Dedi Susila 1 , Ristiawan Muji Laksono 2
Author affiliation:
Abstract
Background & Objective: General anesthesia is commonly used during clavicular fracture surgery; however, it has been associated with hemodynamic fluctuations, airway and respiratory problems, stress response, and postoperative nausea and vomiting. We assessed the effectiveness and side effects of ultrasound-guided interscalene block when used for anesthesia and postoperative analgesia for clavicle fracture surgery.
Methodology: This study was conducted on 48 patients who were planned for clavicle fracture surgery. Patients were given premedication with midazolam 0.05 mg/kg and pethidine 0.5-1 mg/kg intramuscularly. Patients received ultrasound-guided interscalene block using nerve stimulator and 0.5% ropivacaine 30 ml or bupivacaine 0.375%. Postoperatively, almost all patients received non-steroidal anti-inflammatory drugs (NSAIDs) (COX–1 or COX–2). Postoperative pain was evaluated using a visual analog scale (VAS) at 12, 24, 36, and 48 h postoperatively. Patients received a rescue dose of intravenous fentanyl when the VAS > 4. Block was successful if the surgery was completed without shifting to general anesthesia. The data was analyzed using the T-test and Man Whitney-test using SPSS 20.
Result: 95.83% of patients received a successful block. The mean pre-operative VAS was 3.48 ± 1.27 and significantly decreased in the post-operative period; 1.48 ± 0.77 (12 h post-op), 1.79 ± 1.05 (24 h post-op), 1.21 ± 0.41 (36 h postop), and 1.04 ± 0.20 (48 h postoperative) (p=0.000). The preoperative and postoperative mean arterial pressure (MAP) and pulse rate of the patients remained stable. There was no incidence of nausea, vomiting, or other complications.
Conclusion: Ultrasound-guided interscalene block is effective and safe as an anesthetic and for postoperative analgesia in clavicle fracture surgery.
Key words: Clavicular fracture; Interscalene block; Analgesia; Anesthesia
Cittion: Susila D, Laksono RM. Ultrasound-guided interscalene block is effective for anesthesia and postoperative analgesia for clavicle fracture surgery. Anaesth. pain intensive care 2021;26(1):25–30 DOI: 10.35975/apic.v26i1.1762
Received: May 6, 2921, Reviewed: November 5, 2021, Accepted: December 21, 2021
Introduction
Clavicular fractures are commonly reduced using general anesthesia (GA). In several conditions, such as head trauma, pulmonary injury, and the associated comorbids, the patients are more at risk under GA, because of hemodynamic fluctuations, airway and respiratory disorders, stress response, and postoperative nausea and vomiting.1–3 Regional anesthesia might be used in clavicular fracture surgery as it provides excellent analgesia and relaxation. Also, it reduces the need for postoperative analgesia and thus speeding up the recovery.3
The fracture type and location also need to be considered. The interscalene block aims to block the brachial plexus at the C5, C6, and C7, which are expected to provide anesthesia in the skin area over the shoulder and clavicular bone. Clavicular fracture surgery may be performed using peripheral nerve block or combining interscalene plexus block with other nerve blocks, e.g., cervical plexus, supraclavicular nerve, and local infiltration of local anesthetic.1–4 By using ultrasound guidance (USG), it is hoped that the interscalene plexus block alone will be able to reach C5, C6, and C7 and be able to reach C3 and C4, sometimes to C2.5 By performing the interscalene block, patient safety is expected to be increased by minimizing intervention and the medication. The use of a single block also hopes to reduce patient care costs. We assessed the success rate, the effectiveness and the side effects of USG interscalene block as the sole anesthetic and the postoperative analgesia produced by it for clavicle fracture surgery.
Methodology
This study was conducted on 48 patients who had clavicle fractures and underwent surgical reduction during the previous two years. All of the patients signed informed consent to be included in the study. The study was approved by the Research Ethics Committee of Adi Husada Hospital (No. 234A/RSAH/XII/2019). All patients undergoing an elective reduction of fractures of the middle and outer third of the clavicle, age > 21 y, ASA I to III, were included in the study. Patients with clavicle fractures associated with other injuries such as neurological deficits of the brachial plexus, phrenic nerve paralysis; those allergic to local anesthesia (bupivacaine or ropivacaine); known to have blood coagulation disorders, severe pulmonary disorders, anatomical abnormalities, and infections in the neck area were excluded.
After attaching standard monitors, all patients were given premedication with inj. midazolam 0.05 mg/kg and inj. pethidine 0.5-1 mg/kg intramuscularly. The patients were positioned supine with the head turned slightly contralateral. The interscalene plexus block was done using USG. First, the interscalene plexus was identified by visualizing C5, C6, and C7 with USG. A 5 cm long 22G block needle was then inserted towards C5 with an in-plane technique, with confirmation with the nerve stimulator until twitching was obtained with less than 0.5 milliamp. Local anesthetic ropivacaine 0.5% or bupivacaine 0.375% 15 ml were injected at the C5, followed by 7.5 ml each at C6 and C7 (Figure 1).
During the surgery, the patient was given light sedation using midazolam 1-2 mg IV. Blood pressure, pulse, oxygen saturation were recorded every 5 min. The onset of local anesthesia was judged by loss of pain stimulation to pinprick in the supraclavicular area around the area to be operated on and loss of motor strength (the patient unable to lift or abduct his hand). During surgery, the potential side effects of the block were observed. All the possible side effects were examined by clinical examination, and, if necessary, a chest X-ray AP view was performed. During surgery, the need for analgesic drugs and local anesthetics for local infiltration were noted. Block was successful if the surgery was done without converting the anesthetic technique to GA.
The postoperative hemodynamic and pain level of patients were evaluated. Postoperative pain was assessed using VAS ranging from 0 (no pain) to 10 (severe unbearable pain). The evaluation was carried out at 12, 24, 36, and 48 h postoperatively. Patients received a rescue dose of fentanyl 1 µg/kg IV when the VAS > 4. The total number of rescue analgesics given for 24 h was recorded. Data were analyzed using an independent T-test and Mann Whitney-test using SPSS 20 (IMB
Statistic, USA) with CI 95% and p < 0.05 being significant.
Results
This demographic data of the patients, including age, height, weight and genders is given in Table 1.
In two (4.2 %) patients the anesthesia was converted to GA due to an incomplete block. The mean onset time and the mean surgery duration are shown in Table 2. No complication occured during the procedure.
Postoperatively, patients received NSAIDs (COX–1 or COX–2) once in 24 h and werecontinued with oral medications. The patients converted to GA, received
additional fentanyl analgesics and NSAID injections for two days. Pre-operatively, more than 90% of patients reported a VAS > 3. 38% of these patients experienced pain with VAS 3, 25% experience pain with VAS 4, and 23% experience pain with VAS > 4. The mean pre-operative VAS was 3.48 ± 1.27. Postoperative mean
VAS was 1.48 ± 0.77 (12 h), 1.79 ± 1.05 (24 h), 1.21 ± 0.41 (36 h), and 1.04 ± 0.20 (48 h) (p = 0.000). Postoperatively, more than 80% of the patients
experienced a decrease in pain intensity. The VAS scores at different postoperative periods are shown in Figure 2.
The Mean Arterial Pressure (MAP) and the heart rates of the patients remained stable throughout (Figure 3).
Discussion
During the recent past regional anesthesia has been revolutionized with the dvent of USG, which facilitates precise needle tip localization and real time observation of the injectate spread. The complication rate during the procedure has decreased to the minimal level, as in our study. Compared to an earlier study the mean onset of interscalene block using ropivacaine 0.375% was 13.3 and 21.37 min in upper limb surgery.7 This study supports the use of interscalene block in clavicle fracture surgery.
In our study, more than 90% of patients reported a VAS scale >3 (3-6) during pre-operative period. The mean VAS was significantly decreased postoperative, and in majority of the patients VAS 2 and VAS 1 were noted. The pain intensity decreased from moderately–severe to mild–no pain. The mean arterial pressure (MAP) and heart rate of all patients pre and postoperatively remained stable.8,9
Postoperative, patients were well managed with NSAIDs (COX–1 or COX–2) to thwart rebound pain and no narcotics were required. The prevalence of rebound pain after regional anesthesia is between 35%-42%..10 In 49.58% of patients who receive peripheral nerve block the rebound pain might be severe.11 Inadequate postoperative analgesia is associated with a bad outcome, including pulmonary and cardiovascular complications, and the development of postoperative chronic pain.12,13,14 The use of NSAIDs as adjuvants is considered to provide an effective analgesic.15 However, the studies regarding the combination of interscalene block and NSAID for postoperative analgesia in clavicle fracture surgery are limited. In our study, we prescribed NSAID that might have prolonged the block duration up to 48 h postoperative and decreased the VAS score to 1 (mild to no pain).
The brachial plexus is derived from C-5 to T-1 nerve roots. The brachial plexus block results in sensory and motor block of the corresponding dermatome levels. The brachial plexus is entirely wrapped in a fascial covering so that it is shaped like a tube; so that if an injection of adequate volume of local anesthetic is carried out in the tube, it will produce a complete block in the involved nerves in most of the cases.16
This plexus-covering tube is directly connected to the cervical plexus nerves. Injections in the interscalene groove as high as C-6 (cricoid level) usually results in an anesthetic block equally well in the lower cervical plexus.17,18 Interscalene brachial plexus block is more accurately called the cervicobrachial plexus block, as C-4, C-3 nerve roots, and often C-2 is also blocked by an injection of over 20 ml of local anesthetic.17
USG interscalene block has advantages over block using only nerve stimulators. The most important thing is that USG can ensure the local spread of the anesthetic around the brachial plexus under direct vision. Besides that, the amount of volume injected into the plexus can be reduced by DOIng multiple injections.17,19,20 And last but not the least, the risk of injury to the blood vessels and the nerves during the block can be reduced.
Using USG, the brachial plexus at the interscalene level looks to be lateral to the carotid artery between the anterior and medial scalenus muscles. The transducer is moved up and down until two or more brachial plexus trunks are seen between the two scalenus muscles. The brachial plexus is usually seen 1 – 3 cm deep beneath the skin.6
Some literature states that interscalene block is effective when used in lateral clavicle surgery.21,22 But it needs to be combined with cervical plexus block to obtain adequate analgesia for the clavicular surgery on the middle or 1/3 medial parts.23,24 The previous research mainly addresses the interscalene block as an anesthesia technique for clavicular fractures, but its use as an analgesic technique is not yet defined.25 Interscalene blocks using bupivacaine or ropivacaine can provide excellent relaxation and analgesia with a duration of action of 3-5 h and analgesic effect up to 18 h.26,27 Because of this prolonged analgesia, we chose the USG interscalene block for clavicular fractures surgery. Postoperative pain has distinct characteristics, the pain intensity bsing very high in the first 12-24 h and gradually decreases with time.27,28 In this study, USG interscalene block successfully controlled the pain 12-24 h postoperative.
Limitations
The study was carried out on a small number of study subjects, as the number of clavicle fracture surgeries is limited. We only performed 48 surgeries in the past two years. A multi-center study with large sample size is suggeted to provide sufficient data regarding the benefits of the combination of interscalene block and NSAIDs in prolonging blockade duration.
Conclusion
The interscalene block is effective as an anesthetic and postoperative analgesia for clavicle fracture surgery. There is no significant hemodynamic fluctuations in the pre and postoperative periods, and no complications have been observed.
Conflict of interest
The authors declare no conflict of interest. No external funding was involved in the study.
Authors’ contribution
DS: Concept, manuscript writing and editing, literature search, review
RML: Statistical analysis, manuscript writing and editing, literature search, review
References
Author affiliation:
- Department of Anesthesiology & Reanimation, Faculty of Medicine, Airlangga University, Dr. Soetomo General Hospital, Surabaya, East Java, Indonesia
- Department of Anesthesiology and Intensive Care, Faculty of Medicine, Brawijaya University, Dr. Saiful Anwar General Hospital, Malang, East Java, Indonesia.
Abstract
Background & Objective: General anesthesia is commonly used during clavicular fracture surgery; however, it has been associated with hemodynamic fluctuations, airway and respiratory problems, stress response, and postoperative nausea and vomiting. We assessed the effectiveness and side effects of ultrasound-guided interscalene block when used for anesthesia and postoperative analgesia for clavicle fracture surgery.
Methodology: This study was conducted on 48 patients who were planned for clavicle fracture surgery. Patients were given premedication with midazolam 0.05 mg/kg and pethidine 0.5-1 mg/kg intramuscularly. Patients received ultrasound-guided interscalene block using nerve stimulator and 0.5% ropivacaine 30 ml or bupivacaine 0.375%. Postoperatively, almost all patients received non-steroidal anti-inflammatory drugs (NSAIDs) (COX–1 or COX–2). Postoperative pain was evaluated using a visual analog scale (VAS) at 12, 24, 36, and 48 h postoperatively. Patients received a rescue dose of intravenous fentanyl when the VAS > 4. Block was successful if the surgery was completed without shifting to general anesthesia. The data was analyzed using the T-test and Man Whitney-test using SPSS 20.
Result: 95.83% of patients received a successful block. The mean pre-operative VAS was 3.48 ± 1.27 and significantly decreased in the post-operative period; 1.48 ± 0.77 (12 h post-op), 1.79 ± 1.05 (24 h post-op), 1.21 ± 0.41 (36 h postop), and 1.04 ± 0.20 (48 h postoperative) (p=0.000). The preoperative and postoperative mean arterial pressure (MAP) and pulse rate of the patients remained stable. There was no incidence of nausea, vomiting, or other complications.
Conclusion: Ultrasound-guided interscalene block is effective and safe as an anesthetic and for postoperative analgesia in clavicle fracture surgery.
Key words: Clavicular fracture; Interscalene block; Analgesia; Anesthesia
Cittion: Susila D, Laksono RM. Ultrasound-guided interscalene block is effective for anesthesia and postoperative analgesia for clavicle fracture surgery. Anaesth. pain intensive care 2021;26(1):25–30 DOI: 10.35975/apic.v26i1.1762
Received: May 6, 2921, Reviewed: November 5, 2021, Accepted: December 21, 2021
Introduction
Clavicular fractures are commonly reduced using general anesthesia (GA). In several conditions, such as head trauma, pulmonary injury, and the associated comorbids, the patients are more at risk under GA, because of hemodynamic fluctuations, airway and respiratory disorders, stress response, and postoperative nausea and vomiting.1–3 Regional anesthesia might be used in clavicular fracture surgery as it provides excellent analgesia and relaxation. Also, it reduces the need for postoperative analgesia and thus speeding up the recovery.3
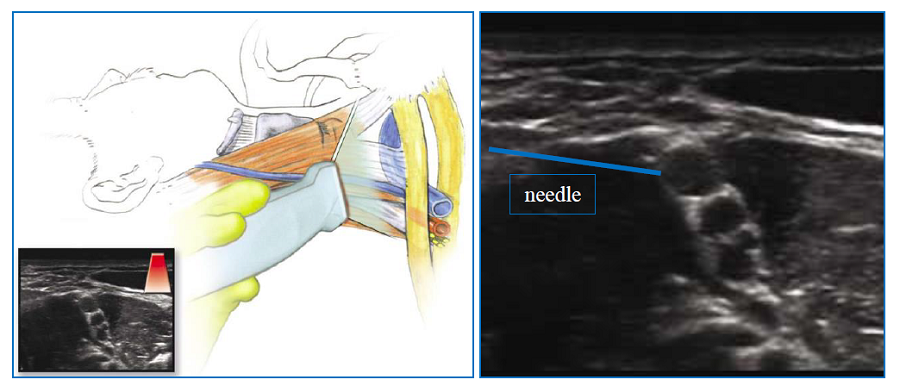 Figure 1: The brachial plexus block-USG guide6 |
Methodology
This study was conducted on 48 patients who had clavicle fractures and underwent surgical reduction during the previous two years. All of the patients signed informed consent to be included in the study. The study was approved by the Research Ethics Committee of Adi Husada Hospital (No. 234A/RSAH/XII/2019). All patients undergoing an elective reduction of fractures of the middle and outer third of the clavicle, age > 21 y, ASA I to III, were included in the study. Patients with clavicle fractures associated with other injuries such as neurological deficits of the brachial plexus, phrenic nerve paralysis; those allergic to local anesthesia (bupivacaine or ropivacaine); known to have blood coagulation disorders, severe pulmonary disorders, anatomical abnormalities, and infections in the neck area were excluded.
After attaching standard monitors, all patients were given premedication with inj. midazolam 0.05 mg/kg and inj. pethidine 0.5-1 mg/kg intramuscularly. The patients were positioned supine with the head turned slightly contralateral. The interscalene plexus block was done using USG. First, the interscalene plexus was identified by visualizing C5, C6, and C7 with USG. A 5 cm long 22G block needle was then inserted towards C5 with an in-plane technique, with confirmation with the nerve stimulator until twitching was obtained with less than 0.5 milliamp. Local anesthetic ropivacaine 0.5% or bupivacaine 0.375% 15 ml were injected at the C5, followed by 7.5 ml each at C6 and C7 (Figure 1).
During the surgery, the patient was given light sedation using midazolam 1-2 mg IV. Blood pressure, pulse, oxygen saturation were recorded every 5 min. The onset of local anesthesia was judged by loss of pain stimulation to pinprick in the supraclavicular area around the area to be operated on and loss of motor strength (the patient unable to lift or abduct his hand). During surgery, the potential side effects of the block were observed. All the possible side effects were examined by clinical examination, and, if necessary, a chest X-ray AP view was performed. During surgery, the need for analgesic drugs and local anesthetics for local infiltration were noted. Block was successful if the surgery was done without converting the anesthetic technique to GA.
The postoperative hemodynamic and pain level of patients were evaluated. Postoperative pain was assessed using VAS ranging from 0 (no pain) to 10 (severe unbearable pain). The evaluation was carried out at 12, 24, 36, and 48 h postoperatively. Patients received a rescue dose of fentanyl 1 µg/kg IV when the VAS > 4. The total number of rescue analgesics given for 24 h was recorded. Data were analyzed using an independent T-test and Mann Whitney-test using SPSS 20 (IMB
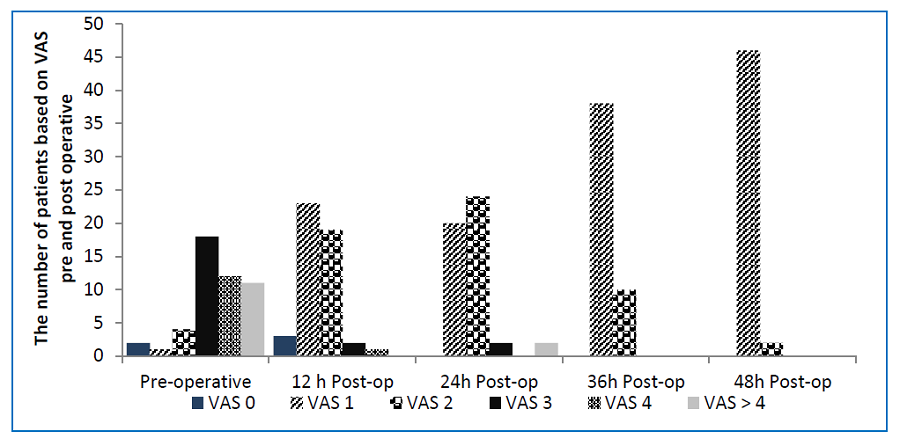 Figure 2: The number of patients based on the Visual Analogue Scale |
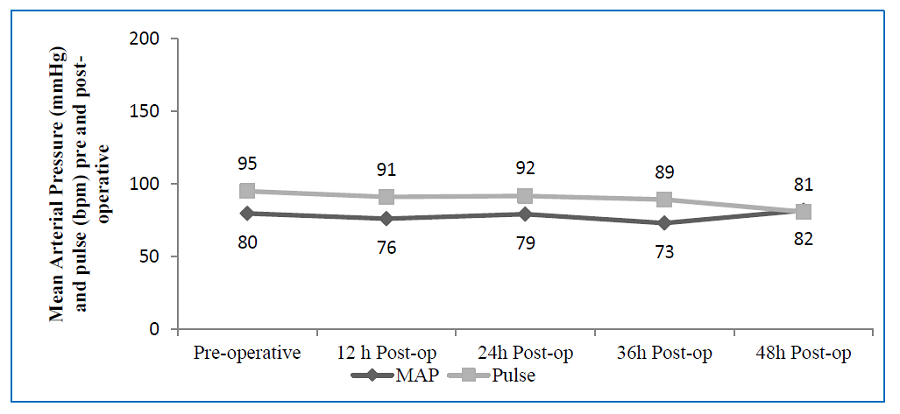 Figure 3. Mean Arterial Pressure and pulse rate pre and postoperative |
Results
This demographic data of the patients, including age, height, weight and genders is given in Table 1.
In two (4.2 %) patients the anesthesia was converted to GA due to an incomplete block. The mean onset time and the mean surgery duration are shown in Table 2. No complication occured during the procedure.
Postoperatively, patients received NSAIDs (COX–1 or COX–2) once in 24 h and werecontinued with oral medications. The patients converted to GA, received
| Table 1: Demographic data of the patients | |
| Parameter | Mean value |
| Age (y) | 39.55 ± 12.53 |
| Height (cm) | 167.42 ± 6.25 |
| Weight (kg) | 65.14 ± 12.44 |
| Gender · Male (n) (%) · Female (n) (%) |
38 (79.17) 10 (20.83) |
VAS was 1.48 ± 0.77 (12 h), 1.79 ± 1.05 (24 h), 1.21 ± 0.41 (36 h), and 1.04 ± 0.20 (48 h) (p = 0.000). Postoperatively, more than 80% of the patients
experienced a decrease in pain intensity. The VAS scores at different postoperative periods are shown in Figure 2.
The Mean Arterial Pressure (MAP) and the heart rates of the patients remained stable throughout (Figure 3).
| Table 2: Anesthesia parameter during surgery | |
| Parameter | Mean ± SD |
| Onset (min) | 17.14 ± 2.18 |
| Operation duration (min) | 81.5 ± 16.25 |
| Converted to GA (n) | 2 |
During the recent past regional anesthesia has been revolutionized with the dvent of USG, which facilitates precise needle tip localization and real time observation of the injectate spread. The complication rate during the procedure has decreased to the minimal level, as in our study. Compared to an earlier study the mean onset of interscalene block using ropivacaine 0.375% was 13.3 and 21.37 min in upper limb surgery.7 This study supports the use of interscalene block in clavicle fracture surgery.
In our study, more than 90% of patients reported a VAS scale >3 (3-6) during pre-operative period. The mean VAS was significantly decreased postoperative, and in majority of the patients VAS 2 and VAS 1 were noted. The pain intensity decreased from moderately–severe to mild–no pain. The mean arterial pressure (MAP) and heart rate of all patients pre and postoperatively remained stable.8,9
Postoperative, patients were well managed with NSAIDs (COX–1 or COX–2) to thwart rebound pain and no narcotics were required. The prevalence of rebound pain after regional anesthesia is between 35%-42%..10 In 49.58% of patients who receive peripheral nerve block the rebound pain might be severe.11 Inadequate postoperative analgesia is associated with a bad outcome, including pulmonary and cardiovascular complications, and the development of postoperative chronic pain.12,13,14 The use of NSAIDs as adjuvants is considered to provide an effective analgesic.15 However, the studies regarding the combination of interscalene block and NSAID for postoperative analgesia in clavicle fracture surgery are limited. In our study, we prescribed NSAID that might have prolonged the block duration up to 48 h postoperative and decreased the VAS score to 1 (mild to no pain).
The brachial plexus is derived from C-5 to T-1 nerve roots. The brachial plexus block results in sensory and motor block of the corresponding dermatome levels. The brachial plexus is entirely wrapped in a fascial covering so that it is shaped like a tube; so that if an injection of adequate volume of local anesthetic is carried out in the tube, it will produce a complete block in the involved nerves in most of the cases.16
This plexus-covering tube is directly connected to the cervical plexus nerves. Injections in the interscalene groove as high as C-6 (cricoid level) usually results in an anesthetic block equally well in the lower cervical plexus.17,18 Interscalene brachial plexus block is more accurately called the cervicobrachial plexus block, as C-4, C-3 nerve roots, and often C-2 is also blocked by an injection of over 20 ml of local anesthetic.17
USG interscalene block has advantages over block using only nerve stimulators. The most important thing is that USG can ensure the local spread of the anesthetic around the brachial plexus under direct vision. Besides that, the amount of volume injected into the plexus can be reduced by DOIng multiple injections.17,19,20 And last but not the least, the risk of injury to the blood vessels and the nerves during the block can be reduced.
Using USG, the brachial plexus at the interscalene level looks to be lateral to the carotid artery between the anterior and medial scalenus muscles. The transducer is moved up and down until two or more brachial plexus trunks are seen between the two scalenus muscles. The brachial plexus is usually seen 1 – 3 cm deep beneath the skin.6
Some literature states that interscalene block is effective when used in lateral clavicle surgery.21,22 But it needs to be combined with cervical plexus block to obtain adequate analgesia for the clavicular surgery on the middle or 1/3 medial parts.23,24 The previous research mainly addresses the interscalene block as an anesthesia technique for clavicular fractures, but its use as an analgesic technique is not yet defined.25 Interscalene blocks using bupivacaine or ropivacaine can provide excellent relaxation and analgesia with a duration of action of 3-5 h and analgesic effect up to 18 h.26,27 Because of this prolonged analgesia, we chose the USG interscalene block for clavicular fractures surgery. Postoperative pain has distinct characteristics, the pain intensity bsing very high in the first 12-24 h and gradually decreases with time.27,28 In this study, USG interscalene block successfully controlled the pain 12-24 h postoperative.
Limitations
The study was carried out on a small number of study subjects, as the number of clavicle fracture surgeries is limited. We only performed 48 surgeries in the past two years. A multi-center study with large sample size is suggeted to provide sufficient data regarding the benefits of the combination of interscalene block and NSAIDs in prolonging blockade duration.
Conclusion
The interscalene block is effective as an anesthetic and postoperative analgesia for clavicle fracture surgery. There is no significant hemodynamic fluctuations in the pre and postoperative periods, and no complications have been observed.
Conflict of interest
The authors declare no conflict of interest. No external funding was involved in the study.
Authors’ contribution
DS: Concept, manuscript writing and editing, literature search, review
RML: Statistical analysis, manuscript writing and editing, literature search, review
References
- Potsangbam S, Kay JP. Efficacy of combined interscalene block and superficial cervical plexus block for surgeries of the clavicle: a prospective observational study. J Clin Diagnostic Res. 2019;13(2):5-8. DOI: 7860/jcdr/2019/39856.12562
- Banerjee S, Acharya R, Sriramka B. Ultrasound-guided inter-scalene brachial plexus block with superficial cervical plexus block compared with general anesthesia in patients undergoing clavicular surgery: A comparative analysis. Anesth Essays Res. 2019;13(1):149-154. [PubMed] DOI: 4103/aer.AER_185_18
- Kay JP, Potsangbam S, Gangmei D, Singh LD, Khuo D, Kumaragurubaran TR. Comparison of combined superficial cervical plexus block (SCPB) and intercalene brachial plexus block (IBPB) with general anaesthesia (GA) in patients for clavicle surgery in terms of outcome in the immediate post-op period. IOSR-JDMS. 2018;17(10):33-40. [FreeFullText]
- Shanthanna H. Ultrasound guided selective cervical nerve root block and superficial cervical plexus block for surgeries on the clavicle. Indian J Anaesth. 2014;58(3):327-329. [PubMed] DOI: 4103/0019-5049.135050
- Zisquit J, Nedeff N. Interscalene Block. [Updated 2021 Sep 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519491/
- Brown DL. Atlas of Regional Anesthesia. 4th ed. Saunders Elsevier; 2014.
- Rathod H, Parikh H, Upadhayaya RM. Comparative study of 0.375% bupivacaine and 0.375% ropivacaine in brachial plexus block via supraclavicular approach. Int J Biomed Res. 2015;6(2):77-82. DOI: 7439/ijbr.v6i2.1601
- DeMers D WD. Physiology, Mean Arterial Pressure. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
- Pickering D. How to measure the pulse. Community Eye Heal J. 2013;26(82):37. [PubMed]
- Dawson S, Loewenstein SN. Severe rebound pain after peripheral nerve block for ambulatory extremity surgery is an underappreciated problem. Comment on Br J Anaesth 2021; 126: 862–71. Br J Anaesth. 2021;126(6):e204-e205. [PubMed] DOI: 1016/j.bja.2021.02.017
- Barry GS, Bailey JG, Sardinha J, Brousseau P, Uppal V. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br J Anaesth. 2021;126(4):862-871. [PubMed] DOI: 1016/j.bja.2020.10.035
- De Oliveira RM, Tenório SB, Tanaka PP, Precoma D. Control of pain trough epidural block and incidence of cardiac dysrhythmias in postoperative period of thoracic and major abdominal surgical procedures: a comparative study. Rev Bras Anestesiol. 2012;62(1):10-18. DOI: 1590/S0034-70942012000100003
- Shea RA, Brooks JA, Dayhoff NE, Keck J. Pain intensity and postoperative pulmonary complications among the elderly after abdominal surgery. Hear Lung. 2002;31(6):440-449. [PubMed] DOI: 1067/mhl.2002.129449
- Fletcher D, Stamer UM, Pogatzki-Zahn E, Zaslansky R, Tanase NV, Perruchoud C, et al. Chronic postsurgical pain in Europe: An observational study. Eur J Anaesthesiol. 2015 Oct;32(10):725-34. [PubMed] DOI: 1097/EJA.0000000000000319
- Edinoff AN, Houk GM, Patil S, et al. Adjuvant drugs for peripheral nerve blocks : the role of alpha-2 agonists , dexamethasone , midazolam , and non-steroidal anti-inflammatory drugs. Anesth Pain Med. 2021 Jul 4;11(3):e117197. [PubMed] DOI: 5812/aapm.117197
- Tiwari P, Avhad V, Mathkar S, Kane D. Prolonged interscalene blockade for 30 hours with 0.5% plain bupivacaine in a case of shoulder arthroscopy. Turk J Anaesthesiol Reanim. 2019 Oct;47(5):423-425. [PubMed] DOI: 5152/TJAR.2019.80217
- Mackey S, Amador E. Stanford Anesthesiology Regional Anesthesia Syllabus; 2002.
- Centre For Anesthesia and Critical Care Medicine. Interscalene Block; 2020. Available from: https://www.ucl.ac.uk/anaesthesia/uclhregional/interscalene-block
- Hadzic A, Vloka J. Peripheral Nerve Blocks Principles and Practice. McGraw Hill; 2014.
- Hadzic A. Hadzic, Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia.2nd McGraw Hill Education; 2012.
- Olofsson M, Taffé P, Kirkham KR, Vauclair F, Morin B, Albrecht E. Interscalene brachial plexus block for surgical repair of clavicle fracture: A matched case-controlled study. BMC Anesthesiol. 2020;20(1):1-6. [PubMed] DOI: 1186/s12871-020-01005-x
- Carter J, Bhat A. Ultrasound Guided Interscalene Brachial Plexus Block. Anaesthesia Tutorial of The Week 233. Department of Anaesthesia Queen Elizabeth Hospital, King ' s Lynn. Ultrasound; 2011 Jul 25. Available from: http://www.csen.com/brach.pdf
- Choi DS, Atchabahian A, Brown AR. Postoperative Analgesia for Clavicle Open Reduction and Internal Fixation with Classic and Modified Cervical Plexus Block, Figure: 1; 2020. [FreeFullText]
- Pal A, Dawar N, Biswas R, Biswas C. A combination of interscalene brachial plexus block and superficial cervical plexus block for fracture clavicle surgery in a patient with dilated. Ind Anaesth Forum. 2011;(August):1-3.
- Balaban O, Dülgeroǧlu TC, Aydin T. Ultrasound-guided combined interscalene-cervical plexus block for surgical anesthesia in clavicular fractures: a retrospective observational study. Anesthesiol Res Pract. 2018;2018:7842128. [PubMed] DOI: 1155/2018/7842128
- Review Course Lectures Presented at the 82nd Clinical and Scientific Congress of the International Anesthesia Research Society San Francisco, California; 2008. [FreeFullText]
- Becker DE, Reed KL. Local anesthetics: review of pharmacological considerations. Anesth Prog. 2012;59(2):90-101. [PubMed] DOI: 2344/0003-3006-59.2.90
- Tighe PJ, King CD, Zou B, Fillingim RB. Time to onset of sustained postoperative pain relief (SuPPR): evaluation of a new systems-level metric for acute pain management. Clin J Pain. 2016 May;32(5):371-9. [PubMed] DOI: 1097/AJP.0000000000000285