Amanjot Singh , Jaskirat Kaur , Sarvjeet Kaur , Kewal Krishan Gupta
Author affiliations:
Guru Gobind Singh (GGS) Medical College & Hospital, Faridkot – 151203, Punjab, India.
Correspondence: Dr. Kewal Krishan Gupta; E-mail: doc_krishan31@yahoo.co.in; Phone: 91 9988316306
Abstract
Background & objectives: The laryngeal mask airway Supreme™ (LMA-S) is a new, single-use, supraglottic device that combines the functionality of the ProSeal™ and Fastrach™ airways. Till now, there have been conflicting results regarding the oropharyngeal leak pressure (OLP) of the LMA Supreme™ vs. the LMA ProSeal™, which is the major determinant of effective ventilation and airway protection during LMA use. We compared the safety and efficacy of the LMA ProSeal™ vs. the LMA Supreme™ in ambulatory surgeries.
Methodology: In this prospective, comparative trial, eighty adult patients undergoing elective surgery, were randomly allocated to one of the two groups: Group LMA–P (LMA ProSeal™ group) and Group LMA–S (LMA Supreme™ group) of 40 patients each. OLP, insertion times, number of insertion attempts, ease of insertion and pharyngolaryngeal morbidity were assessed. Statistical analysis was performed using SPSS version 21.0 software using Student’s t-test and Chi-square test. P < 0.05 was considered to be statistically significant.
Results: Oropharyngeal leak pressure in Group LMA–P (26.65 ± 1.59 cmH2O) was comparable to Group LMA–S (26.08 ± 1.67 cmH2O) and both provided adequate seal and effective ventilation. The mean effective airway time was significantly less in Group LMA–S as compared to Group LMA–P (14.80 ± 1.24 sec and 17.80 ± 1.47 sec) respectively. Mean number of successful insertion attempts, hemodynamic response and pharyngolaryngeal morbidity were comparable in both the groups.
Conclusion: Both LMA Supreme™ and LMA ProSeal™ are equally efficacious and safe for maintaining airway and ventilation in paralyzed patients. However, LMA Supreme™ is easier to insert with shorter effective airway time than LMA ProSeal™.
Abbreviations: SAD - Supraglottic airway device; ETI - Endotracheal intubation; LMA - Laryngeal mask airways; PPV - Positive pressure ventilation; OLP - oropharyngeal leak pressure
Key words: LMA ProSeal™, LMA Supreme™, Oropharyngeal leak pressure; Airway; Aieway management
Citation: Singh A, Kaur J, Kaur S, Gupta KK. Safety and efficacy of LMA Supreme™ vs. LMA ProSeal™ for ambulatory surgeries in adult patients. Anaesth. pain intensive care 2021;26(1):63-68. DOI: 10.35975/apic.v26i1.1769
Received: June 02, 2021, Reviewed: December 13, 2021, Accepted: December 15, 2021
Introduction
In modern era, supraglottic airway devices (SADs) have brought revolution in airway management filling a niche between the facemask and endotracheal tube in terms of both anatomical position and degree of invasiveness.1 The American Standards for Testing Materials (ASTM) Committee F29 on Anesthetic and Respiratory Equipment has defined SADs as “Airways that are intended to open, secure, and seal the supraglottic area to provide an unobstructed airway in spontaneously breathing or ventilated patients, typically during anesthetic procedures”.2
Endotracheal intubation (ETI) has been considered the conventional gold standard technique for securing the airway during general anesthesia. However, laryngoscopy and endotracheal intubation may be associated with considerable morbidities, ranging from minor side effects such as sore throat to more serious complications such as autonomic stimulation and difficult or failed intubation. In such scenario, an SAD offers an alternative airway option with distinct advantages including faster and easy placement, better hemodynamic stability along with continued oxygenation during induction and emergence,3 and lesser postoperative sore throat.4 Also for insertion of an SAD, the deeper planes of anesthesia and muscle relaxants are not required if compared to endotracheal intubation.
Second generation laryngeal mask airways (LMA) have been specially designed for providing high seal cuff for effective positive pressure ventilation (PPV) and protection against pulmonary aspiration with an added gastric port.5 This added gastric tube also allows quick clinical diagnosis of device misplacement after insertion and its removal. ProSeal™ laryngeal mask airway (LMA ProSeal™) is a reusable SGA, with a modified cuff made of silicone and a double tube arrangement.6 The LMA Supreme™ is an advanced form of the SGA which is disposable, made of polyvinylchloride (PVC) that shares attributes with Fastrach™ LMA, LMA Unique™ and LMA ProSeal™ .7
We compared the efficacy and safety of LMA ProSeal™ and LMA Supreme™, primarily in terms of oropharyngeal leak pressure (OLP); and ease of insertion, effective airway time, hemodynamic changes and complications as secondary outcomes for elective surgeries in adult patients.
Methodology
This prospective, randomized, comparative, clinical trial was conducted as per the Indian Council of Medical Research guidelines for biomedical research in human subjects and in accordance with the principles of Declaration of Helsinki 2013. After the Institutional Ethical Committee approval and registering the trial with the Clinical Trial Registry of India (CTRI/2019/10/021609), this study was conducted on 80 adult male and female patients of ASA Grade I or II, aged 21-55 y, scheduled for elective open surgeries under general anesthesia after their informed written consent. Patients with anticipated difficult airway, body mass index >30 kg/m2, an acute or chronic respiratory tract infection, increased risk of aspiration (gastroesophageal reflux disorder, hiatus hernia, and pregnancy), cervical spine fracture or instability, and undergoing head & neck surgery were excluded from the study.
Eighty patients were randomly allocated into two groups: in Group LMA–P (n = 40) airway was secured with LMA ProSeal™ and in Group S (n = 40) airway was secured with LMA Supreme™. Randomization was done by computer‑generated randomization program and allocation was done by the supervisor opening a sealed opaque envelope just prior to surgery. All device insertions were supervised by the senior anesthesiologists and performed by anesthesia trainees with a prior experience of at least 20 successful insertions of each of the devices. Selection of size of the device was as per manufacturer’s guidelines based on the patient’s weight.
A thorough preoperative assessment of the patient was done by an anesthesiologist and patients received premedication of tab. alprazolam 0.25 mg and tab. ranitidine 150 mg orally at night before surgery. All patients were kept fasting as per standard guidelines before surgery. After arrival of the patient in the operating room, standard monitors like ECG, pulse oximeter, and noninvasive blood pressure (NIBP) were attached and baseline parameters were recorded and intravenous (IV) infusion was started. Pre–medication with glycopyrrolate (0.004 mg/kg), ondansetron (0.15 mg/kg) and fentanyl (2 µg/kg) was given IV. After premedication, preoxygenation with 100% oxygen was done for 3 min. Patient was kept supine with the patient’s head in the neutral position and induced by intravenous propofol (2 mg/kg) and atracurium (0.5 mg/kg IV). After 3 min of manual ventilation, SAD was inserted according to the group allocation. The device was checked, inserted and secured according to the corresponding manufacturer’s recommendations. 2% lidocaine jelly was used as a lubricant for both airway devices and this was put on tip and posterior surface of the device. After insertion, the cuff of the device was inflated to an intracuff pressure of 60 cmH2O and maintained at that pressure throughout surgery. After securing the device, mechanical ventilation with isoflurane 0.8 - 1.0% in oxygen and nitrous oxide was started. An effective airway and ventilation was judged by square wave capnography with normal end tidal CO2 value and absence of audible gas leak. In both groups an appropriate sized lubricated nasogastric tube was inserted through the gastric drain channel.
An unblinded anesthesia resident collected data on the number of attempts for successful LMA insertion, the time taken and the ease of LMA insertion. The success of first attempt insertion was noted. If it was not possible to insert the device or ventilate through it, two more attempts of insertion were allowed. If placement failed even after three attempts, the airway was secured through endotracheal tube and the case was excluded from the study. Time taken for insertion was defined as the time between picking up the prepared supraglottic airway device and obtaining the first normal capnograph. Ease of insertion was decided by the attending anesthesiologist and was graded as very easy, easy and difficult.8 The OLP was determined after 10 min of induction by closing the expiratory valve of the circle system at a fixed gas flow of 3 L/min. For safety concerns, the maximum OLP of 40 cmH2O was allowed.
At the end of surgery, the anesthetic gas mixture was replaced with 100% oxygen. After the return of spontaneous ventilation, the reversant – a mixture of glycopyrrolate (0.002 mg/kg) and neostigmine (0.05 mg/kg) was given. The SAD was removed after the patient regained consciousness. Complications, e.g., blood staining of the device, any trauma to the mouth leading to dysphonia or dysphagia and sore throat were noted.
Statistical Analysis:
Sample size was calculated on the basis of OLP as primary outcome. Based on previous literature and 80% power along with 5% probability of type 1 error, total sample size of 80 patients (40 in each group) was considered adequate to detect the mean difference of 15% in this primary parameter. After completion of the study, all the results were analyzed by using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, N.Y., USA). Numerical variables were analyzed using Student’s unpaired t-test and Pearson’s chi square (χ2) test was used for categorical values. For all statistical analyses, p < 0.05 was considered as significant.
Results
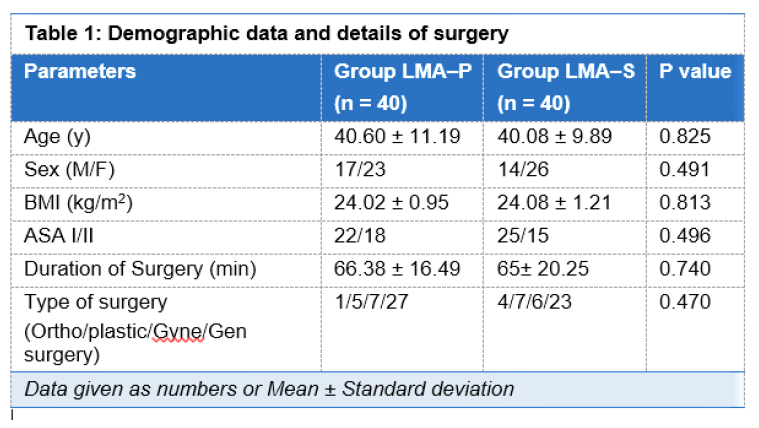
The study population consisted of 80 ASA I–II, patients posted for elective surgery under general anesthesia which were randomly divided into two groups of 40 each, and all the patients completed the study without any drop out. Regarding demographic parameters including age, sex, body mass index (BMI), ASA I- II status, duration of surgery and type of surgery, both the groups were comparable without statistical significant difference (Table 1). Hemodynamic parameters including HR, NIBP, SpO2 and EtCO2, measured just before insertion, just after insertion, for every minute for first 5 min and then every 10 min till the end of the surgery, found no statistically significant differences between the groups.
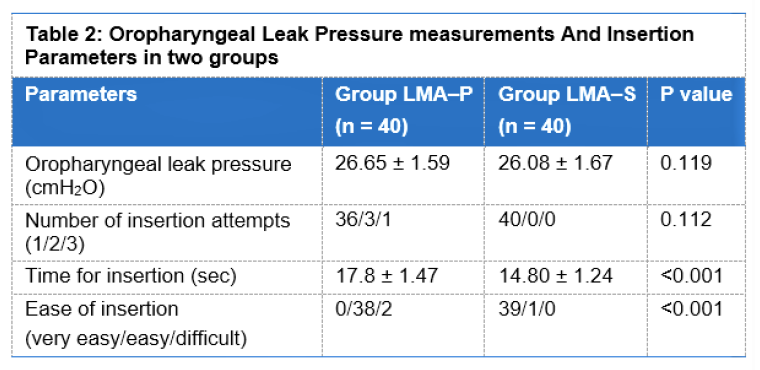
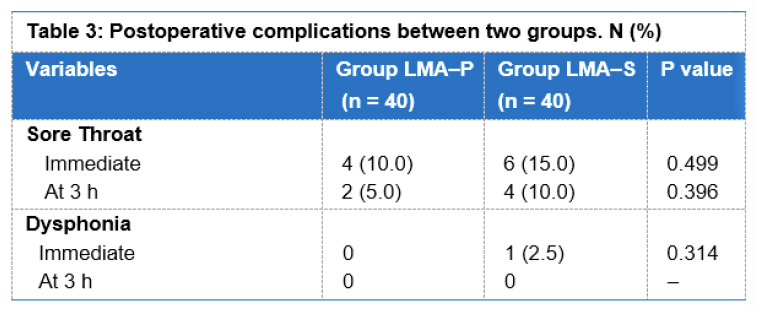
The mean value of OLP in Group LMA–P was 26.65 ± 1.59 cmH2O as compared to 26.08 ± 1.67 cmH2O in Group LMA–S. Both the groups showed comparable results. During insertion and establishment of the airway, the first insertion attempt was successful in 90% patients with LMA ProSeal™ and 100% patients with LMA Supreme™ (Table 2). The effective airway time for insertion of LMA Supreme™ was less than LMA ProSeal™ and difference between the two groups was statistically significant (Table 2). Regarding grade of ease of insertion, it was ‘very easy’ in 97.5% of the patients of Group LMA–S as compared to Group LMA–P where it was graded ‘easy’ in 95% of the patients; this difference was found to be statistically significant (Table 2). On inspection after removal of the device, no blood staining was found in any patient in both groups. No significant difference in postoperative throat complications was noted between the two groups except for a higher incidence of sore throat in Group LMA–P (Table 3).
Discussion
Supraglottic airway devices (SAD’s) have been a very significant addition to the airway management armamentarium and its application in elective or emergency surgeries and cardiopulmonary resuscitation has been constantly expanding.9 It is one of the major boons for difficult airway management. Presently there are numerous SAD’s with sealing mechanism: cuffed perilaryngeal sealers, cuffed pharyngeal sealers, cuffless anatomically preshaped sealers etc. However, Laryngeal Mask Airway (LMA) has been divided into three generations with different characteristic features. But the introduction of second generation LMA with gastric port to prevent aspiration has made the use of LMA in routine clinical practice safer.1 However, our search for an ideal SAD still continues, which must have high airway seal pressures during spontaneous and positive pressure ventilation, low resistance to the flow of gases and which offers protection against pulmonary aspiration including gastric drainage.10,11
In the present study we compared two second generation SADs: LMA ProSeal™ with LMA Supreme™ amongst 80 patients (aged 21- 55 years) who underwent general anesthesia with controlled ventilation of duration less than 2 h for elective surgeries. The study demonstrated that the OLP was comparable in the both the groups. The LMA Supreme™ was easier to insert and had a higher first attempt success rate and took less time to insert in comparison to the LMA ProSeal™. However no significant differences existed between the two groups with respect to the insertion of the gastric tube, effect on hemodynamic parameters and the incidence of postoperative complications.
The oropharyngeal leak pressure (OLP) is defined as the fresh gas pressure at the moment when audible sound of gas leakage from mouth was heard. OLP test is commonly performed to indicate efficacy and safety of SAD with respect to the feasibility of positive pressure ventilation and the degree of airway protection.12 A higher leak pressure suggests a better seal between surrounding soft tissues of the neck (including pharyngeal muscles) and the cuff of the mask. We observed that Group LMA–P was having almost similar OLP compared to Group LMA–S (Table 2) and the difference was statistically not significant (p > 0.05).
Clinical studies have compared the LMA Supreme™ and LMA ProSeal™ for OLP with conflicting results.7,13-16 Present results were in concordance with the results of Verghese C et al., who compared LMA ProSeal™ and LMA Supreme™ in 36 adult female patients with general anesthesia, neuromuscular block (NMB) and positive pressure ventilation (PPV). Here mean glottic seal pressure was 28.58 cmH2O in LMA ProSeal™ group and 28.47 cmH2O in LMA Supreme™ group which were comparable.7 Other studies done by Hosten T et al. and Tham et al., comparing LMA ProSeal™ and LMA Supreme™ had similar oropharyngeal leak pressures and comparable clinical performance of the LMA Supreme™ as a ventilator device with that of the LMA ProSeal™.13,14
In contrast to the current study, Belena M et al. had found that the mean OLP in the LMA ProSeal™ group was significantly higher than that in the LMA Supreme™ group (30.7 ± 6.2 vs. 26.8 ± 4.1 cmH2O; P < 0.01) in patients undergoing elective laparoscopic cholecystectomy.15 Similarly Lee AKY et al. also reported lower mean OLP in LMA Supreme™ group as compared to LMA ProSeal™ group (27.9 ± 4.7 vs. 31.7± 6.3 cmH2O, P = 0.007).16 However there was no difference in the ability to provide adequate ventilation and oxygenation during anesthesia. The higher OLP observed in LMA ProSeal™ may be because of its double cuff which is made of soft silicone rubber that readily conforms to the contours of the hypopharynx, compared with the polyvinyl chloride single cuff of the LMA Supreme™.
Present study shows that LMA Supreme™ is significantly easier to insert and the mean effective airway time is significantly shorter for Group LMA–S compared to Group LMA–P e.g., 14.80 ± 1.24 sec vs. 17.80 ± 1.47 sec respectively. This mean difference of 3 sec between the two devices might be of clinical importance in patients with airway changes. Similarly Zundert V et al. and Singh A et al. found that the LMA Supreme™ had a shorter effective airway time and easier insertion than the LMA ProSeal™ and I-Gel.17,18 We presume that the insertion time of LMA Supreme™ was probably shorter because of the feature of the anatomically shaped preformed airway tube with a thin wedge-shaped leading edge. By contrast, the LMA ProSeal™ has a dedicated metal introducer for insertion and the removal of this introducer before cuff inflation is an additional step which increases time of insertion compared with the LMA Supreme™. However, some clinical studies found no difference between ease of insertion and effective airway time with LMA Supreme™ and LMA ProSeal™ contrary to our results.16,18
We found that in the first attempt insertion success with LMA Supreme™ was 100% compared to LMA ProSeal™, which was 90%, but the mean numbers of successful attempts were comparable in both groups similar to other clinical studies.16,19 However, Belena M et al. found significant higher first success rate with LMA Supreme™ as compared to LMA ProSeal™.15
Regarding hemodynamics variables in our study both the groups were comparable at various time intervals with P > 0.05 and the results were in concordance with the study conducted by Anand LK et al. in 84 patients using LMA ProSeal™ and LMA Supreme™ in laparoscopic cholecystectomy.20
High intracuff pressure in LMAs may impede pharyngeal mucosal perfusion, and it may lead to pharyngolaryngeal complications. In the present study, mild sore throat was observed postoperatively at 0 h and at 3 h without any statistically significant difference between the two groups. The overall complication rate in our study was low in both groups and comparable to previous studies that evaluated the LMA Supreme™ and LMA ProSeal™.18,21
Limitations
Our study has some limitations. First, the anesthesiologist involved was not blind to the type of LMA used, and hence provided a possible source of bias. To palliate this factor, the postoperative observer and patients were blinded to the group assignment. Secondly, we did not use fiberoptic bronchoscope to evaluate the position of the airway tube in order to maintain the usual surgical turnover rate and also checking the placement by fiberoptic bronchoscopy has not been suggested as a pre-use check by the manufacturers. Thirdly, our study did not include children, obese and pregnant patients, so these results cannot be directly extrapolated to specific subgroups of patients. Fourthly, SADs were inserted in paralyzed patients, so OLP values might be low compared to non-paralyzed patients as reported previously.
Conclusion
We conclude that both, LMA Supreme™ and LMA ProSeal™ are suitable for maintaining airway and ventilation in paralyzed patients due to comparable OLP and low pharyngolaryngeal morbidity. However, LMA Supreme™ is easier to insert, and has shorter effective airway time than LMA ProSeal™.
Conflict of Interest
None declared by the authors. No internal or external funding was involved in the conduct of this study.
Authors’ contribution
DS, JK: Conduct of study, literature search, statistical analysis or manuscript writing & editing.
SK: Design & conduct of study, literature search, statistical analysis and manuscript reviewing
KK: Conduct of study, literature search, manuscript writing or manuscript editing
References
Author affiliations:
Guru Gobind Singh (GGS) Medical College & Hospital, Faridkot – 151203, Punjab, India.
Correspondence: Dr. Kewal Krishan Gupta; E-mail: doc_krishan31@yahoo.co.in; Phone: 91 9988316306
Abstract
Background & objectives: The laryngeal mask airway Supreme™ (LMA-S) is a new, single-use, supraglottic device that combines the functionality of the ProSeal™ and Fastrach™ airways. Till now, there have been conflicting results regarding the oropharyngeal leak pressure (OLP) of the LMA Supreme™ vs. the LMA ProSeal™, which is the major determinant of effective ventilation and airway protection during LMA use. We compared the safety and efficacy of the LMA ProSeal™ vs. the LMA Supreme™ in ambulatory surgeries.
Methodology: In this prospective, comparative trial, eighty adult patients undergoing elective surgery, were randomly allocated to one of the two groups: Group LMA–P (LMA ProSeal™ group) and Group LMA–S (LMA Supreme™ group) of 40 patients each. OLP, insertion times, number of insertion attempts, ease of insertion and pharyngolaryngeal morbidity were assessed. Statistical analysis was performed using SPSS version 21.0 software using Student’s t-test and Chi-square test. P < 0.05 was considered to be statistically significant.
Results: Oropharyngeal leak pressure in Group LMA–P (26.65 ± 1.59 cmH2O) was comparable to Group LMA–S (26.08 ± 1.67 cmH2O) and both provided adequate seal and effective ventilation. The mean effective airway time was significantly less in Group LMA–S as compared to Group LMA–P (14.80 ± 1.24 sec and 17.80 ± 1.47 sec) respectively. Mean number of successful insertion attempts, hemodynamic response and pharyngolaryngeal morbidity were comparable in both the groups.
Conclusion: Both LMA Supreme™ and LMA ProSeal™ are equally efficacious and safe for maintaining airway and ventilation in paralyzed patients. However, LMA Supreme™ is easier to insert with shorter effective airway time than LMA ProSeal™.
Abbreviations: SAD - Supraglottic airway device; ETI - Endotracheal intubation; LMA - Laryngeal mask airways; PPV - Positive pressure ventilation; OLP - oropharyngeal leak pressure
Key words: LMA ProSeal™, LMA Supreme™, Oropharyngeal leak pressure; Airway; Aieway management
Citation: Singh A, Kaur J, Kaur S, Gupta KK. Safety and efficacy of LMA Supreme™ vs. LMA ProSeal™ for ambulatory surgeries in adult patients. Anaesth. pain intensive care 2021;26(1):63-68. DOI: 10.35975/apic.v26i1.1769
Received: June 02, 2021, Reviewed: December 13, 2021, Accepted: December 15, 2021
Introduction
In modern era, supraglottic airway devices (SADs) have brought revolution in airway management filling a niche between the facemask and endotracheal tube in terms of both anatomical position and degree of invasiveness.1 The American Standards for Testing Materials (ASTM) Committee F29 on Anesthetic and Respiratory Equipment has defined SADs as “Airways that are intended to open, secure, and seal the supraglottic area to provide an unobstructed airway in spontaneously breathing or ventilated patients, typically during anesthetic procedures”.2
Endotracheal intubation (ETI) has been considered the conventional gold standard technique for securing the airway during general anesthesia. However, laryngoscopy and endotracheal intubation may be associated with considerable morbidities, ranging from minor side effects such as sore throat to more serious complications such as autonomic stimulation and difficult or failed intubation. In such scenario, an SAD offers an alternative airway option with distinct advantages including faster and easy placement, better hemodynamic stability along with continued oxygenation during induction and emergence,3 and lesser postoperative sore throat.4 Also for insertion of an SAD, the deeper planes of anesthesia and muscle relaxants are not required if compared to endotracheal intubation.
Second generation laryngeal mask airways (LMA) have been specially designed for providing high seal cuff for effective positive pressure ventilation (PPV) and protection against pulmonary aspiration with an added gastric port.5 This added gastric tube also allows quick clinical diagnosis of device misplacement after insertion and its removal. ProSeal™ laryngeal mask airway (LMA ProSeal™) is a reusable SGA, with a modified cuff made of silicone and a double tube arrangement.6 The LMA Supreme™ is an advanced form of the SGA which is disposable, made of polyvinylchloride (PVC) that shares attributes with Fastrach™ LMA, LMA Unique™ and LMA ProSeal™ .7
We compared the efficacy and safety of LMA ProSeal™ and LMA Supreme™, primarily in terms of oropharyngeal leak pressure (OLP); and ease of insertion, effective airway time, hemodynamic changes and complications as secondary outcomes for elective surgeries in adult patients.
Methodology
This prospective, randomized, comparative, clinical trial was conducted as per the Indian Council of Medical Research guidelines for biomedical research in human subjects and in accordance with the principles of Declaration of Helsinki 2013. After the Institutional Ethical Committee approval and registering the trial with the Clinical Trial Registry of India (CTRI/2019/10/021609), this study was conducted on 80 adult male and female patients of ASA Grade I or II, aged 21-55 y, scheduled for elective open surgeries under general anesthesia after their informed written consent. Patients with anticipated difficult airway, body mass index >30 kg/m2, an acute or chronic respiratory tract infection, increased risk of aspiration (gastroesophageal reflux disorder, hiatus hernia, and pregnancy), cervical spine fracture or instability, and undergoing head & neck surgery were excluded from the study.
Eighty patients were randomly allocated into two groups: in Group LMA–P (n = 40) airway was secured with LMA ProSeal™ and in Group S (n = 40) airway was secured with LMA Supreme™. Randomization was done by computer‑generated randomization program and allocation was done by the supervisor opening a sealed opaque envelope just prior to surgery. All device insertions were supervised by the senior anesthesiologists and performed by anesthesia trainees with a prior experience of at least 20 successful insertions of each of the devices. Selection of size of the device was as per manufacturer’s guidelines based on the patient’s weight.
A thorough preoperative assessment of the patient was done by an anesthesiologist and patients received premedication of tab. alprazolam 0.25 mg and tab. ranitidine 150 mg orally at night before surgery. All patients were kept fasting as per standard guidelines before surgery. After arrival of the patient in the operating room, standard monitors like ECG, pulse oximeter, and noninvasive blood pressure (NIBP) were attached and baseline parameters were recorded and intravenous (IV) infusion was started. Pre–medication with glycopyrrolate (0.004 mg/kg), ondansetron (0.15 mg/kg) and fentanyl (2 µg/kg) was given IV. After premedication, preoxygenation with 100% oxygen was done for 3 min. Patient was kept supine with the patient’s head in the neutral position and induced by intravenous propofol (2 mg/kg) and atracurium (0.5 mg/kg IV). After 3 min of manual ventilation, SAD was inserted according to the group allocation. The device was checked, inserted and secured according to the corresponding manufacturer’s recommendations. 2% lidocaine jelly was used as a lubricant for both airway devices and this was put on tip and posterior surface of the device. After insertion, the cuff of the device was inflated to an intracuff pressure of 60 cmH2O and maintained at that pressure throughout surgery. After securing the device, mechanical ventilation with isoflurane 0.8 - 1.0% in oxygen and nitrous oxide was started. An effective airway and ventilation was judged by square wave capnography with normal end tidal CO2 value and absence of audible gas leak. In both groups an appropriate sized lubricated nasogastric tube was inserted through the gastric drain channel.
An unblinded anesthesia resident collected data on the number of attempts for successful LMA insertion, the time taken and the ease of LMA insertion. The success of first attempt insertion was noted. If it was not possible to insert the device or ventilate through it, two more attempts of insertion were allowed. If placement failed even after three attempts, the airway was secured through endotracheal tube and the case was excluded from the study. Time taken for insertion was defined as the time between picking up the prepared supraglottic airway device and obtaining the first normal capnograph. Ease of insertion was decided by the attending anesthesiologist and was graded as very easy, easy and difficult.8 The OLP was determined after 10 min of induction by closing the expiratory valve of the circle system at a fixed gas flow of 3 L/min. For safety concerns, the maximum OLP of 40 cmH2O was allowed.
At the end of surgery, the anesthetic gas mixture was replaced with 100% oxygen. After the return of spontaneous ventilation, the reversant – a mixture of glycopyrrolate (0.002 mg/kg) and neostigmine (0.05 mg/kg) was given. The SAD was removed after the patient regained consciousness. Complications, e.g., blood staining of the device, any trauma to the mouth leading to dysphonia or dysphagia and sore throat were noted.
Statistical Analysis:
Sample size was calculated on the basis of OLP as primary outcome. Based on previous literature and 80% power along with 5% probability of type 1 error, total sample size of 80 patients (40 in each group) was considered adequate to detect the mean difference of 15% in this primary parameter. After completion of the study, all the results were analyzed by using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, N.Y., USA). Numerical variables were analyzed using Student’s unpaired t-test and Pearson’s chi square (χ2) test was used for categorical values. For all statistical analyses, p < 0.05 was considered as significant.
Results
The study population consisted of 80 ASA I–II, patients posted for elective surgery under general anesthesia which were randomly divided into two groups of 40 each, and all the patients completed the study without any drop out. Regarding demographic parameters including age, sex, body mass index (BMI), ASA I- II status, duration of surgery and type of surgery, both the groups were comparable without statistical significant difference (Table 1). Hemodynamic parameters including HR, NIBP, SpO2 and EtCO2, measured just before insertion, just after insertion, for every minute for first 5 min and then every 10 min till the end of the surgery, found no statistically significant differences between the groups.
The mean value of OLP in Group LMA–P was 26.65 ± 1.59 cmH2O as compared to 26.08 ± 1.67 cmH2O in Group LMA–S. Both the groups showed comparable results. During insertion and establishment of the airway, the first insertion attempt was successful in 90% patients with LMA ProSeal™ and 100% patients with LMA Supreme™ (Table 2). The effective airway time for insertion of LMA Supreme™ was less than LMA ProSeal™ and difference between the two groups was statistically significant (Table 2). Regarding grade of ease of insertion, it was ‘very easy’ in 97.5% of the patients of Group LMA–S as compared to Group LMA–P where it was graded ‘easy’ in 95% of the patients; this difference was found to be statistically significant (Table 2). On inspection after removal of the device, no blood staining was found in any patient in both groups. No significant difference in postoperative throat complications was noted between the two groups except for a higher incidence of sore throat in Group LMA–P (Table 3).
Discussion
Supraglottic airway devices (SAD’s) have been a very significant addition to the airway management armamentarium and its application in elective or emergency surgeries and cardiopulmonary resuscitation has been constantly expanding.9 It is one of the major boons for difficult airway management. Presently there are numerous SAD’s with sealing mechanism: cuffed perilaryngeal sealers, cuffed pharyngeal sealers, cuffless anatomically preshaped sealers etc. However, Laryngeal Mask Airway (LMA) has been divided into three generations with different characteristic features. But the introduction of second generation LMA with gastric port to prevent aspiration has made the use of LMA in routine clinical practice safer.1 However, our search for an ideal SAD still continues, which must have high airway seal pressures during spontaneous and positive pressure ventilation, low resistance to the flow of gases and which offers protection against pulmonary aspiration including gastric drainage.10,11
In the present study we compared two second generation SADs: LMA ProSeal™ with LMA Supreme™ amongst 80 patients (aged 21- 55 years) who underwent general anesthesia with controlled ventilation of duration less than 2 h for elective surgeries. The study demonstrated that the OLP was comparable in the both the groups. The LMA Supreme™ was easier to insert and had a higher first attempt success rate and took less time to insert in comparison to the LMA ProSeal™. However no significant differences existed between the two groups with respect to the insertion of the gastric tube, effect on hemodynamic parameters and the incidence of postoperative complications.
The oropharyngeal leak pressure (OLP) is defined as the fresh gas pressure at the moment when audible sound of gas leakage from mouth was heard. OLP test is commonly performed to indicate efficacy and safety of SAD with respect to the feasibility of positive pressure ventilation and the degree of airway protection.12 A higher leak pressure suggests a better seal between surrounding soft tissues of the neck (including pharyngeal muscles) and the cuff of the mask. We observed that Group LMA–P was having almost similar OLP compared to Group LMA–S (Table 2) and the difference was statistically not significant (p > 0.05).
Clinical studies have compared the LMA Supreme™ and LMA ProSeal™ for OLP with conflicting results.7,13-16 Present results were in concordance with the results of Verghese C et al., who compared LMA ProSeal™ and LMA Supreme™ in 36 adult female patients with general anesthesia, neuromuscular block (NMB) and positive pressure ventilation (PPV). Here mean glottic seal pressure was 28.58 cmH2O in LMA ProSeal™ group and 28.47 cmH2O in LMA Supreme™ group which were comparable.7 Other studies done by Hosten T et al. and Tham et al., comparing LMA ProSeal™ and LMA Supreme™ had similar oropharyngeal leak pressures and comparable clinical performance of the LMA Supreme™ as a ventilator device with that of the LMA ProSeal™.13,14
In contrast to the current study, Belena M et al. had found that the mean OLP in the LMA ProSeal™ group was significantly higher than that in the LMA Supreme™ group (30.7 ± 6.2 vs. 26.8 ± 4.1 cmH2O; P < 0.01) in patients undergoing elective laparoscopic cholecystectomy.15 Similarly Lee AKY et al. also reported lower mean OLP in LMA Supreme™ group as compared to LMA ProSeal™ group (27.9 ± 4.7 vs. 31.7± 6.3 cmH2O, P = 0.007).16 However there was no difference in the ability to provide adequate ventilation and oxygenation during anesthesia. The higher OLP observed in LMA ProSeal™ may be because of its double cuff which is made of soft silicone rubber that readily conforms to the contours of the hypopharynx, compared with the polyvinyl chloride single cuff of the LMA Supreme™.
Present study shows that LMA Supreme™ is significantly easier to insert and the mean effective airway time is significantly shorter for Group LMA–S compared to Group LMA–P e.g., 14.80 ± 1.24 sec vs. 17.80 ± 1.47 sec respectively. This mean difference of 3 sec between the two devices might be of clinical importance in patients with airway changes. Similarly Zundert V et al. and Singh A et al. found that the LMA Supreme™ had a shorter effective airway time and easier insertion than the LMA ProSeal™ and I-Gel.17,18 We presume that the insertion time of LMA Supreme™ was probably shorter because of the feature of the anatomically shaped preformed airway tube with a thin wedge-shaped leading edge. By contrast, the LMA ProSeal™ has a dedicated metal introducer for insertion and the removal of this introducer before cuff inflation is an additional step which increases time of insertion compared with the LMA Supreme™. However, some clinical studies found no difference between ease of insertion and effective airway time with LMA Supreme™ and LMA ProSeal™ contrary to our results.16,18
We found that in the first attempt insertion success with LMA Supreme™ was 100% compared to LMA ProSeal™, which was 90%, but the mean numbers of successful attempts were comparable in both groups similar to other clinical studies.16,19 However, Belena M et al. found significant higher first success rate with LMA Supreme™ as compared to LMA ProSeal™.15
Regarding hemodynamics variables in our study both the groups were comparable at various time intervals with P > 0.05 and the results were in concordance with the study conducted by Anand LK et al. in 84 patients using LMA ProSeal™ and LMA Supreme™ in laparoscopic cholecystectomy.20
High intracuff pressure in LMAs may impede pharyngeal mucosal perfusion, and it may lead to pharyngolaryngeal complications. In the present study, mild sore throat was observed postoperatively at 0 h and at 3 h without any statistically significant difference between the two groups. The overall complication rate in our study was low in both groups and comparable to previous studies that evaluated the LMA Supreme™ and LMA ProSeal™.18,21
Limitations
Our study has some limitations. First, the anesthesiologist involved was not blind to the type of LMA used, and hence provided a possible source of bias. To palliate this factor, the postoperative observer and patients were blinded to the group assignment. Secondly, we did not use fiberoptic bronchoscope to evaluate the position of the airway tube in order to maintain the usual surgical turnover rate and also checking the placement by fiberoptic bronchoscopy has not been suggested as a pre-use check by the manufacturers. Thirdly, our study did not include children, obese and pregnant patients, so these results cannot be directly extrapolated to specific subgroups of patients. Fourthly, SADs were inserted in paralyzed patients, so OLP values might be low compared to non-paralyzed patients as reported previously.
Conclusion
We conclude that both, LMA Supreme™ and LMA ProSeal™ are suitable for maintaining airway and ventilation in paralyzed patients due to comparable OLP and low pharyngolaryngeal morbidity. However, LMA Supreme™ is easier to insert, and has shorter effective airway time than LMA ProSeal™.
Conflict of Interest
None declared by the authors. No internal or external funding was involved in the conduct of this study.
Authors’ contribution
DS, JK: Conduct of study, literature search, statistical analysis or manuscript writing & editing.
SK: Design & conduct of study, literature search, statistical analysis and manuscript reviewing
KK: Conduct of study, literature search, manuscript writing or manuscript editing
References
- Cook TM, Howes B. Supraglottic airway devices: recent advances. Contin Educ Anaesth Crit Care Pain. 2011;2:56-61. DOI: 1093/bjaceaccp/mkq058
- Sharma B, Sahai C, Sood J. Extraglottic airway devices: technology update. Med Devices (Auckl). 2017;10:189-205. [PubMed] DOI: 2147/MDER.S110186
- Dyer RA, Llewellyn RL, James MF. Total iv anaesthesia with propofol and the laryngeal mask for orthopaedic surgery. Br J Anaesth. 1995;74:123‑ [PubMed] DOI: 10.1093/bja/74.2.123
- Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth. 2002;88:582‑ [PubMed] DOI: 10.1093/bja/88.4.582
- O’Connor CJ, Stix MS. Bubble solution diagnosis ProSeal insertion in the glottis. Anesth Analg. 2002; 94:1671– [PubMed] DOI: 10.1097/00000539-200206000-00065
- Brain AI, Verghese C, Strube PJ. The LMA ‘ProSeal’—A laryngeal mask with an oesophageal vent. Br J Anaesth. 2000;84:650‑ [PubMed] DOI: 10.1093/bja/84.5.650
- Verghese C, Ramaswamy B. LMA-Supreme- a new single-use LMA with gastric access: a report on its clinical efficacy. Br J Anaesth. 2008;101:405 [PubMed] DOI: 1093/bja/aen174
- Richez B, Saltel L, Banchereau F, Torrielli R, Cros AM. A new single use supraglottic airway device with a noninflatable cuff and an esophageal vent: an observational study of the i-gel. Anesth Analg. 2008;106:1137-9. [PubMed] DOI: 1213/ane.0b013e318164f062
- Timmermann A, Bergner UA, Russo SG. Laryngeal mask airway indications: new frontiers for second-generation supraglottic airways. Current Opinion in Anesthesiology. 2015;28: 717-726. [PubMed] DOI: 1097/ACO.0000000000000262
- Michálek P, Miller DM. Airway management evolution – in a search for an Ideal extraglottic airway device. Prague Med Rep. 2014;115:87–103. [PubMed] DOI: 14712/23362936.2014.40
- Dwivedi Y, Gupta A, Srivastava U, Jagar KD, Mohan A, Mangla S. Comparison of i-gel™, LMA Proseal™ and LMA Classic™ in spontaneously breathing pediatric patients. Anaesth Pain Intensive Care. 2016;20(2):176-181. [FreeFullText]
- Keller C, Brimbacombe JR, Keller K, Morris R. Comparison of four methods for assessing airway sealing pressure with the laryngeal mask airway in adult patients. Br J Anaesth. 1999;82:286-7. [PubMed] DOI: 1093/bja/82.2.286
- Hosten T, Gurkan Y, Ozdamar D, Tekin M, Toker K, Solak M. A new supraglottic airway device: LMA Supreme comparison with LMA Proseal. Acta Anaesthesiol Scand. 2009;53(7):852-7. [PubMed] DOI: 1111/j.1399-6576.2009.01986.x
- Tham HM, Tan SM, Woon KL, Zhao YD. A comparison of the supreme laryngeal mask airway with the proseal laryngeal mask airway in anesthetized paralyzed adult patients: a randomized crossover study. Can J Anaesth. 2010;57(7):672-8. [PubMed] DOI: 1007/s12630-010-9312-6
- Belena JM, Nunez M, Anta D, Carnero M, Gracia JL, Ayala J, et al. Comparison of laryngeal mask airway supreme and laryngeal mask airway proseal with respect to oropharyngeal leak pressure during laparoscopic cholecystectomy: a randomised controlled trial. Eur J Anaesthesiol. 2013;30:119-23. [PubMed] DOI: 1097/EJA.0b013e32835aba6a
- Lee AKY, Tey JBL, Lim Y, Sia ATH. Comparison of the single use LMA Supreme with the reusable Proseal LMA for anesthesia in gynaecological laparoscopic surgery. Anaesth Intensive Care. 2009;37:815-9. [PubMed] DOI: 1177/0310057X0903700537
- Zundert VT, Brimacombe JR. Similar oropharyngeal leak pressures during anaesthesia with i-gelTM, LMA-ProSealTM and LMA-SupremeTM laryngeal masks. Acta Anaesth Belg. 2012;63:35-41. [PubMed]
- Singh A, Bhalotra AR, Anand R. A comparative evaluation of ProSeal laryngeal mask airway, I-gel and Supreme laryngeal mask airway in adult patients undergoing elective surgery: A randomised trial. Indian J Anaesth. 2018;62:858-64. [PubMed] DOI: 4103/ija.IJA_153_18
- Gill RK, Tarat A, Pathak D, Dutta S. Comparative study of two laryngeal mask airways: proseal laryngeal mask airway and supreme laryngeal mask airway in anesthetized paralyzed adults undergoing elective surgery. Anesth Essays Res. 2017;11:23-27. [PubMed] DOI: 4103/0259-1162.177184
- Anand LK, Goel N, Singh M, Kapoor D. Comparison of the supreme and the proseal laryngeal mask airway in patients undergoing laparoscopic cholecystectomy: a randomized controlled trial. Acta Anaesthesiol Taiwan. 2016;54(2):44-50. [PubMed] DOI: 1016/j.aat.2016.03.001
- Maitra S, Khanna P, Baidya DK. Comparison of laryngeal mask airway Supreme and laryngeal mask airway Pro-Seal for controlled ventilation during general anesthesia in adult patients: systematic review with meta-analysis. Eur J Anaesthesiol. 2014;31:266-73. [PubMed] DOI: 10.1097/01.EJA.0000435015.89651.3d