Mohamed A. Wadood1, Mahmoud Abdelgalil Abdelrahman2, Mamdouh Mahmoud Mostafe3, Ekramy Mansour Abdelghafar4, Reham Mohamed Gamal5
Author affiliations:
Background & objective: Pain during nephrectomy has been reported to be extremely intense and may trigger complex biochemical and physiological stress response if managed inadequately. Erector spinae plane block (ESPB) and thoracic epidural analgesia (TEA) both have been advocated for pain management in adult patients undergoing open nephrectomy under general anesthesia. We compared the efficacy and the dynamics of both of these procedures.
Methodology: This was a randomized, double-blinded, controlled trial involving 54 patients were undergoing open nephrectomy for malignant kidney tumors. All patients were ASA class II, had a BMI 20-40 kg/m2, and were between the ages of 18-65 y. Through random assignment, people were divided into two identical, equivalent groups: Group A (n = 27) received TEA, whereas Group B (n = 27) received US-guided continuous ESPB. Mean arterial pressure (MAP) and intraoperative heart rate (HR) were recorded before and after incision, and at 30 min, 1 h, and 1.5 h. Postoperative HR, MAP were recorded at 6 h and 12 h, both at rest and when moving. Numerical rating scale (NRS) score was used to compare the intensity of postoperative pain.
Results: Postoperative HR, MAP, at 6 h and 12 h, at rest and when moving, were substantially reduced in the TEA group than those in the ESPB group. The NRS score of the ESPB group was substantially greater than that of the TEA group. In contrast to the TEA group, much more total amount of morphine was consumed in the ESPB group. The time to first rescue analgesia was substantially shorter in ESPB group than that of the TEA group.
Conclusions: The results of our study prove that US guided erector spinae plane block is effective in providing postoperative analgesia, decreasing use of intraoperative and postoperative opioids in patients having open nephrectomy. However, it is still inferior to thoracic epidural analgesia in terms of pain control after 6 h postoperatively. Otherwise, erector spinae plane block has fewer side effects compared to thoracic epidural analgesia. So, it may be used as an alternative to thoracic epidural analgesia.
Key words: Erector Spinae Plane Block; Epidural Analgesia; Open Nephrectomy; Pain, Postoperative; Ultrasound
Citation: Wadood MA, Abdelrahman MA, Mostafe MM, Abdelghafar EM. Ultrasound-guided continuous erector spinae plane block versus thoracic epidural analgesia in open nephrectomy for renal malignancy: a randomized controlled study, Anaesth. pain intensive care 2024;28(1):26-32; DOI: 10.35975/apic.v28i1.2377
Received July 24, 2023; Revised: September 08, 2023; Accepted: October 03, 2023
Renal cell carcinoma (RCC) is the third most prevalent cancer of the genitourinary tract and makes up between 2% -3% of all malignancies.1 The acknowledged curative procedure for resectable kidney tumors for many years has been open nephrectomy. Nephrectomy-related pain is well-known to be quite intense and to result in severe biochemical and physiological stress. Therefore, effective treatment of initial postoperative pain is crucial for the patient satisfaction.2 Opioids have been the most effective medication for treating postoperative pain, but using them in high doses can have negative side effects.3 Hence substitutes to opioids are advised for effective analgesia.
The cornerstone of the peri-operative treatment for abdominal procedures, delivering the most effective analgesia, is thought to be thoracic epidural analgesia (TEA). However, TEA has been linked to major side effects such as hypotension, urine retention, decreased lower limb motor function, injury to the spinal cord, breathing problems brought on by the use of opioids, dural puncture with a needle or catheter, and headache following a dural puncture.4
The erector spinae plane block (ESPB) was initially shown to be utilized for treating long-term thoracic neuropathic discomfort by injecting local anesthetic into the erector spinae muscle plane (ESP) at the level of T5.5 It is reasonably easy procedure to carry out, with end points for the insertion of needles and for the application of local anesthetic and plainly discernible sonographic markers.5 It has been applied both in thoracic and abdominal surgeries with high success rates providing both visceral and somatic analgesia. 5, 6 ESPB can provide sensory block in the distribution area from T2-T4 to L1–L2.5, 6
ESPB is regarded to be theoretically simpler, even though it can offer a block that is identical to the paravertebral block, given that the needle is oriented away from the pleura, thus reducing the possibility of the block related complications, e.g., pneumothorax.7 In addition, it is likely to be safe in patients with suboptimal coagulation status. It has a lesser risk of blood vessel or injury to the brain than an epidural or a paravertebral block.8
In order to visualize and identify the normal and unusual positions of nerves, blood vessels, ultrasound (US) imaging is utilized to deposit and disseminate local anesthetics (LA) in the appropriate plane and around the intended nerve/s while the needle is passed through the tissues.9
We compared ESPB and TEA blocks for their efficacy in pain relief following surgery of adult individuals undergoing open nephrectomy under general anesthesia.
This randomized, double-blinded, controlled study was conducted at the National Cancer Institute and comprised 54 patients with malignant kidney tumors, ASA class II, ages 18-65 y, Body Mass Index (BMI) 20-40 kg/m2, scheduled for open nephrectomy under general anesthesia.
All patients gave their informed written consent. Approval of institutional ethics committee was secured.
The exclusion criteria included, an infection at the puncture site, coagulopathies with a platelet count below 100,000 or an INR of greater than 1.3, renal and hepatic insufficiency, unsteady heart disease, a history of psychiatric and cognitive disorders, patients allergic to the drugs to be used, and inappropriate anatomy of the thoracic region.
By random selection, the patients were split into two just comparable groups: Group A (n = 27) got continuous TEA, whereas Group B (n = 27) received continuous ESPB that was US-guided.
Every patient had a thorough history review, physical examination, and standard laboratory tests.
2.1. Group A (TEA)
Skin infiltration with 3 ml of lidocaine 2% was performed with the patient seated and under complete aseptic conditions. The epidural space was located using the loss of resistance technique at the T8 interspace with an 18-G Tuohy needle and a 20-G catheter (Perifix, Braun, Germany) was then advanced 3 cm. To check for inadvertent intrathecal or IV delivery, a test dose of 3 ml of lidocaine 2% with epinephrine in 1:200,000 was given. After a negative response, 10 ml of 0.25% bupivacaine was injected as a bolus dose into the epidural catheter until general anesthesia begun. The patient was placed in the supine posture. The sensory block on the operated side was assessed by pinprick every two minutes in the midclavicular line. After 15 min, if the sensory block level was still below T5, another 5 ml of bupivacaine was given. The dose of bupivacaine 0.125% was then gradually increased over the course of 24 h, based on the pain score and negative consequences, rate modification.10, 11
2.2. Group B (ESPB)
While the patient was sitting, a high-frequency linear US transducer (Fujifilm Sonosite, Inc., Bothell, WA) was positioned in a longitudinal orientation 3 cm lateral to the T8 spinous process. This should draw attention to the three muscles that are superficial to the hyperechoic transverse process shadow: the trapezius, rhomboid major, and erector spinae. To numb the skin, 3 ml of lidocaine 2% was used. An 18-G Tuohy needle with a 20-G catheter (Perifix, Braun, Germany) was placed in-plane and cephalad-to-caudad on the deep (anterior) side of the ESM, 30 min before to the induction of general anesthesia, and 20 ml of 0.25% bupivacaine was administered as a bolus dose in the epidural catheter. The patient was then shifted to the supine position. The sensory block on the operated side was assessed with pinprick every two minutes in the midclavicular line. After 15 min, if the sensory block level was still below T5, another 5 ml of bupivacaine was given. Following the skin incision, bupivacaine 0.125% was constantly infused at a rate of 6 ml/h, and the dosage was boosted by 2 ml/h increments up to 10 ml/h for 24 h. Customizing rates according to the pain score and adverse effects.12-14 Patients with failed block were excluded.

The identical approach was used to provide general anesthesia to each patient. Rocuronium 0.5 mg/kg, fentanyl 1 g/kg IV, and propofol 2 mg/kg were used to induce anesthesia and endotracheal intubation secured. Isoflurane with MAC 1.2% was used to maintain anesthesia in a mixture of 50% air and oxygen.
After two hours of supervision in the postoperative care unit, the patients got rescue analgesia in the form of IV morphine 3 mg boluses. Every patient's total dose of morphine over the course of a day was noted. The patients were then moved to a ward and given 1 g of paracetamol IV every 8 h.
The primary outcome parameter was the total amount of morphine taken in the preceding 24 h, and the secondary outcome variables included the total amount of fentanyl used during surgery, the time at which the first rescue analgesic was given, and pain as assessed by the Numerical Rating Scale (NRS), both at rest and while moving. NRS was used to measure pain ratings in the PACU and for the following 24 h (1, 2, 4, 6, 12 and 24 h) following surgery. Before the LA injection, mean arterial pressure (MAP) and heart rate (HR) were measured to establish a baseline value. After the LA injection, follow-up readings were taken promptly before and after the surgical incision as well as at 30-min intervals through the operation. The consumption of the entire amount of bupivacaine and the occurrence of adverse reactions, such as hemodynamic instability, nausea, vomiting, dural puncture, post dural puncture headache, failed block, unintentional intravascular injection of LA, and local anesthetic toxicity were noted (NRS scores 1-3: mild discomfort, 4-6: moderate pain, and 7-10: severe discomfort).
Postoperative nausea / vomiting (PONV) was assessed on a four-point verbal scale (none = no nausea, mild = little nausea but no vomiting, moderate = one occurrence of vomiting, severe = many bouts of vomiting).15 Patients with mild to severe PONV received an IV dose of ondansetron 0.1 mg/kg.
2.3. Statistical analysis
IBM, Chicago, Illinois, USA's SPSS v27 was used for the statistical analysis. The Shapiro-Wilks test and histograms were utilized to figure out if the data distribution was normal. Quantitative parametric data including mean and standard deviation (SD) were analyzed using an unpaired student t-test. Interquartile range (IQR) and the median were used to report and assess quantitative non-parametric data, respectively. When applicable, qualitative variables were investigated utilizing the Chi-square test or Fisher's exact test and offered as frequency and percentage (%). Statistical reliability was known as a two tailed P ≤ 0.05.
We enrolled 79 participants out of which 21 did not match the qualifying requirements for this study, while 4 patients declined to take part. The remainder of fifty-four individuals were split randomly into two groups of 27 each. One patient dropped out in group A due to dural puncture, and two patients dropped out in group, one due to block failure and the other due to massive blood loss.
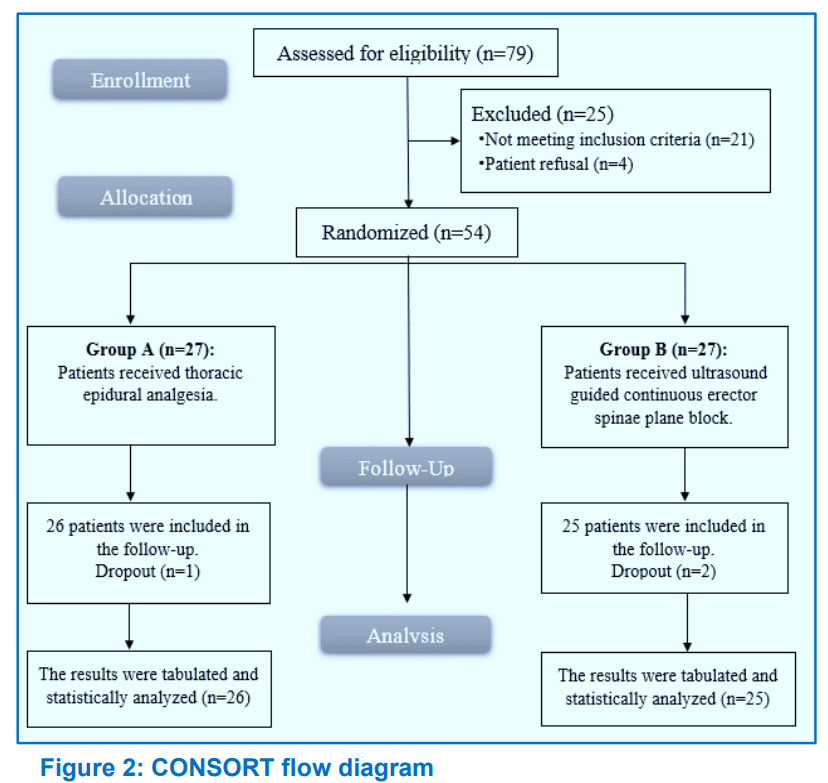
Fifty-one patients were monitored and studied statistically (Figure 2).
The demographic information of the participants and the duration of the procedure were not statistically different between the two groups (Table 1).
Before the incision, in Group A patients intraoperative heart rate was substantially lower than that of Group B. After incision, at 30 min, 1 h, and 1.5 h heart rates were statistically equivalent (P = 0.030, 0.013, 0.034, 0.003 and 0.039 respectively) and was insignificantly different at baseline, 2 h, 2.5 h and between the two groups after the conclusion of operation. As compared to Group B, intraoperative MAP was significantly lower in Group A before surgical incision, after surgical incision, at 30 min, 1 h, and 1.5 h (P = 0.011, < 0.001, < 0.001, < 0.018, and < 0.001 respectively), but there was no difference between the two groups at baseline, 2 h, 2.5 h, or at the conclusion of surgery.
Postoperative HR was insignificantly different between both groups except at 6 h and 12 h, as ESPB group values were substantially higher than TEA group values (P = 0.001 and < 0.043, respectively), but the differences were statistically not significant. Except at 6 and 12 h, when the ESPB group's postoperative MAP was considerably higher than the TEA group's, there was no statistically significant difference between the two groups. (P < 0.001, 0.035 respectively)
With the exception of 6 and 12 h, when the ESPB group's NRS score was considerably higher than the TEA group's, there was no significant difference between the two groups' NRS scores during rest (P < 0.001) (Table 2).
NRS score at movement was insignificantly different between both groups except at 6 h and 12 h, when it was significantly higher in ESPB group contrasted to TEA group (P < 0.001 and 0.004) (Table 3).
In Groups A and B, the median (IQR) of total morphine intake was 0 (0-0) and 3 (0-3) respectively. In comparison to Group A, Group B had considerably greater total morphine consumption, number of patients who needed morphine, and total bupivacaine consumption. Group B experienced the first rescue analgesia earlier than Group A. In comparison to Group A, Group B had a substantially larger number of patients who needed a bolus of bupivacaine (P = 0.022). There was no significant difference in the amount of intraoperative fentanyl consumed between the two groups (Table 4).
PONV, hypotension, and dural puncture were side effects / complications and did not substantially differ between the two groups. Local anesthetic toxicity, respiratory depression, post-dural puncture headache, and inadvertent intravascular injection of LA did not happen in either group (Table 5).
During the intra-operative period, our results showed that before the incision, intraoperative HR in the TEA group was considerably lower than it was in the ESPB group, and was insignificantly different at baseline, 2 h, 2.5 h and after the conclusion of the procedure in both groups. These results are consistent with that of Moawad, et al.16 as at 2, 2½, 3, and 3½ h into the operation, compared to the PVB group, the HR in the epidural group significantly dropped. The reading of HR in the TEA group was statistically substantially lower than the reading in the ESPB group, according to Seleem et al. (P = 0.001).17 But according to Elsabeeny et al.18, HR values were comparable between the TEA and ESPB groups throughout the intraoperative time frame, with the exception of around 105 min, when recorded values for the ESPB group were greater than the ESPB and TEA groups.
This discrepancy may be attributed to the fact that we injected 20 ml while they used 30 ml of bupivacaine for the ESPB procedure and that we injected 10 ml while they employed 7.5 ml for the TEA process.
In our study, intraoperative MAP in the TEA group was substantially less than in the ESPB group prior to surgical incision, after surgical incision, at 30 min, 1 h and 1.5 h and was insignificantly different at baseline, 2 h, 2.5 h and between the two groups after the conclusion of operation. Similarly, Seleem et al.17 found that there was a statistically significant lower reading of MAP in TEA group than ESPB group (P < 0.001) Moreover, Elsabeeny et al.18 reported that at 60, 75, and 90 min into the procedure, the intraoperative MAP values for the TEA group were substantially lower than those for the SAPB and ESPB groups; in contrast to our findings, it was also significantly lower at 105, 135, and 150 min while it was not statistically different in our study.
The present investigation then found that ESPB had superior intraoperative hemodynamic stability than TEA.
In addition, we discovered that there was no discernible difference between the two groups in terms of intraoperative fentanyl intake. According to Nagaraja et al.19 their outcomes concur with ours in that there was no appreciable difference in the intraoperative fentanyl usage between TEA and ESPB patients. Elsabeeny et al.18 additionally discovered that no patients in the TEA group required intraoperative rescue fentanyl, whereas only two patients in the ESPB group and five patients in the SAPB group, respectively, received it (P = 0.043). Controversially, Seleem et al. asserted that ESPB utilized considerably more intraoperative fentanyl than TEA.17
During postoperative period, the present study showed that postoperative HR was insignificantly different between both groups except at 6 h and 12 h that was considerably greater in the ESPB group than in the TEA group. In agreement with our results, El-Sherbiny et al.20 showed that, according to the HR, no statistical significance was found between the groups under study. However, after 6 and 12 h, we noticed greater HR in the ESPB group compared to the TEA group, which may have been caused by the decreased infusion rate in the ESPB group. Elsabeeny et al.18 reported controversially that ESPB and SAPB levels were in excess of in the TEA group, however we only detected after 6 and 12 h after surgery, and there were substantial variances in HR values. This variation between two studies could be as they performed the blocks in higher levels in TEA (T6-7) and ESPB (T5) groups. Also, Moharam et al.21 found that as regards HR; there was an early significant increase in group TEA compared to ESPB group at 4, 6, and 12 h postoperatively. The noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot.
In our study, postoperative MAP was insignificantly different between both groups except considerably higher in the ESPB group compared to TEA group at 6 and 12 h.
In line with our findings, Elsabeeny et al.18 identified substantial decreased MAP values for the TEA group during the length of the postoperative period. The TEA and ESPB groups' MAP values at 24 h were comparable. Nevertheless, Seleem et al.17 found that MAP was substantially greater in the TEA group compared to the ESPB group at 8, 12, and 24 h afterwards (P = 0.028, 0.001, and 0.003, correspondingly). This variation between two studies could be explained as we performed a continuous ESPB, but their block was single shot.
The rest and mobility scores were not statistically distinct between the two groups, with the exception of 6 and 12 h, when the NRS ratings in our research were substantially greater in the ESPB group compared to the TEA group.
There was no difference in significance in the VAS ratings between the research groups, according to EL-Sherbiny et al.20, who agreed with our findings, although we did note only at 6 and 12 h did the ESPB group outperform the TEA group in terms of VAS scores (P = 0.001 and 0.043, correspondingly), that may be associated to the ESPB group's lesser infusion rate. Also, Elsabeeny et al.18 study, as their results showed that VAS scores at rest were significantly lower in the TEA group at the post-anesthesia care unit and 24 h compared to ESPB. Our results disagree with Moharam et al.21 noted an early increase in VAS in TEA group at 4, 6, and 12 h postoperatively compared to ESPB group. The noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot. In addition, Seleem et al.17 recorded that At 2, 4, 8, and 12 h after surgery, the TEA group's VAS scores were considerably greater than those of the ESPB group (P < 0.001). This variation between two studies could be as they performed the blocks in higher levels in TEA and ESPB groups (T4) and single shot.
In our study, in comparison to the TEA group, the total amount of morphine consumed, the number of patients who required morphine, and the total amount of bupivacaine consumed were all considerably greater in the ESPB group.
Similar to this, Elsabeeny et al.18 observed that a substantial fraction of participants in the ESPB group (47.1%) required morphine, but none of the TEA group's patients needed it (P < 0.001). Our findings are not in line with Moharam et al.21 who reported that meperidine consumption in the 1st 24h showed TEA group consumed more than ESPB group did (P < 0.001). The noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot.
In our study, the ESPB group's initial rescue analgesia time was noticeably shorter than that of the TEA group. Contrary to our findings, Elsabeeny et al.18 discovered that it took the ESPB group longer than the TEA group to get morphine for the first time (P = 0.001). Noted variation between both studies could be as they performed higher infusion rate (8-10 ml/h) in ESPB group from start. Also, Moharam et al.21 observed different results as TEA group had earlier analgesic need than ESPB group did (P < 0.001). Noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot. EL-Sherbiny et al.20 stated that the time of the first analgesic request was comparable between TEA and ESPB groups without recorded statistical significance (P > 0.05).
In our study, there was no appreciable distinction between the two groups' side effects. Our findings are consistent with those of Elsabeeny et al.18, who found that two reported cases of postoperative nausea in the TEA group and one incidence of postoperative nausea in the ESPB group both spontaneously vanished. No issues with the epidural insertion or the ESPB were found. According to Moharam et al.21, a substantial distinction between the TEA group and ESPB group was observed in the early incidence of intraoperative hypotension and bradycardia at 30 min.
The sympatholytic impact of the epidural injection can be used to explain why the TEA group had a substantially greater incidence of hypotension. This followed in the same line as Khalil et al.22 reported that the TEA group had hypotension noticeably more frequently. According to Singh et al.23, hypotension was noticeably more common in the TEA group.
We suggest that ESPB can be used as a helpful alternative to thoracic epidural in patients undergoing open nephrectomy, providing a nearly identical analgesic profile and having fewer adverse effects, provided that the ESPB group's infusion rate is raised. In line with our findings, Nagaraja et al.19 shown that bilateral ESPB may be utilized as a successful substitute for thoracic epidural in the management of perioperative pain, with similar postoperative pain ratings. Additionally, Munoz et al.24 brought out that ESPB appeared to be a viable thoracic epidural substitution with a broader safe record.
The study has limitations, such as its single center design and limited sampling size, short follow up (24 hrs.) and the absence of chronic pain assessment, double blind study that both groups had the same bupivacaine infusion rate. We recommend future larger randomized clinical trials with longer postoperative follow up to confirm our findings and future studies to assess and compare chronic pain after both blocks (TEA and ESPB), we should increase bupivacaine infusion rate of ESPB group to be effective as TEA group.
The US guided ESPB is effective in providing analgesia, lowering the use of opioids during surgery and thereafter in patients having open nephrectomy. However, it is still inferior to TEA in terms of pain control after 6 h postoperatively. Otherwise, ESPB has fewer side effects compared to TEA. So, it may be an efficient alternative to TEA.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
The authors declare no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
All authors took part in the conduct of the study, collection of data, literature search and manuscript preparation.
Author affiliations:
- Mohamed A. Wadood, Lecturer, Anesthesia, ICU & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; E-mail: m_wadod@yahoo.com; ORCID: {0000-0002-1952-5849}
- Mahmoud Abdelgalil Abdelrahman, Lecturer, Anesthesia, ICU & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; E-mail: mahmoud.abdelgilil@nci.cu.edu.eg
- Mamdouh Mahmoud Mostafe, Lecturer, Anesthesia, ICU & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; E-mail: mamdouh.mahmoud@nci.cu.edu.eg
- Ekramy Mansour Abdelghafar, Professor of Anesthesia, ICU & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; E-mail: Ekrameymansoure@yahoo.com
- Reham Mohamed Gamal, Lecturer, Anesthesia, ICU & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; E-mail: rehamgamal_nci@hotmail.com; ORCID: {0000-0003-2865-8122}
ABSTRACT
Background & objective: Pain during nephrectomy has been reported to be extremely intense and may trigger complex biochemical and physiological stress response if managed inadequately. Erector spinae plane block (ESPB) and thoracic epidural analgesia (TEA) both have been advocated for pain management in adult patients undergoing open nephrectomy under general anesthesia. We compared the efficacy and the dynamics of both of these procedures.
Methodology: This was a randomized, double-blinded, controlled trial involving 54 patients were undergoing open nephrectomy for malignant kidney tumors. All patients were ASA class II, had a BMI 20-40 kg/m2, and were between the ages of 18-65 y. Through random assignment, people were divided into two identical, equivalent groups: Group A (n = 27) received TEA, whereas Group B (n = 27) received US-guided continuous ESPB. Mean arterial pressure (MAP) and intraoperative heart rate (HR) were recorded before and after incision, and at 30 min, 1 h, and 1.5 h. Postoperative HR, MAP were recorded at 6 h and 12 h, both at rest and when moving. Numerical rating scale (NRS) score was used to compare the intensity of postoperative pain.
Results: Postoperative HR, MAP, at 6 h and 12 h, at rest and when moving, were substantially reduced in the TEA group than those in the ESPB group. The NRS score of the ESPB group was substantially greater than that of the TEA group. In contrast to the TEA group, much more total amount of morphine was consumed in the ESPB group. The time to first rescue analgesia was substantially shorter in ESPB group than that of the TEA group.
Conclusions: The results of our study prove that US guided erector spinae plane block is effective in providing postoperative analgesia, decreasing use of intraoperative and postoperative opioids in patients having open nephrectomy. However, it is still inferior to thoracic epidural analgesia in terms of pain control after 6 h postoperatively. Otherwise, erector spinae plane block has fewer side effects compared to thoracic epidural analgesia. So, it may be used as an alternative to thoracic epidural analgesia.
Key words: Erector Spinae Plane Block; Epidural Analgesia; Open Nephrectomy; Pain, Postoperative; Ultrasound
Citation: Wadood MA, Abdelrahman MA, Mostafe MM, Abdelghafar EM. Ultrasound-guided continuous erector spinae plane block versus thoracic epidural analgesia in open nephrectomy for renal malignancy: a randomized controlled study, Anaesth. pain intensive care 2024;28(1):26-32; DOI: 10.35975/apic.v28i1.2377
Received July 24, 2023; Revised: September 08, 2023; Accepted: October 03, 2023
1. INTRODUCTION
Renal cell carcinoma (RCC) is the third most prevalent cancer of the genitourinary tract and makes up between 2% -3% of all malignancies.1 The acknowledged curative procedure for resectable kidney tumors for many years has been open nephrectomy. Nephrectomy-related pain is well-known to be quite intense and to result in severe biochemical and physiological stress. Therefore, effective treatment of initial postoperative pain is crucial for the patient satisfaction.2 Opioids have been the most effective medication for treating postoperative pain, but using them in high doses can have negative side effects.3 Hence substitutes to opioids are advised for effective analgesia.
The cornerstone of the peri-operative treatment for abdominal procedures, delivering the most effective analgesia, is thought to be thoracic epidural analgesia (TEA). However, TEA has been linked to major side effects such as hypotension, urine retention, decreased lower limb motor function, injury to the spinal cord, breathing problems brought on by the use of opioids, dural puncture with a needle or catheter, and headache following a dural puncture.4
The erector spinae plane block (ESPB) was initially shown to be utilized for treating long-term thoracic neuropathic discomfort by injecting local anesthetic into the erector spinae muscle plane (ESP) at the level of T5.5 It is reasonably easy procedure to carry out, with end points for the insertion of needles and for the application of local anesthetic and plainly discernible sonographic markers.5 It has been applied both in thoracic and abdominal surgeries with high success rates providing both visceral and somatic analgesia. 5, 6 ESPB can provide sensory block in the distribution area from T2-T4 to L1–L2.5, 6
ESPB is regarded to be theoretically simpler, even though it can offer a block that is identical to the paravertebral block, given that the needle is oriented away from the pleura, thus reducing the possibility of the block related complications, e.g., pneumothorax.7 In addition, it is likely to be safe in patients with suboptimal coagulation status. It has a lesser risk of blood vessel or injury to the brain than an epidural or a paravertebral block.8
In order to visualize and identify the normal and unusual positions of nerves, blood vessels, ultrasound (US) imaging is utilized to deposit and disseminate local anesthetics (LA) in the appropriate plane and around the intended nerve/s while the needle is passed through the tissues.9
We compared ESPB and TEA blocks for their efficacy in pain relief following surgery of adult individuals undergoing open nephrectomy under general anesthesia.
2. METHODOLOGY
This randomized, double-blinded, controlled study was conducted at the National Cancer Institute and comprised 54 patients with malignant kidney tumors, ASA class II, ages 18-65 y, Body Mass Index (BMI) 20-40 kg/m2, scheduled for open nephrectomy under general anesthesia.
All patients gave their informed written consent. Approval of institutional ethics committee was secured.
The exclusion criteria included, an infection at the puncture site, coagulopathies with a platelet count below 100,000 or an INR of greater than 1.3, renal and hepatic insufficiency, unsteady heart disease, a history of psychiatric and cognitive disorders, patients allergic to the drugs to be used, and inappropriate anatomy of the thoracic region.
By random selection, the patients were split into two just comparable groups: Group A (n = 27) got continuous TEA, whereas Group B (n = 27) received continuous ESPB that was US-guided.
Every patient had a thorough history review, physical examination, and standard laboratory tests.
2.1. Group A (TEA)
Skin infiltration with 3 ml of lidocaine 2% was performed with the patient seated and under complete aseptic conditions. The epidural space was located using the loss of resistance technique at the T8 interspace with an 18-G Tuohy needle and a 20-G catheter (Perifix, Braun, Germany) was then advanced 3 cm. To check for inadvertent intrathecal or IV delivery, a test dose of 3 ml of lidocaine 2% with epinephrine in 1:200,000 was given. After a negative response, 10 ml of 0.25% bupivacaine was injected as a bolus dose into the epidural catheter until general anesthesia begun. The patient was placed in the supine posture. The sensory block on the operated side was assessed by pinprick every two minutes in the midclavicular line. After 15 min, if the sensory block level was still below T5, another 5 ml of bupivacaine was given. The dose of bupivacaine 0.125% was then gradually increased over the course of 24 h, based on the pain score and negative consequences, rate modification.10, 11
2.2. Group B (ESPB)
While the patient was sitting, a high-frequency linear US transducer (Fujifilm Sonosite, Inc., Bothell, WA) was positioned in a longitudinal orientation 3 cm lateral to the T8 spinous process. This should draw attention to the three muscles that are superficial to the hyperechoic transverse process shadow: the trapezius, rhomboid major, and erector spinae. To numb the skin, 3 ml of lidocaine 2% was used. An 18-G Tuohy needle with a 20-G catheter (Perifix, Braun, Germany) was placed in-plane and cephalad-to-caudad on the deep (anterior) side of the ESM, 30 min before to the induction of general anesthesia, and 20 ml of 0.25% bupivacaine was administered as a bolus dose in the epidural catheter. The patient was then shifted to the supine position. The sensory block on the operated side was assessed with pinprick every two minutes in the midclavicular line. After 15 min, if the sensory block level was still below T5, another 5 ml of bupivacaine was given. Following the skin incision, bupivacaine 0.125% was constantly infused at a rate of 6 ml/h, and the dosage was boosted by 2 ml/h increments up to 10 ml/h for 24 h. Customizing rates according to the pain score and adverse effects.12-14 Patients with failed block were excluded.
The identical approach was used to provide general anesthesia to each patient. Rocuronium 0.5 mg/kg, fentanyl 1 g/kg IV, and propofol 2 mg/kg were used to induce anesthesia and endotracheal intubation secured. Isoflurane with MAC 1.2% was used to maintain anesthesia in a mixture of 50% air and oxygen.
After two hours of supervision in the postoperative care unit, the patients got rescue analgesia in the form of IV morphine 3 mg boluses. Every patient's total dose of morphine over the course of a day was noted. The patients were then moved to a ward and given 1 g of paracetamol IV every 8 h.
The primary outcome parameter was the total amount of morphine taken in the preceding 24 h, and the secondary outcome variables included the total amount of fentanyl used during surgery, the time at which the first rescue analgesic was given, and pain as assessed by the Numerical Rating Scale (NRS), both at rest and while moving. NRS was used to measure pain ratings in the PACU and for the following 24 h (1, 2, 4, 6, 12 and 24 h) following surgery. Before the LA injection, mean arterial pressure (MAP) and heart rate (HR) were measured to establish a baseline value. After the LA injection, follow-up readings were taken promptly before and after the surgical incision as well as at 30-min intervals through the operation. The consumption of the entire amount of bupivacaine and the occurrence of adverse reactions, such as hemodynamic instability, nausea, vomiting, dural puncture, post dural puncture headache, failed block, unintentional intravascular injection of LA, and local anesthetic toxicity were noted (NRS scores 1-3: mild discomfort, 4-6: moderate pain, and 7-10: severe discomfort).
Postoperative nausea / vomiting (PONV) was assessed on a four-point verbal scale (none = no nausea, mild = little nausea but no vomiting, moderate = one occurrence of vomiting, severe = many bouts of vomiting).15 Patients with mild to severe PONV received an IV dose of ondansetron 0.1 mg/kg.
2.3. Statistical analysis
IBM, Chicago, Illinois, USA's SPSS v27 was used for the statistical analysis. The Shapiro-Wilks test and histograms were utilized to figure out if the data distribution was normal. Quantitative parametric data including mean and standard deviation (SD) were analyzed using an unpaired student t-test. Interquartile range (IQR) and the median were used to report and assess quantitative non-parametric data, respectively. When applicable, qualitative variables were investigated utilizing the Chi-square test or Fisher's exact test and offered as frequency and percentage (%). Statistical reliability was known as a two tailed P ≤ 0.05.
3. RESULTS
We enrolled 79 participants out of which 21 did not match the qualifying requirements for this study, while 4 patients declined to take part. The remainder of fifty-four individuals were split randomly into two groups of 27 each. One patient dropped out in group A due to dural puncture, and two patients dropped out in group, one due to block failure and the other due to massive blood loss.
Fifty-one patients were monitored and studied statistically (Figure 2).
The demographic information of the participants and the duration of the procedure were not statistically different between the two groups (Table 1).
| Table 1: Demographic data comparison for both groups | |||
| Variable | Group A
(n = 26) |
Group B
(n = 25) |
P value |
| Age (y) | 56.31 ± 5.99 | 54.24 ± 6.81 | 0.254 |
| Sex | 19 (73.08) | 17 (68) | 0.660 |
| Weight (kg) | 76.67 ± 13.96 | 75 ± 15.48 | 0.687 |
| Height (m) | 1.59 ± 0.08 | 1.56 ± 0.06 | 0.070 |
| BMI (kg/m2) | 30.29 ± 5.4 | 30.87 ± 5.6 | 0.703 |
| Duration of surgery (min) | 174.96 ± 18.52 | 175.6 ± 37.61 | 0.894 |
| .The data are shown as mean ± SD or n (%); BMI - Body mass index | |||
Before the incision, in Group A patients intraoperative heart rate was substantially lower than that of Group B. After incision, at 30 min, 1 h, and 1.5 h heart rates were statistically equivalent (P = 0.030, 0.013, 0.034, 0.003 and 0.039 respectively) and was insignificantly different at baseline, 2 h, 2.5 h and between the two groups after the conclusion of operation. As compared to Group B, intraoperative MAP was significantly lower in Group A before surgical incision, after surgical incision, at 30 min, 1 h, and 1.5 h (P = 0.011, < 0.001, < 0.001, < 0.018, and < 0.001 respectively), but there was no difference between the two groups at baseline, 2 h, 2.5 h, or at the conclusion of surgery.
Postoperative HR was insignificantly different between both groups except at 6 h and 12 h, as ESPB group values were substantially higher than TEA group values (P = 0.001 and < 0.043, respectively), but the differences were statistically not significant. Except at 6 and 12 h, when the ESPB group's postoperative MAP was considerably higher than the TEA group's, there was no statistically significant difference between the two groups. (P < 0.001, 0.035 respectively)
With the exception of 6 and 12 h, when the ESPB group's NRS score was considerably higher than the TEA group's, there was no significant difference between the two groups' NRS scores during rest (P < 0.001) (Table 2).
NRS score at movement was insignificantly different between both groups except at 6 h and 12 h, when it was significantly higher in ESPB group contrasted to TEA group (P < 0.001 and 0.004) (Table 3).
In Groups A and B, the median (IQR) of total morphine intake was 0 (0-0) and 3 (0-3) respectively. In comparison to Group A, Group B had considerably greater total morphine consumption, number of patients who needed morphine, and total bupivacaine consumption. Group B experienced the first rescue analgesia earlier than Group A. In comparison to Group A, Group B had a substantially larger number of patients who needed a bolus of bupivacaine (P = 0.022). There was no significant difference in the amount of intraoperative fentanyl consumed between the two groups (Table 4).
PONV, hypotension, and dural puncture were side effects / complications and did not substantially differ between the two groups. Local anesthetic toxicity, respiratory depression, post-dural puncture headache, and inadvertent intravascular injection of LA did not happen in either group (Table 5).
| Table 2: NRS score changes at rest among each group | |||
| Time of recording | Group A
(n = 26) |
Group B
(n = 25) |
P value |
| PACU | 2 (1-3) | 2 (2-3) | 0.386 |
| 1 h | 2 (1-3) | 2 (1-2) | 0.140 |
| 2 h | 2 (1-2) | 2 (1-3) | 0.079 |
| 4 h | 1 (0.25-3) | 2 (1-3) | 0.330 |
| 6 h | 2 (1.25-3) | 3 (3-4) | < 0.001* |
| 12 h | 1 (0.25-2) | 3 (2-3) | < 0.001* |
| 24 h | 1 (0-2) | 1 (1-3) | 0.133 |
| Data are provided as medians (IQR), with P < 0.05 indicating significance.
PACU - post-anesthesia care unit. |
|||
| Table 3: NRS score changes at movement in both groups | |||
| Time of recording | Group A
(n = 26) |
Group B
(n = 25) |
P value |
| PACU | 3 (2-3) | 3 (3-3) | 0.271 |
| 1 h | 2 (2-3) | 3 (2-3) | 0.284 |
| 2 h | 2 (1-3) | 2 (2-3) | 0.601 |
| 4 h | 2.5 (1.25-3) | 2 (1-2) | 0.188 |
| 6 h | 3 (2-3) | 3 (3-6) | < 0.001* |
| 12 h | 3 (2-3) | 3 (3-3) | 0.004* |
| 24 h | 2 (0-2.75) | 2 (1-2) | 0.503 |
| Data given as n (IQR); PACU - post-anesthesia care unit; * P < 0.05 is significant | |||
| Table 4: Bupivacaine, fentanyl and morphine consumption between each group | |||
| Parameter | Group A
(n = 26) |
Group B
(n = 25) |
P value |
| Patients required preop bolus bupivacaine | 0 (0.0%) | 5 (20.00%) | 0.022* |
| Patients required intraop fentanyl | 0 (0.0%) | 2 (8%) | 0.235 |
| Intraop fentanyl consumption (μg) | 75 ± 16.79 | 66.8 ± 22.86 | 0.150 |
| Patients required postop morphine (number) | 2 (7.4%) | 15 (55.6%) | < 0.001* |
| Time of first rescue analgesia (h) | 17 (16.5-17.5) | 6 (6-8) | 0.014* |
| Total morphine consumption in 1st 24 h postop (mg) | 0 (0-0) | 3 (0-3) | 0.002* |
| Total bupivacaine consumption in 1st 24 h postop (ml) | 147.23 ± 11.43 | 191.36 ± 25.76 | < 0.001* |
| Data reported as n (%), mean ± standard deviation, or median (IQR), with * P < 0.05 is significant | |||
4. DISCUSSION
During the intra-operative period, our results showed that before the incision, intraoperative HR in the TEA group was considerably lower than it was in the ESPB group, and was insignificantly different at baseline, 2 h, 2.5 h and after the conclusion of the procedure in both groups. These results are consistent with that of Moawad, et al.16 as at 2, 2½, 3, and 3½ h into the operation, compared to the PVB group, the HR in the epidural group significantly dropped. The reading of HR in the TEA group was statistically substantially lower than the reading in the ESPB group, according to Seleem et al. (P = 0.001).17 But according to Elsabeeny et al.18, HR values were comparable between the TEA and ESPB groups throughout the intraoperative time frame, with the exception of around 105 min, when recorded values for the ESPB group were greater than the ESPB and TEA groups.
This discrepancy may be attributed to the fact that we injected 20 ml while they used 30 ml of bupivacaine for the ESPB procedure and that we injected 10 ml while they employed 7.5 ml for the TEA process.
In our study, intraoperative MAP in the TEA group was substantially less than in the ESPB group prior to surgical incision, after surgical incision, at 30 min, 1 h and 1.5 h and was insignificantly different at baseline, 2 h, 2.5 h and between the two groups after the conclusion of operation. Similarly, Seleem et al.17 found that there was a statistically significant lower reading of MAP in TEA group than ESPB group (P < 0.001) Moreover, Elsabeeny et al.18 reported that at 60, 75, and 90 min into the procedure, the intraoperative MAP values for the TEA group were substantially lower than those for the SAPB and ESPB groups; in contrast to our findings, it was also significantly lower at 105, 135, and 150 min while it was not statistically different in our study.
The present investigation then found that ESPB had superior intraoperative hemodynamic stability than TEA.
| Table 5: Comparative side effects / complications between the two groups. Data given as n (%) | |||
| Side effect / complication | Group A
(n = 26) |
Group B
(n = 25) |
P value |
| PONV | 3 (11.54) | 6 (24) | 0.465 |
| Hypotension | 4 (15.38) | 1 (4) | 0.349 |
| Dural puncture | 1 (4.0) | 0 (0.0) | 1.000 |
| Post dural puncture headache | 0 (0.0) | --- | --- |
| Intravascular injection of LA | 0 (0.0) | 0 (0.0) | --- |
| Local anesthetic toxicity | 0 (0.0) | 0 (0.0) | --- |
| Respiratory depression | 0 (0.0) | 0 (0.0) | --- |
In addition, we discovered that there was no discernible difference between the two groups in terms of intraoperative fentanyl intake. According to Nagaraja et al.19 their outcomes concur with ours in that there was no appreciable difference in the intraoperative fentanyl usage between TEA and ESPB patients. Elsabeeny et al.18 additionally discovered that no patients in the TEA group required intraoperative rescue fentanyl, whereas only two patients in the ESPB group and five patients in the SAPB group, respectively, received it (P = 0.043). Controversially, Seleem et al. asserted that ESPB utilized considerably more intraoperative fentanyl than TEA.17
During postoperative period, the present study showed that postoperative HR was insignificantly different between both groups except at 6 h and 12 h that was considerably greater in the ESPB group than in the TEA group. In agreement with our results, El-Sherbiny et al.20 showed that, according to the HR, no statistical significance was found between the groups under study. However, after 6 and 12 h, we noticed greater HR in the ESPB group compared to the TEA group, which may have been caused by the decreased infusion rate in the ESPB group. Elsabeeny et al.18 reported controversially that ESPB and SAPB levels were in excess of in the TEA group, however we only detected after 6 and 12 h after surgery, and there were substantial variances in HR values. This variation between two studies could be as they performed the blocks in higher levels in TEA (T6-7) and ESPB (T5) groups. Also, Moharam et al.21 found that as regards HR; there was an early significant increase in group TEA compared to ESPB group at 4, 6, and 12 h postoperatively. The noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot.
In our study, postoperative MAP was insignificantly different between both groups except considerably higher in the ESPB group compared to TEA group at 6 and 12 h.
In line with our findings, Elsabeeny et al.18 identified substantial decreased MAP values for the TEA group during the length of the postoperative period. The TEA and ESPB groups' MAP values at 24 h were comparable. Nevertheless, Seleem et al.17 found that MAP was substantially greater in the TEA group compared to the ESPB group at 8, 12, and 24 h afterwards (P = 0.028, 0.001, and 0.003, correspondingly). This variation between two studies could be explained as we performed a continuous ESPB, but their block was single shot.
The rest and mobility scores were not statistically distinct between the two groups, with the exception of 6 and 12 h, when the NRS ratings in our research were substantially greater in the ESPB group compared to the TEA group.
There was no difference in significance in the VAS ratings between the research groups, according to EL-Sherbiny et al.20, who agreed with our findings, although we did note only at 6 and 12 h did the ESPB group outperform the TEA group in terms of VAS scores (P = 0.001 and 0.043, correspondingly), that may be associated to the ESPB group's lesser infusion rate. Also, Elsabeeny et al.18 study, as their results showed that VAS scores at rest were significantly lower in the TEA group at the post-anesthesia care unit and 24 h compared to ESPB. Our results disagree with Moharam et al.21 noted an early increase in VAS in TEA group at 4, 6, and 12 h postoperatively compared to ESPB group. The noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot. In addition, Seleem et al.17 recorded that At 2, 4, 8, and 12 h after surgery, the TEA group's VAS scores were considerably greater than those of the ESPB group (P < 0.001). This variation between two studies could be as they performed the blocks in higher levels in TEA and ESPB groups (T4) and single shot.
In our study, in comparison to the TEA group, the total amount of morphine consumed, the number of patients who required morphine, and the total amount of bupivacaine consumed were all considerably greater in the ESPB group.
Similar to this, Elsabeeny et al.18 observed that a substantial fraction of participants in the ESPB group (47.1%) required morphine, but none of the TEA group's patients needed it (P < 0.001). Our findings are not in line with Moharam et al.21 who reported that meperidine consumption in the 1st 24h showed TEA group consumed more than ESPB group did (P < 0.001). The noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot.
In our study, the ESPB group's initial rescue analgesia time was noticeably shorter than that of the TEA group. Contrary to our findings, Elsabeeny et al.18 discovered that it took the ESPB group longer than the TEA group to get morphine for the first time (P = 0.001). Noted variation between both studies could be as they performed higher infusion rate (8-10 ml/h) in ESPB group from start. Also, Moharam et al.21 observed different results as TEA group had earlier analgesic need than ESPB group did (P < 0.001). Noted variation between both studies could be as we performed a continuous ESPB, but their block was single shot. EL-Sherbiny et al.20 stated that the time of the first analgesic request was comparable between TEA and ESPB groups without recorded statistical significance (P > 0.05).
In our study, there was no appreciable distinction between the two groups' side effects. Our findings are consistent with those of Elsabeeny et al.18, who found that two reported cases of postoperative nausea in the TEA group and one incidence of postoperative nausea in the ESPB group both spontaneously vanished. No issues with the epidural insertion or the ESPB were found. According to Moharam et al.21, a substantial distinction between the TEA group and ESPB group was observed in the early incidence of intraoperative hypotension and bradycardia at 30 min.
The sympatholytic impact of the epidural injection can be used to explain why the TEA group had a substantially greater incidence of hypotension. This followed in the same line as Khalil et al.22 reported that the TEA group had hypotension noticeably more frequently. According to Singh et al.23, hypotension was noticeably more common in the TEA group.
We suggest that ESPB can be used as a helpful alternative to thoracic epidural in patients undergoing open nephrectomy, providing a nearly identical analgesic profile and having fewer adverse effects, provided that the ESPB group's infusion rate is raised. In line with our findings, Nagaraja et al.19 shown that bilateral ESPB may be utilized as a successful substitute for thoracic epidural in the management of perioperative pain, with similar postoperative pain ratings. Additionally, Munoz et al.24 brought out that ESPB appeared to be a viable thoracic epidural substitution with a broader safe record.
5. LIMITATIONS
The study has limitations, such as its single center design and limited sampling size, short follow up (24 hrs.) and the absence of chronic pain assessment, double blind study that both groups had the same bupivacaine infusion rate. We recommend future larger randomized clinical trials with longer postoperative follow up to confirm our findings and future studies to assess and compare chronic pain after both blocks (TEA and ESPB), we should increase bupivacaine infusion rate of ESPB group to be effective as TEA group.
6. CONCLUSION
The US guided ESPB is effective in providing analgesia, lowering the use of opioids during surgery and thereafter in patients having open nephrectomy. However, it is still inferior to TEA in terms of pain control after 6 h postoperatively. Otherwise, ESPB has fewer side effects compared to TEA. So, it may be an efficient alternative to TEA.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
The authors declare no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
All authors took part in the conduct of the study, collection of data, literature search and manuscript preparation.
11. REFERENCES
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71-96. [PubMed] DOI: 3322/CA.2007.0010
- Perkins FM, Kehlet H. Chronic pain as an outcome of surgery. A review of predictive factors. Anesthesiology. 2000;93:1123-33. [PubMed] DOI: 1097/00000542-200010000-00038
- Randerath WJ, George S. Opioid-induced sleep apnea: is it a real problem? J Clin Sleep Med. 2012;8:577-8. [PubMed] DOI: 5664/jcsm.2162
- Royse C, Royse A, Soeding P, Blake D, Pang J. Prospective randomized trial of high thoracic epidural analgesia for coronary artery bypass surgery. Ann Thorac Surg. 2003;75:93-100. [PubMed] DOI: 1016/s0003-4975(02)04074-2
- Forero M, Rajarathinam M, Adhikary S, Chin KJ. Continuous erector spinae plane block for rescue analgesia in thoracotomy after epidural failure: a case report. A A Case Rep. 2017;8:254-6. [PubMed] DOI: 1213/XAA.0000000000000478
- Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: A report of 3 cases. Reg Anesth Pain Med. 2017;42:372-6. [PubMed] DOI: 1097/AAP.0000000000000581
- Tulgar S, Balaban O. Local anaesthetic injection point of erector spinae plane block. Indian J Anaesth. 2018;62:403-4. [PubMed] DOI: 4103/ija.IJA_200_18
- Hamilton DL, Manickam B. The erector spinae plane block. Reg Anesth Pain Med. 2017;42:276-80. [PubMed] DOI: 1097/AAP.0000000000000565
- Marhofer P, Willschke H, Kettner S. Current concepts and future trends in ultrasound-guided regional anesthesia. Curr Opin Anaesthesiol. 2010;23:632-6. [PubMed] DOI: 1097/ACO.0b013e32833e2891
- Ahmed FI. Continuous spinal versus continuous thoracic epidural anesthesia for major abdominal surgery in patients with chronic obstructive pulmonary disease. Res Opin Anesth Intensive Care. 2019;6:362-9. [FreeFullText]
- Aditianingsih D, Anasy N, Tantri AR, Mochtar CA. A randomized controlled trial on analgesic effect of repeated Quadratus Lumborum block versus continuous epidural analgesia following laparoscopic nephrectomy. BMC Anesthesiol. 2019;19:221. [PubMed] DOI: 1186/s12871-019-0891-7
- Restrepo-Garces CE, Chin KJ, Suarez P, Diaz A. Bilateral continuous erector spinae plane block contributes to effective postoperative analgesia after major open abdominal surgery: A case report. A A Case Rep. 2017;9:319-21. [PubMed] DOI: 1213/XAA.0000000000000605
- Piangatelli C, Dalla Bona E, Tavoletti D, Rosanò E, Mocchegiani F, Vivarelli M, et al. Continuous erector spinae plane block for pain management in laparoscopic liver resection: case report. Rev Esp Anestesiol Reanim. 2020;48:164-8. DOI: 1097/CJ9.0000000000000167
- Altıparmak B, Korkmaz Toker M, Uysal AI, Kuşçu Y, Gümüş Demirbilek S. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: Randomized, controlled trial. J Clin Anesth. 2019;57:31-6. [PubMed] DOI: 1016/j.jclinane.2019.03.012
- Apfel CC, Kranke P, Eberhart LH, Roos A, Roewer N. Comparison of predictive models for postoperative nausea and vomiting. Br J Anaesth. 2002;88:234-40. [PubMed] DOI: 1093/bja/88.2.234
- Moawad HE, Mousa SA, El-Hefnawy AS. Single-dose paravertebral blockade versus epidural blockade for pain relief after open renal surgery: A prospective randomized study. Saudi J Anaesth. 2013;7:61-7. [PubMed] DOI: 4103/1658-354X.109814
- Seleem MR, Hammad RA, Sultan SS, Sayed MA, Fahmy NG. Comparison between erector spinae plane block and thoracic epidural in breast cancer surgeries under general anesthesia. Egypti J Surg. 2022;41:456-62. [FreeFullText]
- Elsabeeny WY, Ibrahim MA, Shehab NN, Mohamed A, Wadod MA. Serratus anterior plane block and erector spinae plane block versus thoracic epidural analgesia for perioperative thoracotomy pain control: A randomized controlled study. J Cardiothorac Vasc Anesth. 2021;35:2928-36. [PubMed] DOI: 1053/j.jvca.2020.12.047
- Nagaraja PS, Ragavendran S, Singh NG, Asai O, Bhavya G, Manjunath N, et al. Comparison of continuous thoracic epidural analgesia with bilateral erector spinae plane block for perioperative pain management in cardiac surgery. Ann Card Anaesth. 2018;21:323-7. [PubMed] DOI: 4103/aca.ACA_16_18
- El-Sherbiny SM, Kamal RA, Elhadary IH, Abdallah MY. Erector spinae plane block versus thoracic epidural block as analgesic techniques for chest trauma: a randomized controlled trial. Res Opin Anesth Intensive Care. 2022;9:220-7. [FreeFullText]
- Moharam SA, Elkeblawy AM, Marouf HM, Elnoamany TM. Comparison of ultrasound guided thoracic erector spinae plane, thoracic paravertebral and thoracic epidural blocks for pain management after nephrectomy. J Adv Med Med Res. 2022:34(19):44-52. DOI: 9734/jammr/2022/v34i1931437
- Khalil AE, Abdallah NM, Bashandy GM, Kaddah TA. Ultrasound-guided serratus anterior plane block versus thoracic epidural analgesia for thoracotomy pain. J Cardiothorac Vasc Anesth. 2017;31:152-8. [PubMed] DOI: 1053/j.jvca.2016.08.023
- Singh S, Jacob M, Hasnain S, Krishnakumar M. Comparison between continuous thoracic epidural block and continuous thoracic paravertebral block in the management of thoracic trauma. Med J Armed Forces India. 2017;73:146-51. [PubMed] DOI: 1016/j.mjafi.2016.11.005
- Muñoz F, Cubillos J, Bonilla AJ, Chin KJ. Erector spinae plane block for postoperative analgesia in pediatric oncological thoracic surgery. Can J Anaesth. 2017;64:880-2. [PubMed] DOI: 1007/s12630-017-0894-0