Elvia AS¹, Rudyanto Sedono2, Yohanes WH George3
Author affiliation:
Bacterial endotoxins in sepsis induce dysregulation and excessive release of inflammatory mediators and cytokines, leading to organ dysfunction. Removing excess endotoxins and cytokines from the circulation could potentially reverse the dysregulation of the immune response. oXiris filter is capable of filtration and adsorption middle-size molecule cytokines and large molecular archives such as endotoxins.
A man, 77 years old, weighing 70 kg, with 174 cm height and 23.17 BMI was diagnosed with septic shock with Fournier gangrene, acute on chronic kidney disease, uncontrolled blood sugar, and history of diabetes mellitus. He was put on meropenem antibiotic therapy. After necrotomies, increase in the levels of leukocytes, urea, creatinine, procalcitonin, D-dimer, NT-proBNP, and IL 6 was observed. Vasopressor dose was increased, and the patient also experienced tachycardia and fever.
Meropenem was stopped and replaced with ceftaroline fosamil, and 24 h later hemofiltration with an oXiris filter was performed for 48 h. After hemofiltration, there was a decrease in vasopressor dose, urea, creatinine, and procalcitonin values. The patient′s hemodynamic status was stable without vasopressor, the dose of furosemide was decreased, and the urine output was increased. Then, the patient was transferred to the ward. The current patient had an upregulation of pro-inflammatory mediators as evidenced by clinical symptoms and laboratory findings. Additional treatment with extracorporeal blood purification techniques such as hemofiltration is required in these patients to facilitate the treatment of septic shock through the modulation of the immune response.
Keywords: septic shock, dysregulation, hemofiltration, immunomodulation
Citation: Elvia AS, Sedono R, George YWH. Early hemofiltration as immunomodulation for septic shock in acute on chronic kidney disease: a case report. Anaesth. pain intensive care 2024;28(1):182−186.
DOI: 10.35975/apic.v28i1.2271
Received: August 17, 2023; Reviewed: December 23, 2023; Accepted: December 23, 2023
Sepsis is a life-threatening organ dysfunction caused by dysregulation of the host response to infection. Septic shock is the development of sepsis resulting in circulatory, cellular, and metabolic disturbances, thereby increasing the mortality risk.1 Sepsis affects approximately 1.7 million adults in the United States each year and has the potential to contribute to more than 250,000 deaths. Various studies estimate that sepsis occurs in 30% to 50% of hospitalizations and results in death.2 Extracorporeal blood purification is proposed as an adjuvant therapy for sepsis, aiming to control immune system-related dysregulation, which induces organ dysfunction.3 Hemofiltration by a novel small-sized filter called oXiris has made the procedure simplified and easier. We present a case of the use of this filter in an old male patient.
A 77 years old man, weighing 70 kg, with 174 cm height, and 23.17 kg/m2 BMI came to the emergency room with severely painful swelling in the scrotal, peri-anal, and lower abdominal regions. The patient had a history of type II diabetes mellitus (DM) and had been on oral anti-diabetic drug. The patient had no history of hypertension, heart disease, kidney disease, or lung disease. On physical examination, blood pressure was 100/70 mmHg, heart rate 98 beats/min, respiratory rate 28 times/min, and temperature 36.8˚C.
Laboratory examination revealed leukocyte count of 16,470/ml, urea 93 mg/dl, creatinine 2.57 mg/dl, blood sugar 588 mg/dl, HbA1c 9.7%, and procalcitonin 14.02 ng/dl. Chest X-ray and electrocardiography were within normal limits.
The patient was diagnosed with sepsis, cellulitis with Fournier′s gangrene, type II diabetes mellitus with ketosis, and acute on chronic kidney disease. He was treated with inj meropenem 1 gram IV three times daily, inj metronidazole 500 mg three times daily, inj paracetamol 1000 mg IV three times daily, ringer lactate 500 ml/12 h, gelofusal 500 ml/24 h, and insulin 2 units/h with blood sugar correction every 6 h.
The patient was treated in the ward and was planned for necrotomy surgery after the blood sugar was controlled. During treatment, the blood pressure was 90/48 mmHg, body temperature 38.50 C, respiration rate 28 times per minute, and peripheral oxygen saturation was 96% with oxygen 4 L/min through nasal cannula. Laboratory examination revealed blood ketone 3.1 mmol/L.
The patient was transferred to the ICU and a central venous catheter (CVC) was inserted. He was given norepinephrine with a titrated dose of 0.15 mg/kg/h. The patient then underwent immediate necrotomy under general anesthesia in the operating room and returned to the ICU. During post-surgery monitoring, the patient’s blood pressure was stable, and norepinephrine dose could be reduced and then stopped. The patient was planned to be transferred to the general ward.
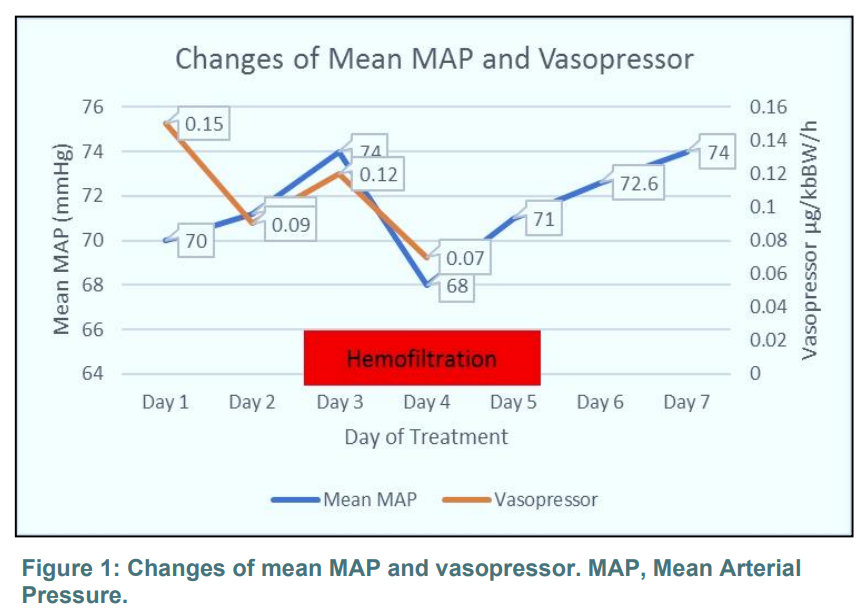
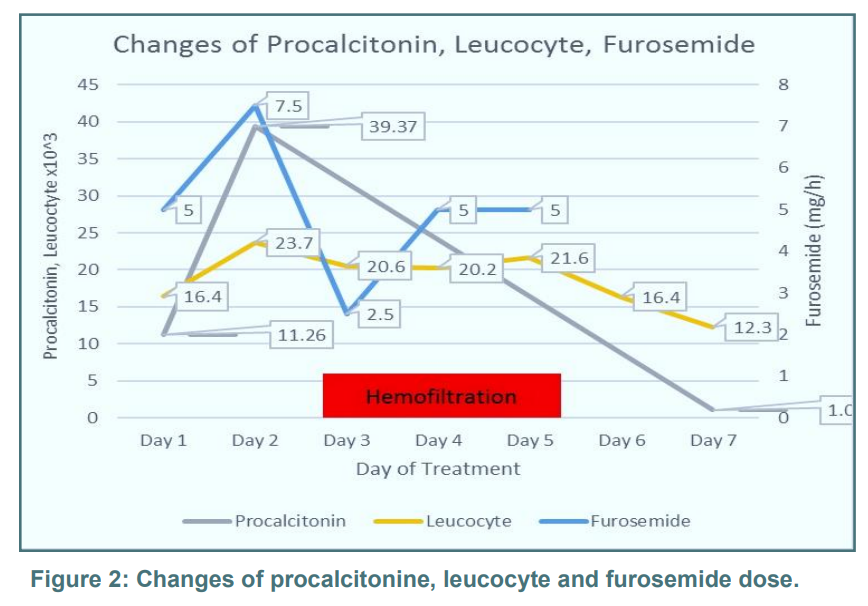
However, 12 h postoperatively patient was restless, his blood pressure fell, and he experienced tachycardia. Urine output was 0.47 mg/h and CVP increased to about 10 to 14 mmHg. Laboratory examination revealed an increase of leukocytes to 20.700/ml, procalcitonin 39.37 ng/dl, urea 115 mg/dl, creatinine 2.27 mg/dl, NT pro-BNP 2150 ng/dl, d-dimer 8 ng/dl, and IL-6 543.9 pg/dl. Meropenem was stopped and switched to 600 mg ceftaroline twice daily, norepinephrine was given with a titrated dose of 0.09 µg/kg/h. Furosemide was also administered at a dose of 5 mg/h. On the second day of ICU treatment, the dose of norepinephrine had to be increased to 0.12 mg/kg/h, and furosemide to 7.5 mg/h. Double lumen catheter (CDL) was inserted and the patient was started on hemofiltration with oXiris filter @ 25-35 ml/kg/h.
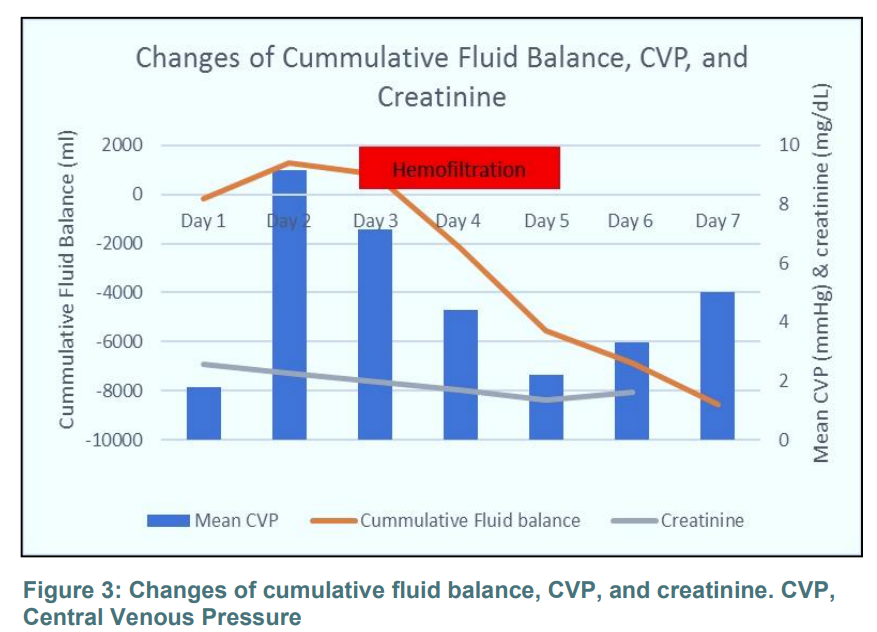
After 48 h of hemofiltration, the patient's general condition improved, his blood pressure was stable, the norepinephrine dose could be decreased and stopped, and the pulse rate reduced. Laboratory examinations found that his leukocyte count was decreased to 16,380/ml, urea 57 mg/dl, creatinine 1.67 mg/dl, and procalcitonin 1.07 ng/dl. Urine production was increased and furosemide could be stopped. The patient was transferred to the general ward on the sixth day.
The success of therapy can be assessed clinically by increasing blood pressure and decreasing the need for vasopressor doses (Figure 1). The procalcitonin and leukocyte levels also decreased as the patient's condition improved (Figure 2). Increased urine production is indicated by an increase in the cumulative fluid balance, a decrease in central venous pressure, followed by a decrease in the creatinine level (Figure 3). Removing circulating endotoxins and excess cytokines from the circulation restores chemotactic gradients, localizing the immune response to the principal site of infection and re-establishing a regulated immune response.
The first step in initiating the host response to pathogen is the activation of innate immune cells, which are composed primarily of macrophages, monocytes, neutrophils, and natural killer cells. Macrophages bind to PAMPs (pathogen-associated molecular patterns) such as bacterial endotoxins and exotoxins, lipids, and fungal B glucans at specific receptors (toll-like receptors, TLRs) on the surface of antigen-presenting cells (APCs) and monocytes.
In addition, damage-associated molecular patterns (DAMPs), which are intracellular materials or molecules released from dead tissue or damaged host cells such as ATP and mitochondrial DNA, can also interact in the same way. These molecules activate specific receptors on the surface of APCs and monocytes, thereby initiating the clinical syndrome of sepsis through transcription of genes involved in inflammation, cell metabolism, and adaptive immunity.
This leads to the immediate expression of activated pro-inflammatory genes such as IL-1, IL-12, IL-18, tumor necrosis factor (TNF-a), and interferon (IFN). These inflammatory mediators lead to further activation of cytokines (such as IFN-y, IL-6, IL-8), complement and coagulation pathways, and negative feedback, downregulation of adaptive components of the immune system.
In the early stages of sepsis, there is an increase in the pro-inflammatory and anti-inflammatory cytokines. Proinflammatory cytokines cause leukocyte activation and proliferation, activation of the complement system, upregulation of endothelial adhesion molecules and chemokine expression, production of tissue factors, and induction of hepatic acute-phase reactants. In sepsis, an exaggerated immune response, as described above, results in collateral damage and death of host cells and tissues. Hyporesponsive or hyper-responsive immunological responses are individual in nature. In some patients, it can occur simultaneously with immunosuppression caused by downregulation of activated cell surface molecules increasing cell immune apoptosis, and T cell exhaustion. Immunoparalysis leads to patients being susceptible to nosocomial infections, opportunistic pathogens, and viral reactivation.6
In sepsis, there is a decrease in oxygen delivery and utilization by cells due to hypoperfusion. Hypoperfusion occurs due to cardiovascular dysfunction. Septic cardiomyopathy can occur because cytokines such as TNFα and IL-1β cause depression of cardiac myocytes and impair mitochondrial function. Septic cardiomyopathy is acute in onset and reversible, and the incidence varies from 18% to 60%.
Inflammatory mediators induce arterial and venous vasodilation, and microvascular vasodilation in arterioles, venules, and capillaries, resulting in reduced venous return, hypotension, and distributive shock. Loss of endothelial barrier function caused by changes in the endothelium and tight junctions results in leakage of intravascular fluid into the interstitial spaces. The occurrence of hemodynamic changes in the body along with microvascular thrombosis can result in hypoperfusion of tissues and organs. As a result, there is an increase in anaerobic glycolysis in cells that produce lactic acid.4, 5, 6
This patient was infected by pathogens, resulting in an excessive increase in proinflammatory mediators. He had been given septic shock treatment according to the 2021 Surviving Sepsis Campaign guidelines in the form of fluid resuscitation, antibiotic therapy in the first one hour, control of infection source, and vasopressors. However, the shock did not resolve, as leukocyte count, creatinine, procalcitonin, IL-6, and d-dimer increased, and urine production decreased. The patient then underwent hemofiltration with oXiris filter in the early phase of sepsis for 48 h. oXiris is a Continuous Renal Replacement Therapy (CRRT) filter that can simultaneously adsorb endotoxin and inflammatory mediators while providing renal support. Therefore, using a hemofilter with an endotoxin and cytokine adsorption device can provide additional therapeutic benefits compared to conventional CRRT filter. The success of this treatment modality can be assessed through clinical improvement of hemodynamic stability and increased urine production. In laboratory parameters, there was a decrease in leukocyte count as well as the levels of creatinine and procalcitonin. Removing circulating endotoxins and excess cytokines from the circulation restores chemotactic gradients, localizing the immune response to the principal site of infection and re-establishing a regulated immune response.
Extracorporeal blood purification techniques have been developed to facilitate the treatment of sepsis by modulating the immune response and removing circulating endotoxin and excess cytokines from the circulation. It may be a useful technique for removing these molecules from circulation. The complexity and heterogeneity of the hypotheses on the immune system in septic patients, prompted us to seek individual treatment modalities based on the patient's clinical and immunopathophysiological background. Therefore, the concept of blood purification is to attenuate the remarkable systemic expression of proinflammatory and anti-inflammatory mediators. Restoration of immune homeostasis is thought to improve yield and survival.
Ronco et al. hypothesized that removing peak blood cytokine concentrations during the early phase of sepsis could halt inflammatory cascade, limit organ damage, and reduce the incidence of multi-organ failure syndrome.7
Honoré and Matson's hypothesis states that the removal of cytokines from the blood compartment leads to the removal of cytokines located at the tissue level due to a concentration balance between these two compartments.8 Meanwhile, Paternoster G. proposed that blood purification therapy acts on cellular level inflammation to restore immune function through the regulation of monocytes, neutrophils, and lymphocytes.6
Lumlertgul and Srisawat conducted a retrospective study of a case series of extracorporeal blood purification in septic shock patients with acute kidney injury (AKI) or end-stage renal disease (ESDR) using oXiris hemofilter during CRRT therapy.9
The results showed a significant reduction in norepinephrine dose, inotropic score, and vasopressor dependence index in both the AKI and ESRD groups. Hemodynamic stabilization and improvement in inotropic scores, vasopressor dependence indices, and cardiovascular SOFA scores paralleled increased lactate clearance and alkaline overload in patients using oXiris membrane during CRRT.5
Blood purification through removing excessive endotoxins and cytokines from the circulation can reverse the excess regulation of immune responses. By using an oXiris filter capable of filtration and adsorption, middle molecule cytokines and large molecular archives such as endotoxins can be filtered.
5. Acknowledgement
We gratefully thank Faculty of Medicine, Universitas Indonesia – Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia.
6. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
7. Authors’ contribution
EAS: conceptualization, data curation, formal analysis, project administration, writing-original draft, writing-review and editing.
RS, YWHG: writing-original draft, writing-review and editing.
Author affiliation:
- Elvia AS, Trainee of Intensive Care Fellowship Program, Department of Anesthesiology & Intensive Care, Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia.
- Rudyanto Sedono, Department of Anesthesiology & Intensive Care, Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia.
- Yohanes WH George, Department of Anesthesiology & Intensive Care, Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo National General Hospital, Jakarta. Emergency & Intensive Care Unit Pondok Indah Hospital, Jakarta, Indonesia.
ABSTRACT
Bacterial endotoxins in sepsis induce dysregulation and excessive release of inflammatory mediators and cytokines, leading to organ dysfunction. Removing excess endotoxins and cytokines from the circulation could potentially reverse the dysregulation of the immune response. oXiris filter is capable of filtration and adsorption middle-size molecule cytokines and large molecular archives such as endotoxins.
A man, 77 years old, weighing 70 kg, with 174 cm height and 23.17 BMI was diagnosed with septic shock with Fournier gangrene, acute on chronic kidney disease, uncontrolled blood sugar, and history of diabetes mellitus. He was put on meropenem antibiotic therapy. After necrotomies, increase in the levels of leukocytes, urea, creatinine, procalcitonin, D-dimer, NT-proBNP, and IL 6 was observed. Vasopressor dose was increased, and the patient also experienced tachycardia and fever.
Meropenem was stopped and replaced with ceftaroline fosamil, and 24 h later hemofiltration with an oXiris filter was performed for 48 h. After hemofiltration, there was a decrease in vasopressor dose, urea, creatinine, and procalcitonin values. The patient′s hemodynamic status was stable without vasopressor, the dose of furosemide was decreased, and the urine output was increased. Then, the patient was transferred to the ward. The current patient had an upregulation of pro-inflammatory mediators as evidenced by clinical symptoms and laboratory findings. Additional treatment with extracorporeal blood purification techniques such as hemofiltration is required in these patients to facilitate the treatment of septic shock through the modulation of the immune response.
Keywords: septic shock, dysregulation, hemofiltration, immunomodulation
Citation: Elvia AS, Sedono R, George YWH. Early hemofiltration as immunomodulation for septic shock in acute on chronic kidney disease: a case report. Anaesth. pain intensive care 2024;28(1):182−186.
DOI: 10.35975/apic.v28i1.2271
Received: August 17, 2023; Reviewed: December 23, 2023; Accepted: December 23, 2023
1. INTRODUCTION
Sepsis is a life-threatening organ dysfunction caused by dysregulation of the host response to infection. Septic shock is the development of sepsis resulting in circulatory, cellular, and metabolic disturbances, thereby increasing the mortality risk.1 Sepsis affects approximately 1.7 million adults in the United States each year and has the potential to contribute to more than 250,000 deaths. Various studies estimate that sepsis occurs in 30% to 50% of hospitalizations and results in death.2 Extracorporeal blood purification is proposed as an adjuvant therapy for sepsis, aiming to control immune system-related dysregulation, which induces organ dysfunction.3 Hemofiltration by a novel small-sized filter called oXiris has made the procedure simplified and easier. We present a case of the use of this filter in an old male patient.
2. CASE REPORT
A 77 years old man, weighing 70 kg, with 174 cm height, and 23.17 kg/m2 BMI came to the emergency room with severely painful swelling in the scrotal, peri-anal, and lower abdominal regions. The patient had a history of type II diabetes mellitus (DM) and had been on oral anti-diabetic drug. The patient had no history of hypertension, heart disease, kidney disease, or lung disease. On physical examination, blood pressure was 100/70 mmHg, heart rate 98 beats/min, respiratory rate 28 times/min, and temperature 36.8˚C.
Laboratory examination revealed leukocyte count of 16,470/ml, urea 93 mg/dl, creatinine 2.57 mg/dl, blood sugar 588 mg/dl, HbA1c 9.7%, and procalcitonin 14.02 ng/dl. Chest X-ray and electrocardiography were within normal limits.
The patient was diagnosed with sepsis, cellulitis with Fournier′s gangrene, type II diabetes mellitus with ketosis, and acute on chronic kidney disease. He was treated with inj meropenem 1 gram IV three times daily, inj metronidazole 500 mg three times daily, inj paracetamol 1000 mg IV three times daily, ringer lactate 500 ml/12 h, gelofusal 500 ml/24 h, and insulin 2 units/h with blood sugar correction every 6 h.
The patient was treated in the ward and was planned for necrotomy surgery after the blood sugar was controlled. During treatment, the blood pressure was 90/48 mmHg, body temperature 38.50 C, respiration rate 28 times per minute, and peripheral oxygen saturation was 96% with oxygen 4 L/min through nasal cannula. Laboratory examination revealed blood ketone 3.1 mmol/L.
The patient was transferred to the ICU and a central venous catheter (CVC) was inserted. He was given norepinephrine with a titrated dose of 0.15 mg/kg/h. The patient then underwent immediate necrotomy under general anesthesia in the operating room and returned to the ICU. During post-surgery monitoring, the patient’s blood pressure was stable, and norepinephrine dose could be reduced and then stopped. The patient was planned to be transferred to the general ward.
However, 12 h postoperatively patient was restless, his blood pressure fell, and he experienced tachycardia. Urine output was 0.47 mg/h and CVP increased to about 10 to 14 mmHg. Laboratory examination revealed an increase of leukocytes to 20.700/ml, procalcitonin 39.37 ng/dl, urea 115 mg/dl, creatinine 2.27 mg/dl, NT pro-BNP 2150 ng/dl, d-dimer 8 ng/dl, and IL-6 543.9 pg/dl. Meropenem was stopped and switched to 600 mg ceftaroline twice daily, norepinephrine was given with a titrated dose of 0.09 µg/kg/h. Furosemide was also administered at a dose of 5 mg/h. On the second day of ICU treatment, the dose of norepinephrine had to be increased to 0.12 mg/kg/h, and furosemide to 7.5 mg/h. Double lumen catheter (CDL) was inserted and the patient was started on hemofiltration with oXiris filter @ 25-35 ml/kg/h.
After 48 h of hemofiltration, the patient's general condition improved, his blood pressure was stable, the norepinephrine dose could be decreased and stopped, and the pulse rate reduced. Laboratory examinations found that his leukocyte count was decreased to 16,380/ml, urea 57 mg/dl, creatinine 1.67 mg/dl, and procalcitonin 1.07 ng/dl. Urine production was increased and furosemide could be stopped. The patient was transferred to the general ward on the sixth day.
The success of therapy can be assessed clinically by increasing blood pressure and decreasing the need for vasopressor doses (Figure 1). The procalcitonin and leukocyte levels also decreased as the patient's condition improved (Figure 2). Increased urine production is indicated by an increase in the cumulative fluid balance, a decrease in central venous pressure, followed by a decrease in the creatinine level (Figure 3). Removing circulating endotoxins and excess cytokines from the circulation restores chemotactic gradients, localizing the immune response to the principal site of infection and re-establishing a regulated immune response.
3. DISCUSSION
The first step in initiating the host response to pathogen is the activation of innate immune cells, which are composed primarily of macrophages, monocytes, neutrophils, and natural killer cells. Macrophages bind to PAMPs (pathogen-associated molecular patterns) such as bacterial endotoxins and exotoxins, lipids, and fungal B glucans at specific receptors (toll-like receptors, TLRs) on the surface of antigen-presenting cells (APCs) and monocytes.
In addition, damage-associated molecular patterns (DAMPs), which are intracellular materials or molecules released from dead tissue or damaged host cells such as ATP and mitochondrial DNA, can also interact in the same way. These molecules activate specific receptors on the surface of APCs and monocytes, thereby initiating the clinical syndrome of sepsis through transcription of genes involved in inflammation, cell metabolism, and adaptive immunity.
This leads to the immediate expression of activated pro-inflammatory genes such as IL-1, IL-12, IL-18, tumor necrosis factor (TNF-a), and interferon (IFN). These inflammatory mediators lead to further activation of cytokines (such as IFN-y, IL-6, IL-8), complement and coagulation pathways, and negative feedback, downregulation of adaptive components of the immune system.
In the early stages of sepsis, there is an increase in the pro-inflammatory and anti-inflammatory cytokines. Proinflammatory cytokines cause leukocyte activation and proliferation, activation of the complement system, upregulation of endothelial adhesion molecules and chemokine expression, production of tissue factors, and induction of hepatic acute-phase reactants. In sepsis, an exaggerated immune response, as described above, results in collateral damage and death of host cells and tissues. Hyporesponsive or hyper-responsive immunological responses are individual in nature. In some patients, it can occur simultaneously with immunosuppression caused by downregulation of activated cell surface molecules increasing cell immune apoptosis, and T cell exhaustion. Immunoparalysis leads to patients being susceptible to nosocomial infections, opportunistic pathogens, and viral reactivation.6
In sepsis, there is a decrease in oxygen delivery and utilization by cells due to hypoperfusion. Hypoperfusion occurs due to cardiovascular dysfunction. Septic cardiomyopathy can occur because cytokines such as TNFα and IL-1β cause depression of cardiac myocytes and impair mitochondrial function. Septic cardiomyopathy is acute in onset and reversible, and the incidence varies from 18% to 60%.
Inflammatory mediators induce arterial and venous vasodilation, and microvascular vasodilation in arterioles, venules, and capillaries, resulting in reduced venous return, hypotension, and distributive shock. Loss of endothelial barrier function caused by changes in the endothelium and tight junctions results in leakage of intravascular fluid into the interstitial spaces. The occurrence of hemodynamic changes in the body along with microvascular thrombosis can result in hypoperfusion of tissues and organs. As a result, there is an increase in anaerobic glycolysis in cells that produce lactic acid.4, 5, 6
This patient was infected by pathogens, resulting in an excessive increase in proinflammatory mediators. He had been given septic shock treatment according to the 2021 Surviving Sepsis Campaign guidelines in the form of fluid resuscitation, antibiotic therapy in the first one hour, control of infection source, and vasopressors. However, the shock did not resolve, as leukocyte count, creatinine, procalcitonin, IL-6, and d-dimer increased, and urine production decreased. The patient then underwent hemofiltration with oXiris filter in the early phase of sepsis for 48 h. oXiris is a Continuous Renal Replacement Therapy (CRRT) filter that can simultaneously adsorb endotoxin and inflammatory mediators while providing renal support. Therefore, using a hemofilter with an endotoxin and cytokine adsorption device can provide additional therapeutic benefits compared to conventional CRRT filter. The success of this treatment modality can be assessed through clinical improvement of hemodynamic stability and increased urine production. In laboratory parameters, there was a decrease in leukocyte count as well as the levels of creatinine and procalcitonin. Removing circulating endotoxins and excess cytokines from the circulation restores chemotactic gradients, localizing the immune response to the principal site of infection and re-establishing a regulated immune response.
Extracorporeal blood purification techniques have been developed to facilitate the treatment of sepsis by modulating the immune response and removing circulating endotoxin and excess cytokines from the circulation. It may be a useful technique for removing these molecules from circulation. The complexity and heterogeneity of the hypotheses on the immune system in septic patients, prompted us to seek individual treatment modalities based on the patient's clinical and immunopathophysiological background. Therefore, the concept of blood purification is to attenuate the remarkable systemic expression of proinflammatory and anti-inflammatory mediators. Restoration of immune homeostasis is thought to improve yield and survival.
Ronco et al. hypothesized that removing peak blood cytokine concentrations during the early phase of sepsis could halt inflammatory cascade, limit organ damage, and reduce the incidence of multi-organ failure syndrome.7
Honoré and Matson's hypothesis states that the removal of cytokines from the blood compartment leads to the removal of cytokines located at the tissue level due to a concentration balance between these two compartments.8 Meanwhile, Paternoster G. proposed that blood purification therapy acts on cellular level inflammation to restore immune function through the regulation of monocytes, neutrophils, and lymphocytes.6
Lumlertgul and Srisawat conducted a retrospective study of a case series of extracorporeal blood purification in septic shock patients with acute kidney injury (AKI) or end-stage renal disease (ESDR) using oXiris hemofilter during CRRT therapy.9
The results showed a significant reduction in norepinephrine dose, inotropic score, and vasopressor dependence index in both the AKI and ESRD groups. Hemodynamic stabilization and improvement in inotropic scores, vasopressor dependence indices, and cardiovascular SOFA scores paralleled increased lactate clearance and alkaline overload in patients using oXiris membrane during CRRT.5
4. CONCLUSION
Blood purification through removing excessive endotoxins and cytokines from the circulation can reverse the excess regulation of immune responses. By using an oXiris filter capable of filtration and adsorption, middle molecule cytokines and large molecular archives such as endotoxins can be filtered.
5. Acknowledgement
We gratefully thank Faculty of Medicine, Universitas Indonesia – Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia.
6. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
7. Authors’ contribution
EAS: conceptualization, data curation, formal analysis, project administration, writing-original draft, writing-review and editing.
RS, YWHG: writing-original draft, writing-review and editing.
8. REFERENCES
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic Shock: 2016. Intensive Care Med. 2017;43(3):304-377. [PubMed] DOI: 1007/s00134-017-4683-6
- Rhee C, Jones TM, Hamad Y, Pande A, Varon J, O'Brien C, et al. Prevalence, underlying causes, and preventability of sepsis- associated mortality in US acute care hospitals. JAMA Netw Open. 2019;2:e187571. [PubMed] DOI: 1001/jamanetworkopen.2018.7571
- Jarczak D, Kluge S, Nierhaus A. Sepsis – pathophysiology and therapeutic concepts. Front Med. 2021;8:628302. [PubMed] DOI: 3389/fmed.2021.628302
- Gyawali B, Ramakrishna K, Dhamoon AS. Sepsis: the evolution in definition, pathophysiology, and management. SAGE Open Med. 2019;7:2050312119835043. [PubMed] DOI: 1177/2050312119835043
- Rimmelé T, Kellum JA. Clinical review: blood purification for sepsis. Crit Care. 2011;15:205. [PubMed] DOI: 1186/cc9411
- Paternoster G. Immunomodulation, immunostimulation and extracorporeal blood purification. Messenger Anesthesiol Resus. 2019;16:96-106. [FreeFullText]
- Ronco C, Bellomo R, Kellum JA. Acute kidney injury. Lancet. 2019;394(10212):1949-1964. [PubMed] DOI: 1016/S0140-6736(19)32563-2
- Honoré PM, Matson JR. Hemofiltration, adsorption, sieving and the challenge of sepsis therapy design. Crit Care. 2002;6(5):394-6. [PubMed] DOI: 1186/cc1826
- Lumlertgul N, Srisawat N. The haemodynamic effects of oXiris haemofilter in septic shock patients requiring renal support: A single-centre experience. Int J Artif Organs. 2021;44:17-24. [PubMed] DOI: 10.1177/0391398820917150