Mohammed Nour Al-Halabi, Nada Bshara, Zuhair AlNerabieah
Pediatric Dentistry Department, Dental College, Damascus University, Al-Mazzeh Street, Damascus, (Syria)
Correspondence: Mohammed Nour Alhalabi, Al-Mazzeh Street, Pediatric Dentistry Department, Dental College, Damascus University, Damascus, (Syria); Mobile: +963946459369; E-mail: dr.m.nour.h@gmail.com
ABSTRACT
Aim: The aim of this study was to evaluate the effectiveness of two different audiovisual distraction techniques, e.g. audio-visual (AV) eyeglasses – virtual reality box (VR Box) or a Tablet) in the management of anxious pediatric patients during inferior alveolar nerve block (IAN) block.
Study design: A randomized clinical trial carried out on 102 children (60 boys and 42 girls) aged between 6 and 10 years (mean age of 7.4 years) to investigate the effect of using VR eyeglasses ‘VR Box’ and tablet device with wireless headphone in reducing the dental anxiety of children during IAN administration.
Methodology: 102 children were randomly divided into three groups; Group A (Control group): IAN administrated with basic behavior guidance techniques and without using any type of distraction aids. Group B: IAN administrated with using AV eyeglasses ‘VR Box’ and wireless headphone. Group C: IAN administrated with using tablet device and wireless headphones. The participants were selected from children attending the department of the pediatric dentistry at the Faculty of Dentistry, Damascus University, who required local anesthesia (LA) administration in the mandibular arch. All of the children who experienced an IAN block with/without distraction were assessed by using a combination of measures: Wong–Baker FACES (self-report), pulse rate (physiological) and behavior (using FLACC behavior rating scale (‘external evaluator’).
Results: 101 children completed the study out of 102 children. There was no statistically significant difference in the anxiety of audiovisual groups as reported by the Wong–Baker FACES values (p = 0.536) and FLACC scale (p = 0.454). However, there was a statistically significant difference in the anxiety and pain level in pulse rate (p = 0.043).
Conclusions: Distraction using video shown on tablet device was the best in relieving dental anxiety and pain during IAN block. Although using ‘VR Box’ had no added advantage in a majority of children, ‘VR Box’ was more acceptable in older patients (8-10 years) than younger patients and gave the children some exciting experiences which may lead to far better behavior in the next dental visits.
Keywords: Distraction; Behavior management; Children’s dental anxiety
Citation: Al-Halabi MN, Bshara N, AlNerabieah Z. Effectiveness of audio visual distraction using virtual reality eyeglasses versus tablet device in child behavioral management during inferior alveolar nerve block. Anaesth Pain & Intensive Care 2018;22(1):55-61
Received – 13 Nov 2017; Reviewed – 2 Feb 2018, 22 Feb 2018; Corrected - 25 Feb 2018; Accepted – 25 Feb 2018
INTRODUCTION
Researchers have found that one of the most provocation aspects of child behavior management is poor pain control. Even though it is challenging but it is important that clinicians must try their best to reduce pain and discomfort during dental treatment, especially injection procedure.1 In this regard ‘the needle’ is considered as the biggest reason of the pediatric dental patients’ fear.(2)
Dental fear and anxiety can have negative impact on the outcome of the dental treatment, even more on the patients’ oral health related to quality of life as many studies have reported.3-6 A variety of behavioral management techniques has emerged to manage dental fear including pharmacological and non-pharmacological methods.7 Previous studies have stated that use of distraction during dental treatment is useful to patients by reducing their distress and in turn decrease their perception of pain sensation especially during injections with local anesthesia.8
Most children could be made unaware of receiving the injection with the use of topical anesthetic, distraction and a good injection technique.9 It was observed that audiovisual distraction technique was superior in managing anxious pediatric dental patients than using audio distraction alone.10 Using audiovisual aids for distraction during dental injection can alleviate dental anxiety by distracting two types of sensations; hearing and seeing.11 Recently, several studies have shown that AV eyeglasses are effective in distracting pediatric patients during dental procedures.12,13
Therefore, the aim of this study was to evaluate the effectiveness of two different audiovisual distraction techniques (AV eyeglasses ‘VR Box’ vs. tablet) in the management of anxious pediatric patients during IAN block.
METHODOLOGY
The sample size was a total of 102 children, which was calculated using G-Power 3.1 statistical program with (α=0.05, and Power=0.95). The informed consent was taken from parents or legal guardians before the procedures were carried out.
The 102 subjects were randomized into 3 groups. A random allocation list was generated using a randomization website ‘Random.org’. This single-blind randomized clinical trial (RCT) was designed and conducted according to the CONSORT statement over a period of 6 months from April 2017 to October 2017.
The participants were selected from children attending the Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, based on the following inclusion criteria:
Tablet: The tablet (Innjoo F2™, China) capable of playing MP4 audio-visual files, was fixed on the hand of the dental chair using tablet holder (AboveTEK™ tablet holder, China)
Pain assessment scale: The Wong-Baker FACES pain rating scale was used in this study to measure pain after delivering inferior alveolar block injection. Children were asked to choose one of the scale’s faces that best described how they felt during the procedure (Figure 1).
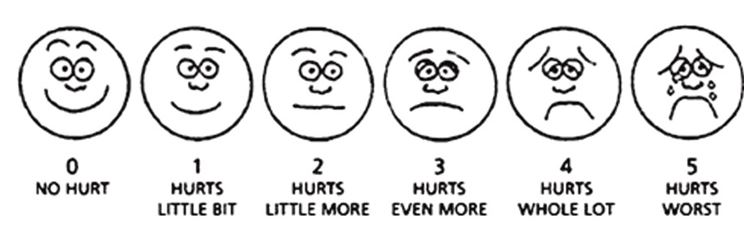
Figure 1: Wong-Baker FACES pain rating scale
Behavior assessment scale: The ‘Face, Legs, Activity, Cry, Consolability’ scale (FLACC scale) was used in this study duo to the reliability that was proved by Dak-Albab et al., in Syrian Arab Republic.14
The following table provides the criteria for the FLACC Behavioral pain scale (Table 1).
Table 1: FLACC scale
Each category is scored on the 0-2 scale which results in a total score of 0-100 = Relaxed and comfortable; 1-3 = Mild discomfort; 4-6 = Moderate pain; 7-10 = Severe discomfort/pain
Pulse rate measures: The pulse rate was recorded for the first time when patients were seated on the dental chair and immediately after IAN block was finished. Then, the difference between the two measures was calculated.
Intervention: 102 children were randomized into three groups according to the distraction type:
Group A (Control group): IAN administrated with basic behavior guidance techniques and without using any type of distraction aids.
Group B: IAN administrated with using AV eyeglasses ‘VR Box’ and wireless headphone.
Group C: IAN administrated with using tablet device and wireless headphone.
For each child patient, a disposable oral examination kit and a traditional oral anesthesia kit (27-gauge long needle, 2 % lidocaine (1:100,000 epinephrine) solution, and an aspirating syringe) was used in this study.
In group B and C, children were asked to choose one episode of the popular cartoon series ─ ‘Tom and Jerry’, ‘Gumball’, ‘Pink Panther’ or ‘SpongeBob’. The first measure of pulse rate was recorded directly when the patient seated comfortably on the dental chair. Afterwards, a 20% benzocaine topical anesthetic gel was applied after drying the injection area for 30 seconds protocol (McDonald et al. 2016). During the application of the topical anesthetic, children were prepared for the injection. Then, inferior alveolar nerve block was administered following the standard protocol (McDonald et al. 2016) by a single researcher (AM) (Figures 2 & 3).
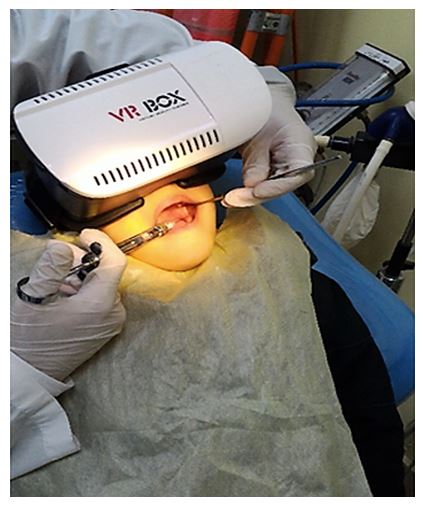
Figure 2: Use of AV eyeglasses ‘VR Box’ and wireless headphone for distraction
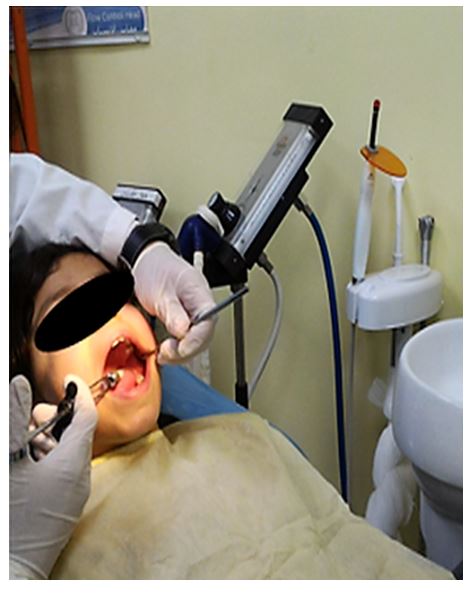
Figure 3: Use of video on tablet and wireless headphone for distraction
After anesthesia was given, the second pulse rate was recorded and the children were asked to choose a face that described their status from one of the Wong-Baker faces scale.
For each patient, all of the body responses were video recorded during the whole procedure and then were evaluated by an external evaluator to determine the children behavioral score according to FLAAC scale.
Statistical analysis: The statistical analysis was carried out using SPSS 21.0 software (SPSS, Inc, Chicago, Ill). One-way Anova was used to study the differences between the three groups according to behavioral scales scores (FLACC score, Wong-Baker faces scale and pulse rate).
Independent T-test was used to evaluate the three scales in all three groups according to gender. The differences were considered statistically significant when p-value was less than 0.05.
RESULTS
A total of 102 children, 101 children (60 boys and 41 girls, mean age 7.4) completed the study, whereas one patient was excluded duo to behavioral problems.
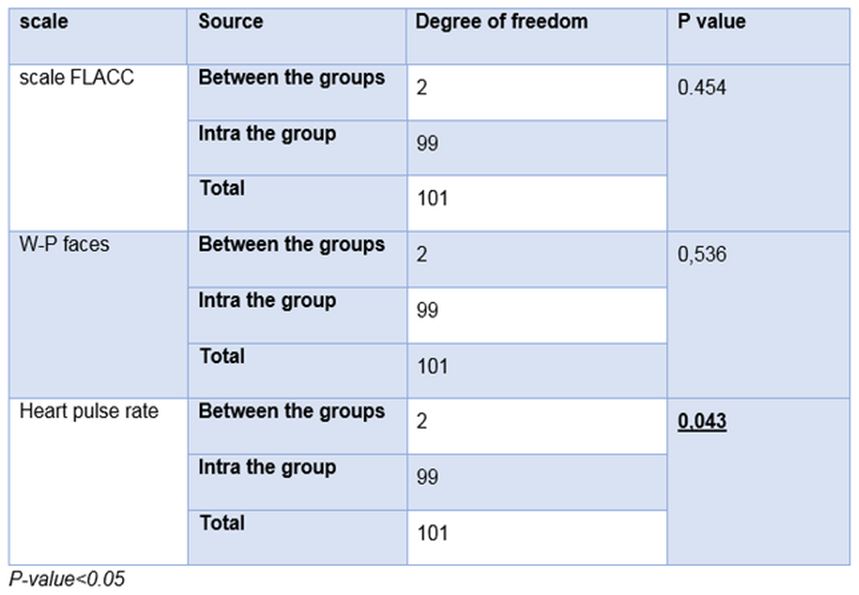
In all groups, pain and behavioral scales scores (Heart pulse rate, W-P faces, FLACC) were recorded. Normality of data was tested using Kolmogorov-Smirnov (Table 2). Then one-way Anova statistical test was done, significant difference was noticed between three groups in the heart pulse rate scale (P=0.0430) and no significant difference was noticed between three groups in the W-P faces (p = 0.536) and FLACC scales (p = 0.454) as shown in (Table 3).
Table 2: Normality of data using Kolmogorov-Smirnov table
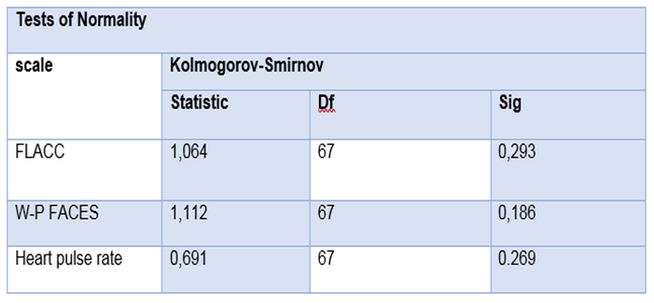
Table 3: One-way Anova to study the difference in the three scales in three groups
Bonferroni test was used for multiple-correction comparison for heart pulse rate results as shown in (Table 4).
Table 4: Bonferroni test for multiple-correction comparison for pulse rates
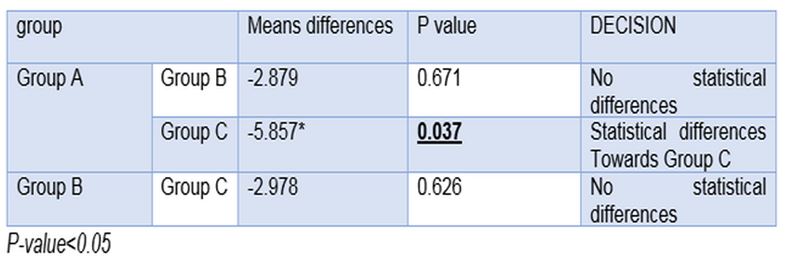
As noted in (Table 3), there was significant difference between Group A and Group C (p = 0.037). Nevertheless, there were no significant differences between Group A and Group B (p = 0.671) or between Group B and Group C (p = 0.626).
In control group, pulse rate was higher than in Group C. All Sig for Kolmogorov-Smirnov test were higher than 0.05, all date was normally distributed.
There were no statistical differences between the three groups in FLACC scale and W-P faces scale, however, statistical differences were founded in pulse rates between the three groups (Table 3).
DISCUSSION
In pediatric dentistry, there is a strong relationship between a child dental anxiety and successful dental treatment. Even more, the painful situations like needle insertion can result in fear and affect the behavioral of the child.15
The use of pharmacological aids can reduce the painful needle insertion into the tissue, as reported by Tugla et al. Benzocaine 20% gel has the best pain relieving effect for needle insertion in children.16 Non- pharmacological methods also have been reported as a valuable method in reliving dental anxiety, VR eyewear can be used as a distraction method and decrease the amount of the children’s anxiety during dental painful procedures.17
The use of pharmacological methods (topical anesthetic agent) along with non-pharmacological methods (AV distraction) has been considered as the best method in reducing needle insertion pain and child anxiety during dental anesthesia.18
Therefore, we used pharmacological method along with non-pharmacological methods during dental anesthesia in mandible (inferior alveolar nerve block).
Many researchers have used FLACC pain scale “Face–Leg–Activity–Cry-Consolability” to evaluate patient discomfort during treatment,13,19 and the Royal College for Nursing recommended using FLACC scale to evaluate the pain in over 3-year-old children regardless of their cooperation level (20).
As our study results show, the use of AV eyeglasses ‘VR Box’ has no added advantage in child behavioral management and pain relieving during IAN block on all three assessment scales.
On the other hand, many articles concluded that the use of AV eyeglasses ‘VR Box’ resulted in less pain and less anxiety. In those studies, they used the AV eyeglasses ‘VR Box’ during the whole treatment procedures including LA administration. Therefore, it might increase the duration of watching the video on AV eyeglasses ‘VR Box’, thereby, more time of watching VR. Since most of the procedures will become non-painful and will have no pain feeling after delivering LA.17,21,22
In addition, it has been noted in this study, that the use of AV eyeglasses ‘VR Box’ could be difficult to wear and it could block the practitioner vision of what’s inside the mouth, especially the IAN Block site. Thereby, the dental procedures will be more difficult. Although, other studies used VR eyeglasses on older children which may be easy to use with.23 VR eyeglasses might be helpful when used with special needs patients because it will block patient’s vision from dental equipment. Such as, autism patients who are afraid from dental chair light.21
In contrast to our finding, some studies have found that the use of AV eyeglasses may provide better distraction than watching video on screen.24 We noted that AV eyeglasses ‘VR Box’ had no added advantage in child behavioral management which was similar to the findings in the control group. This could be due to the fact that the use of AV eyeglasses ‘VR Box’ can block out the real world’s vision, thus increasing the child anxiety from the new and threatening surrounding environment. This was similar to the child anxiety which was faced by the children in the control group from the vision of the dental instruments.25
Nevertheless, audio visual distraction using tablet device, which was fixed to the dental chair, was superior in child behavioral management and pain control during IAN block compared to using AV eyeglasses ‘VR Box’ and control group.
However, another study found that watching cartoons on TV did not have any effect on distracting children during anesthesia or reducing their pain. The possible reason behind that, might be the younger children and there was no application of a topical anesthesia gel before the insertion of the needle. In addition to that, using wireless headphone in our study might have superior distraction effect. So that, the children were more focused on the shown cartoons (24). It was noted that pulse rate was lower in the tablet device group compared to AV eyeglasses ‘VR Box’ and the control group. This added advantage was duo to the useful audio and visual distraction from the dental instruments and no threatening vision block of the child patient.
LIMITATIONS
The limitation of this study was the inability of blinding the external investigator from child’s use of the AV eyeglasses ‘VR Box’. In addition, the size of the VR Box used in this study was a little too big for many children.
CONCLUSION
Within the limitations of this study it can be concluded that using video show on tablet device gave the best result in relieving dental anxiety and pain during IAN block in children.
Although the use of AV eyeglasses ‘VR Box’ had no added advantage in a majority of children, but it was more acceptable in patients of 8-10 years than younger ones and gave the children some exciting experiences which may lead to better behavior in the next dental visits.
Acknowledgment: This study has been carried out in the Dental College at Damascus University, which deserves a great appreciation for all academic and financial support.
Conflict of interest: None declared by the authors
Authors’ contribution: All of the authors took part in the conduct of study, manuscript preparation and editing.
REFERENCES
Pediatric Dentistry Department, Dental College, Damascus University, Al-Mazzeh Street, Damascus, (Syria)
Correspondence: Mohammed Nour Alhalabi, Al-Mazzeh Street, Pediatric Dentistry Department, Dental College, Damascus University, Damascus, (Syria); Mobile: +963946459369; E-mail: dr.m.nour.h@gmail.com
ABSTRACT
Aim: The aim of this study was to evaluate the effectiveness of two different audiovisual distraction techniques, e.g. audio-visual (AV) eyeglasses – virtual reality box (VR Box) or a Tablet) in the management of anxious pediatric patients during inferior alveolar nerve block (IAN) block.
Study design: A randomized clinical trial carried out on 102 children (60 boys and 42 girls) aged between 6 and 10 years (mean age of 7.4 years) to investigate the effect of using VR eyeglasses ‘VR Box’ and tablet device with wireless headphone in reducing the dental anxiety of children during IAN administration.
Methodology: 102 children were randomly divided into three groups; Group A (Control group): IAN administrated with basic behavior guidance techniques and without using any type of distraction aids. Group B: IAN administrated with using AV eyeglasses ‘VR Box’ and wireless headphone. Group C: IAN administrated with using tablet device and wireless headphones. The participants were selected from children attending the department of the pediatric dentistry at the Faculty of Dentistry, Damascus University, who required local anesthesia (LA) administration in the mandibular arch. All of the children who experienced an IAN block with/without distraction were assessed by using a combination of measures: Wong–Baker FACES (self-report), pulse rate (physiological) and behavior (using FLACC behavior rating scale (‘external evaluator’).
Results: 101 children completed the study out of 102 children. There was no statistically significant difference in the anxiety of audiovisual groups as reported by the Wong–Baker FACES values (p = 0.536) and FLACC scale (p = 0.454). However, there was a statistically significant difference in the anxiety and pain level in pulse rate (p = 0.043).
Conclusions: Distraction using video shown on tablet device was the best in relieving dental anxiety and pain during IAN block. Although using ‘VR Box’ had no added advantage in a majority of children, ‘VR Box’ was more acceptable in older patients (8-10 years) than younger patients and gave the children some exciting experiences which may lead to far better behavior in the next dental visits.
Keywords: Distraction; Behavior management; Children’s dental anxiety
Citation: Al-Halabi MN, Bshara N, AlNerabieah Z. Effectiveness of audio visual distraction using virtual reality eyeglasses versus tablet device in child behavioral management during inferior alveolar nerve block. Anaesth Pain & Intensive Care 2018;22(1):55-61
Received – 13 Nov 2017; Reviewed – 2 Feb 2018, 22 Feb 2018; Corrected - 25 Feb 2018; Accepted – 25 Feb 2018
INTRODUCTION
Researchers have found that one of the most provocation aspects of child behavior management is poor pain control. Even though it is challenging but it is important that clinicians must try their best to reduce pain and discomfort during dental treatment, especially injection procedure.1 In this regard ‘the needle’ is considered as the biggest reason of the pediatric dental patients’ fear.(2)
Dental fear and anxiety can have negative impact on the outcome of the dental treatment, even more on the patients’ oral health related to quality of life as many studies have reported.3-6 A variety of behavioral management techniques has emerged to manage dental fear including pharmacological and non-pharmacological methods.7 Previous studies have stated that use of distraction during dental treatment is useful to patients by reducing their distress and in turn decrease their perception of pain sensation especially during injections with local anesthesia.8
Most children could be made unaware of receiving the injection with the use of topical anesthetic, distraction and a good injection technique.9 It was observed that audiovisual distraction technique was superior in managing anxious pediatric dental patients than using audio distraction alone.10 Using audiovisual aids for distraction during dental injection can alleviate dental anxiety by distracting two types of sensations; hearing and seeing.11 Recently, several studies have shown that AV eyeglasses are effective in distracting pediatric patients during dental procedures.12,13
Therefore, the aim of this study was to evaluate the effectiveness of two different audiovisual distraction techniques (AV eyeglasses ‘VR Box’ vs. tablet) in the management of anxious pediatric patients during IAN block.
METHODOLOGY
The sample size was a total of 102 children, which was calculated using G-Power 3.1 statistical program with (α=0.05, and Power=0.95). The informed consent was taken from parents or legal guardians before the procedures were carried out.
The 102 subjects were randomized into 3 groups. A random allocation list was generated using a randomization website ‘Random.org’. This single-blind randomized clinical trial (RCT) was designed and conducted according to the CONSORT statement over a period of 6 months from April 2017 to October 2017.
The participants were selected from children attending the Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, based on the following inclusion criteria:
- age group between 6 and 10 years
- with no previous dental experience
- without any systemic or mental disorders
- who could be categorized under definitely positive or positive ratings of Frank scale
- who required LA administration in the mandibular arch (IAN block)
Tablet: The tablet (Innjoo F2™, China) capable of playing MP4 audio-visual files, was fixed on the hand of the dental chair using tablet holder (AboveTEK™ tablet holder, China)
Pain assessment scale: The Wong-Baker FACES pain rating scale was used in this study to measure pain after delivering inferior alveolar block injection. Children were asked to choose one of the scale’s faces that best described how they felt during the procedure (Figure 1).
Figure 1: Wong-Baker FACES pain rating scale
Behavior assessment scale: The ‘Face, Legs, Activity, Cry, Consolability’ scale (FLACC scale) was used in this study duo to the reliability that was proved by Dak-Albab et al., in Syrian Arab Republic.14
The following table provides the criteria for the FLACC Behavioral pain scale (Table 1).
Table 1: FLACC scale
| Behavior | 0 | 1 | 2 |
| Face | No particular expression or smile | Occasional grimace or frown, withdrawn, disinterested | Frequent to constant quivering chin, clenched jow |
| Legs | Normal position or relaxed | Uneasy, restless, tense | Kicking or legs drawn up |
| Activity | Lying quietly, normal position, moves easily | Squirming, shifting, back and forth, tense | Arched, rigid or jerking |
| Cry | No cry (awake or asleep) | Moans or whimpers; occasional complaint | Crying steadily, screams, sobs, frequent complaints |
| Consolability | Content, relaxed | Reassured by touching, hugging or being talked to, distractible | Difficult to console or comfort |
Pulse rate measures: The pulse rate was recorded for the first time when patients were seated on the dental chair and immediately after IAN block was finished. Then, the difference between the two measures was calculated.
Intervention: 102 children were randomized into three groups according to the distraction type:
Group A (Control group): IAN administrated with basic behavior guidance techniques and without using any type of distraction aids.
Group B: IAN administrated with using AV eyeglasses ‘VR Box’ and wireless headphone.
Group C: IAN administrated with using tablet device and wireless headphone.
For each child patient, a disposable oral examination kit and a traditional oral anesthesia kit (27-gauge long needle, 2 % lidocaine (1:100,000 epinephrine) solution, and an aspirating syringe) was used in this study.
In group B and C, children were asked to choose one episode of the popular cartoon series ─ ‘Tom and Jerry’, ‘Gumball’, ‘Pink Panther’ or ‘SpongeBob’. The first measure of pulse rate was recorded directly when the patient seated comfortably on the dental chair. Afterwards, a 20% benzocaine topical anesthetic gel was applied after drying the injection area for 30 seconds protocol (McDonald et al. 2016). During the application of the topical anesthetic, children were prepared for the injection. Then, inferior alveolar nerve block was administered following the standard protocol (McDonald et al. 2016) by a single researcher (AM) (Figures 2 & 3).
Figure 2: Use of AV eyeglasses ‘VR Box’ and wireless headphone for distraction
Figure 3: Use of video on tablet and wireless headphone for distraction
After anesthesia was given, the second pulse rate was recorded and the children were asked to choose a face that described their status from one of the Wong-Baker faces scale.
For each patient, all of the body responses were video recorded during the whole procedure and then were evaluated by an external evaluator to determine the children behavioral score according to FLAAC scale.
Statistical analysis: The statistical analysis was carried out using SPSS 21.0 software (SPSS, Inc, Chicago, Ill). One-way Anova was used to study the differences between the three groups according to behavioral scales scores (FLACC score, Wong-Baker faces scale and pulse rate).
Independent T-test was used to evaluate the three scales in all three groups according to gender. The differences were considered statistically significant when p-value was less than 0.05.
RESULTS
A total of 102 children, 101 children (60 boys and 41 girls, mean age 7.4) completed the study, whereas one patient was excluded duo to behavioral problems.
In all groups, pain and behavioral scales scores (Heart pulse rate, W-P faces, FLACC) were recorded. Normality of data was tested using Kolmogorov-Smirnov (Table 2). Then one-way Anova statistical test was done, significant difference was noticed between three groups in the heart pulse rate scale (P=0.0430) and no significant difference was noticed between three groups in the W-P faces (p = 0.536) and FLACC scales (p = 0.454) as shown in (Table 3).
Table 2: Normality of data using Kolmogorov-Smirnov table
Table 3: One-way Anova to study the difference in the three scales in three groups
Bonferroni test was used for multiple-correction comparison for heart pulse rate results as shown in (Table 4).
Table 4: Bonferroni test for multiple-correction comparison for pulse rates
As noted in (Table 3), there was significant difference between Group A and Group C (p = 0.037). Nevertheless, there were no significant differences between Group A and Group B (p = 0.671) or between Group B and Group C (p = 0.626).
In control group, pulse rate was higher than in Group C. All Sig for Kolmogorov-Smirnov test were higher than 0.05, all date was normally distributed.
There were no statistical differences between the three groups in FLACC scale and W-P faces scale, however, statistical differences were founded in pulse rates between the three groups (Table 3).
DISCUSSION
In pediatric dentistry, there is a strong relationship between a child dental anxiety and successful dental treatment. Even more, the painful situations like needle insertion can result in fear and affect the behavioral of the child.15
The use of pharmacological aids can reduce the painful needle insertion into the tissue, as reported by Tugla et al. Benzocaine 20% gel has the best pain relieving effect for needle insertion in children.16 Non- pharmacological methods also have been reported as a valuable method in reliving dental anxiety, VR eyewear can be used as a distraction method and decrease the amount of the children’s anxiety during dental painful procedures.17
The use of pharmacological methods (topical anesthetic agent) along with non-pharmacological methods (AV distraction) has been considered as the best method in reducing needle insertion pain and child anxiety during dental anesthesia.18
Therefore, we used pharmacological method along with non-pharmacological methods during dental anesthesia in mandible (inferior alveolar nerve block).
Many researchers have used FLACC pain scale “Face–Leg–Activity–Cry-Consolability” to evaluate patient discomfort during treatment,13,19 and the Royal College for Nursing recommended using FLACC scale to evaluate the pain in over 3-year-old children regardless of their cooperation level (20).
As our study results show, the use of AV eyeglasses ‘VR Box’ has no added advantage in child behavioral management and pain relieving during IAN block on all three assessment scales.
On the other hand, many articles concluded that the use of AV eyeglasses ‘VR Box’ resulted in less pain and less anxiety. In those studies, they used the AV eyeglasses ‘VR Box’ during the whole treatment procedures including LA administration. Therefore, it might increase the duration of watching the video on AV eyeglasses ‘VR Box’, thereby, more time of watching VR. Since most of the procedures will become non-painful and will have no pain feeling after delivering LA.17,21,22
In addition, it has been noted in this study, that the use of AV eyeglasses ‘VR Box’ could be difficult to wear and it could block the practitioner vision of what’s inside the mouth, especially the IAN Block site. Thereby, the dental procedures will be more difficult. Although, other studies used VR eyeglasses on older children which may be easy to use with.23 VR eyeglasses might be helpful when used with special needs patients because it will block patient’s vision from dental equipment. Such as, autism patients who are afraid from dental chair light.21
In contrast to our finding, some studies have found that the use of AV eyeglasses may provide better distraction than watching video on screen.24 We noted that AV eyeglasses ‘VR Box’ had no added advantage in child behavioral management which was similar to the findings in the control group. This could be due to the fact that the use of AV eyeglasses ‘VR Box’ can block out the real world’s vision, thus increasing the child anxiety from the new and threatening surrounding environment. This was similar to the child anxiety which was faced by the children in the control group from the vision of the dental instruments.25
Nevertheless, audio visual distraction using tablet device, which was fixed to the dental chair, was superior in child behavioral management and pain control during IAN block compared to using AV eyeglasses ‘VR Box’ and control group.
However, another study found that watching cartoons on TV did not have any effect on distracting children during anesthesia or reducing their pain. The possible reason behind that, might be the younger children and there was no application of a topical anesthesia gel before the insertion of the needle. In addition to that, using wireless headphone in our study might have superior distraction effect. So that, the children were more focused on the shown cartoons (24). It was noted that pulse rate was lower in the tablet device group compared to AV eyeglasses ‘VR Box’ and the control group. This added advantage was duo to the useful audio and visual distraction from the dental instruments and no threatening vision block of the child patient.
LIMITATIONS
The limitation of this study was the inability of blinding the external investigator from child’s use of the AV eyeglasses ‘VR Box’. In addition, the size of the VR Box used in this study was a little too big for many children.
CONCLUSION
Within the limitations of this study it can be concluded that using video show on tablet device gave the best result in relieving dental anxiety and pain during IAN block in children.
Although the use of AV eyeglasses ‘VR Box’ had no added advantage in a majority of children, but it was more acceptable in patients of 8-10 years than younger ones and gave the children some exciting experiences which may lead to better behavior in the next dental visits.
Acknowledgment: This study has been carried out in the Dental College at Damascus University, which deserves a great appreciation for all academic and financial support.
Conflict of interest: None declared by the authors
Authors’ contribution: All of the authors took part in the conduct of study, manuscript preparation and editing.
REFERENCES
- Schwartz S, Kupietzky A. local anesthesia. Behavior Management in Dentistry for Children, Second Edition. 2014:107-24.
- Soxman JA, Malamed SF. Local anesthesia for the pediatric. Handbook of Clinical Techniques in Pediatric Dentistry. 2015:5. [Free full text]
- Carrillo-Diaz M, Crego A, Romero‐Maroto M. The influence of gender on the relationship between dental anxiety and oral health‐related emotional well‐ International journal of paediatric dentistry. 2013;23(3):180-7. [Free full text]
- Klingberg G, Berggren U, Carlsson SG, Noren JG. Child dental fear: cause‐related factors and clinical effects. Eur J Oral Sci. 1995 Dec;103(6):405-12.[PubMed]
- Townend E, Dimigen G, Fung D. A clinical study of child dental anxiety. Behaviour research and therapy. 2000;38(1):31-46. [PubMed]
- Nuttall NM, Gilbert A, Morris J. Children's dental anxiety in the United Kingdom in 2003. Journal of dentistry. 2008;36(11):857-60. [Free full text]
- Klassen JA, Liang Y, Tjosvold L, Klassen TP, Hartling L. Music for pain and anxiety in children undergoing medical procedures: a systematic review of randomized controlled trials. Ambul Pediatr. 2008 Mar-Apr;8(2):117-28. doi: 10.1016/j.ambp.2007.12.005.. [PubMed] [Free full text]
- Al-Namankany A, Petrie A, Ashley P. Video modelling and reducing anxiety related to dental injections–a randomised clinical trial. Br Dent J. 2014 Jun;216(12):675-9. doi: 10.1038/sj.bdj.2014.497. [PubMed] [Free full text]
- Soxman JA. Handbook of clinical techniques in pediatric dentistry: John Wiley & Sons; 2015.
- Naithani M, Viswanath D. Child's dental anxiety: Management by audio and audio-Visual distraction technique-A comparative study. Universal Research Journal of Dentistry. 2014;4(2):101.
- Attar R, Baghdadi Z. Comparative efficacy of active and passive distraction during restorative treatment in children using an iPad versus audiovisual eyeglasses: a randomised controlled trial. European Archives of Paediatric Dentistry. 2015;16(1):1-8. [Free full text]
- Aminabadi NA, Erfanparast L, Sohrabi A, Oskouei SG, Naghili A. The impact of virtual reality distraction on pain and anxiety during dental treatment in 4-6 year-old children: a randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospects. 2012 Fall;6(4):117-24. doi: 10.5681/joddd.2012.025. [PubMed] [Free full text]
- El-Sharkawi HF, El-Housseiny AA, Aly AM. Effectiveness of new distraction technique on pain associated with injection of local anesthesia for children. Pediatr dentist. 2012;34(2):35E-8E.
- Dak-Albab R, Al-Monaqel MB, Koshha R, Shakhashero H, Soudan R. A comparison between the effectiveness of vibration with Dentalvibe and benzocaine gel in relieving pain associated with mandibular injection: a randomized clinical trial. Anaesth, Pain & Intensive Care. 2016;20(1). [Free full text]
- Milsom MK, Tickle M, Humphris GM, Blinkhorn A. The relationship between anxiety and dental treatment experience in 5-year-old children. British dental journal. 2003;194(9):503-6. [Free full text]
- Primosch RE, Rolland-Asensi G. Comparison of topical EMLA 5% oral adhesive to benzocaine 20% on the pain experienced during palatal anesthetic infiltration in children. Pediatr Dent. 2001 Jan-Feb;23(1):11-4.. [PubMed]
- Panda A. Effect of Virtual Reality Distraction on Pain Perception during Dental Treatment in Children. Children. 2017;5(3):1-4. [Free full text]
- AgArwAl N, DhAwAN J, KumAr D, Anand A, Tangri K. Effectiveness of Two Topical Anaesthetic Agents used along with Audio Visual Aids in Paediatric Dental Patients. Journal of clinical and diagnostic research. J Clin Diagn Res. 2017 Jan;11(1):ZC80-ZC83. doi: 10.7860/JCDR/2017/23180.9217.[PubMed] [Free full text]
- Voepel-Lewis T, Zanotti J, Dammeyer JA, Merkel S. Reliability and validity of the face, legs, activity, cry, consolability behavioral tool in assessing acute pain in critically ill patients. Am J Crit Care. 2010 Jan;19(1):55-61; quiz 62. doi: 10.4037/ajcc2010624. [PubMed] [Free full text]
- Polit DF, Beck CT. Nursing research: Generating and assessing evidence for nursing practice: Lippincott Williams & Wilkins; 2008.
- Bagattoni S, D'Alessandro G, Sadotti A, Alkhamis N, Piana G. Effects of audiovisual distraction in children with special healthcare needs during dental restorations: a randomized crossover clinical trial. Int J Paediatr Dent. 2018 Jan;28(1):111-120. doi: 10.1111/ipd.12304. [PubMed] [Free full text]
- Mitrakul K, Asvanund Y, Arunakul M, Paka‐Akekaphat S. Effect of audiovisual eyeglasses during dental treatment in 5–8 year‐old children. Eur J Paediatr Dent 2015; 16: 239– [Free full text]
- Al-Khotani A, Bello LA, Christidis N. Effects of audiovisual distraction on children’s behaviour during dental treatment: a randomized controlled clinical trial. Acta Odontol Scand. 2016 Aug;74(6):494-501. doi: 10.1080/00016357.2016.1206211. [PubMed] [Free full text]
- Cassidy KL, Reid GJ, McGrath PJ, Finley GA, Smith DJ, Morley C, et al. Watch needle, watch TV: Audiovisual distraction in preschool immunization. Pain Medicine. 2002;3(2):108-18. [PubMed] [Free full text]
- Fakhruddin KS, El Batawi H, Gorduysus MO. Effectiveness of audiovisual distraction with computerized delivery of anesthesia during the placement of stainless steel crowns in children with Down syndrome. Eur J Dent. 2017 Jan-Mar;11(1):1-5. doi: 10.4103/ejd.ejd_288_16. [PubMed] [Free full text]