Aditia Pria Laksana1*, Sidharta Kusuma Manggala2, Vera Irawany3
Author affiliations:
Blunt abdominal trauma is an event that can cause massive internal bleeding and can be life-threatening. Splenectomy is often performed to treat organ injuries in patients with blunt abdominal trauma. However, splenectomy can cause hemostasis problems, which can cause more bleeding and risk complications such as Acute Kidney Injury (AKI).
This case report aims to discuss the role of prothrombin complex concentrate (PCC) in treating bleeding and preventing AKI in blunt abdominal trauma patients after splenectomy at Fatmawati Hospital, Jakarta, Indonesia.
A 15-year-old woman experienced blunt abdominal trauma due to a sports accident and sustained internal bleeding. After a thorough evaluation, she underwent an emergency splenectomy to stop the bleeding. However, patients developed hemostasis problem which made the control of postoperative bleeding difficult. To overcome this problem, patient was administered PCC intravenously, which resulted in significant improvement in controlling postoperative bleeding. The hematocrit level and red blood cell count steadily increased, indicating the effectiveness of PCC in improving the patient's hemostasis.
PCC can play an important role in treating post-splenectomy bleeding in patients with blunt abdominal trauma. Apart from that, the use of PCC can also help prevent AKI, which is a serious and life-threatening complication. Further research and clinical trials are needed to confirm the benefits of using PCC in a broader patient population with similar conditions.
Abbreviations: AKI- Acute Kidney Injury; PCC- Prothrombin Complex Concentrate
Keywords: Acute Kidney Injury; Bleeding; Blunt Abdominal Trauma; Prothrombin Complex Concentrate; Splenectomy
Citation: Laksana AP, Manggala SK, Irawany V. The role of prothrombin complex concentrate to control critical bleeding after splenectomy for blunt abdominal trauma; A case report. Anaesth. pain intensive care 2024;28(1):177−181; DOI: 10.35975/apic.v28i1.2289
Received: September 13, 2023; Reviewed: October 29, 2023; Accepted: December 19, 2023
Blunt abdominal trauma is a serious injury that can cause internal bleeding and be life-threatening. Blunt abdominal trauma can be caused by various events, such as traffic accidents, sports accidents, or hard physical impacts. 1 It generally affects important organs in the abdominal cavity, including the spleen, liver, pancreas, and kidneys. In some cases of severe blunt abdominal trauma, surgery may be necessary to stop bleeding and treat organ damage. 2 One of the surgical procedures commonly performed to treat blunt abdominal trauma is splenectomy. A spleen damaged by trauma often causes heavy bleeding and requires immediate action to avoid more serious complications. One of the complications that can occur after splenectomy is disruption of the blood coagulation system, which can cause hemostasis problems and make it difficult to control bleeding.3 This condition is a serious concern because it can result in significant blood loss and risks causing problems with circulation of the vital organs including the kidneys. 4–6
Acute Kidney Injury (AKI), or acute kidney damage, is a serious complication that can occur in trauma patients with heavy bleeding. Prolonged bleeding can cause renal hypoperfusion, which reduces blood flow to the kidneys and results in damage to the renal cells. If not treated quickly and appropriately, AKI can cause potentially life-threatening kidney failure. Anemia and AKI are both important health problems because they are associated with morbidity and mortality.4–6 AKI increases depending on the decrease in hemoglobin levels and the ideal hemoglobin threshold associated with an increased risk of AKI is 10.5 g/dL. In a normal physiological response, the kidneys receive approximately 20-25 percent of the blood from cardiac output. This is the highest requirement in the entire body concerning the weight of the organ. As a pathological response, anemia directly reduces oxygen delivery. Because AKI often develops in ischemic conditions, anemia may be one of the causes of the high incidence of AKI in hospitalized patients. Patients with anemia and AKI had a higher risk of death than the peer group. This may be because anemia and AKI exacerbate organ dysfunction or delay organ recovery. 4–6 Current ICU outcomes remain suboptimal. Therefore, it is important to monitor these two conditions in patients admitted to the ICU and patients who survive the ICU.4–6 Future follow-up studies will evaluate the mechanisms underlying the association between anemia and AKI. Additionally, new data should reveal when to correct the anemia of critically ill patients to achieve personalized treatment approaches and better survival outcomes. Five million people per year (worldwide) die from traumatic injuries, 10-20% of which are potentially preventable. The biggest cause of preventable death is early bleeding within the first 6 hours after injury and delayed bleeding after more than 24 hours or within days. 4
In the treatment of blunt abdominal trauma after splenectomy with bleeding and risk of AKI, administration of prothrombin complex concentrate (PCC) has become one of the therapeutic options applied. PCC is a blood product that contains blood clotting factors, including factors II, VII, IX, and X, as well as proteins C and S. The use of PCC aims to improve hemostasis and stop bleeding. 4–6
This case study aims to evaluate the effectiveness and benefits of using PCC in patients with this condition. It is hoped that the results of this case report will provide guidance and a better understanding of the management of major bleeding and coagulopathy after trauma in the future.
The research subject was a 15-year-old lady who was treated at Fatmawati General Hospital, Jakarta with a diagnosis of blunt abdominal trauma. The patient suffered a serious injury due to a sports accident and experienced significant internal bleeding, necessitating a splenectomy as an emergency measure to treat spleen damage.
Data collected included patient demographic information, history of trauma and previous surgery, physical and laboratory examination results, radiology results (abdominal CT scan, renal ultrasonography), and surgical records during splenectomy. In addition, the data also included information of the blood removed during surgery and post-surgery, along with the interventions and therapies administered, including PCC.
After a thorough evaluation and confirmation of severe internal bleeding and significant splenic damage, the patient underwent an emergency splenectomy. During surgery, the patient experienced hemostasis problems requiring the use of PCC as part of therapy to control bleeding. Her serial blood parameters and blood gas analysis were done and the reports are reproduced as Table 1 and 2. Blood chemistry report ia reproduced as Table 3.
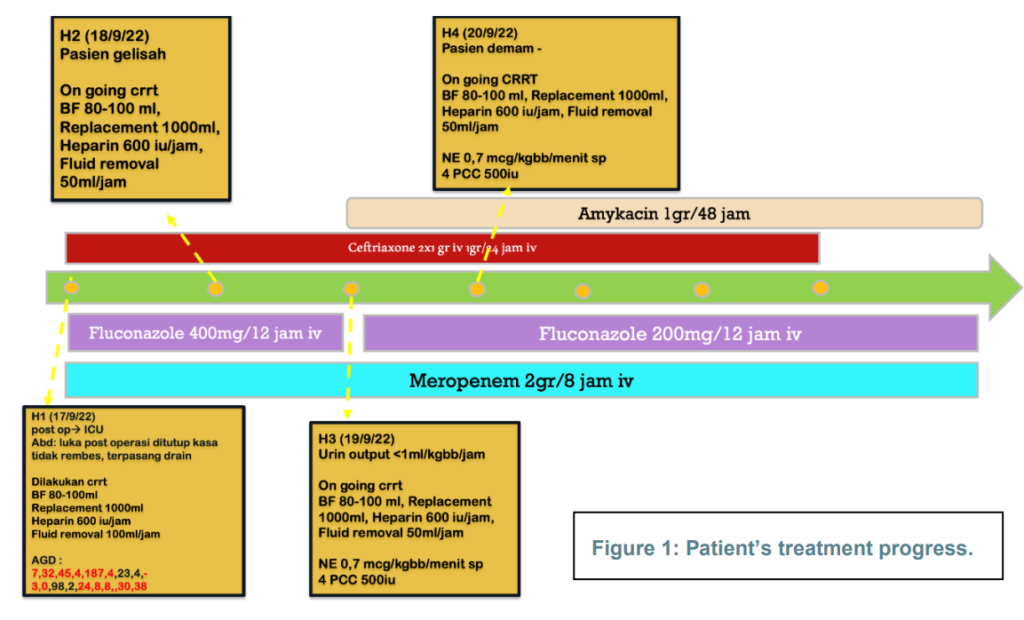
During surgery, the patient experienced hemostasis problems that made it difficult to control bleeding. To treat this condition, she was administered PCC intravenously as part of therapy to promote hemostasis and stop bleeding as per body weight, 500 iu at 3rd hour and repeated at 4th hour (Figure 1).
After administration of PCC, positive changes were noted in the patient's hematological parameters.
Hematocrit levels and red blood cell counts increased significantly, indicating the effectiveness of therapy in stopping bleeding and replacing blood components lost during surgery. The patient did not show any sign of excessive post-surgical bleeding after administration of PCC.
The patient received intensive care during the postoperative recovery period, including close monitoring of renal function and hemostasis status. She also received appropriate nutritional support and fluid therapy to facilitate the healing process. Apart from that, the medical team also provided education and psychosocial support to the patient and her family during the recovery period.
Handling blunt abdominal trauma after splenectomy with the risk of bleeding and AKI, is a complex challenge for the medical team.4 In this case report, we discussed the role of PCC in treating bleeding and preventing AKI in a 15-year-old female patient who suffered a serious injury due to a sports accident. This patient underwent splenectomy as an emergency measure to stop bleeding in the damaged spleen. After surgery, the patient experienced hemostasis problems requiring the administration of PCC as adjuvant therapy to stop bleeding and prevent complications of AKI.
In this case, intravenous administration of PCC succeeded in increasing the patient's hemostasis ability. Patients experienced significant increases in hematocrit and red blood cell count following administration of this therapy. This suggests that PCC is effective in replacing blood clotting factors lost during heavy bleeding andhelps stop postoperative bleeding. PCC contains significantly higher amounts of the clotting factors compared to FFP; one dose of PCC equals 8 to 16 units of FFP.
These results are consistent with previous studies showing the benefits of PCC in improving hemostasis in patients with blood clotting disorders. The use of PCC has been proven to be an effective therapy in treating heavy bleeding in various clinical conditions, including blunt abdominal trauma after splenectomy.9.10
A complication that often arises after severe blunt abdominal trauma is AKI. Prolonged bleeding causes renal hypoperfusion and can cause acute kidney damage. In this case, the use of PCC also helps prevent AKI. By stopping bleeding and improving hemostasis, patients do not experience a decrease in diuresis or a significant increase in serum creatinine, which are the main signs of AKI.
This case report shows that administration of prothrombin complex concentrate is effective in stopping post-splenectomy bleeding in patients with blunt abdominal trauma. In addition, the use of PCC also helps prevent AKI as a serious complication. However, further research with a more robust study design is needed to confirm the benefits of using PCC in a broader patient population with similar conditions. Medical teams should remain alert to the risk of bleeding and AKI in post-splenectomy blunt abdominal trauma patients and consider the use of PCC as part of a holistic and effective treatment strategy.
Prothrombin complex concentrate has a significant role in treating post-splenectomy bleeding in blunt abdominal trauma patients, especially in these cases with a risk of AKI. Administration of prothrombin complex concentrate helps improve hemostasis, prevent AKI, and facilitate patient recovery.
5. Acknowledgments
We would like to thank Fatmawati Hospital, Jakarta, Indonesia who provided place and patient support for this research. In addition, we would like to extend our sincere thanks to all of the participants in our study, who generously shared their time, experiences, and insights with us.
6. Authors’ contribution
APL: Write, Concept, conduction of the study work, manuscript editing and revising
SKM, VI: Mentor (clinical), editor
Author affiliations:
- Aditia Pria Laksana, Intensive Care Consultant/Specialist Doctor Education Program, Department of Anesthesiology and Intensive Therapy, University of Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia; E-mail: dr.aditiapl@gmail.com
- Sidharta Kusuma Manggala, Department of Anesthesiology and Intensive Therapy, University of Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia; E-mail: maninjau3@gmail.com
- Vera Irawany, Department of Anesthesiology and Intensive Therapy, Fatmawati Hospital, Jakarta, Indonesia.
ABSTRACT
Blunt abdominal trauma is an event that can cause massive internal bleeding and can be life-threatening. Splenectomy is often performed to treat organ injuries in patients with blunt abdominal trauma. However, splenectomy can cause hemostasis problems, which can cause more bleeding and risk complications such as Acute Kidney Injury (AKI).
This case report aims to discuss the role of prothrombin complex concentrate (PCC) in treating bleeding and preventing AKI in blunt abdominal trauma patients after splenectomy at Fatmawati Hospital, Jakarta, Indonesia.
A 15-year-old woman experienced blunt abdominal trauma due to a sports accident and sustained internal bleeding. After a thorough evaluation, she underwent an emergency splenectomy to stop the bleeding. However, patients developed hemostasis problem which made the control of postoperative bleeding difficult. To overcome this problem, patient was administered PCC intravenously, which resulted in significant improvement in controlling postoperative bleeding. The hematocrit level and red blood cell count steadily increased, indicating the effectiveness of PCC in improving the patient's hemostasis.
PCC can play an important role in treating post-splenectomy bleeding in patients with blunt abdominal trauma. Apart from that, the use of PCC can also help prevent AKI, which is a serious and life-threatening complication. Further research and clinical trials are needed to confirm the benefits of using PCC in a broader patient population with similar conditions.
Abbreviations: AKI- Acute Kidney Injury; PCC- Prothrombin Complex Concentrate
Keywords: Acute Kidney Injury; Bleeding; Blunt Abdominal Trauma; Prothrombin Complex Concentrate; Splenectomy
Citation: Laksana AP, Manggala SK, Irawany V. The role of prothrombin complex concentrate to control critical bleeding after splenectomy for blunt abdominal trauma; A case report. Anaesth. pain intensive care 2024;28(1):177−181; DOI: 10.35975/apic.v28i1.2289
Received: September 13, 2023; Reviewed: October 29, 2023; Accepted: December 19, 2023
1. INTRODUCTION
Blunt abdominal trauma is a serious injury that can cause internal bleeding and be life-threatening. Blunt abdominal trauma can be caused by various events, such as traffic accidents, sports accidents, or hard physical impacts. 1 It generally affects important organs in the abdominal cavity, including the spleen, liver, pancreas, and kidneys. In some cases of severe blunt abdominal trauma, surgery may be necessary to stop bleeding and treat organ damage. 2 One of the surgical procedures commonly performed to treat blunt abdominal trauma is splenectomy. A spleen damaged by trauma often causes heavy bleeding and requires immediate action to avoid more serious complications. One of the complications that can occur after splenectomy is disruption of the blood coagulation system, which can cause hemostasis problems and make it difficult to control bleeding.3 This condition is a serious concern because it can result in significant blood loss and risks causing problems with circulation of the vital organs including the kidneys. 4–6
Acute Kidney Injury (AKI), or acute kidney damage, is a serious complication that can occur in trauma patients with heavy bleeding. Prolonged bleeding can cause renal hypoperfusion, which reduces blood flow to the kidneys and results in damage to the renal cells. If not treated quickly and appropriately, AKI can cause potentially life-threatening kidney failure. Anemia and AKI are both important health problems because they are associated with morbidity and mortality.4–6 AKI increases depending on the decrease in hemoglobin levels and the ideal hemoglobin threshold associated with an increased risk of AKI is 10.5 g/dL. In a normal physiological response, the kidneys receive approximately 20-25 percent of the blood from cardiac output. This is the highest requirement in the entire body concerning the weight of the organ. As a pathological response, anemia directly reduces oxygen delivery. Because AKI often develops in ischemic conditions, anemia may be one of the causes of the high incidence of AKI in hospitalized patients. Patients with anemia and AKI had a higher risk of death than the peer group. This may be because anemia and AKI exacerbate organ dysfunction or delay organ recovery. 4–6 Current ICU outcomes remain suboptimal. Therefore, it is important to monitor these two conditions in patients admitted to the ICU and patients who survive the ICU.4–6 Future follow-up studies will evaluate the mechanisms underlying the association between anemia and AKI. Additionally, new data should reveal when to correct the anemia of critically ill patients to achieve personalized treatment approaches and better survival outcomes. Five million people per year (worldwide) die from traumatic injuries, 10-20% of which are potentially preventable. The biggest cause of preventable death is early bleeding within the first 6 hours after injury and delayed bleeding after more than 24 hours or within days. 4
In the treatment of blunt abdominal trauma after splenectomy with bleeding and risk of AKI, administration of prothrombin complex concentrate (PCC) has become one of the therapeutic options applied. PCC is a blood product that contains blood clotting factors, including factors II, VII, IX, and X, as well as proteins C and S. The use of PCC aims to improve hemostasis and stop bleeding. 4–6
This case study aims to evaluate the effectiveness and benefits of using PCC in patients with this condition. It is hoped that the results of this case report will provide guidance and a better understanding of the management of major bleeding and coagulopathy after trauma in the future.
2. CASE REPORT
The research subject was a 15-year-old lady who was treated at Fatmawati General Hospital, Jakarta with a diagnosis of blunt abdominal trauma. The patient suffered a serious injury due to a sports accident and experienced significant internal bleeding, necessitating a splenectomy as an emergency measure to treat spleen damage.
Data collected included patient demographic information, history of trauma and previous surgery, physical and laboratory examination results, radiology results (abdominal CT scan, renal ultrasonography), and surgical records during splenectomy. In addition, the data also included information of the blood removed during surgery and post-surgery, along with the interventions and therapies administered, including PCC.
| Table 1: Blood parameters (Abnormal readings are given as bold figures) | ||||||||
| Parameter | Normal value | Date and time of sampling | ||||||
| 12/09/22 | 13/09/22
13.07 |
13/09/22
22.35 |
14/09/22
15.42 |
14/09/22
22.50 |
15/09/22 | 16/09/22 | ||
| Hb (g/dL) | 10-14 | 3.7 | 11.2 | 10 | 9.1 | 9 | 8.2 | 9.9 |
| Ht (% of RBCs) | 30-42 | 12 | 33 | 30 | 27 | 27 | 24 | 30 |
| Leukocytes | 5000-10000 | 15400 | 32100 | 26000 | 12500 | 14600 | 18300 | 19500 |
| Platelets | 150-350 | 264 | 104 | 112 | 102 | 96 | 88 | 85 |
| Erythrocytes | 3.5-5.0 | 1.6 | 4.2 | 3.7 | 3.4 | 3.4 | 3.0 | 3.6 |
| Lactate (mmol/L) | 0.5-2.2 | 5.3 | ||||||
| Table 2: Blood gas analysis (Abnormal readings are given as bold figures) | ||||||
| Parameter | Normal value | Date and time of sampling | ||||
| 16/09/22 | 17/09/22
08.30 |
17/09/22
11.57 |
18/09/22
00.14 |
18/09/22
13.29 |
||
| PH | 7.35-7.45 | 7.228 | 7.32 | 7.15 | 7.34 | |
| PCO2 (mmHg) | 35-45 | 40.4 | 45.4 | 70.1 | 68.2 | |
| PO2 (mmHg) | 75-95 | 198 | 187.4 | 45.0 | 52.6 | |
| HCO3− (mmol/L) | 22-29 | 17 | 23.4 | 24.9 | 37.0 | |
| BE ecf (mmol/L) | -10.9 | −10.9 | ||||
| BE b (mmol/L) | -11.1 | −10.5 | −3.0 | −4.1 | 11.0 | |
| SO2 (%) | 94-98 | 99.5 | 98.2 | 66.0 | 82.0 | |
| T CO2 (mEq/L) | 23-30 | 18.3 | 24.8 | 27.0 | 39.1 | |
| CRP quantitative | 8.6 | 3,26 | 18.63 | |||
| Procalcitonin (µg/L) | 30.38 | >32.0 | 8.43 | |||
After a thorough evaluation and confirmation of severe internal bleeding and significant splenic damage, the patient underwent an emergency splenectomy. During surgery, the patient experienced hemostasis problems requiring the use of PCC as part of therapy to control bleeding. Her serial blood parameters and blood gas analysis were done and the reports are reproduced as Table 1 and 2. Blood chemistry report ia reproduced as Table 3.
During surgery, the patient experienced hemostasis problems that made it difficult to control bleeding. To treat this condition, she was administered PCC intravenously as part of therapy to promote hemostasis and stop bleeding as per body weight, 500 iu at 3rd hour and repeated at 4th hour (Figure 1).
After administration of PCC, positive changes were noted in the patient's hematological parameters.
Hematocrit levels and red blood cell counts increased significantly, indicating the effectiveness of therapy in stopping bleeding and replacing blood components lost during surgery. The patient did not show any sign of excessive post-surgical bleeding after administration of PCC.
| Table 3: Blood chemistry | |||||
| Parameter | Date of sampling (Abnormal readings are given as bold figures) | ||||
| 17/09/22 | 18/09/22 | 18/09/22 | 19/09/22 | 20/09/22 | |
| Hb (g/dL) | 9.6 | 10.8 | 8.4 | 7.6 | 7.9 |
| Ht (% of RBCs) | 28.9 | 32.2 | 24.6 | 22.0 | 21.9 |
| Leukocytes (103/mm3) | 18700 | 19400 | 19500 | 28400 | 46700 |
| Platelets (103/µL) | 105 | 164 | 159 | 195 | 172 |
| NLR | 14.2 (84/6) | 22.5 (83/4) | 17.7 (82/5) | 14.0 (84/6) | 11.3 (83/7) |
| SGOT/SGPT | 1260/553 | ||||
| Albumin (g/dL) | 2.68 | 2.14 | |||
| PT/control (sec) | 14.3 (15.7) | ||||
| aPTT (sec) | 24.3 (36.2) | 60.1 (36.2) | |||
| Fibrinogen (mg/dL) | 521 | ||||
| D-dimer | >20000 | ||||
| Urea (mg/dL) | 233.5 | 135.2 | |||
| Creatinine (mg/dl) | 8.53 | 3.56 | |||
| Na/K/Cl (mmol/L) | 141/7.4/105 | 137/4.3/100 | 136/3.7/100 | 134/3.5/99 | 133/3.9/97 |
| Ca Ion (mmol/L) | 0.8 | 1.06 | 0.99 | 0.96 | |
| Mg (mg/dL) | 2.3 | 2.0 | 1.9 | 2.0 | 2.4 |
| Lactate (mmol/L) | 4.9 | 1.9 | 3.8 | 2.2 | |
| Lymphocytes (absolute) (/µL) | 784 | 895 | 1703 | 3411 | |
The patient received intensive care during the postoperative recovery period, including close monitoring of renal function and hemostasis status. She also received appropriate nutritional support and fluid therapy to facilitate the healing process. Apart from that, the medical team also provided education and psychosocial support to the patient and her family during the recovery period.
3. DISCUSSION
Handling blunt abdominal trauma after splenectomy with the risk of bleeding and AKI, is a complex challenge for the medical team.4 In this case report, we discussed the role of PCC in treating bleeding and preventing AKI in a 15-year-old female patient who suffered a serious injury due to a sports accident. This patient underwent splenectomy as an emergency measure to stop bleeding in the damaged spleen. After surgery, the patient experienced hemostasis problems requiring the administration of PCC as adjuvant therapy to stop bleeding and prevent complications of AKI.
In this case, intravenous administration of PCC succeeded in increasing the patient's hemostasis ability. Patients experienced significant increases in hematocrit and red blood cell count following administration of this therapy. This suggests that PCC is effective in replacing blood clotting factors lost during heavy bleeding andhelps stop postoperative bleeding. PCC contains significantly higher amounts of the clotting factors compared to FFP; one dose of PCC equals 8 to 16 units of FFP.
These results are consistent with previous studies showing the benefits of PCC in improving hemostasis in patients with blood clotting disorders. The use of PCC has been proven to be an effective therapy in treating heavy bleeding in various clinical conditions, including blunt abdominal trauma after splenectomy.9.10
A complication that often arises after severe blunt abdominal trauma is AKI. Prolonged bleeding causes renal hypoperfusion and can cause acute kidney damage. In this case, the use of PCC also helps prevent AKI. By stopping bleeding and improving hemostasis, patients do not experience a decrease in diuresis or a significant increase in serum creatinine, which are the main signs of AKI.
This case report shows that administration of prothrombin complex concentrate is effective in stopping post-splenectomy bleeding in patients with blunt abdominal trauma. In addition, the use of PCC also helps prevent AKI as a serious complication. However, further research with a more robust study design is needed to confirm the benefits of using PCC in a broader patient population with similar conditions. Medical teams should remain alert to the risk of bleeding and AKI in post-splenectomy blunt abdominal trauma patients and consider the use of PCC as part of a holistic and effective treatment strategy.
4. CONCLUSION
Prothrombin complex concentrate has a significant role in treating post-splenectomy bleeding in blunt abdominal trauma patients, especially in these cases with a risk of AKI. Administration of prothrombin complex concentrate helps improve hemostasis, prevent AKI, and facilitate patient recovery.
5. Acknowledgments
We would like to thank Fatmawati Hospital, Jakarta, Indonesia who provided place and patient support for this research. In addition, we would like to extend our sincere thanks to all of the participants in our study, who generously shared their time, experiences, and insights with us.
6. Authors’ contribution
APL: Write, Concept, conduction of the study work, manuscript editing and revising
SKM, VI: Mentor (clinical), editor
7. REFERENCES
- Bhatt HV, Subramaniam K. PRO: Prothrombin Complex Concentrate Should Be Used in Preference to Fresh Frozen Plasma for Hemostasis in Cardiac Surgical Patients. J Cardiothorac Vasc Anesth. 2018;32(2):1062-1067. [PubMed] DOI: 1053/j.jvca.2017.05.044
- Dickneite G, Pragst I. Prothrombin complex concentrate vs fresh frozen plasma for reversal of dilutional coagulopathy in a porcine trauma model. Br J Anaesth. 2009;102(3):345-54. [PubMed] DOI: 1093/bja/aen391
- Desmettre T, Dehours E, Samama CM, Jhundoo S, Pujeau F, Guillaudin C, et al. Reversal of Vitamin K Antagonist (VKA) effect in patients with severe bleeding: a French multicenter observational study (Optiplex) assessing the use of Prothrombin Complex Concentrate (PCC) in current clinical practice. Crit Care. 2012;16(5):R185. [PubMed] DOI: 1186/cc11669
- Grottke O, Levy JH. Prothrombin complex concentrates in trauma and perioperative bleeding. Anesthesiology. 2015;122(4):923-31. [PubMed] DOI: 1097/ALN.0000000000000608
- Han SS, Baek SH, Ahn SY, Chin HJ, Na KY, Chae DW, Kim S. Anemia Is a Risk Factor for Acute Kidney Injury and Long-Term Mortality in Critically Ill Patients. Tohoku J Exp Med. 2015;237(4):287-95. [PubMed]. DOI: 1620/tjem.237.287
- Samama CM. Prothrombin complex concentrates: a brief review. Eur J Anaesthesiol. 2008;25(10):784-9. [PubMed] DOI: 1017/S0265021508004675
- Sayce AC, Neal MD, Leeper CM. Viscoelastic monitoring in trauma resuscitation. Transfusion. 2020;60 Suppl 6:S33-S51. [PubMed] DOI: 1111/trf.16074
- Spahn DR, Bouillon B, Cerny V, Duranteau J, Filipescu D, Hunt BJ, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care. 2019;23(1):98. [PubMed] DOI: 1186/s13054-019-2347-3
- Yasaka M, Sakata T, Naritomi H, Minematsu K. Optimal dose of prothrombin complex concentrate for acute reversal of oral anticoagulation. Thromb Res. 2005;115(6):455-9. [PubMed] DOI: 1016/j.thromres.2004.09.002
- Zemrak W, Manuel F, Smith KE, Rolfe S, Hayes T, Trowbridge RL, et al. Low-dose compared to manufacturer-recommended dose four-factor prothrombin complex concentrate for acute warfarin reversal. Thromb Thrombolysis. 2019;47(2):263-271. [PubMed] DOI: 10.1007/s11239-018-1768-1