Hanik Badriyah Hidayati1, Vania Ayu Puspamaniar2, Alexander Tikara Sugondo3, Fajar Sena Firdausa4
Author affiliations:
Peripheral nerve blocks, including occipital nerve blocks (ONBs), have received increased attention and support as pain management tools during the previous few decades. Researchers have documented usefulness of ONBs particularly for acute headache management in the outpatient setting. The blocks also play a role in other healthcare settings, such as in the emergency department. The potential role of ONBs for the management of acute headache episodes in primary and emergency care settings is not yet fully practiced. In this paper, we will review block techniques of third occipital nerve (TON): indication, medication selection, complications and measures that can help improve safety in this procedure of headache management.
Key word: Analgesia, Regional; Headache; Occipital Nerve Block; Occipital Neuralgia; Third Occipital Nerve; Ultrasound-Guide.
Citation: Hidayati HB, Puspamaniar VA, Sugondo AT, Firdausa FS. Ultrasound-guided third occipital nerve (TON) blocks. Anaesth. pain intensive care 2024;28(1):166−170; DOI: 10.35975/apic.v28i1.2390
Received: October 13, 2023; Reviewed: October 18, 2023; Accepted: January 02, 2024
Regional anesthesia has witnessed many ups and downs. The initial phases of both spinal as well as epidural analgesia were associated with poor pharmacologic and even anatomic knowledge, but with the passage of time our knowledge was rapidly proliferated, and with it came the renaissance of regional analgesia. Further progress was made with the advent of selective nerve blocks. A few decades passed with the regional anesthetists continued the landmark technique for the nerve blocks, followed by the introduction of nerve stimulators, which increased the precision and reduced the chances of block failure, while also reducing the frequency of accidental nerve damage. The great revolution was witnessed with the use of ultrasound guidance (USG) for location of the nerves and to judge the site and extent of the spread of injectate. Hand held probes will soon be found in the pockets of the anesthetists.
The USG nerve blocks were not confined for the sole or supplementary anesthesia for the surgical procedures; but the use was quickly picked up by the pain management enthusiasts. This review offers salient highlights of management of headache by blocking third occipital nerve (TON).
Occipital nerve blocks are useful in the treatment of headache.1 Third occipital nerve (TON) block (Figure 1) is useful in the diagnosis and treatment of TON headaches.3 The symptoms of TON neuralgia are similar to those of greater occipital nerve (GON) neuralgia.4 In TON headaches, it is suspected that the source is at the C2-C3 facet joints. TON headaches are commonly seen in patients who have suffered cervical spine trauma from whiplash injuries. Patients suffering from TON headaches complain of pain in the posterior neck as well as occipital headache accompanied by stiffness in the C2-C3 facet joints.3
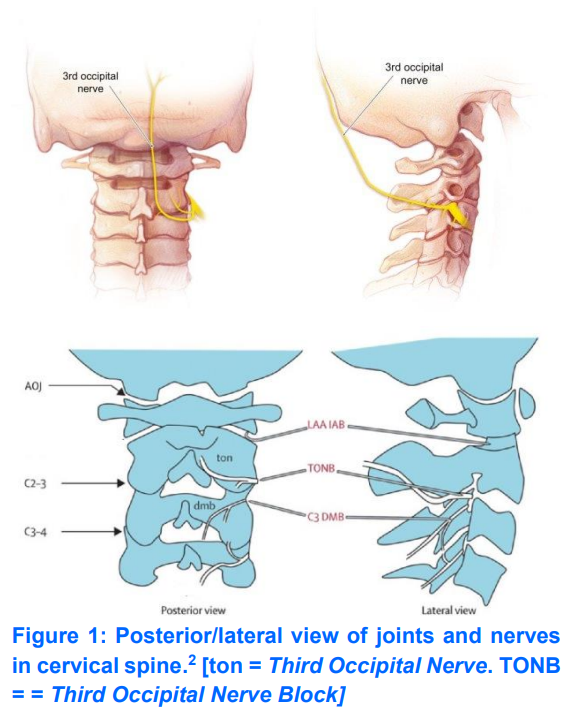
The dorsal ramus of C3 has a complex branch pattern. It originates from the articular pillar of the C3 vertebra. The nerve then divides into lateral and medial branches. The medial branch divides into deep and superficial branches. The superficial medial branch is known as the TON.4
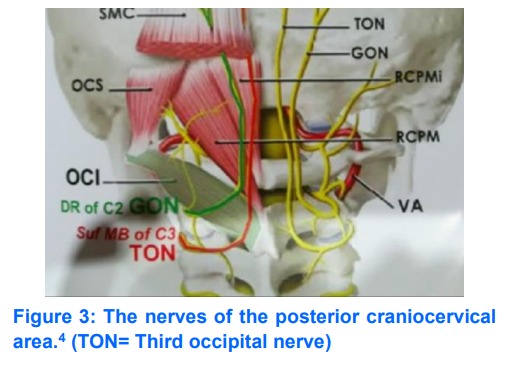
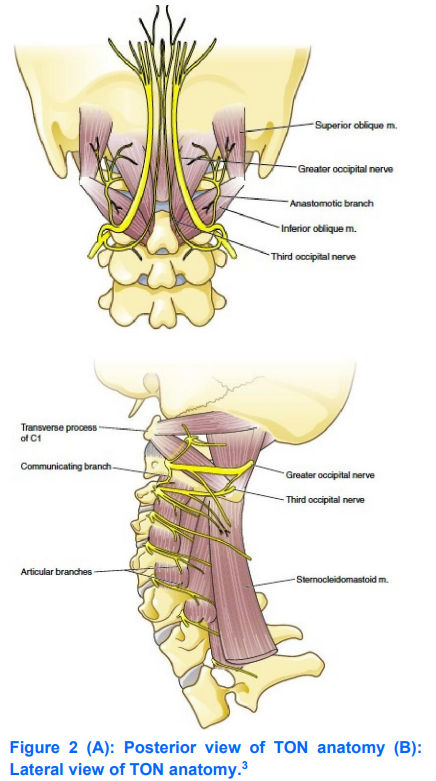
TON originates from the dorsal ramus of the cervical nerve as one of the three branches, at the level of the trapezius muscle (Figure 2). 2,4,5 It runs on the dorsomedial superior articular process of vertebra C3 (Figure 3),3 and the dorsolateral surface of the facet joints C2-3.4 The TON fibers from the medial branch of C3 and the small communicating fibers of the C2 nerve provide the primary innervation to the C2-C3 facet joints.3 Interestingly, the C2-3 level is innervated only by the TON alone, whereas levels below C2-3 are each innervated by 2 branches from the dorsal rami.4 The TON fibers then run upward to provide sensory innervation to the ipsilateral suboccipital area.3 The TON provides innervation to the semispinalis capitis (SSC) muscle and travels into the muscle before sending communicating branches to the GON. After exiting the muscle, the GON becomes cutaneous and supplies a small area of skin below the superior nuchal line (Figure 3).4
When TON is successfully blocked with local anesthetic, the patient will experience numbness in a small area behind the ipsilateral ear (Figure 4).3
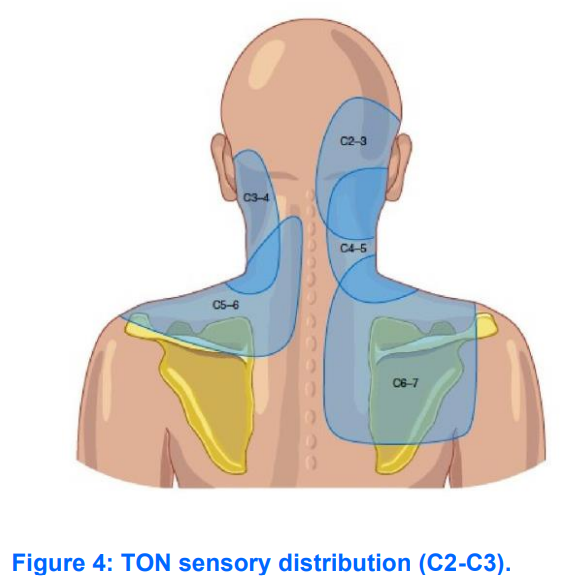
The pain map in the Figure 4 shows the distribution pattern of cervical zygapophysial joint pain from C2-C3 to C6-C7 levels. When a patient is suspected of having cervicogenic headache, the lateral atlantoaxial (C1-C2) and atlanto-occipital (C0-C1) joints should be considered as to be its source. Pain maps from the C0-C1, C1-C2, C2-C3, and C3-C4 joints overlap, they may provide clues to a possible source of cervicogenic headache. Pain maps in the thoracic spine region also overlap.3
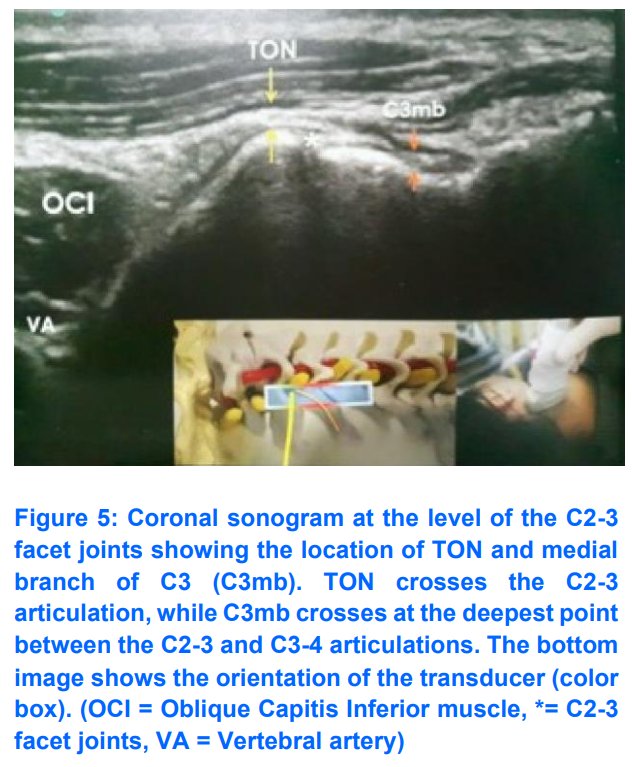
TON block with ultrasound guidance can be performed by placing the patient in the lateral decubitus position with the injection position on the upper side. The high-frequency (13-6 MHz) linear transducers are placed in a coronal position, where the facet columns could be identified. C2-3 characteristically appears as a drop off sign (Figure 5). At this level the TON appears as a hypoechoic structure overlying the C2-3 facet joints. If the transducer on C2-3 is rotated into a transverse plane, you will see the Inferior Articular Process (IAP) and Transversus Process (TP) of C2.4
Pain originating at C2-3 facet joints can be blocked by TON ipsilaterally when crossing the C2-3 facet joints. Pain from joints below C2-3 can be blocked by the medial cervical branch as it passes around the lumbar articular pillar.4
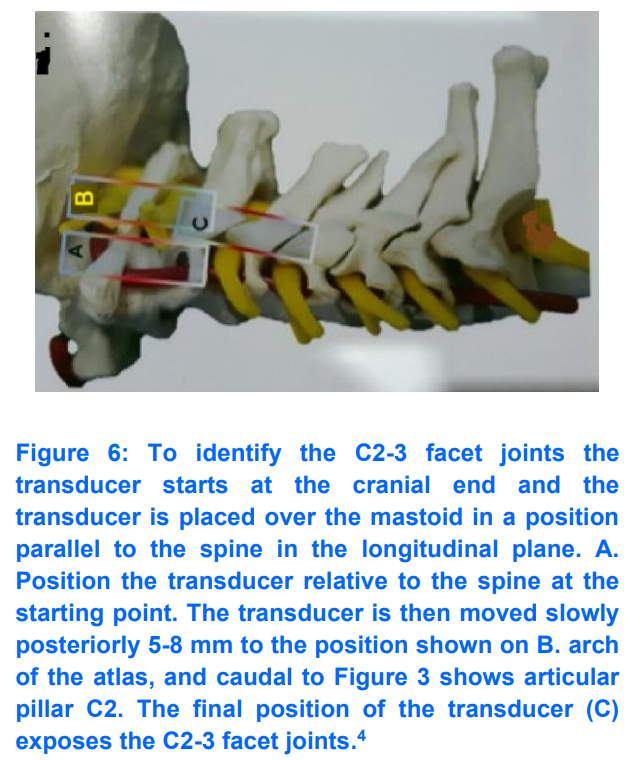
To identify the C2-3 facet joints the transducer starts at the cranial end and the transducer is placed over the mastoid in a position parallel to the spine in the longitudinal plane. The transducer is then moved anteriorly and posteriorly until the superficial bony shadow of the C1 transverse process is visible. By rotating the transducer slightly, the transverse process of C2 will be exposed, which is 2 cm from the transverse process of C1. Vertebral artery pulsation will be seen between the transverse processes of C1 and C2. Color Doppler can be used as a tool to help facilitate the identification of the vertebral arteries. In this position the vertebral arteries are on the anterolateral aspect of the C1-2 joints.4
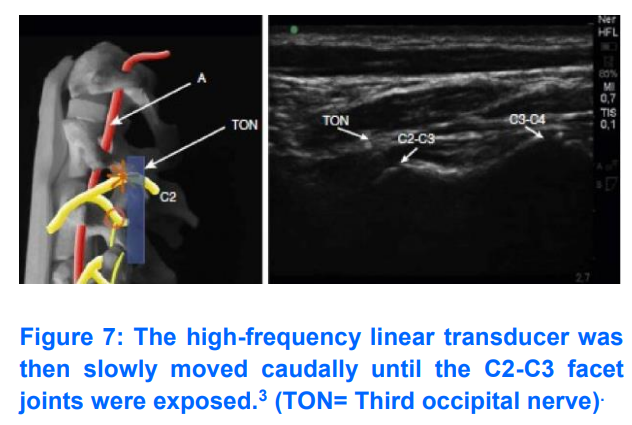
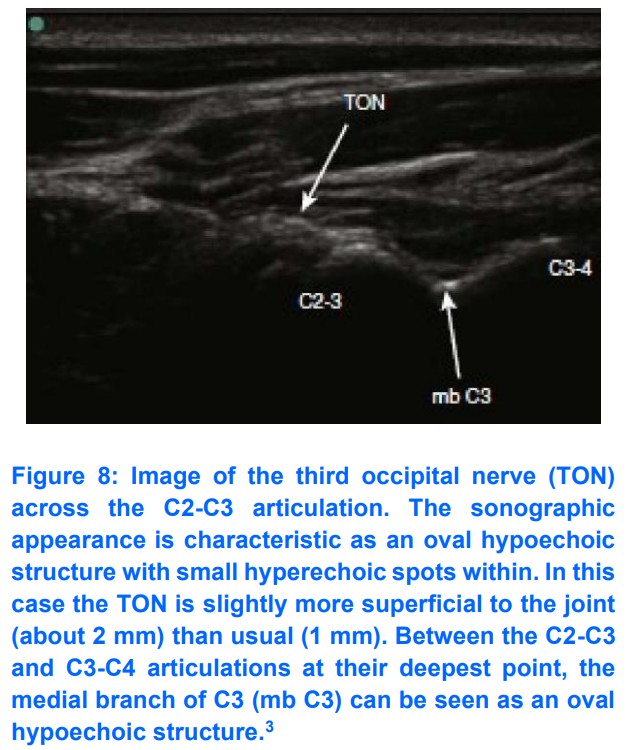
The transducer is then moved slowly posteriorly 5–8 mm (Figure 7B) until the curve of C1 (atlas) and the articular pillars of C2 (axis) can be identified.3, 4 The transducer is then moved slowly caudally,3,4 keeping the transducer in a longitudinal position with respect to the neck,4 until the C2-C3 facet joints are exposed (Figure 7).3 Place the articulation images C2-C3 and C3-C4 in the center of the ultrasound screen (Figure 5). The ultrasound transducer was then gently rotated toward the acoustic auditory meatus until the identified TONs passed just above the “hills” of the C2–C3 facet joints (Figure 8). The TON passes through the C2-3 facet joints at an average distance of 1 mm from the bone. The TON will appear as a hypoechoic point with internal hyperechoic.4 The C3 medial branch is visualized as a “valley” between the articulations of the C2-C3 facet joints and the C3-C4 facet joints.3
Once a TON is identified, a 3-inch needle is inserted anterior to the ultrasound transducer. The approach used is out-of-plane. The needle is inserted from anterior to posterior. The needle is advanced until it approaches the TON.3 Other literature says that the needle is inserted in- plane. The needle is inserted from the lateral side of the transducer until it contacts the C2 periosteum. The transducer is then rotated into the coronal position to confirm that the needle tip is near the nerve or just over joint C2-3.4
After gentle aspiration, 2 mL of the solution is then injected carefully to avoid the vertebral arteries. The vertebral arteries lie anterior to the facet joints. A total of 2 mL of the local anesthetic is drawn into a 10-mL sterile syringe. If the pain is suspected to have an inflammatory component, then 40 to 80 mg of depot steroid is added to the local anesthetic. The skin is then cleaned with an antiseptic solution. Identification of the mastoid process is done by palpation. Superior to the longitudinal orientation, a high-frequency linear ultrasound transducer is placed at the inferior border of the mastoid process, and a sonogram is taken.3 The needle is then removed. To avoid the formation of a hematoma at the injection site, pressure is applied.3
To get the potential effect of reducing pain symptoms for a longer time, radiofrequency ablation can be continued after a successful nerve block is performed.2 For TON block injection with the C-arm guidance technique, three needles need to be placed,2,4 namely superior to joint, at joint level and inferior to joint C2-3.2 Each joint is treated with 0.3 mL local anesthetic (total 0.9 mL). With ultrasound guidance the block is achieved with 0.5 mL.4
The proximity of TON to the exiting spinal nerve roots makes nerve root trauma and injection into the subarachnoid, subdural, or epidural spaces possible. Careful placement of the needle must be performed to avoid inserting the needle into the foramen magnum. Entry of local anesthetic into the subarachnoid can cause total spinal anesthesia.3
Because this area is highly vascularized,3 coupled with the fact that the TON is in close proximity to the vertebral arteries,3,4 this means that the pain specialists must carefully observe patients undergoing TON blocks because intravascular injection can occur.3 If intravascular injection occurs, it can cause significant central nervous system side effects, including ataxia, dizziness, and rarely, seizures.3 Doppler mode can be used to avoid vertebral artery puncture and injection.4
The proximity of the TON to the exit of the spinal nerve roots can result in trauma to the nerve roots and subarachnoid, subdural or epidural injections. Care should be taken to avoid inadvertent needle placement into the foramen magnum because subarachnoid administration of local anesthetic in this region will result in total direct spinal anesthesia.3
TON headache may be an underdiagnosed type of chronic daily headache. TON headache occurs after trauma to the upper cervical spine. The most common reason a TON block fails to relieve headache is because of a misdiagnosis of TON headache. In the absence of trauma, TON rarely causes headaches. More commonly, patients with headaches involving the occipital region suffer from tension-type headaches (TTH) or, less commonly, occipital neuralgia. In conjunction with cervical epidural nerve block with steroids, the TTH type of headache does not respond to TON block but responds to treatment with antidepressant compounds such as amitriptyline. Therefore, pain management specialists should reconsider the diagnosis of TON headache in patients whose symptoms are consistent with TON headaches but fail to respond to TON blocks (2017).6
Any patient with sufficiently severe headache requiring nerve block as part of the treatment plan should undergo head magnetic resonance imaging to rule out unexpected intracranial pathology that may mimic the clinical presentation of a TON headache.6 In addition, radiography of the cervical spine should be considered to rule out congenital abnormalities such as Arnold-Chiari malformation which may be a hidden cause of the patient's occipital headache.3
8. Acknowledgement
We gratefully thank the Faculty of Medicine, as well as the authors of the pictures used in this mini-review. Picture credits go to the original authors, mentioned with reference numbers.
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
HBH: research, performed the analysis, manuscript editing
VAP, ATS: literature research, manuscript reviewing and revising
Author affiliations:
- Hanik Badriyah Hidayati, Teaching Staff of Neurology Department, Faculty of Medicine Airlangga University – RSUD Dr. Soetomo, Surabaya, East Java, Indonesia: E-mail: hanikhidayati@fk.unair.ac.id
- Vania Ayu Puspamaniar, Student, Faculty of Medicine Airlangga University – RSUD Dr. Soetomo, Surabaya, East Java, Indonesia: E-mail: puspamaniar06@gmail.com
- Alexander Tikara Sugondo, Student, Faculty of Medicine Airlangga University – RSUD Dr. Soetomo, Surabaya, East Java, Indonesia: E-mail: alexandertikara37@gmail.com
- Fajar Sena Firdausa, Education Staff of Faculty of Medicine Airlangga University, Surabaya, East Java, Indonesia: E-mail: fajarbore2309@gmail.com
ABSTRACT
Peripheral nerve blocks, including occipital nerve blocks (ONBs), have received increased attention and support as pain management tools during the previous few decades. Researchers have documented usefulness of ONBs particularly for acute headache management in the outpatient setting. The blocks also play a role in other healthcare settings, such as in the emergency department. The potential role of ONBs for the management of acute headache episodes in primary and emergency care settings is not yet fully practiced. In this paper, we will review block techniques of third occipital nerve (TON): indication, medication selection, complications and measures that can help improve safety in this procedure of headache management.
Key word: Analgesia, Regional; Headache; Occipital Nerve Block; Occipital Neuralgia; Third Occipital Nerve; Ultrasound-Guide.
Citation: Hidayati HB, Puspamaniar VA, Sugondo AT, Firdausa FS. Ultrasound-guided third occipital nerve (TON) blocks. Anaesth. pain intensive care 2024;28(1):166−170; DOI: 10.35975/apic.v28i1.2390
Received: October 13, 2023; Reviewed: October 18, 2023; Accepted: January 02, 2024
1. INTRODUCTION
Regional anesthesia has witnessed many ups and downs. The initial phases of both spinal as well as epidural analgesia were associated with poor pharmacologic and even anatomic knowledge, but with the passage of time our knowledge was rapidly proliferated, and with it came the renaissance of regional analgesia. Further progress was made with the advent of selective nerve blocks. A few decades passed with the regional anesthetists continued the landmark technique for the nerve blocks, followed by the introduction of nerve stimulators, which increased the precision and reduced the chances of block failure, while also reducing the frequency of accidental nerve damage. The great revolution was witnessed with the use of ultrasound guidance (USG) for location of the nerves and to judge the site and extent of the spread of injectate. Hand held probes will soon be found in the pockets of the anesthetists.
The USG nerve blocks were not confined for the sole or supplementary anesthesia for the surgical procedures; but the use was quickly picked up by the pain management enthusiasts. This review offers salient highlights of management of headache by blocking third occipital nerve (TON).
2. INDICATIONS
Occipital nerve blocks are useful in the treatment of headache.1 Third occipital nerve (TON) block (Figure 1) is useful in the diagnosis and treatment of TON headaches.3 The symptoms of TON neuralgia are similar to those of greater occipital nerve (GON) neuralgia.4 In TON headaches, it is suspected that the source is at the C2-C3 facet joints. TON headaches are commonly seen in patients who have suffered cervical spine trauma from whiplash injuries. Patients suffering from TON headaches complain of pain in the posterior neck as well as occipital headache accompanied by stiffness in the C2-C3 facet joints.3
3. CLINICAL ANATOMY
The dorsal ramus of C3 has a complex branch pattern. It originates from the articular pillar of the C3 vertebra. The nerve then divides into lateral and medial branches. The medial branch divides into deep and superficial branches. The superficial medial branch is known as the TON.4
TON originates from the dorsal ramus of the cervical nerve as one of the three branches, at the level of the trapezius muscle (Figure 2). 2,4,5 It runs on the dorsomedial superior articular process of vertebra C3 (Figure 3),3 and the dorsolateral surface of the facet joints C2-3.4 The TON fibers from the medial branch of C3 and the small communicating fibers of the C2 nerve provide the primary innervation to the C2-C3 facet joints.3 Interestingly, the C2-3 level is innervated only by the TON alone, whereas levels below C2-3 are each innervated by 2 branches from the dorsal rami.4 The TON fibers then run upward to provide sensory innervation to the ipsilateral suboccipital area.3 The TON provides innervation to the semispinalis capitis (SSC) muscle and travels into the muscle before sending communicating branches to the GON. After exiting the muscle, the GON becomes cutaneous and supplies a small area of skin below the superior nuchal line (Figure 3).4
When TON is successfully blocked with local anesthetic, the patient will experience numbness in a small area behind the ipsilateral ear (Figure 4).3
The pain map in the Figure 4 shows the distribution pattern of cervical zygapophysial joint pain from C2-C3 to C6-C7 levels. When a patient is suspected of having cervicogenic headache, the lateral atlantoaxial (C1-C2) and atlanto-occipital (C0-C1) joints should be considered as to be its source. Pain maps from the C0-C1, C1-C2, C2-C3, and C3-C4 joints overlap, they may provide clues to a possible source of cervicogenic headache. Pain maps in the thoracic spine region also overlap.3
4. SONOANATOMY
TON block with ultrasound guidance can be performed by placing the patient in the lateral decubitus position with the injection position on the upper side. The high-frequency (13-6 MHz) linear transducers are placed in a coronal position, where the facet columns could be identified. C2-3 characteristically appears as a drop off sign (Figure 5). At this level the TON appears as a hypoechoic structure overlying the C2-3 facet joints. If the transducer on C2-3 is rotated into a transverse plane, you will see the Inferior Articular Process (IAP) and Transversus Process (TP) of C2.4
5. USG INJECTION TECHNIQUE
Pain originating at C2-3 facet joints can be blocked by TON ipsilaterally when crossing the C2-3 facet joints. Pain from joints below C2-3 can be blocked by the medial cervical branch as it passes around the lumbar articular pillar.4
To identify the C2-3 facet joints the transducer starts at the cranial end and the transducer is placed over the mastoid in a position parallel to the spine in the longitudinal plane. The transducer is then moved anteriorly and posteriorly until the superficial bony shadow of the C1 transverse process is visible. By rotating the transducer slightly, the transverse process of C2 will be exposed, which is 2 cm from the transverse process of C1. Vertebral artery pulsation will be seen between the transverse processes of C1 and C2. Color Doppler can be used as a tool to help facilitate the identification of the vertebral arteries. In this position the vertebral arteries are on the anterolateral aspect of the C1-2 joints.4
The transducer is then moved slowly posteriorly 5–8 mm (Figure 7B) until the curve of C1 (atlas) and the articular pillars of C2 (axis) can be identified.3, 4 The transducer is then moved slowly caudally,3,4 keeping the transducer in a longitudinal position with respect to the neck,4 until the C2-C3 facet joints are exposed (Figure 7).3 Place the articulation images C2-C3 and C3-C4 in the center of the ultrasound screen (Figure 5). The ultrasound transducer was then gently rotated toward the acoustic auditory meatus until the identified TONs passed just above the “hills” of the C2–C3 facet joints (Figure 8). The TON passes through the C2-3 facet joints at an average distance of 1 mm from the bone. The TON will appear as a hypoechoic point with internal hyperechoic.4 The C3 medial branch is visualized as a “valley” between the articulations of the C2-C3 facet joints and the C3-C4 facet joints.3
Once a TON is identified, a 3-inch needle is inserted anterior to the ultrasound transducer. The approach used is out-of-plane. The needle is inserted from anterior to posterior. The needle is advanced until it approaches the TON.3 Other literature says that the needle is inserted in- plane. The needle is inserted from the lateral side of the transducer until it contacts the C2 periosteum. The transducer is then rotated into the coronal position to confirm that the needle tip is near the nerve or just over joint C2-3.4
After gentle aspiration, 2 mL of the solution is then injected carefully to avoid the vertebral arteries. The vertebral arteries lie anterior to the facet joints. A total of 2 mL of the local anesthetic is drawn into a 10-mL sterile syringe. If the pain is suspected to have an inflammatory component, then 40 to 80 mg of depot steroid is added to the local anesthetic. The skin is then cleaned with an antiseptic solution. Identification of the mastoid process is done by palpation. Superior to the longitudinal orientation, a high-frequency linear ultrasound transducer is placed at the inferior border of the mastoid process, and a sonogram is taken.3 The needle is then removed. To avoid the formation of a hematoma at the injection site, pressure is applied.3
To get the potential effect of reducing pain symptoms for a longer time, radiofrequency ablation can be continued after a successful nerve block is performed.2 For TON block injection with the C-arm guidance technique, three needles need to be placed,2,4 namely superior to joint, at joint level and inferior to joint C2-3.2 Each joint is treated with 0.3 mL local anesthetic (total 0.9 mL). With ultrasound guidance the block is achieved with 0.5 mL.4
6. ADVERSE EFFECTS
The proximity of TON to the exiting spinal nerve roots makes nerve root trauma and injection into the subarachnoid, subdural, or epidural spaces possible. Careful placement of the needle must be performed to avoid inserting the needle into the foramen magnum. Entry of local anesthetic into the subarachnoid can cause total spinal anesthesia.3
Because this area is highly vascularized,3 coupled with the fact that the TON is in close proximity to the vertebral arteries,3,4 this means that the pain specialists must carefully observe patients undergoing TON blocks because intravascular injection can occur.3 If intravascular injection occurs, it can cause significant central nervous system side effects, including ataxia, dizziness, and rarely, seizures.3 Doppler mode can be used to avoid vertebral artery puncture and injection.4
The proximity of the TON to the exit of the spinal nerve roots can result in trauma to the nerve roots and subarachnoid, subdural or epidural injections. Care should be taken to avoid inadvertent needle placement into the foramen magnum because subarachnoid administration of local anesthetic in this region will result in total direct spinal anesthesia.3
7. SPECIAL NOTES
TON headache may be an underdiagnosed type of chronic daily headache. TON headache occurs after trauma to the upper cervical spine. The most common reason a TON block fails to relieve headache is because of a misdiagnosis of TON headache. In the absence of trauma, TON rarely causes headaches. More commonly, patients with headaches involving the occipital region suffer from tension-type headaches (TTH) or, less commonly, occipital neuralgia. In conjunction with cervical epidural nerve block with steroids, the TTH type of headache does not respond to TON block but responds to treatment with antidepressant compounds such as amitriptyline. Therefore, pain management specialists should reconsider the diagnosis of TON headache in patients whose symptoms are consistent with TON headaches but fail to respond to TON blocks (2017).6
Any patient with sufficiently severe headache requiring nerve block as part of the treatment plan should undergo head magnetic resonance imaging to rule out unexpected intracranial pathology that may mimic the clinical presentation of a TON headache.6 In addition, radiography of the cervical spine should be considered to rule out congenital abnormalities such as Arnold-Chiari malformation which may be a hidden cause of the patient's occipital headache.3
8. Acknowledgement
We gratefully thank the Faculty of Medicine, as well as the authors of the pictures used in this mini-review. Picture credits go to the original authors, mentioned with reference numbers.
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
HBH: research, performed the analysis, manuscript editing
VAP, ATS: literature research, manuscript reviewing and revising
11. REFERENCES
- Voigt CL, Murphy MO. Occipital nerve blocks in the treatment of headaches: safety and efficacy. J Emerg Med. 2015;48(1):115-29. [PubMed] DOI: 1016/j.jemermed.2014.09.007
- Rana MV. Managing and treating headache of cervicogenic origin. Med Clin North Am. 2013;97(2):267-80. [PubMed] DOI: 1016/j.mcna.2012.11.003
- Waldman SD. Third Occipital Nerve Block. In: Waldman SD, editor. Atlas of Pain Management Injection Techniques. 4th ed. Kansas: Elsevier; 2017. p. 77–81.
- Moon DE. Ultrasound Guided Cervical Spine Injections: Greater Occipital Nerve, Third Occipital Nerve, Medial Branch, Facet Joint, Stellate Ganglion and Superior Cervical Sympathethic Ganglion Block. In: Karmakar MK, editor. Musculoskeletal Ultrasound for Regional Anaesthesia and Pain Medicine. 2nd ed. Hong Kong: CU Medicine; 2016. p. 655–670.
- Candido KD, Day M. Nerve Blocks of the Head and Neck. In: Rathmell JP, Wu CL, editors. Practical Management of Pain. 5th ed. Philadelphia; 2014. p. 697–715.
- Waldman SD. Greater and Lesser Occipital Nerve Block. In: Waldman SD, editor. Atlas of Interventional Pain Management [Internet]. 4th ed. Kansas: Elsevier Saunders; 2015. p. 24.