Yahya1, Hanik Badriyah Hidayati2, Alexander Tikara Sugondo3, Vania Ayu Puspamaniar4, Fajar Sena Firdausa5
Author affiliations:
Dialysis disequilibrium syndrome (DDS) is a rare syndrome that can occur in patients with severe azotemia undergoing an initial hemodialysis (HD) session. DDS is associated with a more rapid decrease in urea concentration in the blood than in the brain during dialysis. Although severe DDS is less common, the milder forms of DDS may be missed by doctors. A 53-year-old male patient had the main complaint of severe dizziness in the last 10 months accompanied by a sensation of a wobbling head and tinnitus in his right ear. The patient had previously been diagnosed with polycystic kidney disease in 2018 and underwent regular hemodialysis two times a week since June 2019. In the patient's neurological status, cerebellar examination was positive for left dysmetria, left positive past pointing, Romberg test (open eye) fell to the right, and Romberg test (closed eye) fell to the right. There was no nystagmus on the patient's neuro-ophthalmological examination. Patients with kidney failure are at risk of developing DDS, so that appropriate precautions are needed. Due to the variability of symptoms, DDS often goes undiagnosed. Thus, it is important to be aware of the risk factors for DDS so that preventive steps can be taken appropriately. Continuous case reporting will raise awareness and the opportunity for further research to improve outcome in severe cases of DDS.
Keywords: Dialysis; Disequilibrium; Dizziness; Polycystic Kidney.
Citation: Yahya, Hidayati HB, Sugondo AT, Puspamaniar VA, Firdausa FS. Dialysis disequilibrium syndrome: A case report. Anaesth. pain intensive care 2024;28(1):191−195; DOI: 10.35975/apic.v28i1.2388
Received: October 10, 2023; Reviewed: December 20, 2023; Accepted: January 02, 2024
Dialysis Disequilibrium Syndrome (DDS) is associated with a rapid decrease in urea concentration in blood as compared to that in the brain during dialysis. Currently, there are approximately 400,000 end-stage renal disease (ESRD) patients undergoing hemodialysis (HD) in the United States. Each patient receives dialysis at least three times a week (156 times per year), with a total of over 62 million dialysis sessions every year. DDS is a rare syndrome that can occur in patients with severe azotemia undergoing initial HD sessions.1 Despite the fact that hemodialysis has been a routine procedure for over 50 years, this syndrome is still not fully understood.2
The first description of DDS was reported in 1962 by Rosen et al.3 DDS can occur in any patient receiving hemodialysis at any time.2 The etiology of DDS is still debated. The onset of these complaints typically occurs toward the end of dialysis; and it is more common in pediatric or older patients, those with a smaller body mass index (indicative of decreased volume distribution), severe azotemia, and in patients with preexisting neurological conditions.4
Although severe DDS is less common, mild forms of DDS may be overlooked by physicians. Therefore, it is important to be aware of this condition, especially in high-risk groups, with the aim to prevent by early detection, to limit the potentially more serious consequences of DDS.5
A 53-year-old married male resident of Surabaya, Indonesia, presented to the Neurology Outpatient Clinic of Dr. Soetomo Hospital Surabaya, on August 27, 2020, with the chief complaint of vertigo. The patient had been experiencing this complaint since July 2019, with worsening over the past 10 months. The vertigo was accompanied by a sensation of head spinning and ringing in the right ear. The patient also frequently complained of being unable to ride a motorcycle due to frequent falls to the right. There were no complaints of ear fullness, hearing loss, facial asymmetry, seizures, or nausea and vomiting. The patient had a history of diabetes mellitus for 10 y and hypertension for 5 y. He also had a history of trauma to the right eye 35 y ago, rendering the right eye nonfunctional. In 2018, the patient was diagnosed with a kidney cyst and started regular hemodialysis twice a week in June 2019. There was no history of stroke, and no family members were known to have similar illnesses. The patient reported taking piracetam (often used for myoclonus, and to improve memory, attention, and learning).
On general examination, the patient had a blood pressure of 169/92 mmHg, while other vital signs and general status were within normal limits. Neurological examination revealed a Glasgow Coma Scale score of E4V5M6, negative meningeal signs, and no signs of neck stiffness. There was no facial or lingual palsy. Motor strength was 5/5 in both right and left extremities, and physiological reflexes were normal (biceps reflex +2/+2, triceps reflex +2/+2, knee reflex +2/+2, ankle reflex +2/+2). Pathological reflexes (Babinski and Chaddock) were negative. Cerebellar examination revealed dysmetria and disdiadokinesia, and the patient had difficulty with finger-to-nose testing and past-pointing. Romberg's test with eyes open or closed, resulted in falling to the right. Sensory and autonomic examinations were within normal limits. On neuro-ophthalmological examination, the patient had no light perception in the right eye and visual acuity of >2/60 in the left eye. The right eye had limited extraocular movements, making it difficult to evaluate, while the left eye exhibited unrestricted movement in all directions. The iris was regular, and the right pupil was difficult to evaluate, while the left pupil was round and measured 3 mm with a positive light reflex. No nystagmus was observed.
Laboratory tests revealed elevated blood urea nitrogen (BUN) and serum creatinine (SC) levels, measuring 70.0 mg/dL and 11.60 mg/dL, respectively.
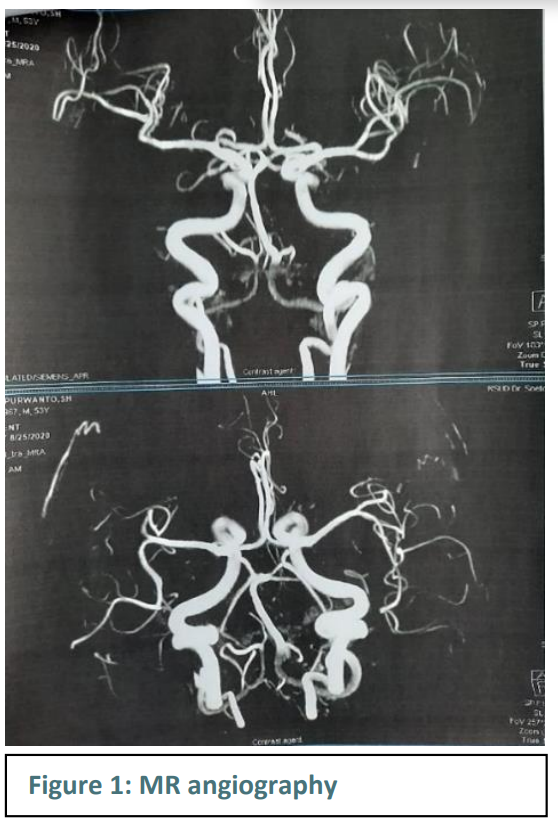
On MR angiography, the circle of Willis appeared patent, and no aneurysms or vascular malformations were detected (Figure 1).
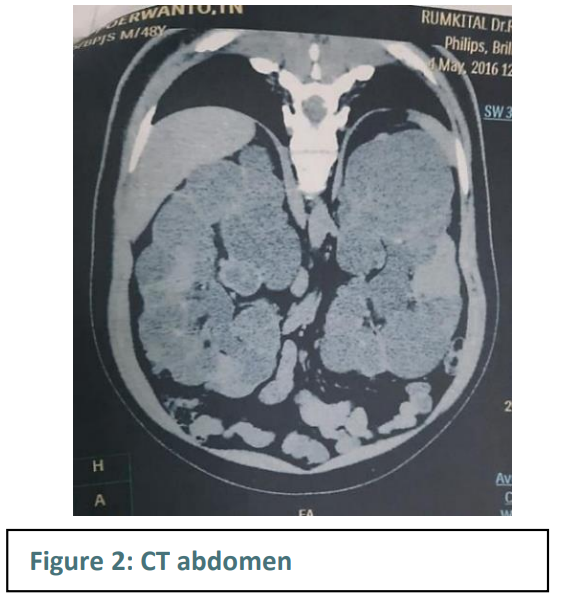
On abdominal CT (dated May 4, 2016), the right kidney was approximately 12.3 x 10.6 x 20 cm in size, with the pelvicalyceal system not clearly visualized, and multiple calcifications and cysts scattered throughout the right kidney. The left kidney measured approximately 14 x 10.5 x 22.4 cm, with the pelvicalyceal system not clearly visualized, and multiple calcifications and cysts scattered throughout the left kidney. The left and right ureters appeared normal (Figure 2).
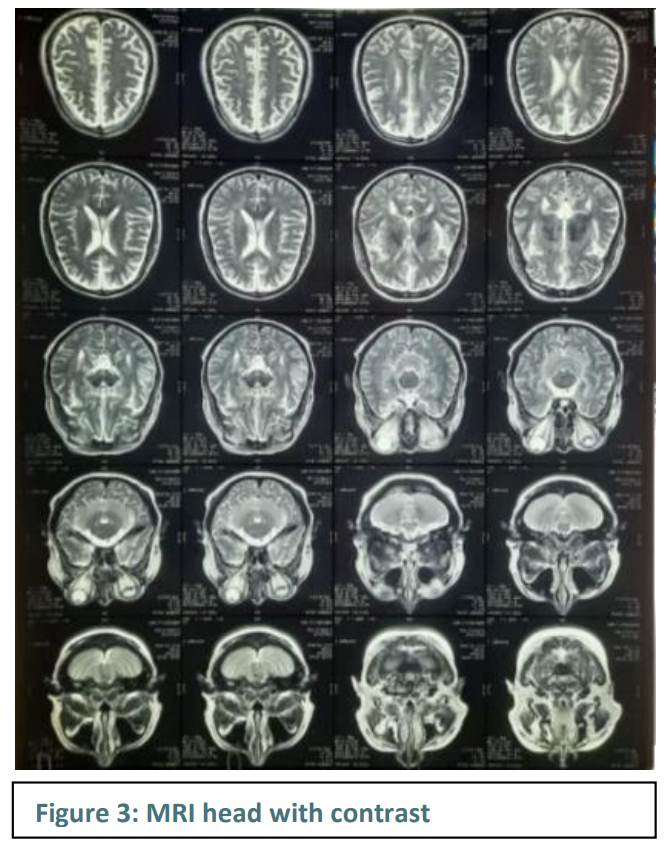
An MRI of the head with contrast showed no mass lesions in the brain parenchyma, no hypointense or hyperintense lesions in the cerebellum, and multiple small ischemic lesions in the right and left centrum semi-ovale and corona radiata. Additionally, sinusitis was observed in the maxillary, ethmoid, and sphenoid sinuses, with deviation of the nasal septum to the right.
The patient was prescribed oral therapy with vitamin B1 twice daily, vitamin B6 twice daily, mecobalamin 500 µg twice daily, and amlodipine 10 mg once daily. The patient was instructed on Cawthorne-Cooksey exercises. In follow-up appointments, the patient continued to receive outpatient care and was monitored at the Neuro-Otology Division of Dr. Soetomo Hospital, Surabaya. The patient's condition did not improve as the sensation of dizziness persisted.
Dialysis disequilibrium syndrome (DDS) is a collection of neurological manifestations that are a rare complication of dialysis.6,7,8 The incidence of DDS has not been clearly reported in the literature due to non-specific clinical manifestations and the difficulty of confirming the diagnosis. However, the incidence of this syndrome is estimated to have decreased due to the implementation of better prevention strategies.6,7
Dialysis disequilibrium syndrome (DDS) is a collection of neurological manifestations that is a rare complication of dialysis.6,7,8 The incidence rate of DDS is not well-defined in the literature because of its non-specific clinical manifestations and the difficulty in confirming the diagnosis.6,7 Nevertheless, it is believed that the incidence of this syndrome has decreased over time due to the implementation of improved prevention strategies.6,7
DDS can occur during and after dialysis, especially in patients undergoing dialysis for the first time.9,10 However, this syndrome can also occur in patients with chronic dialysis.6,11,12 It arises due to fluid shifts during dialysis and electrolyte and protein imbalances that lead to increased intracranial pressure due to cerebral edema, manifesting as neurological symptoms.6,7 In patients undergoing continuous renal replacement therapies (CRRT), where fluid shifts are more limited, this syndrome is less frequently reported.6,10
Risk factors for DDS include aggressive first-time hemodialysis, severe uremia, young age, neurological diseases (such as stroke, malignant hypertension, head trauma, or epilepsy), other medical conditions that cause cerebral edema (hyponatremia, hepatic encephalopathy), and other medical conditions that cause increased blood-brain barrier permeability (sepsis, meningitis, encephalitis, hemolytic uremic syndrome, vasculitis).6,7,12 The patient in this case report had chronic kidney disease and he had been undergoing regular hemodialysis since 2019. The risk factors identified in this patient included hypertension with a blood pressure of 169/92 mmHg and uremia with a blood urea nitrogen (BUN) level of 70.0 mg/dL.6
There are two pathophysiological theories of dialysis disequilibrium syndrome, namely the "reverse urea effect" theory and the intracerebral acidosis theory. While there is no definitive etiology for DDS, the "reverse urea effect" theory is more widely accepted.6,7,11,12
Patients with chronic uremia are in a state of hyperosmolar balance. In conditions, where urea in the blood, brain, and other tissues is in balance, there is no osmotic gradient. Small solutes like urea are rapidly cleared during dialysis, especially in cases of severe azotemia. Urea is a substance that can freely diffuse through cell membranes. The rapid clearance of urea from the serum during dialysis creates a transient osmotic gradient between the plasma and brain cells, leading to a fluid shift into brain cells, resulting in cerebral edema. Cerebral edema is exacerbated by the increased aquaporin channels in the brain and decreased urea channels in chronic kidney disease.6,7,11,13 The theory of cerebral acidosis is based on various studies showing a decrease in intracellular pH in brain cells with carbon dioxide retention in patients after dialysis initiation.6 The decrease in pH causes sodium and potassium to become osmotically active. The adaptive retention of organic osmolytes in the brain, such as glutamine, glutamate, taurine, and myoinositol, results in decreased pH and increased brain osmolality, leading to cerebral edema.6,13
The clinical manifestation of DDS in our patient was vertigo. Symptoms that occur in DDS can vary from mild symptoms such as headaches, vertigo, muscle cramps, tremors, nausea, blurred vision to severe symptoms such as coma, cerebral edema, and death.7,12,14 DDS symptoms generally occur immediately after dialysis begins and disappear within a few hours. Some symptoms like vertigo and muscle cramps have a longer onset. DDS can also manifest as increased intraocular pressure. In severe cases, symptoms can progress to seizures, somnolence, stupor, or coma, and even death. Death in DDS can be caused by central herniation.12,14
DDS is a clinical diagnosis. There are no specific laboratory tests or imaging studies for confirming the diagnosis.6,7,11 In the case of this patient, laboratory tests and head imaging with MRI/Spectro with contrast were performed.
Differential diagnoses for DDS include uremia, stroke, subdural hemorrhage, metabolic disorders (hyponatremia, hypoglycemia), drug-induced encephalopathy, and infections (meningitis, encephalitis).11,12 Electroencephalography has been studied to assist in diagnosis but has limited potential. MRI imaging, especially with diffusion-weighted imaging (DWI) that can evaluate brain water content, can aid in diagnosis.11,12
The management of DDS primarily focuses on prevention rather than treatment. DDS prevention includes increasing dialysate osmolality, shorter but more frequent hemodialysis sessions, lower blood flow rates through the dialyzer, gradual urea clearance to prevent osmotic gradients, and the administration of osmotically active compounds.6,7
In patients who have developed symptoms, management options to consider include reducing intracranial pressure with IV mannitol or hypertonic saline. However, the use of these therapies is still limited and yields varied outcomes.7,11,15 Patients need to be monitored, and if symptoms worsen, discontinuation of the dialysis session is recommended.11 The management given to this patient is nonspecific, consisting of vitamin B1, B6, mecobalamin, and Cawthorne-Cooksey exercises to reduce vertigo symptoms. The patient is also prescribed amlodipine to control hypertension, which is one of the risk factors.
Most cases of DDS are mild and self-limited, resulting in a favorable prognosis. Therefore, dialysis does not need to be discontinued in most cases. However, in severe cases, the prognosis can be very poor, with symptoms progressing to seizures, somnolence, stupor, or coma, and even death.6,7,12
Patients with kidney failure are at risk of developing dialysis disequilibrium syndrome as a consequence of hemodialysis, necessitating appropriate preventive measures. The exact underlying mechanisms are still debated. Due to the variability in symptoms, it often goes undiagnosed. Therefore, it is crucial to be vigilant about dialysis disequilibrium syndrome risk factors so that preventive measures can be implemented effectively. Continuous case reporting will increase awareness and provide further research opportunities to improve outcomes in severe cases.
5. Conflict of interests
The authors declare no conflict of interests.
6. Ethical considerations
Written consent of the patient was obtained to publish his data as an academic service. Ethical approval of the institutional ethical committee was granted.
7. Authors’ contribution
Y, HBH: research, performed the analysis, manuscript editing
ATS, VAP: literature research, manuscript reviewing and revising
Author affiliations:
- Yahya, Teaching Staff, Neurology Department, Faculty of Medicine Airlangga University – RSUD Dr. Soetomo, Surabaya, Jawa, Indonesia; E-mail: dr.yahyaassegaff@gmail.com
- Hanik Badriyah, Staff of Neurology Department, Faculty of Medicine Airlangga University – RSUD Dr. Soetomo, Surabaya, Jawa, Indonesia; E-mail: hanikhidayati@fk.unair.ac.id
- Alexander Tikara Sugondo, Student, Faculty of Medicine, Airlangga University – RSUD Dr. Soetomo, Surabaya, Jawa, Indonesia; E-mail: alexandertikara37@gmail.com
- Vania Ayu Puspamaniar, General Practitioner Petrokimia Gresik Hospital, Gresik, Indonesia; E-mail: puspamaniar06@gmail.com
- Fajar Sena Firdausa, Education Staff, Faculty of Medicine, Airlangga University, Surabaya, Jawa, Indonesia; E-mail: fajarbore2309@gmail.com
ABSTRACT
Dialysis disequilibrium syndrome (DDS) is a rare syndrome that can occur in patients with severe azotemia undergoing an initial hemodialysis (HD) session. DDS is associated with a more rapid decrease in urea concentration in the blood than in the brain during dialysis. Although severe DDS is less common, the milder forms of DDS may be missed by doctors. A 53-year-old male patient had the main complaint of severe dizziness in the last 10 months accompanied by a sensation of a wobbling head and tinnitus in his right ear. The patient had previously been diagnosed with polycystic kidney disease in 2018 and underwent regular hemodialysis two times a week since June 2019. In the patient's neurological status, cerebellar examination was positive for left dysmetria, left positive past pointing, Romberg test (open eye) fell to the right, and Romberg test (closed eye) fell to the right. There was no nystagmus on the patient's neuro-ophthalmological examination. Patients with kidney failure are at risk of developing DDS, so that appropriate precautions are needed. Due to the variability of symptoms, DDS often goes undiagnosed. Thus, it is important to be aware of the risk factors for DDS so that preventive steps can be taken appropriately. Continuous case reporting will raise awareness and the opportunity for further research to improve outcome in severe cases of DDS.
Keywords: Dialysis; Disequilibrium; Dizziness; Polycystic Kidney.
Citation: Yahya, Hidayati HB, Sugondo AT, Puspamaniar VA, Firdausa FS. Dialysis disequilibrium syndrome: A case report. Anaesth. pain intensive care 2024;28(1):191−195; DOI: 10.35975/apic.v28i1.2388
Received: October 10, 2023; Reviewed: December 20, 2023; Accepted: January 02, 2024
1. INTRODUCTION
Dialysis Disequilibrium Syndrome (DDS) is associated with a rapid decrease in urea concentration in blood as compared to that in the brain during dialysis. Currently, there are approximately 400,000 end-stage renal disease (ESRD) patients undergoing hemodialysis (HD) in the United States. Each patient receives dialysis at least three times a week (156 times per year), with a total of over 62 million dialysis sessions every year. DDS is a rare syndrome that can occur in patients with severe azotemia undergoing initial HD sessions.1 Despite the fact that hemodialysis has been a routine procedure for over 50 years, this syndrome is still not fully understood.2
The first description of DDS was reported in 1962 by Rosen et al.3 DDS can occur in any patient receiving hemodialysis at any time.2 The etiology of DDS is still debated. The onset of these complaints typically occurs toward the end of dialysis; and it is more common in pediatric or older patients, those with a smaller body mass index (indicative of decreased volume distribution), severe azotemia, and in patients with preexisting neurological conditions.4
Although severe DDS is less common, mild forms of DDS may be overlooked by physicians. Therefore, it is important to be aware of this condition, especially in high-risk groups, with the aim to prevent by early detection, to limit the potentially more serious consequences of DDS.5
2. CASE REPORT
A 53-year-old married male resident of Surabaya, Indonesia, presented to the Neurology Outpatient Clinic of Dr. Soetomo Hospital Surabaya, on August 27, 2020, with the chief complaint of vertigo. The patient had been experiencing this complaint since July 2019, with worsening over the past 10 months. The vertigo was accompanied by a sensation of head spinning and ringing in the right ear. The patient also frequently complained of being unable to ride a motorcycle due to frequent falls to the right. There were no complaints of ear fullness, hearing loss, facial asymmetry, seizures, or nausea and vomiting. The patient had a history of diabetes mellitus for 10 y and hypertension for 5 y. He also had a history of trauma to the right eye 35 y ago, rendering the right eye nonfunctional. In 2018, the patient was diagnosed with a kidney cyst and started regular hemodialysis twice a week in June 2019. There was no history of stroke, and no family members were known to have similar illnesses. The patient reported taking piracetam (often used for myoclonus, and to improve memory, attention, and learning).
On general examination, the patient had a blood pressure of 169/92 mmHg, while other vital signs and general status were within normal limits. Neurological examination revealed a Glasgow Coma Scale score of E4V5M6, negative meningeal signs, and no signs of neck stiffness. There was no facial or lingual palsy. Motor strength was 5/5 in both right and left extremities, and physiological reflexes were normal (biceps reflex +2/+2, triceps reflex +2/+2, knee reflex +2/+2, ankle reflex +2/+2). Pathological reflexes (Babinski and Chaddock) were negative. Cerebellar examination revealed dysmetria and disdiadokinesia, and the patient had difficulty with finger-to-nose testing and past-pointing. Romberg's test with eyes open or closed, resulted in falling to the right. Sensory and autonomic examinations were within normal limits. On neuro-ophthalmological examination, the patient had no light perception in the right eye and visual acuity of >2/60 in the left eye. The right eye had limited extraocular movements, making it difficult to evaluate, while the left eye exhibited unrestricted movement in all directions. The iris was regular, and the right pupil was difficult to evaluate, while the left pupil was round and measured 3 mm with a positive light reflex. No nystagmus was observed.
Laboratory tests revealed elevated blood urea nitrogen (BUN) and serum creatinine (SC) levels, measuring 70.0 mg/dL and 11.60 mg/dL, respectively.
On MR angiography, the circle of Willis appeared patent, and no aneurysms or vascular malformations were detected (Figure 1).
On abdominal CT (dated May 4, 2016), the right kidney was approximately 12.3 x 10.6 x 20 cm in size, with the pelvicalyceal system not clearly visualized, and multiple calcifications and cysts scattered throughout the right kidney. The left kidney measured approximately 14 x 10.5 x 22.4 cm, with the pelvicalyceal system not clearly visualized, and multiple calcifications and cysts scattered throughout the left kidney. The left and right ureters appeared normal (Figure 2).
An MRI of the head with contrast showed no mass lesions in the brain parenchyma, no hypointense or hyperintense lesions in the cerebellum, and multiple small ischemic lesions in the right and left centrum semi-ovale and corona radiata. Additionally, sinusitis was observed in the maxillary, ethmoid, and sphenoid sinuses, with deviation of the nasal septum to the right.
The patient was prescribed oral therapy with vitamin B1 twice daily, vitamin B6 twice daily, mecobalamin 500 µg twice daily, and amlodipine 10 mg once daily. The patient was instructed on Cawthorne-Cooksey exercises. In follow-up appointments, the patient continued to receive outpatient care and was monitored at the Neuro-Otology Division of Dr. Soetomo Hospital, Surabaya. The patient's condition did not improve as the sensation of dizziness persisted.
3. DISCUSSION
Dialysis disequilibrium syndrome (DDS) is a collection of neurological manifestations that are a rare complication of dialysis.6,7,8 The incidence of DDS has not been clearly reported in the literature due to non-specific clinical manifestations and the difficulty of confirming the diagnosis. However, the incidence of this syndrome is estimated to have decreased due to the implementation of better prevention strategies.6,7
Dialysis disequilibrium syndrome (DDS) is a collection of neurological manifestations that is a rare complication of dialysis.6,7,8 The incidence rate of DDS is not well-defined in the literature because of its non-specific clinical manifestations and the difficulty in confirming the diagnosis.6,7 Nevertheless, it is believed that the incidence of this syndrome has decreased over time due to the implementation of improved prevention strategies.6,7
DDS can occur during and after dialysis, especially in patients undergoing dialysis for the first time.9,10 However, this syndrome can also occur in patients with chronic dialysis.6,11,12 It arises due to fluid shifts during dialysis and electrolyte and protein imbalances that lead to increased intracranial pressure due to cerebral edema, manifesting as neurological symptoms.6,7 In patients undergoing continuous renal replacement therapies (CRRT), where fluid shifts are more limited, this syndrome is less frequently reported.6,10
Risk factors for DDS include aggressive first-time hemodialysis, severe uremia, young age, neurological diseases (such as stroke, malignant hypertension, head trauma, or epilepsy), other medical conditions that cause cerebral edema (hyponatremia, hepatic encephalopathy), and other medical conditions that cause increased blood-brain barrier permeability (sepsis, meningitis, encephalitis, hemolytic uremic syndrome, vasculitis).6,7,12 The patient in this case report had chronic kidney disease and he had been undergoing regular hemodialysis since 2019. The risk factors identified in this patient included hypertension with a blood pressure of 169/92 mmHg and uremia with a blood urea nitrogen (BUN) level of 70.0 mg/dL.6
There are two pathophysiological theories of dialysis disequilibrium syndrome, namely the "reverse urea effect" theory and the intracerebral acidosis theory. While there is no definitive etiology for DDS, the "reverse urea effect" theory is more widely accepted.6,7,11,12
Patients with chronic uremia are in a state of hyperosmolar balance. In conditions, where urea in the blood, brain, and other tissues is in balance, there is no osmotic gradient. Small solutes like urea are rapidly cleared during dialysis, especially in cases of severe azotemia. Urea is a substance that can freely diffuse through cell membranes. The rapid clearance of urea from the serum during dialysis creates a transient osmotic gradient between the plasma and brain cells, leading to a fluid shift into brain cells, resulting in cerebral edema. Cerebral edema is exacerbated by the increased aquaporin channels in the brain and decreased urea channels in chronic kidney disease.6,7,11,13 The theory of cerebral acidosis is based on various studies showing a decrease in intracellular pH in brain cells with carbon dioxide retention in patients after dialysis initiation.6 The decrease in pH causes sodium and potassium to become osmotically active. The adaptive retention of organic osmolytes in the brain, such as glutamine, glutamate, taurine, and myoinositol, results in decreased pH and increased brain osmolality, leading to cerebral edema.6,13
The clinical manifestation of DDS in our patient was vertigo. Symptoms that occur in DDS can vary from mild symptoms such as headaches, vertigo, muscle cramps, tremors, nausea, blurred vision to severe symptoms such as coma, cerebral edema, and death.7,12,14 DDS symptoms generally occur immediately after dialysis begins and disappear within a few hours. Some symptoms like vertigo and muscle cramps have a longer onset. DDS can also manifest as increased intraocular pressure. In severe cases, symptoms can progress to seizures, somnolence, stupor, or coma, and even death. Death in DDS can be caused by central herniation.12,14
DDS is a clinical diagnosis. There are no specific laboratory tests or imaging studies for confirming the diagnosis.6,7,11 In the case of this patient, laboratory tests and head imaging with MRI/Spectro with contrast were performed.
Differential diagnoses for DDS include uremia, stroke, subdural hemorrhage, metabolic disorders (hyponatremia, hypoglycemia), drug-induced encephalopathy, and infections (meningitis, encephalitis).11,12 Electroencephalography has been studied to assist in diagnosis but has limited potential. MRI imaging, especially with diffusion-weighted imaging (DWI) that can evaluate brain water content, can aid in diagnosis.11,12
The management of DDS primarily focuses on prevention rather than treatment. DDS prevention includes increasing dialysate osmolality, shorter but more frequent hemodialysis sessions, lower blood flow rates through the dialyzer, gradual urea clearance to prevent osmotic gradients, and the administration of osmotically active compounds.6,7
In patients who have developed symptoms, management options to consider include reducing intracranial pressure with IV mannitol or hypertonic saline. However, the use of these therapies is still limited and yields varied outcomes.7,11,15 Patients need to be monitored, and if symptoms worsen, discontinuation of the dialysis session is recommended.11 The management given to this patient is nonspecific, consisting of vitamin B1, B6, mecobalamin, and Cawthorne-Cooksey exercises to reduce vertigo symptoms. The patient is also prescribed amlodipine to control hypertension, which is one of the risk factors.
Most cases of DDS are mild and self-limited, resulting in a favorable prognosis. Therefore, dialysis does not need to be discontinued in most cases. However, in severe cases, the prognosis can be very poor, with symptoms progressing to seizures, somnolence, stupor, or coma, and even death.6,7,12
4. CONCLUSION
Patients with kidney failure are at risk of developing dialysis disequilibrium syndrome as a consequence of hemodialysis, necessitating appropriate preventive measures. The exact underlying mechanisms are still debated. Due to the variability in symptoms, it often goes undiagnosed. Therefore, it is crucial to be vigilant about dialysis disequilibrium syndrome risk factors so that preventive measures can be implemented effectively. Continuous case reporting will increase awareness and provide further research opportunities to improve outcomes in severe cases.
5. Conflict of interests
The authors declare no conflict of interests.
6. Ethical considerations
Written consent of the patient was obtained to publish his data as an academic service. Ethical approval of the institutional ethical committee was granted.
7. Authors’ contribution
Y, HBH: research, performed the analysis, manuscript editing
ATS, VAP: literature research, manuscript reviewing and revising
8. REFERENCES
- Saha M, Allon M. Diagnosis, treatment, and prevention of hemodialysis emergencies. Clin J Am Soc Nephrol. 2017;12(2):357–69. [PubMed] DOI: 2215/CJN.05260516
- Zepeda-Orozco D, Quigley R. Dialysis disequilibrium syndrome. Pediatr Nephrol. 2012;27(12):2205–11. [PubMed] DOI: 1007/s00467-012-2199-4
- Rosen SM, O’Connor K, Shaldon S. Haemodialysis Disequilibrium. Br Med J. 1964;2(5410):672–5. [PubMed] DOI: 1136/bmj.2.5410.672
- Donegan D, Kashani K. Dialysis Disequilibrium Syndrome: A Swell Diagnosis? J Med Cases. 2014;5(8):437–40. DOI: 14740/jmc1847w
- Aziz F, Dutta S, Zaeem M. Dialysis Disequilibrium Syndrome: A Case Report & Concise Review. Greener J Med Sci. 2013;3(6):207–10. DOI: 15580/gjms.2013.6.061213671
- Bhandari B, Komanduri S. Dialysis Disequilibrium Syndrome. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559018/
- George C, Penumalee S, Minter D. Dialysis Disequilibrium Syndrome. Am J Med Case Rep. 2018;6(4):68-71. [FreeFullText]
- Arieff AI. Dialysis disequilibrium syndrome: current concepts on pathogenesis and prevention. Kidney Int. 1994;45(3):629-635. [PubMed] DOI: 1038/ki.1994.84
- Kennedy AC, Linton AL, Eaton JC. Urea levels in cerebrospinal fluid after haemodialysis. Lancet. 1962;1(7226):410-1. [PubMed] DOI: 1016/s0140-6736(62)91365-x
- Tuchman S, Khademian ZP, Mistry K. Dialysis disequilibrium syndrome occurring during continuous renal replacement therapy. Clin Kidney J. 2013;6(5):526-9. [PubMed] DOI: 1093/ckj/sft087
- Adapa S, Konala VM, Aeddula NR, Gayam V, Naramala S. Dialysis Disequilibrium Syndrome: Rare Serious Complication of Hemodialysis and Effective Management. Cureus. 2019;11(6):e5000. [PubMed] DOI: 7759/cureus.5000
- Mistry K. Dialysis disequilibrium syndrome prevention and management. Int J Nephrol Renovasc Dis. 2019;12:69–77. [PubMed] DOI: 2147/IJNRD.S165925
- Silver SM, Sterns RH, Halperin ML. Brain swelling after dialysis: old urea or new osmoles? Am J Kidney Dis. 1996;28(1):1-13. [PubMed] DOI: 1016/s0272-6386(96)90124-9
- Sitprija V, Holmes JH. Preliminary observations on the change in intracranial pressure and intraocular pressure during hemodialysis. Trans Am Soc Artif Intern Organs. 1962;8:300-8. [PubMed] DOI: 1097/00002480-196204000-00061
- Doorenbos CJ, Bosma RJ, Lamberts PJ. Use of urea containing dialysate to avoid disequilibrium syndrome, enabling intensive dialysis treatment of a diabetic patient with renal failure and severe metformin induced lactic acidosis. Nephrol Dial Transplant. 2001;16(6):1303-4. [PubMed] DOI: 1093/ndt/16.6.1303