oxygen administration time or patient position after operation. Furthermore, intravenous opioid injection or sedative administration affect patient airway.30 From the viewpoint of patient characteristics, postoperative airway management should be performed based on age, body weight, oxygenation status, presence of sleep apnea syndrome, and operation performed (Box 3). Such future evidence accumulation can minimize the incidence and severity of airway trouble during the recovery period.
Furthermore, rapid response system focused on postoperative airway crisis is warranted too. The primary concern associated with postoperative airway crises is the occurrence of respiratory suppression or airway obstruction, which can lead to hypoxia. As a result, the initial response of a rapid response system to an airway crisis involves the detection of hypoxia and hypoventilation through patient observation or monitoring. In a clinical setting, the subsequent steps taken by medical staff typically include administering high-flow oxygen and implementing basic airway management techniques to alleviate upper airway obstruction. This may involve the use of the triple airway maneuver or assisting with ventilation, which can be achieved through oral, nasal, or supraglottic airway methods. Additionally, the administration of antagonists can serve as a rescue intervention in cases of respiratory suppression following opioid administration. Since the choice of sedatives and analgesics may vary based on the specific procedure's purpose, interprofessional perioperative airway crisis management training should emphasize the importance of sharing information about the drugs administered with potential rescuers.
To enhance the rapid response system in each recovery department, the following key objectives should be pursued:
I have discussed the future standards for airway management and possible indications for airway management. The introduction of various new airway devices can lead to more practical airway guidelines, along with the incorporation of new evaluation criteria. While most of the evidence regarding airway management has primarily been accumulated during the induction of anesthesia, it is imperative that we explore emergency airway management both during and after surgery. Additionally, we should not limit our focus to adult airway management but also address special situations such as obstetrics or pediatrics. Interprofessional training in airway management is essential for all members of the perioperative team.
8. Competing interests
The author has no affiliation with any manufacturer of any device described in the manuscript, and declare no financial interest in relation to the material described in the manuscript.
9. Funding
This research was partially supported by the Ministry of Education, Science, Sports and Culture, Grant-in Aid for Scientific Research(C), 2022-2024(22K10430, Nobuyasu Komasawa)
Author affiliation:
Nobuyasu Komasawa, MD, PhD, Community Medicine Education Promotion Office, Kagawa Medical University, 1750-1 Ikenobe, Miki-cho, Kita-gun, Kagawa, 761-0793, Japan.
Correspondence: Nobuyasu Komasawa, E-mail: komasawa.nobuyasu@kagawa-u.ac.jp; Phone: +81-87-891-2442; Fax: +81-87-891-2442.
ABSTRACT
Airway management evidence has primarily been gathered within the operating room, particularly during the induction of anesthesia. The introduction of newly developed supraglottic devices and videolaryngoscopes have significantly impacted the guidelines for managing difficult airways, prompting the need for new evaluation criteria. Moreover, airway complications such as accidental extubation may occur during surgery, while aspiration or respiratory suppression can manifest during the recovery period following extubation. In this review, I will explore the potential future standards for airway management and potential indications for its application. Additionally, I will underscore the significance of emergency airway management during both the surgical procedure and the recovery phase. It is imperative that we not only accumulate knowledge related to managing difficult airways but also focus on emergency airway management in the future. This calls for interprofessional airway management training for all members of the perioperative team.
Key words: Airway Management; Videolaryngoscope; Supraglottic Device; Future Direction
Abbreviations: DAM - Difficult Airway Management; DAS - Difficult Airway Society; OR - operating room; SGD - Supraglottic Device; VLS – videolaryngoscope
Citation: Komasawa N. Advancing airway management for enhanced patient outcomes: a narrative review. Anaesth. pain intensive care 2024;28(1):171−176; DOI: 10.35975/apic.v28i1.2391
Received: December 12, 2023; Reviewed: December 16, 2023; Accepted: December 16, 2023
1. INTRODUCTION
Airway management is an art, and the anesthesiologists are considered masters of this art. In fact, some senior anesthesiologists use to say that “Anesthesia is nothing but airway management” (Professor M. Salim, Pakistan). It is the primary skill learnt by the trainees in anesthesiology, and they will always be called throughout their future careers, whenever colleagues from other specialties will face difficulty with airway. However, airway management is not specific to the anesthesiologists, and emergency medicine specialists and intensive care specialists must also be proficient in this skill.
All anesthetic drugs, including sedatives, analgesics, and muscle relaxants, have an impact on airway maintenance to some extent.1,2 Therefore, ensuring the safe management of a patient's airway is the primary responsibility of all anesthesiologists. Worldwide, various airway management guidelines have been established to enhance the safety of patients undergoing general anesthesia. The bulk of evidence related to airway management has been accumulated primarily in the operating room (OR), particularly during the induction of anesthesia.3,4
The advent of newly developed videolaryngoscopes (VLS) and supraglottic devices, has brought about significant changes and opened up new horizons in difficult airway management guidelines. In this review, I will initially address the necessity of tracheal tube passage in the era of VLS and discuss the ventilation scale for supraglottic devices, as well as specific modifications for special situations. Subsequently, I will underscore the expansion of evidence-based airway management to encompass intraoperative and perioperative recovery periods
2. VLS in airway management
Sufficient laryngoscopy does not ensure successful tracheal intubation
The Difficult Airway Management (DAM) Algorithms / Guidelines from the American Society of Anesthesiologists (ASA) delineate five distinct challenging airway scenarios. These include:
1. Challenging mask ventilation;
2. Challenging laryngoscopy;
3. Challenging tracheal intubation;
4. Challenging placement of supraglottic devices (SGD); and
5. Challenging invasive airway management.5
The ASA-DAM recommends anesthesiologists to prepare for airway management based on these guidelines. The most commonly utilized system for anticipating difficult airways is the Mallampati classification, which proves valuable in predicting challenges with mask ventilation and intubation.6 Recent advancements have introduced various types of VLS capable of indirect laryngoscopy.7 These devices simplify the laryngoscopy procedure significantly, and certain guidelines propose them as the preferred choice in specific scenarios.8 However, in some cases, while the glottis may be clearly visible, advancing the tube into the trachea can pose challenges due to factors such as a mismatch between the trachea and tube alignment, anatomical issues like subglottic narrowing, or laryngeal deviation.
Given that the ASA-DAM guidelines differentiate between challenging laryngoscopy and challenging intubation, it is essential to evaluate each on a distinct scale. Although the Cormack-Lehane system is commonly employed for assessing laryngoscopy, there is no equivalent system for grading challenging intubations, i.e., the passage of the tracheal tube through the glottis. A previously proposed alternative evaluation system is the "tracheal tube passage through glottis (TTPG) grade," consisting of four distinct grades: "no resistance," "minor resistance," "major resistance," and "impossible passage" (Box 1).9 Implementing such a novel system would facilitate the evaluation of challenging intubations and allow for correlations with predictive factors for difficult airway management. Furthermore, such tube passage grading can link to difficult airway management to subglottic regions in which clear evidence has not been validated sufficiently yet.
| Box 1: Possible tracheal tube passage through glottis (TTPG) grade (referred and modified from reference 9). | |
| Grade 1 | No resistance |
| Grade 2 | Minor resistance |
| Grade 3 | Major resistance |
| Grade 4 | Impossible passage |
3. Classification of SGDs for emergency airway management
In addition to VLS, a range of new SGDs with varying features have been developed. The guidelines from the Difficult Airway Society (DAS) and the ASA recommend the early use of SGDs for airway rescue in cases where ventilation is insufficient or impossible, aiming to prevent hypoxia-induced cardiac arrest.10 For airway management during resuscitation, both the American Heart Association (AHA) and the European Resuscitation Council (ERC) Cardiopulmonary Resuscitation guidelines recommend SGDs that can be inserted without interrupting chest compressions.11,12 Consequently, SGDs play a critical role in emergent airway management not only in the OR but also in the general wards and prehospital resuscitations.
Various types of SGDs are now available, including the traditional laryngeal mask, anatomically-shaped SGDs like the LMA-ProSeal, cuffless soft gel SGDs such as the i-gel, and esophagus-blocking SGDs like the laryngeal tube and Combitube. These airway management devices are collectively referred to as 'SGDs' because they do not require tracheal intubation and provide a seal within the pharyngeal anatomy.
Several randomized clinical and simulation studies have demonstrated that the rigid curved tube structure of SGDs facilitates easy placement, with added stomach tube passage to prevent aspiration.13 Although these devices have distinct functionalities, the difficulty of SGD insertion can be reduced in various ways, warranting a shift in evaluation focus from 'insertion' to 'ventilation.' To enhance effective emergency airway management with SGDs, there is a compelling need to gather and analyze data, classifying which SGDs are suitable for different scenarios.
While the ASA-DAM defines five patterns of difficult airway management as previously described,13 it is important to note that challenging mask ventilation and challenging tracheal intubation are classified separately.14,15 However, there are currently no equivalent systems for assessing the effectiveness of ventilation with SGDs. Since the primary goal of SGD insertion in ventilation rescue is to secure the airway and provide oxygen to the lungs, the evaluation scale for successful airway rescue with SGDs should differ from that used in general anesthesia, where high-sealing pressure is essential during mechanical ventilation.
The author previously suggested a new evaluation scale, the “ventilation efficacy with SGD (V-SGD) scale,” comprising the following three grades: “insufficient ventilation with SGD and decreased SpO2,” “insufficient ventilation with SGD but with maintained SpO2 (insufficient sealing pressure)” and “sufficient ventilation and maintained SpO2 (sufficient sealing pressure)” (Box 2).16 The V-SGD evaluation scale, which allows for the evaluation of SGD, may be useful not only for evaluating the ventilation status with conventional SGD during general anesthesia but also for decision-making during rescue application of various SGDs in difficult or ‘can’t ventilate, can’t intubate’ emergency situations.
| Box 2: Possible ventilation scoring with supraglottic devices: ventilation efficacy with SGD (V-SGD) scale (Modified from Komasawa N & Minami T)16 | |
| Grade 1 | Sufficient ventilation and maintained SpO2 (sufficient sealing pressure) |
| Grade 2 | Insufficient ventilation with SGD but with maintained SpO2 (insufficient sealing pressure) |
| Grade 3 | Insufficient ventilation with SGD and decreased SpO2 |
In summary, newly developed VLSs or SGDs significantly affected the difficult airway management (Figure 1). In other words, VLS have reduced the frequency of difficult laryngoscopy and clarified the needs of tracheal tube passages, while SGD variations have alleviated insertion difficulty and offered an at-hand means of rescue ventilation.
4. Application and Expansion for DAS Guidelines in Special Situations
Various airway management guidelines have been published worldwide. However, most of the guidelines were established by evidence in adult cases and not in pediatric ones. One major reason of this is that various clinical studies and data accumulation was performed in adult population. As unanticipated DAM often occurs in pediatric or obstetric patients, which show specific anatomic or physiologic characteristics, the establishment or modification of DAM guideline is essential according to the age variations.17,18
When establishing pediatric DAM guidelines, it is crucial to consider specific factors unique to pediatric patients. The children generally have a shorter tolerance time for hypoxia compared to the adults. Additionally, many SGDs, originally designed for adults, are often utilized in pediatric cases, making it imperative to conduct comprehensive evaluations of their suitability for pediatric applications.19 Invasive airway management is typically discouraged in pediatrics due to the inherent challenges associated with identifying the cricothyroid membrane and the relatively extended time required. Furthermore, pediatric patients may present with various congenital syndromes, each posing specific challenges in airway management. Therefore, it is essential to accumulate and analyze data to gain a better understanding of these complexities. In cases involving pediatric patients with congenital cardiac diseases, careful consideration of controlling the pulmonary/systemic blood flow ratio is of utmost importance. The pediatric airway management, especially in unanticipated difficult airway cases, rapid and definitive airway management is needed. Thus, perioperative team training including nurses and medical engineers are essential.20 Based on DAM evidence and database in specific clinical characteristics, a DAM guideline development for special situation is warranted for the future.
5. Need for trouble management guidelines during anesthesia
Although evidence accumulation is not easy and unpractical in emergency response, there are various case reports on the airway management trouble during the maintenance of anesthesia.21, 22, 23 Sudden airway loss in the prone position is a high risk, especially during robot-assisted surgery.24 Pneumothorax or asthma attack is also a high-risk complication during mechanical ventilation. While there is insufficient evidence of successful use of VLS or SGDs for emergency airway management in positions other than supine position, some consensus is still required.
Furthermore, there are several possible mechanisms for impossible ventilation such as anaphylactic reaction, severe asthma attack, or airway fire.25 As these airway troubles need specific resolutions, some basic management flow is warranted in the future. Such guideline should be practiced by all OR members because the airway crisis during operation often needs collaboration of the surgeon and the nurses. Interprofessional training as perioperative team is warranted for airway crises during surgery.
The OR environment stands distinct from other hospital settings due to several key factors. Within the OR, patients receive continuous monitoring, and essential medical information such as body weight and relevant medical history is readily available to the management team during crisis situations. Additionally, the causes of airway crises are often identifiable, such as instances of airway fires or accidental tracheal tube extubation.
Personnel involved in crisis management typically have defined roles, with a clear distinction between those engaged in the operative field (e.g., surgeons, scrub nurses) and those involved in non-operative field activities (e.g., anesthesiologists, circulating nurses, and paramedical staff (medical engineers).26 During crises, personnel in the operative and non-operative fields maintain their designated roles and collaborate within their professional and spatially designated working areas.27 For instance, the surgeons and scrub nurses focus on managing airway fires in the operative field, while others concentrate on resuscitation strategies, such as re-inserting airway devices or ensuring oxygenation.
Incorporating assessments of interaction and collaboration between operative and non-operative field personnel is imperative for effective OR crisis management and teamwork.28 Potential modifications might encompass enhancing "shared situational awareness between the operative and non-operative fields" and ensuring "effective verbal communication between the operative and non-operative fields." Formative assessments of these factors can further enhance the effectiveness of simulation training for perioperative team management during emergency airway resuscitation in the OR.
6. Postoperative airway management guidelines
There is also a need for evidence accumulation and interprofessional guideline for postoperative airway management guideline. One national study showed non-negligible number of airway trouble after recovery of anesthesia.29 As there is no clear evidence on the duration of oxygen administration time or patient position after operation. Furthermore, intravenous opioid injection or sedative administration affect patient airway.30 From the viewpoint of patient characteristics, postoperative airway management should be performed based on age, body weight, oxygenation status, presence of sleep apnea syndrome, and operation performed (Box 3). Such future evidence accumulation can minimize the incidence and severity of airway trouble during the recovery period.
| Box 3: Areas in which evidence accumulation is needed for postoperative recovery period | |
| 1 | Appropriate oxygen time for patients who undergo intravenous opioid administration |
| 2 | Appropriate oxygen administration volume and time based on patient conditions |
| 3 | Patient position or pillow height during recovery period |
| 4 | Appropriate respiratory monitoring |
| 5 | Rapid response system during postoperative recovery period |
Furthermore, rapid response system focused on postoperative airway crisis is warranted too. The primary concern associated with postoperative airway crises is the occurrence of respiratory suppression or airway obstruction, which can lead to hypoxia. As a result, the initial response of a rapid response system to an airway crisis involves the detection of hypoxia and hypoventilation through patient observation or monitoring. In a clinical setting, the subsequent steps taken by medical staff typically include administering high-flow oxygen and implementing basic airway management techniques to alleviate upper airway obstruction. This may involve the use of the triple airway maneuver or assisting with ventilation, which can be achieved through oral, nasal, or supraglottic airway methods. Additionally, the administration of antagonists can serve as a rescue intervention in cases of respiratory suppression following opioid administration. Since the choice of sedatives and analgesics may vary based on the specific procedure's purpose, interprofessional perioperative airway crisis management training should emphasize the importance of sharing information about the drugs administered with potential rescuers.
To enhance the rapid response system in each recovery department, the following key objectives should be pursued:
- Establish a patient safety system that incorporates monitoring and emergency airway management devices to promptly identify cases of emergency respiratory suppression;
- Activate the rapid response system in response to incidents of respiratory suppression;
- Develop a standardized airway rescue protocol for addressing both airway obstruction as well as respiratory suppression; and
- Implement an opioid-specific rescue kit that goes beyond conventional equipment and medications, including various airway devices (such as supraglottic devices) and antagonists like naloxone.
7. CONCLUSION
I have discussed the future standards for airway management and possible indications for airway management. The introduction of various new airway devices can lead to more practical airway guidelines, along with the incorporation of new evaluation criteria. While most of the evidence regarding airway management has primarily been accumulated during the induction of anesthesia, it is imperative that we explore emergency airway management both during and after surgery. Additionally, we should not limit our focus to adult airway management but also address special situations such as obstetrics or pediatrics. Interprofessional training in airway management is essential for all members of the perioperative team.
8. Competing interests
The author has no affiliation with any manufacturer of any device described in the manuscript, and declare no financial interest in relation to the material described in the manuscript.
9. Funding
This research was partially supported by the Ministry of Education, Science, Sports and Culture, Grant-in Aid for Scientific Research(C), 2022-2024(22K10430, Nobuyasu Komasawa)
10. REFERENCES
- Henderson JJ, Popat MT, Latto IP, Pearce AC; Difficult Airway Society. Difficult airway society guidelines for management of the unanticipated difficult intubation. Anaesthesia. 2004;59:675–694. [PubMed] DOI: 1111/j.1365-2044.2004.03831.x
- Cumberworth A, Lewith H, Sud A, Jefferson H, Athanassoglou V, Pandit JJ. Major complications of airway management: a prospective multicentre observational study. Anaesthesia. 2022;77:640-648. [PubMed] DOI: 1111/anae.15668
- Janssens M, Hartstein G. Management of difficult intubation. Eur J Anaesthesiol. 2001;18:3-12. [PubMed] DOI: 1046/j.0265-0215.2000.00777.x
- Kheterpal S, Martin L, Shanks AM, Tremper KK. Prediction and outcomes of impossible mask ventilation: a review of 50,000 anesthetics. Anesthesiology. 2009;110:891-897. [PubMed] DOI: 1097/ALN.0b013e31819b5b87
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022;136:31-81. [PubMed] DOI: 1097/ALN.0000000000004002
- Narra LR, Udongwo N, Dominic JL, Doreswamy S, Bhasir A, Elkherpitawy I, et al. Obesity and the Other Independent Predictors in Elective Endotracheal Tube Intubations: A Narrative Review. J Clin Med Res. 2022;14:177-187. [PubMed] DOI: 14740/jocmr4727
- Kido H, Komasawa N, Matsunami S, Kusaka Y, Minami T. Comparison of McGRATH MAC and Macintosh laryngoscopes for double-lumen endotracheal tube intubation by anesthesia residents: a prospective randomized clinical trial. J Clin Anesth. 2015;27:476-480. [PubMed] DOI: 1016/j.jclinane.2015.05.011
- Komasawa N, Kido H, Miyazaki Y, Tatsumi S, Minami T. Cricoid pressure impedes tracheal intubation with the Pentax-AWS Airwayscope®: a prospective randomized trial. Br J Anaesth. 2016;116:413-416. [PubMed] DOI: 1093/bja/aev438
- Komasawa N, Minami T. A scale for evaluating the difficulty of tracheal tube passage though the glottis is needed; good laryngoscopy does not always ensure intubation success. J Clin Anesth. 2016;28:82-83. [PubMed] DOI: 1016/j.jclinane.2015.06.014
- Komasawa N, Ueki R, Kaminoh Y, Nishi S. Evaluation of chest compression effect on airway management with air-Q, aura-i, i-gel, and Fastrack intubating supraglottic devices by novice physicians: a randomized crossover simulation study. J Anesth. 2014;28:676-680. [PubMed] DOI: 1007/s00540-014-1802-1
- Soar J, Berg KM, Andersen LW, Böttiger BW, Cacciola S, Callaway CW, et al. Adult advanced life support: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2020;156:A80-A119. [PubMed] DOI: 1016/j.resuscitation.2020.09.012
- Merchant RM, Topjian AA, Panchal AR, Cheng A, Aziz K, Berg KM, et al. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S337-S357. [PubMed] DOI: 1161/CIR.0000000000000918
- Ishio J, Komasawa N, Miyazaki Y, Kido H, Minami T. LMA-ProSeal insertion by novice doctors as affected by a 90° bend created by an intubating stylet: a randomized clinical trial. J Clin Anesth. 2016;34:145-150. [PubMed] DOI: 1016/j.jclinane.2016.03.072
- Ohchi F, Komasawa N, Imagawa K, Okamoto K, Minami T. Evaluation of the efficacy of six supraglottic devices for airway management in dark conditions: a crossover randomized simulation trial. J Anesth. 2015;29:887-892. [PubMed] DOI: 1007/s00540-015-2050-8
- Matsunami S, Komasawa N, Konishi Y, Minami T. Head elevation and lateral head rotation effect on facemask ventilation efficiency: Randomized crossover trials. Am J Emerg Med. 2017;35:1709-1712. [PubMed] DOI: 1016/j.ajem.2017.05.004
- Komasawa N, Minami T. Need for a new evaluation scale for the efficacy of ventilation with supraglottic devices. J Clin Anesth. 2016;31:201. [PubMed] DOI: 1016/j.jclinane.2016.02.007
- Jagannathan N, Asai T. Difficult airway management: children are different from adults, and neonates are different from children! Br J Anaesth. 2021;126:1086-1088. [PubMed] DOI: 1016/j.bja.2021.03.012
- Komasawa N, Matsunami S, Minami T. A proposal for pediatric specific difficult airway management guideline. J Clin Anesth. 2020;62:109726. [PubMed] DOI: 1016/j.jclinane.2020.109726
- Black AE, Flynn PE, Smith HL, Thomas ML, Wilkinson KA. Development of a guideline for the management of the unanticipated difficult airway in pediatric practice. Paediatr Anaesth. 2015;25:346-362. [PubMed] DOI: 1111/pan.12615
- Pierre R 2nd, Dym H. Endotracheal Tube Obstruction via Turbinectomy During Nasal Intubation. Anesth Prog. 2018;65:255-258. [PubMed] DOI: 2344/anpr-65-04-09
- Bosch L, Sadurní M, Nuñez M, Pacreu S. Anesthesia management of accidental extubation in the prone position. Rev Esp Anestesiol Reanim. 2017;64:237-239. [PubMed] DOI: 1016/j.redar.2016.11.002
- Wagner KM, Raskin JS, Carling NP, Felberg MA, Kanjia MK, Pan IW, et al. Unplanned Intraoperative Extubations in Pediatric Neurosurgery: Analysis of Case Series to Increase Patient Safety. World Neurosurg. 2018;115:e1-e6. [PubMed] DOI: 1016/j.wneu.2017.10.149
- Mohamed A, Shehada SE, Van Brakel L, Ruhparwar A, Hochreiter M, Berger MM, et al. Anesthetic Management during Robotic-Assisted Minimal Invasive Thymectomy Using the Da Vinci System: A Single Center Experience. J Clin Med. 2022;11:4274. [PubMed] DOI: 3390/jcm11154274
- Iliff HA, El-Boghdadly K, Ahmad I, Davis J, Harris A, Khan S, et al. Management of haematoma after thyroid surgery: systematic review and multidisciplinary consensus guidelines from the Difficult Airway Society, the British Association of Endocrine and Thyroid Surgeons and the British Association of Otorhinolaryngology, Head and Neck Surgery. Anaesthesia. 2022;77:82-95. [PubMed] DOI: 1111/anae.15585
- Fletcher G, McGeorge P, Flin R, Glavin R, Maran N. The role of nontechnical skills in anaesthesia: a review of current literature. Br J Anaesth. 2002;88:418-429. [PubMed] DOI: 1093/bja/88.3.418
- Komasawa N, Berg BW. A proposal for modification of non-technical skill assessment for perioperative crisis management simulation training. J Clin Anesth. 2016;32:25-26. [PubMed] DOI: 1016/j.jclinane.2015.12.031
- Komasawa N, Berg BW. Simulation-based Airway Management Training for Anesthesiologists - A Brief Review of its Essential Role in Skills Training for Clinical Competency. J Educ Perioper Med. 2017;19:E612. [PubMed]
- Nguyen MC, Moffatt-Bruce SD, Strosberg DS, Puttmann KT, Pan YL, Eiferman DS. Agency for Healthcare Research and Quality (AHRQ) Patient Safety Indicator for Postoperative Respiratory Failure (PSI 11) does not identify accurately patients who received unsafe care. Surgery. 2016;160:858-868. [PubMed] DOI: 1016/j.surg.2016.05.032
- Lee LA, Caplan RA, Stephens LS, Posner KL, Terman GW, Voepel-Lewis T, et al. Postoperative opioid-induced respiratory depression: a closed claims analysis. Anesthesiology. 2015;122:659-665. [PubMed] DOI: 1097/ALN.0000000000000564
- Yamasaki T, Komasawa N, Kido H, Minami T. Contribution of the nasal passage to face mask ventilation: a prospective blinded randomized crossover trial. Can J Anaesth. 2017;64:935-939. [PubMed] DOI: 1007/s12630-017-0911-3