Nazmy Edward Seif1, Manar Mahmoud El-Kholy2, Ashgan Raouf Ali3, Moustafa Mohamed Zalat4, Mohamed Elshazly5
Author affiliations:
Background &objective: Transmuscular quadratus lumborum plane block (QLPB), paravertebral plane block (PVPB), and erector spinae plane block (ESPB) are three regional anesthesia techniques for management of perioperative pain for surgical procedures on the trunk, including thorax and abdomen. We compared the effectiveness of PVPB, QLPB type III (QL3), and ESPB for perioperative analgesia during radical cystectomy performed for bladder cancer.
Methodology: This randomized double-blind trial was performed on 120 patients, aged above 18 years, undergoing radical cystectomy under general anesthesia. Individuals were randomly divided into 3 equal groups: ESPB, PVPB, and QLPB. Blocks were performed under ultrasound guidance preoperatively on each side with 30 ml of 0.25% bupivacaine. Time to perform block and time to the first dose of morphine postoperatively, were noted. Intra-operative hemodynamic data, including MAP and heart rate (HR) were noted every 10 min for an hour, and then at 30 min intervals. Postoperatively, MAP and HR were recorded at 0, 2, 6, 12 and 24 hours. The connection between qualitative factors was investigated using the chi-square test and Fisher's exact test. For the purpose of comparing the groups, one-way ANOVA and the Bonferroni correction were used. A two-tailed P value < 0.05 was considered significant.
Results: Time to perform block was substantially reduced in ESPB and QL3 groups compared to PVPB group. Time to the first dose of morphine was substantially delayed in the PVPB group than ESPB and QL3 groups. Total 24 h morphine consumption was substantially lower in the PVPB group than ESPB and QL3 groups. Postoperative visual analog scale measurements were substantially lower at 15 min, 30 min, and 12 h in the PVPB group than ESPB and QL3 groups and at 6 h in the ESPB and QL3 groups than in PVPB group. Postoperative mean arterial blood pressure and heart rate measurements were substantially reduced at 0 and 12 h in the PVPB group than in ESPB and QL3 groups and at 6 h in the ESPB and QL3 groups than in PVPB group.
Conclusions: The ultrasound guided paravertebral plane block was superior to quadratus lumborum plane block type III and erector spinae plane block in providing more effective analgesia but with higher time to perform block.
Abbreviations: ESPB- Erector Spinae Plane Block; PVPB- Paravertebral Plane Block; QLPB- Quadratus Lumborum Plane Block; QL3- Quadratus Lumborum Plane Block Type III
Keywords: Paravertebral Plane Block; Quadratus Lumborum Plane Block; Erector Spinae Plane Block; Ultrasound; Radical Cystectomy
Citation: Seif NE, El-Kholy MM, Ali AR, Zalat MM, Elshazly M. Three ultrasound guided plane blocks for perioperative analgesia in patients undergoing radical cystectomy: a randomized clinical trial. Anaesth. pain intensive care 2024;28(1):85-91; DOI: 10.35975/apic.v28i1.2381
Received: September 28, 2023; Reviewed: October 31, 2023; Accepted: October 31, 2023
Of all bladder cancers, urothelial carcinoma of the bladder (UCB) makes up around 90% of cases. Based on data for the year 2019 provided by the American Cancer Society,1 UCB is the cancer with the 5th highest incidence overall and the 4th most prevalent cancer in men. The patient requires 5 to 10 days to recuperate from a radical cystectomy (RC), a major procedure that causes severe postoperative discomfort and diminished function.2-4
The standard treatment for post-cystectomy pain is opioid analgesics. However, opioids often have negative side effects including postoperative ileus, nausea and vomiting, prolonged sedation, and respiratory depression.5
Regional blocks are one of the primary techniques employed for Enhanced Recovery After Surgery (ERAS) with the aim to reduce postoperative problems, such as postoperative pain and hospital stay, and are a component of multimodal analgesia. Additionally, they outperform systemic opioids in lowering the possibility of postoperative delirium, particularly in elderly individuals.6
The application of ultrasound in regional techniques offers important advantages over traditional approaches like nerve stimulation and reducing resistance, according to an expanding amount of research and advances in technology. We compared the efficacy of three different spinal blocks: the erector spinae plane block (ESPB), transmuscular quadratus lumborum plane block (QLPB), and thoracic paravertebral plane block (PVPB).
This randomized double-blind study was performed on 120 patients, aged above 18 years, of both sexes, American Society of Anesthesiologists (ASA) II-III, undergoing radical cystectomy under general anesthesia. Following permission from the Cairo University Hospitals' Ethics Committee and registration with clinicaltrials.gov (ID: NCT05278598), the research was conducted from April 2022 to January 2023. All patients provided written informed approval.
Criteria for the exclusion were; uncooperative individuals, contraindications for peripheral regional anesthesia blocks, individuals taking opioids for persistent pain pre-operatively, choice of spinal anesthesia or any other regional anesthesia, patients at risk for developing coagulopathy (defined as partial thromboplastin time (PTT) > 40 sec, international normalized ratio (INR) more than 1.4, platelet count less than 100x109, anatomical abnormalities or infections at the site of injection.
Participants were assigned at random to one of the research groups using a computer-generated table. The alphanumeric codes on the sealed envelopes were used to disguise the randomization process. Unrelated to the randomization process, the patient identities were affixed to the opened envelopes and safeguarded. The group assignment was concealed from both the participants and the data assessor. Based on the kind of perioperative analgesia used, the participants were split into 3 groups equally: Group PVPB, ESPB, or QLPB.
As soon as the patient entered the operating room, perioperative monitoring was applied. This included a continuous electrocardiogram, finger-based pulse oximetry, and non-invasive arterial blood pressure monitoring (using a GE-Datex Ohmeda multiparameter monitor).
The group assignment was revealed after the envelopes were opened. Prior to the introduction of general anesthesia, ultrasound-guided blocks were carried out under aseptic conditions. Inj midazolam 1 mg was injected intravenously.
Each block was carried out prior to surgery with 5 cm of 1% lidocaine infiltration at the location of the needle injection on each side.
In all groups, every patient got 30 mL of 0.25% bupivacaine on both sides. A 22-G spinal needle was used for all blocks, and a Siemens Acuson x300 3-5 MHz US machine was used, which was housed under a sterile cover.
2.1. Erector spinae plane block
The block was administered bilaterally at the level of T9 after the patient had been directed laterally. A curvilinear high-frequency U-S transducer was positioned 3 cm laterally to the T9 spinous process, in which a hyper-echoic shadow of the transverse process (TP) and erector spinae was established. Next, the needle was inserted into the TP, traversing the entire group of muscles.
2.2. Thoracic paravertebral plane block
A curved high-frequency US transducer was utilized to view the T10 paravertebral region in the paramedian sagittal plane on both sides, in sitting position; an injection into this area would disseminate to many nearby dermatomes. The spinal needle was put in-plane with respect to the US probe and moved gradually from lateral to medial until the apex of the paravertebral space was reached at the tip. The pleura was displaced anteriorly and it served as the completion of the block.
2.3. Quadratus lumborum plane block
In order to find the triple abdominal muscle layers, the participant was set up laterally on each side. A curved high-frequency US transducer was then placed horizontally in the anterior axillary line, midway between the subcostal border and the iliac crest. With the psoas major muscle positioned anteriorly, the erector spinae muscle posteriorly, and the quadratus lumborum muscle attached to the apex of the TP, this is a pattern that is well known as a shamrock with 3 leaves.7
Fentanyl 1.5 μg/kg, to a maximum dosage of 200 μg, propofol 2 mg/kg and atracurium 0.5 mg/kg were used to induce general anesthesia and to aid tracheal intubation. A urinary catheter was inserted. For the sake of preserving normocapnia, volume-controlled ventilation was modified. Atracurium top-ups at 0.1 mg/kg every 30 min and 1–1.5% isoflurane in a 50/50 combination of oxygen and air were used to maintain anesthesia.
Following skin closure, inhalational anesthesia was stopped, and once the patient's spontaneous breathing had returned, atropine 0.02 mg/kg and neostigmine 0.05 mg/kg were given intravenously to reverse muscular relaxation. Fifteen minutes after extubation, a VAS was used to measure pain, with 0 representing no pain and 10 representing the most severe pain. Rescue analgesia in the form of morphine 0.1 mg/kg was administered if the score reached 4/10. If the score remained over 4 following 30 min after the first dosage, a further administration of morphine 0.1 mg/kg was provided in the PACU. Hemodynamic parameters were recorded intra-operatively and postoperatively.
The primary outcome was to estimate cumulative 24-hour morphine consumption. The secondary outcomes were measurement of postoperative pain intensity, time to first postoperative analgesic request, block procedure time and any complications.
2.4. Sample size calculation
Using a G power program on the level of mean morphine consumption in the first 24 h postoperative using one-way ANOVA because it was the main outcome variable in the present study. A previous study has reported that the mean (SD) first 24 h of morphine consumed in the ESPB group versus TAP block in radical cystectomy was 3.2571(0.78) and 5.6571(1.55), respectively [8]. In a pilot study on 5 patients, the morphine consumption in the first 24 h was 4.2(1.8) mg. With a minimum of thirty-five participants per group, a study's power was predicted to be 95% and its alpha error to be 0.05. In order to account for potential dropouts, this number was raised to forty participants in each group.
2.5. Statistical analysis
Software such as Medcalc and SPSS v15 (Chicago, IL) were used for statistical analysis. The mean and standard deviation (SD) of the quantitative parameters were reported, and they were contrasted for the same group using a paired Student's t-test. Frequency and percentages (%) were used to illustrate qualitative parameters. The connection between qualitative factors was investigated using the chi-square test and Fisher's exact test. For the purpose of comparing the groups, one-way ANOVA and the Bonferroni correction were used. A two-tailed P value < 0.05 was considered significant.
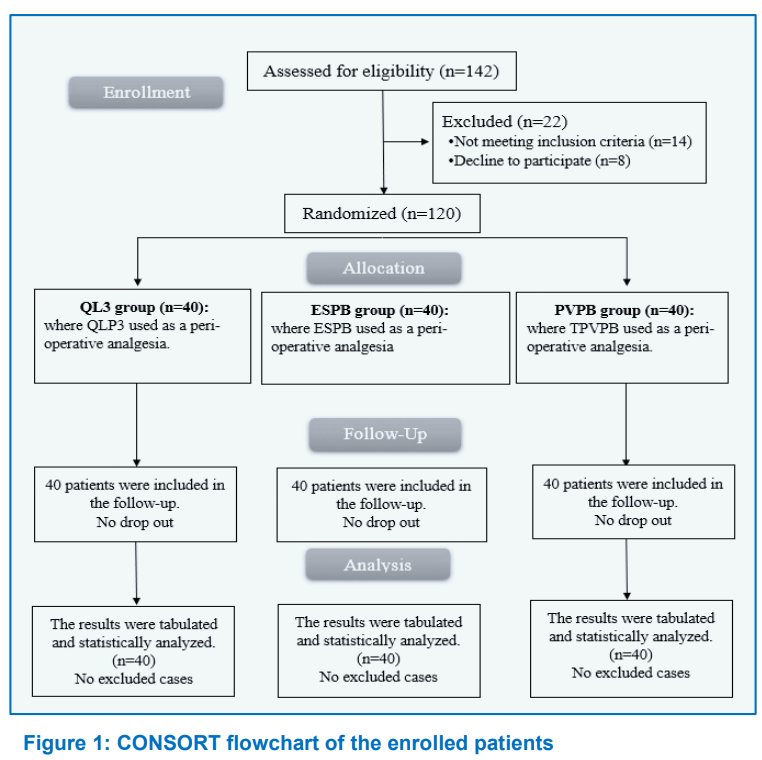
For this research 142 participants were screened; 14 were found to be ineligible, and 8 individuals declined to take part. The other 120 individuals were divided into 3 groups, each with 40 participants. All of the participants followed up and statistically analyzed (Figure 1).
The demographic data of the participants, including age, sex, BMI, ASA physical status, and surgeries duration were equivalent among the three groups (Table 1).
The time to execute the block, time to administer the initial dose of morphine, and total 24-hour morphine intake were not statistically different from each other in the ESPB group and QL3 group, and in both of these groups time to conduct the block was considerably shorter than that of the PVPB group. In comparison to ESPB group and QL3 group, time to the first dosage of morphine was considerably delayed in PVPB group. The PVPB group consumed much less morphine overall throughout the course of a 24-hour period than the ESPB group and QL3 group. Comparing the PVPB group to the ESPB group and the QL3 group, complications were much more common (Table 2).
Postoperative VAS measurements at 15 min, 30 min, and 12 h were insignificantly different among the ESPB group and QL3 group. They were substantially reduced in the PVPB group than the ESPB group and QL3 group.
Postoperative VAS measurements at 6 h were insignificantly different among the ESPB group and QL3 group and were substantially greater in the PVPB group than the ESPB group and QL3 group (Table 3).
Intraoperative mean blood pressure measurements were insignificantly different in all measurements among the three groups (Table 4).
Intraoperative heart rate (HR) measurements were insignificantly different among the three groups (Table 4).
Postoperative MAP and HR measurements at 0 and 12 h were significantly lower in the PVPB group than ESPB group and QL3group. They were significantly higher in the PVPB group than the ESPB group and QL3group at 6 h (Table 6).
The typical approach to post-cystectomy management of pain is opioid analgesics.5 However, opioids often have negative side effects including postoperative ileus, severe sedation, and depressed breathing.6
In the present study, the time to execute the block was substantially reduced in the ESPB group and QL3 group compared to the PVPB group. Our findings contradict the results of Thomas et al.9 study, which showed that the time to perform the block was insignificantly different between the ESPB and the PVPB groups. The contrary result was observed by Abd Ellatif and Abdelnaby,10 who stated that the time to execute block was significantly reduced in the ESPB group compared to the QLPB group.
In our study, intraoperative mean blood pressure measurements and HR were insignificantly different at all measurements among the three groups, denoting that all blocks were efficiently doing their effect with good hypnosis and muscle relaxation. In agreement to our results, Various researchers reported insignificant statistical differences in the MAP and HR intraoperatively between both groups. Also, Mohamed et al. reported insignificant statistical differences in the me MAP and HR intraoperatively between the ESPB and QLPB groups. 9,11,12,13
According to our results, postoperative VAS measurements at 15 min, 30 min, and 12 h were significantly reduced in the PVPB group than in the ESPB group and QL3 group. They were significantly greater in the PVPB group than the ESPB group and QL3 group at 6 h postoperatively, with insignificant variations across the 3 groups at 2 and 24 h. Postoperative VAS measurements always were insignificantly different between the ESPB group and QL3 group. Our findings disagreed with Elewa et al.,13 who reported that concerning postoperative pain, the ESPB had an extended analgesic effect than the PVB, as indicated by the significant decrease in the VAS score at 8 h and 12 h after the operation. This difference could be due to the different surgical procedures. Our findings agree with Abd Ellatif and Abdelnaby et al. the VAS score was insignificantly different between QLPB and ESPB groups at any time.10
Following our results, Xiong et al. results showed that for patients having thoracic and breast surgeries, PVB substantially decreased the postoperative pain ratings at rest at 0-1, 4-6, and 24 h in comparison to ESPB.14 Moreover, Mohamed et al. found that the postoperative VAS measurements were insignificantly different between ESPB and QL3 groups.12
The previous changes detected in pain perception were reflected in the postoperative hemodynamic changes (MAP and HR). The postoperative MAP and HR measurements at 0 and 12 h were significantly lower in the PVPB group than the ESPB group and QL3group, due to the good analgesia of PVPB as mentioned before. At the same time, they were significantly higher in the PVPB group than the ESPB group and QL3group at 6h, caused by the elimination of the LA effect and the need for morphine dose. There was an insignificant difference between the groups at 2 and 24 h. Postoperative MAP measurements were insignificantly different between the ESPB group and QL3 group. Supporting our results, Elkotory et al. reported insignificant statistical differences in the postoperative MAP measurements between QLB and ESB groups.11 In contrast to our results, Mohamed et al. showed that postoperative MAP detected a significant increase in the ESPB group compared to the QLPB group at 1h, 2 h and 16 h.12
In the current study, the time to the first dose of morphine and total 24 h morphine consumption were insignificantly different between the ESPB group and QL3 group and significantly delayed in the PVPB group than the ESPB group and QL3 group with a significant decrease in the PVPB group than ESPB group and QL3 group reflecting the good analgesic effect of PVPB.
Elewa et al. reported discrepant results.13 The first required analgesia showed insignificant difference between the ESPB and PVB groups. Furthermore, Abd Ellatif and Abdelnaby et al.10 showed that the time to first rescue analgesic was insignificantly different between QLPB and ESPB groups. Conforming our results, Mohamed et al. demonstrated that the time to first analgesic request was insignificantly different between the ESPB group and QL3 group.12
Complications occurred in 10% of the patients in the PVPB group but not in patients in the QLPB and ESPB groups. The difference was significant. In studies by other researchers no complications were reported regarding the block placement QLPB group and ESPB group or PVPB group.10,13
We believe no previous study contrasted the efficiency of US-guided PVPB, QLB (III), and ESPB in bladder cancer cases having radical cystectomy surgery. The study's strength was the predetermined calculation of sample size, proper randomization of the participants, and the fact that the same anesthesiologist conducted all steps to prevent researcher bias.
The study was performed on a small sample size and in a single center. A single injection was used for all groups; however. To prolong the duration of the block and further lower postoperative morphine usage, a catheter use for continuous analgesia may be utilized. Another limitation was that the study did not include a control group without any block.
The US-guided paravertebral plane block was superior to quadratus lumborum plane block and erector spinae plane block in providing more effective analgesia but with higher time to perform block and postoperative complications. Quadratus lumborum plane block and erector spinae plane block had a similar analgesic effect with no observed side effects compared to paravertebral plane block.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Acknowledgement
We gratefully thank Faculty of Medicine
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
NES: Concept and collecting the data
MME: Manuscript writing, Supervision
ARA: Concept and conduction of the study
MMZ: Collecting the data and Manuscript writing
ME: Supervision
Author affiliations:
- Nazmy Edward Seif, Lecturer of Anesthesia & Intensive Care, Faculty of Medicine, Cairo University, Cairo, Egypt; E-mail: drnazmyseif@yahoo.com
- Manar Mahmoud El-Kholy, Professor of Anesthesia & Intensive Care, Faculty of Medicine, Cairo University, Cairo, Egypt; E-mail: Manarelkholy@kasralainy.Edu.eg
- Ashgan Raouf Ali, Professor of Anesthesia & Intensive Care, Faculty of Medicine, Cairo University, Cairo, Egypt; Email: ashganraouf@yahoo.com
- Moustafa Mohamed Zalat, Assistant Lecturer of Anesthesia & Intensive Care, Faculty of Medicine, Cairo University, Cairo, Egypt; E-mail: Drmoustafazalat@gmail.com
- Mohamed Elshazly, Lecturer of Anesthesia & Intensive Care, Faculty of Medicine, Cairo University, Cairo, Egypt; E-mail: Dr.mohamed.elshazly8686@gmail.com
ABSTRACT
Background &objective: Transmuscular quadratus lumborum plane block (QLPB), paravertebral plane block (PVPB), and erector spinae plane block (ESPB) are three regional anesthesia techniques for management of perioperative pain for surgical procedures on the trunk, including thorax and abdomen. We compared the effectiveness of PVPB, QLPB type III (QL3), and ESPB for perioperative analgesia during radical cystectomy performed for bladder cancer.
Methodology: This randomized double-blind trial was performed on 120 patients, aged above 18 years, undergoing radical cystectomy under general anesthesia. Individuals were randomly divided into 3 equal groups: ESPB, PVPB, and QLPB. Blocks were performed under ultrasound guidance preoperatively on each side with 30 ml of 0.25% bupivacaine. Time to perform block and time to the first dose of morphine postoperatively, were noted. Intra-operative hemodynamic data, including MAP and heart rate (HR) were noted every 10 min for an hour, and then at 30 min intervals. Postoperatively, MAP and HR were recorded at 0, 2, 6, 12 and 24 hours. The connection between qualitative factors was investigated using the chi-square test and Fisher's exact test. For the purpose of comparing the groups, one-way ANOVA and the Bonferroni correction were used. A two-tailed P value < 0.05 was considered significant.
Results: Time to perform block was substantially reduced in ESPB and QL3 groups compared to PVPB group. Time to the first dose of morphine was substantially delayed in the PVPB group than ESPB and QL3 groups. Total 24 h morphine consumption was substantially lower in the PVPB group than ESPB and QL3 groups. Postoperative visual analog scale measurements were substantially lower at 15 min, 30 min, and 12 h in the PVPB group than ESPB and QL3 groups and at 6 h in the ESPB and QL3 groups than in PVPB group. Postoperative mean arterial blood pressure and heart rate measurements were substantially reduced at 0 and 12 h in the PVPB group than in ESPB and QL3 groups and at 6 h in the ESPB and QL3 groups than in PVPB group.
Conclusions: The ultrasound guided paravertebral plane block was superior to quadratus lumborum plane block type III and erector spinae plane block in providing more effective analgesia but with higher time to perform block.
Abbreviations: ESPB- Erector Spinae Plane Block; PVPB- Paravertebral Plane Block; QLPB- Quadratus Lumborum Plane Block; QL3- Quadratus Lumborum Plane Block Type III
Keywords: Paravertebral Plane Block; Quadratus Lumborum Plane Block; Erector Spinae Plane Block; Ultrasound; Radical Cystectomy
Citation: Seif NE, El-Kholy MM, Ali AR, Zalat MM, Elshazly M. Three ultrasound guided plane blocks for perioperative analgesia in patients undergoing radical cystectomy: a randomized clinical trial. Anaesth. pain intensive care 2024;28(1):85-91; DOI: 10.35975/apic.v28i1.2381
Received: September 28, 2023; Reviewed: October 31, 2023; Accepted: October 31, 2023
1. INTRODUCTION
Of all bladder cancers, urothelial carcinoma of the bladder (UCB) makes up around 90% of cases. Based on data for the year 2019 provided by the American Cancer Society,1 UCB is the cancer with the 5th highest incidence overall and the 4th most prevalent cancer in men. The patient requires 5 to 10 days to recuperate from a radical cystectomy (RC), a major procedure that causes severe postoperative discomfort and diminished function.2-4
The standard treatment for post-cystectomy pain is opioid analgesics. However, opioids often have negative side effects including postoperative ileus, nausea and vomiting, prolonged sedation, and respiratory depression.5
Regional blocks are one of the primary techniques employed for Enhanced Recovery After Surgery (ERAS) with the aim to reduce postoperative problems, such as postoperative pain and hospital stay, and are a component of multimodal analgesia. Additionally, they outperform systemic opioids in lowering the possibility of postoperative delirium, particularly in elderly individuals.6
The application of ultrasound in regional techniques offers important advantages over traditional approaches like nerve stimulation and reducing resistance, according to an expanding amount of research and advances in technology. We compared the efficacy of three different spinal blocks: the erector spinae plane block (ESPB), transmuscular quadratus lumborum plane block (QLPB), and thoracic paravertebral plane block (PVPB).
2. METHODOLOGY
This randomized double-blind study was performed on 120 patients, aged above 18 years, of both sexes, American Society of Anesthesiologists (ASA) II-III, undergoing radical cystectomy under general anesthesia. Following permission from the Cairo University Hospitals' Ethics Committee and registration with clinicaltrials.gov (ID: NCT05278598), the research was conducted from April 2022 to January 2023. All patients provided written informed approval.
Criteria for the exclusion were; uncooperative individuals, contraindications for peripheral regional anesthesia blocks, individuals taking opioids for persistent pain pre-operatively, choice of spinal anesthesia or any other regional anesthesia, patients at risk for developing coagulopathy (defined as partial thromboplastin time (PTT) > 40 sec, international normalized ratio (INR) more than 1.4, platelet count less than 100x109, anatomical abnormalities or infections at the site of injection.
Participants were assigned at random to one of the research groups using a computer-generated table. The alphanumeric codes on the sealed envelopes were used to disguise the randomization process. Unrelated to the randomization process, the patient identities were affixed to the opened envelopes and safeguarded. The group assignment was concealed from both the participants and the data assessor. Based on the kind of perioperative analgesia used, the participants were split into 3 groups equally: Group PVPB, ESPB, or QLPB.
As soon as the patient entered the operating room, perioperative monitoring was applied. This included a continuous electrocardiogram, finger-based pulse oximetry, and non-invasive arterial blood pressure monitoring (using a GE-Datex Ohmeda multiparameter monitor).
The group assignment was revealed after the envelopes were opened. Prior to the introduction of general anesthesia, ultrasound-guided blocks were carried out under aseptic conditions. Inj midazolam 1 mg was injected intravenously.
Each block was carried out prior to surgery with 5 cm of 1% lidocaine infiltration at the location of the needle injection on each side.
In all groups, every patient got 30 mL of 0.25% bupivacaine on both sides. A 22-G spinal needle was used for all blocks, and a Siemens Acuson x300 3-5 MHz US machine was used, which was housed under a sterile cover.
2.1. Erector spinae plane block
The block was administered bilaterally at the level of T9 after the patient had been directed laterally. A curvilinear high-frequency U-S transducer was positioned 3 cm laterally to the T9 spinous process, in which a hyper-echoic shadow of the transverse process (TP) and erector spinae was established. Next, the needle was inserted into the TP, traversing the entire group of muscles.
2.2. Thoracic paravertebral plane block
A curved high-frequency US transducer was utilized to view the T10 paravertebral region in the paramedian sagittal plane on both sides, in sitting position; an injection into this area would disseminate to many nearby dermatomes. The spinal needle was put in-plane with respect to the US probe and moved gradually from lateral to medial until the apex of the paravertebral space was reached at the tip. The pleura was displaced anteriorly and it served as the completion of the block.
2.3. Quadratus lumborum plane block
In order to find the triple abdominal muscle layers, the participant was set up laterally on each side. A curved high-frequency US transducer was then placed horizontally in the anterior axillary line, midway between the subcostal border and the iliac crest. With the psoas major muscle positioned anteriorly, the erector spinae muscle posteriorly, and the quadratus lumborum muscle attached to the apex of the TP, this is a pattern that is well known as a shamrock with 3 leaves.7
Fentanyl 1.5 μg/kg, to a maximum dosage of 200 μg, propofol 2 mg/kg and atracurium 0.5 mg/kg were used to induce general anesthesia and to aid tracheal intubation. A urinary catheter was inserted. For the sake of preserving normocapnia, volume-controlled ventilation was modified. Atracurium top-ups at 0.1 mg/kg every 30 min and 1–1.5% isoflurane in a 50/50 combination of oxygen and air were used to maintain anesthesia.
Following skin closure, inhalational anesthesia was stopped, and once the patient's spontaneous breathing had returned, atropine 0.02 mg/kg and neostigmine 0.05 mg/kg were given intravenously to reverse muscular relaxation. Fifteen minutes after extubation, a VAS was used to measure pain, with 0 representing no pain and 10 representing the most severe pain. Rescue analgesia in the form of morphine 0.1 mg/kg was administered if the score reached 4/10. If the score remained over 4 following 30 min after the first dosage, a further administration of morphine 0.1 mg/kg was provided in the PACU. Hemodynamic parameters were recorded intra-operatively and postoperatively.
The primary outcome was to estimate cumulative 24-hour morphine consumption. The secondary outcomes were measurement of postoperative pain intensity, time to first postoperative analgesic request, block procedure time and any complications.
2.4. Sample size calculation
Using a G power program on the level of mean morphine consumption in the first 24 h postoperative using one-way ANOVA because it was the main outcome variable in the present study. A previous study has reported that the mean (SD) first 24 h of morphine consumed in the ESPB group versus TAP block in radical cystectomy was 3.2571(0.78) and 5.6571(1.55), respectively [8]. In a pilot study on 5 patients, the morphine consumption in the first 24 h was 4.2(1.8) mg. With a minimum of thirty-five participants per group, a study's power was predicted to be 95% and its alpha error to be 0.05. In order to account for potential dropouts, this number was raised to forty participants in each group.
| Table 1: Patient’s demographic data and duration of surgery | |||||
| Parameter | QL3 group (n = 40) |
ESPB group (n = 40) |
PVPB group (n = 40) |
P value | |
| Age (years) | 60 ± 9.69 | 57.8 ± 9.98 | 57.6 ± 8.59 | 0.457 | |
| Sex (Male) | 30 (75) | 26 (65) | 25 (62.5) | 0.450 | |
| BMI (Kg/m2) | 25.3 ± 3.26 | 24.5 ± 2.97 | 25.5 ± 2.95 | 0.287 | |
| ASA PS | II | 38 (95) | 38 (95) | 0.272 | 0.272 |
| III | 2 (5) | 2 (5) | 6 (15) | ||
| Duration of surgery (h) | 4.1 ± 1.22 | 4.2 ± 1.08 | 4.7 ± 1.24 | 0.062 | |
| Data are presented as mean ± SD or frequency (%). ASA: American Society of Anesthesiologists, BMI: Body mass index. QL3: quadratus lumborum 3. ESPB: erector spine plane block. PVPB: paravertebral plane block | |||||
| Table 2: Time to perform the block, and morphine use | ||||
| Variable | QL3 group (n = 40) |
ESPB group (n = 40) |
PVPB group (n = 40) |
P value |
| Time to perform block (min) | 5.6 ± 0.64 | 5.5 ± 0.88 | 8.5 ± 0.7 | P1 = 0.901 P2 < 0.001* P3 < 0.001* |
| Time to first dose morphine (min) | 328 ± 42.38 | 346.5 ± 47.15 | 507.8 ± 31.58 | P1 = 0.111 P2 < 0.001* P3 < 0.001* |
| Total 24h morphine consumption (mg) | 10.4 ± 1.48 | 10.1 ± 1.62 | 7.3 ± 0.88 | P1 = 0.589 P2 < 0.001* P3 < 0.001* |
| Incidence of Complications | 0 (0%) | 0 (0%) | 4 (10%) | 0 .016* |
| Data are presented as mean ± SD or frequency. * Significant as p value <0.05, P1: P value between groups QL3 and ESPB, P2: P value between groups QL3 and PVPB, P3: P value between groups ESPB and PVPB. QL3: quadratus lumborum 3. ESPB: erector spine plane block. PVPB: paravertebral plane block | ||||
2.5. Statistical analysis
Software such as Medcalc and SPSS v15 (Chicago, IL) were used for statistical analysis. The mean and standard deviation (SD) of the quantitative parameters were reported, and they were contrasted for the same group using a paired Student's t-test. Frequency and percentages (%) were used to illustrate qualitative parameters. The connection between qualitative factors was investigated using the chi-square test and Fisher's exact test. For the purpose of comparing the groups, one-way ANOVA and the Bonferroni correction were used. A two-tailed P value < 0.05 was considered significant.
3. RESULTS
For this research 142 participants were screened; 14 were found to be ineligible, and 8 individuals declined to take part. The other 120 individuals were divided into 3 groups, each with 40 participants. All of the participants followed up and statistically analyzed (Figure 1).
The demographic data of the participants, including age, sex, BMI, ASA physical status, and surgeries duration were equivalent among the three groups (Table 1).
The time to execute the block, time to administer the initial dose of morphine, and total 24-hour morphine intake were not statistically different from each other in the ESPB group and QL3 group, and in both of these groups time to conduct the block was considerably shorter than that of the PVPB group. In comparison to ESPB group and QL3 group, time to the first dosage of morphine was considerably delayed in PVPB group. The PVPB group consumed much less morphine overall throughout the course of a 24-hour period than the ESPB group and QL3 group. Comparing the PVPB group to the ESPB group and the QL3 group, complications were much more common (Table 2).
| Table 3: Postoperative visual analog scale (VAS) measurements among the three groups | ||||
| Recording time | QL3 group (n = 40) |
ESPB group (n = 40) |
PVPB group (n = 40) |
P value |
| 15 min | 1 (0 - 4) | 1 (0 - 4) | 0 (0 - 1) | P1 = 0.975 P2 = 0.003* P3 = 0.003* |
| 30 min | 1 (0 - 3) | 1.5 (0 - 4) | 0 (0 - 1) | P1 = 0.712 P2 = 0.002* P3 < 0.001* |
| 2 h | 2 (1 - 2) | 2.5 (0 - 4) | 2 (1 - 3.25) | 0.807 |
| 6 h | 1 (0 - 2) | 1 (0 - 2) | 2 (2 - 3) | P1 = 0.751 P2 < 0.001* P3 < 0.001* |
| 12 h | 3 (3 - 3) | 3.5 (3 - 4) | 1 (0 - 2.25) | P1 = 0.205 P2 < 0.001* P3 < 0.001* |
| 24 h | 3 (2 - 4) | 3 (2 - 4) | 3 (3 - 4) | 0.124 |
| Data are presented as median (IQR), * significant as P < 0.05, P1: P value between groups QL3 and ESPB, P2: P value between groups QL3 and PVPB, P3: P value between groups ESPB and PVPB. QL3: quadratus lumborum 3. ESPB: erector spine plane block. PVPB: paravertebral plane block | ||||
Postoperative VAS measurements at 15 min, 30 min, and 12 h were insignificantly different among the ESPB group and QL3 group. They were substantially reduced in the PVPB group than the ESPB group and QL3 group.
Postoperative VAS measurements at 6 h were insignificantly different among the ESPB group and QL3 group and were substantially greater in the PVPB group than the ESPB group and QL3 group (Table 3).
Intraoperative mean blood pressure measurements were insignificantly different in all measurements among the three groups (Table 4).
Intraoperative heart rate (HR) measurements were insignificantly different among the three groups (Table 4).
Postoperative MAP and HR measurements at 0 and 12 h were significantly lower in the PVPB group than ESPB group and QL3group. They were significantly higher in the PVPB group than the ESPB group and QL3group at 6 h (Table 6).
4. DISCUSSION
The typical approach to post-cystectomy management of pain is opioid analgesics.5 However, opioids often have negative side effects including postoperative ileus, severe sedation, and depressed breathing.6
In the present study, the time to execute the block was substantially reduced in the ESPB group and QL3 group compared to the PVPB group. Our findings contradict the results of Thomas et al.9 study, which showed that the time to perform the block was insignificantly different between the ESPB and the PVPB groups. The contrary result was observed by Abd Ellatif and Abdelnaby,10 who stated that the time to execute block was significantly reduced in the ESPB group compared to the QLPB group.
In our study, intraoperative mean blood pressure measurements and HR were insignificantly different at all measurements among the three groups, denoting that all blocks were efficiently doing their effect with good hypnosis and muscle relaxation. In agreement to our results, Various researchers reported insignificant statistical differences in the MAP and HR intraoperatively between both groups. Also, Mohamed et al. reported insignificant statistical differences in the me MAP and HR intraoperatively between the ESPB and QLPB groups. 9,11,12,13
| Table 4: Intraoperative mean blood pressure (mmHg) and intraoperative heart rate (bpm) measurements among the three groups | ||||
| Recording time | QL3 group (n = 40) |
ESPB group (n = 40) |
PVPB group (n = 40) |
P value |
| Intraoperative mean blood pressure | ||||
| Baseline | 87.95 ± 9.71 | 92.3 ± 9.79 | 91.98 ± 7.75 | 0.064 |
| 10 min | 84 ± 9.58 | 87.4 ± 8.44 | 86.05 ± 8.1 | 0.219 |
| 20 min | 84.38 ± 8.99 | 86.3 ± 5.31 | 84.75 ± 6.67 | 0.445 |
| 30 min | 83.25 ± 8.12 | 84.63 ± 7.06 | 83.83 ± 6.27 | 0.692 |
| 40 min | 83.18 ± 7.56 | 84.95 ± 6.54 | 84.53 ± 6.02 | 0.471 |
| 50 min | 85.05 ± 7.81 | 86.5 ± 5.75 | 84.63 ± 6.32 | 0.423 |
| 60 min | 83.55 ± 7.1 | 84.23 ± 8.26 | 83.88 ± 6.14 | 0.916 |
| 90 min | 83.6 ± 7.04 | 83.43 ± 6.88 | 83.8 ± 6.24 | 0.969 |
| 120 min | 82.93 ± 6.24 | 83.63 ± 7.22 | 83.9 ± 6.24 | 0.792 |
| 150 min | 83.25 ± 6.28 | 83.33 ± 7.39 | 82.83 ± 6.5 | 0.938 |
| Intraoperative heart rate | ||||
| Baseline | 78.33 ± 8.95 | 81.2 ± 7.58 | 80.43 ± 8.9 | 0.298 |
| 10 min | 76.98 ± 8.84 | 78.68 ± 6.48 | 79.5 ± 7.86 | 0.339 |
| 20 min | 78.28 ± 8.15 | 76.35 ± 5.44 | 77.93 ± 6.84 | 0.416 |
| 30 min | 75.4 ± 8.25 | 74.45 ± 5.71 | 76.25 ± 5.61 | 0.481 |
| 40 min | 74.68 ± 6.63 | 74.53 ± 4.62 | 74.95 ± 5.24 | 0.942 |
| 50 min | 73.73 ± 6.24 | 73.78 ± 4.68 | 73.98 ± 3.17 | 0.971 |
| 60 min | 73.53 ± 5.94 | 74.23 ± 4.46 | 74.68 ± 4.77 | 0.598 |
| 90 min | 73.63 ± 5.76 | 73.75 ± 4.4 | 73.95 ± 4.24 | 0.955 |
| 120 min | 74.08 ± 6.02 | 73.68 ± 4.43 | 74.4 ± 3.91 | 0.801 |
| 150 min | 72.78 ± 12.38 | 73.9 ± 4.65 | 74.1 ± 3.93 | 0.725 |
| Data are presented as mean ± SD. QL3: quadratus lumborum 3. ESPB: erector spine plane block. PVPB: paravertebral plane block | ||||
According to our results, postoperative VAS measurements at 15 min, 30 min, and 12 h were significantly reduced in the PVPB group than in the ESPB group and QL3 group. They were significantly greater in the PVPB group than the ESPB group and QL3 group at 6 h postoperatively, with insignificant variations across the 3 groups at 2 and 24 h. Postoperative VAS measurements always were insignificantly different between the ESPB group and QL3 group. Our findings disagreed with Elewa et al.,13 who reported that concerning postoperative pain, the ESPB had an extended analgesic effect than the PVB, as indicated by the significant decrease in the VAS score at 8 h and 12 h after the operation. This difference could be due to the different surgical procedures. Our findings agree with Abd Ellatif and Abdelnaby et al. the VAS score was insignificantly different between QLPB and ESPB groups at any time.10
Following our results, Xiong et al. results showed that for patients having thoracic and breast surgeries, PVB substantially decreased the postoperative pain ratings at rest at 0-1, 4-6, and 24 h in comparison to ESPB.14 Moreover, Mohamed et al. found that the postoperative VAS measurements were insignificantly different between ESPB and QL3 groups.12
The previous changes detected in pain perception were reflected in the postoperative hemodynamic changes (MAP and HR). The postoperative MAP and HR measurements at 0 and 12 h were significantly lower in the PVPB group than the ESPB group and QL3group, due to the good analgesia of PVPB as mentioned before. At the same time, they were significantly higher in the PVPB group than the ESPB group and QL3group at 6h, caused by the elimination of the LA effect and the need for morphine dose. There was an insignificant difference between the groups at 2 and 24 h. Postoperative MAP measurements were insignificantly different between the ESPB group and QL3 group. Supporting our results, Elkotory et al. reported insignificant statistical differences in the postoperative MAP measurements between QLB and ESB groups.11 In contrast to our results, Mohamed et al. showed that postoperative MAP detected a significant increase in the ESPB group compared to the QLPB group at 1h, 2 h and 16 h.12
| Table 5: Postoperative mean arterial blood pressure (mmHg) and Postoperative heart rate (bpm) measurements among the three groups | |||||
| QL3 group (n = 40) |
ESPB group (n = 40) |
PVPB group (n = 40) |
P value | ||
| Postoperative mean arterial blood pressure | |||||
| 0 | 97.23 ± 10.86 | 96.23 ± 10.96 | 90.55 ± 7.64 | P1 = 0.895 P2 = 0.009* P3 = 0.032* |
|
| 2 h | 89.60 ± 7.49 | 93.18 ± 8.20 | 90.15 ± 8.11 | 0.100 | |
| 6 h | 88.48 ± 7.68 | 87.90 ± 7.24 | 93.30 ± 6.90 | P1 = 0.934 P2 < 0.001* P3 = 0.003* |
|
| 12 h | 92.78 ± 8.23 | 93.38 ± 6.45 | 86.60 ± 15.77 | P1 = 0.967 P2 = 0.034* P3 = 0.018* |
|
| 24 h | 92.83 ± 9.66 | 93.58 ± 6.88 | 94.83 ± 6.89 | 0.523 | |
| Postoperative heart rate | |||||
| 0 | 84.90 ± 8.67 | 83.83 ± 9.90 | 77.83 ± 7.41 | < 0.001* | P1 = 0.846 P2 < 0.001* P3 = 0.007* |
| 2 h | 80.98 ± 6.36 | 82.60 ± 5.83 | 81.98 ± 7.27 | 0 .533 | |
| 6 h | 80.45 ± 8.12 | 79.78 ± 5.92 | 84.85 ± 9.93 | 0 .012* | P1 = 0.927 P2 = 0.045* P3 = 0.017* |
| 12 h | 84.68 ± 6.13 | 85.20 ± 6.66 | 79.30 ± 7.44 | < 0.001* | P1 = 0.936 P2 = 0.002* P3 < 0.001* |
| 24 h | 83.08 ± 7.21 | 84.38 ± 6.99 | 85.65 ± 7.78 | 0 .259 | |
| Data are presented as mean ± SD. * Significant as p value <0.05, P1: P value between groups QL3 and ESPB, P2: P value between groups QL3 and PVPB, P3: P value between groups ESPB and PVPB. QL3: quadratus lumborum 3. ESPB: erector spine plane block. PVPB: paravertebral plane block. 0: Time immediately post-extubation | |||||
In the current study, the time to the first dose of morphine and total 24 h morphine consumption were insignificantly different between the ESPB group and QL3 group and significantly delayed in the PVPB group than the ESPB group and QL3 group with a significant decrease in the PVPB group than ESPB group and QL3 group reflecting the good analgesic effect of PVPB.
Elewa et al. reported discrepant results.13 The first required analgesia showed insignificant difference between the ESPB and PVB groups. Furthermore, Abd Ellatif and Abdelnaby et al.10 showed that the time to first rescue analgesic was insignificantly different between QLPB and ESPB groups. Conforming our results, Mohamed et al. demonstrated that the time to first analgesic request was insignificantly different between the ESPB group and QL3 group.12
Complications occurred in 10% of the patients in the PVPB group but not in patients in the QLPB and ESPB groups. The difference was significant. In studies by other researchers no complications were reported regarding the block placement QLPB group and ESPB group or PVPB group.10,13
We believe no previous study contrasted the efficiency of US-guided PVPB, QLB (III), and ESPB in bladder cancer cases having radical cystectomy surgery. The study's strength was the predetermined calculation of sample size, proper randomization of the participants, and the fact that the same anesthesiologist conducted all steps to prevent researcher bias.
5. LIMITATIONS
The study was performed on a small sample size and in a single center. A single injection was used for all groups; however. To prolong the duration of the block and further lower postoperative morphine usage, a catheter use for continuous analgesia may be utilized. Another limitation was that the study did not include a control group without any block.
6. CONCLUSIONS
The US-guided paravertebral plane block was superior to quadratus lumborum plane block and erector spinae plane block in providing more effective analgesia but with higher time to perform block and postoperative complications. Quadratus lumborum plane block and erector spinae plane block had a similar analgesic effect with no observed side effects compared to paravertebral plane block.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Acknowledgement
We gratefully thank Faculty of Medicine
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
NES: Concept and collecting the data
MME: Manuscript writing, Supervision
ARA: Concept and conduction of the study
MMZ: Collecting the data and Manuscript writing
ME: Supervision
11. REFERENCES
- Viale PH. The American Cancer Society's Facts & Figures: 2020 Edition. J Adv Pract Oncol. 2020;11:135-6. [PubMed] DOI: 6004/jadpro.2020.11.2.1
- Hautmann RE, de Petriconi RC, Volkmer BG. Lessons learned from 1,000 neobladders: the 90-day complication rate. J Urol. 2010;184:990-4. [PubMed] DOI: 1016/j.juro.2010.05.037
- Hounsome LS, Verne J, McGrath JS, Gillatt DA. Trends in operative caseload and mortality rates after radical cystectomy for bladder cancer in England for 1998-2010. Eur Urol. 2015;67:1056-62. [PubMed] DOI: 1016/j.eururo.2014.12.002
- Bhalla RG, Wang L, Chang SS, Tyson MD. Association between Preoperative Albumin Levels and Length of Stay after Radical Cystectomy. J Urol. 2017;198:1039-45. [PubMed] DOI: 1016/j.juro.2017.05.066
- Barletta JF. Clinical and economic burden of opioid use for postsurgical pain: focus on ventilatory impairment and ileus. Pharmacotherapy. 2012;32:12s-8s. [PubMed] DOI: 1002/j.1875-9114.2012.01178.x
- Xu W, Daneshmand S, Bazargani ST, Cai J, Miranda G, Schuckman AK, et al. Postoperative Pain Management after Radical Cystectomy: Comparing Traditional versus Enhanced Recovery Protocol Pathway. J Urol. 2015;194:1209-13. [PubMed] DOI: 1016/j.juro.2015.05.083
- Lu Y, Zhang J, Xu X, Chen W, Zhang S, Zheng H, et al. Sensory assessment and block duration of transmuscular quadratus lumborum block at L2 versus L4 in volunteers: a randomized controlled trial. Minerva Anestesiol. 2019;85:1273-80. [PubMed] DOI: 23736/S0375-9393.19.13656-5
- Kumar GD, Gnanasekar N, Kurhekar P, Prasad TK. A comparative study of transversus abdominis plane block versus quadratus lumborum block for postoperative analgesia following lower abdominal surgeries: a prospective double-blinded study. Anesth Essays Res. 2018;12:919-23. [PubMed] DOI: 4103/aer.AER_158_18
- Thomas AB. Comparison of Single Injection of Erector Spinae Plane Block and Paravertebral Block in Reducing Post Operative Pain in Children: A Prospective, Double Blinded, Randomized Controlled Trial: Christian Medical College, Vellore; 2020.
- Abd Ellatif SE, Abdelnaby SM. Ultrasound guided erector spinae plane block versus quadratus lumborum block for postoperative analgesia in patient undergoing open nephrectomy: a randomized controlled study. Egypt J Anaesth. 2021;37:123-34.DOI: 1080/11101849.2021.1894661
- Elkotory ME, Amer GF, El Badawy MA. Comparative study between ultrasound guided quadratus lumborum plane block versus ultrasound guided erector spinae plane block for postoperative pain relief in patients undergoing elective caesarean sectio Al-Azhar Int Med J. 2022;3(2).DOI: 10.21608/AIMJ.2022.104869.1648
- Mohamed AH, Mohamed SR, Farouk M. Analgesic effect of ultrasound guided regional block in laparoscopic cholecystectomy. Minia J Med Res 2020;31:150-61. DOI: 21608/mjmr.2022.220854
- Elewa AM, Faisal M, Sjöberg F, Abuelnaga ME. Comparison between erector spinae plane block and paravertebral block regarding postoperative analgesic consumption following breast surgery: a randomized controlled study. BMC Anesthesiol. 2022;22:189. [PubMed] DOI: 1186/s12871-022-01724-3
- Xiong C, Han C, Zhao D, Peng W, Xu D, Lan Z. Postoperative analgesic effects of paravertebral block versus erector spinae plane block for thoracic and breast surgery: A meta-analysis. PLoS One. 2021;16:256611. [PubMed] DOI: 10.1371/journal.pone.0256611