Ahmad Tajuddin Mat Yusoff 1 , Wan Mohd Nazaruddin Wan Hassan1 , Mohd Hasyizan Hassan1 , Muhamad Saiful Bahri Yusoff2 , Wan Fadzlina Wan Muhd Shukeri1 , Najib Majidi Yaacob3
Authors affiliations:
Abstract
Background: It has been observed that some candidates do very well in postgraduate examinations and get through in the very first attempt, whereas the others may not do very well and have to go for multiple attempts to get through the same examination. This study aimed to determine the factors affecting the performance and the success rate in the first attempt in the Master of Medicine (Anesthesiology) Part–1 examination.
Methodology: This was a cross-sectional study involving 73 postgraduate candidates who passed the Master of Medicine (Anesthesiology) Part–1 examination between 2016 and 2017. The candidates were required to respond to various questions about various factors assumed to be affecting their performance, including sociodemographic factors, pre–training, and in–training factors. Statistical analysis of the received responses was done and linked to the performance in the Part-1 examination.
Results: The candidates with more than 5 y of medical service had 85% lower odds than those with 5 or fewer years (adjusted OR 0.15; 95% CI 0.03–0.81; p = 0.027). Those who passed the entrance examination after 2 or more attempts also had 80% lower odds than those who passed at the first attempt (adjusted OR 0.20; 95% CI 0.06–0.70; p = 0.011). The odds of the candidates who often had small-group discussions during their study leave were 16.21 times higher to pass than those who seldom had any discussion (adjusted OR 16.21; 95% CI 1.81–145.41; p = 0.013).
Conclusions: The success in the Master of Medicine (Anesthesiology) Part–1 examination in first attempt was determined by a shorter duration of medical service, single attempt at the entrance examination, and regular small-group discussions.
Key words: Anesthesiology; Postgraduate; Medicine; Examination; Candidate
Abbreviations: UKM – Universiti Kebangsaan Malaysia; USM – Universiti Sains Malaysia; OSCE – Objective Structured Clinical Examination; SPM – Sijil Pelajaran Malaysia
Citation: Yusoff ATM, Hassan WMNW, Hassan MH, Yusoff MSB, Shukeri WFWM, Yaacob NM. A study of the factors affecting the academic performance of postgraduate examinees in the Master of Medicine (Anesthesiology) Part-1 examination. Anaesth. pain intensive care 2021;25(4):478–486.
DOI: 10.35975/apic.v25i4.1568
Received: April 16, 2021, Reviewed: May 30, 2021, Accepted: 2 June 2021
Introduction
The Master of Medicine in Anesthesiology (MMed-Anesthesiology) is a postgraduate clinical program in Malaysia that was established in 1988, with the main objective of producing more anesthesiologists in Malaysia using a structured training program. In the beginning, there were two different systems running independently according to the curriculum decided by each university. The curriculum that was initiated jointly by the University of Malaya (UM) and Universiti Kebangsaan Malaysia (UKM) in 1988 mostly resembled the format of the Australia–New Zealand examination, whereas the curriculum by Universiti Sains Malaysia (USM) in 1993 was similar to the format of the UK examination.
The format of the MMed-Anesthesiology UM–UKM examination consisted of an aptitude test at 6th month of enrollment, followed by the Part–1 examination at 18 months and the Part–2 examination at the end of the 4th year. The Part–1 examination comprised of a written part and viva voce in 2 main subjects – physiology/clinical measurement and pharmacology, which were assessed separately.
On the contrary, the format of the MMed-Anesthesiology USM examination was slightly different. The Part-1 examination was taken at the end of year 1, and the Part-2 examination was at the end of the year 4 without any aptitude test. The format of the examination consisted of theory and clinical examination in the form of short cases and viva voce, as well as the Objective Structured Clinical Examination (OSCE). All subjects were combined in one theory paper, and there was no separation between physiology and pharmacology.
The move to standardize the MMed-Anesthesiology program in Malaysia was initiated by the formation of the Conjoint Board Committee consisting of the 3 main universities, UM–UKM–USM, in order to standardize the quality of training and skills of anesthesiologists in Malaysia. After a few years, 2 other main universities—Universiti Putra Malaysia and International Islamic University of Malaysia—also joined the committee. The decision to standardize training and examination focused more on mutual understanding and a paradigm shift in clinical specialty training at that time toward the conjoint program of the main universities in Malaysia. There is no previous study comparing the effectiveness of 2 different systems of anesthesiology training in Malaysia. According to a study by Bowhay and Watmough on the first part of the Fellowship of the Royal College of Anaesthetists (FRCA) examination, notable change in the curriculum did not lead to performance deterioration in postgraduate examination in medical schools in the United Kingdom.1 The first Conjoint Examination for Part-2 was started in 2008, and the Part-1 was started in 2014. The format of the Part-1 examination adopted more of the old format of the MMed-Anesthesiology UM–UKM examination with the omission of the aptitude test, and the examination was conducted at the end of the year 1. There are 2 main subjects in the Part-1 Examination, which are pharmacology and physiology/clinical measurement. Each subject consists of theory and viva. Theory consists of 80 multiple-choice questions (MCQs) and 6 short-answer questions (SEQs), and the candidates must pass the theory examination to be able to proceed to the viva for each subject. The candidates are considered to have passed the Part-1 examination if they clear all sections for both subjects. Those who fail the examination repeat only the failed subject, and 3 consecutive repeat examinations are allowed for each candidate, with 1 extra appeal if still unable to pass after 3 repeat examinations.
The Part-1 Conjoint Examination is considered tough, and the passing rate has been around 30%–50% since the first examination. As stated by Bowhay and Watmough in their study, passing the primary FRCA examination at the first attempt for graduates of each medical school is very difficult, and the average pass percentage was 56.1%.1 There are many potential factors that might be affecting the performance of postgraduate candidates. Lane et al. stated that individual proficiency mediated the relationship between performance accomplishments and academic performance of postgraduate students.2
This study determined the factors affecting the pass percentage at the first attempt of the Part–1 MMed-Anesthesiology examination, including sociodemographic, pre–training, and in–training aspects.
.
Methodology
This is a cross-sectional study conducted after obtaining approval from the Institutional Ethics Committee (USM/JEPeM approval code: 17090413) and written consent from the candidates. The inclusion criteria were postgraduate students in USM who passed their Part–1 Conjoint Examination for MMed-Anesthesiology between 2016 and 2017, and the exclusion criteria involved those who passed the Part-1 examination using the old format of examination.
A total of 73 eligible candidates were included in this study, and the group that passed the Part–1 examination at the first attempt and the group that required multiple attempts to pass were compared. All the candidates were required to respond to questionnaires online, with a timeline of one week. The questionnaires were self-administered, and the duration to answer these questionnaires was about 20 min. They contained 35 items and were divided into 6 parts:
Part–1: The demographic data and socioeconomic background of the candidates
Part 2: The academic background before joining the program, including the Malaysian Certificate of Education for secondary school or well known as the “Sijil Pelajaran Malaysia” (SPM) result
Part 3: The background of medical service before joining MMed-Anesthesiology training
Part 4: The background of MMed-Anesthesiology training
Part 5: The assessment of facilities for study and clinical training, availability of teaching program, involvement of academic supervisor, involvement of other specialists, adequacy of time to study, and
.
allocation of time to study per day. These factors were initially assessed in 5 grades: (i) very poor, (ii) poor, (iii) fair, (iv) good, and (v) excellent. These were further narrowed down to 2 groups: (i) very poor to fair and (ii) good to excellent
Part 6: The assessment of the availability of small discussion groups, regularity in attending scheduled classes, regularity of impromptu discussions with seniors, regularity of practicing past-year questions, availability of extra classes, availability of small-group discussions during study leave, frequency of going home late from work, level of happiness while working with colleagues, level of energy during working, and availability of time to meet family members. These factors were assessed in 7 categories: (i) never, (ii) a few times per year or less, (iii) once a month or less, (iv) a few times per month, (v) once a week, (vi) a few times per week, and (vii) every day. These were further narrowed down to 2 groups: (i) seldom (never to once a month) and (ii) often (a few times per month to every day).
Data were analyzed using SPSS Statistics (v.25; IBM Corp. Armonk, NY, USA). All the factors were initially analyzed using the simple logistic regression (SLR) test, and the factors that had a p < 0.25 were included in the multiple logistic regression (MLR) test. A p < 0.05 was considered statistically significant.
Results
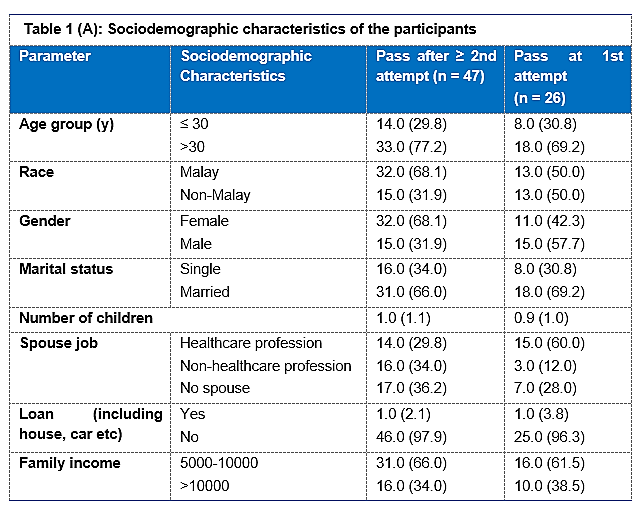
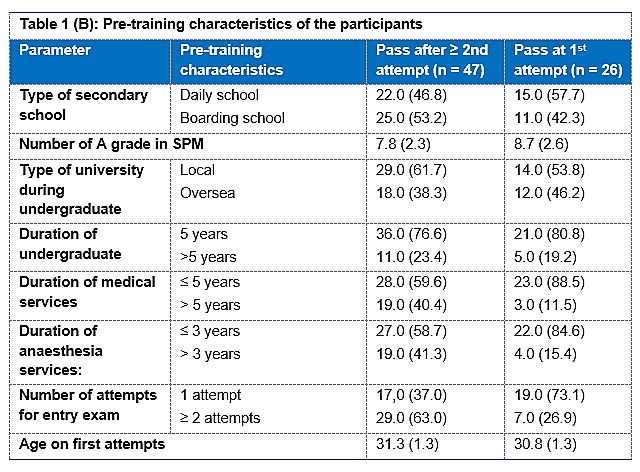
The eligible candidates were 73 and the survey response rate was 100%. The descriptive statistics of sociodemographic, pre–training, and in–training factors are presented in Tables 1 (A, B and C).
On the basis of the SLR test, there were few factors that had a p < 0.25 that was significant to proceed for the MLR test. Significant factors in sociodemographic characteristics were gender, race, and spouse’s profession (Table 2).
Significant factors in pre–training characteristics were the number of A grades in the SPM result, duration of medical service, duration of anesthesia service, number of attempts for the entrance examination, and age on first attempts (Table 3).
Significant factors in in–training characteristics were the hospital placement, study facilities, teaching program, helpful academic supervisors, helpful other lecturers/specialists, adequate time to study, time spent studying per day, small-group discussions, and small-group discussions during study leave (Table 4).
.
.
On the basis of the MLR test, only the duration of medical service, number of attempts for the entrance examination, and small-group discussions during study leave were significantly associated with passing at the first attempt in the Part–1 examination (Table 5).
The group with a duration of medical service longer than 5 y had 85% lower odds of passing at the first attempt of the Part–1 examination than the group with less than 5 y of service (adjusted OR 0.15; 95% CI 0.03–0.81; p = 0.027). Those who passed the entrance examination after more than 1 attempt had 80% lower odds of passing at the first attempt of the Part–1 examination than those who passed the entrance examination at the first attempt (adjusted OR 0.20; 95% CI 0.06–0.70; p = 0.011), and the candidates with regular small-group discussions during their study leave had 16.21 times higher odds of passing at the first attempt of the Part–1 examination than those who seldom (adjusted OR 16.21; 95% CI 1.81–145.41; p = 0.013).
Discussion
This study showed that the main factors that determined the higher chance of passing the examination at the first attempt were the duration of medical service for at least 5 years, single attempt at the entrance examination, and regular small-group discussions during study leave.
The minimal criteria for joining the MMed-Anesthesiology program include the completion of 3 years of compulsory medical service, a year of experience in anesthesia service, and passing the entrance examination. Normally, those with longer durations of medical service fail to get through the entrance examination. Our result showed that those with a long duration of medical service (>5 years) had lower odds by 85% to pass the Part–1 examination at the first attempt. Candidates with a strong academic background should be able to clear the entrance examination at the first attempt as well as the subsequent Part–1 examination despite a short duration in medical service before joining the program. According to the descriptive data of this study, 88.5% of the candidates who passed the Part–1 examination at the first attempt had at least 5 years of medical service. When they are in the service for long, they might become complacent in performing routine tasks, lack of motivation to attend specialty training and increased family commitment. A study by Dieste et al to determine the influence of years of experience on the performance of professionals in the software
.
industry showed that the experience gained in the industry does not appear to have any effect on quality and productivity and is a poor predictor of performance.3 Other than the minimal duration of 3 years in medical service, passing the entrance examination is another important prerequisite for entering the MMed-Anesthesiology program. This study showed that the candidates with at least 2 attempts at the entrance examination had 80% lower odds of passing the Part–1 examination at the first attempt than those with a straight pass of the entrance examination. Establishing the link between the
.
entrance examination and the Part–1 examination, it can be seen that those who struggle to pass the entrance examination had difficulties in their first attempt at the Part–1 examination. The gap between passing the entrance examination and the first attempt at the Part–1 examination is approximately 18 mos. According to descriptive data, 73.1% of the candidates in the group that passed the Part–1 examination at the first attempt were found to clear the entrance examination in a single attempt, whereas only 37.0% in the group that passed the Part–1 examination in 2 or more attempts were taking a single attempt at the entrance examination.. This finding indirectly indicate that the entrance examination is an effective way to identify excellent and average candidates for the MMed-Anesthesiology program. There were some studies looking at the relationship of selection criteria with resident performance. A study by Burkhardt et al showed that academic performance in medical schools was not associated with clinical performance in emergency medicine residency.4 Egol et al stated that high scores on the United States Medical Licensing Examination (USMLE) Step 1 have been shown to correlate with high orthopedic in-training examination scores and an improved surgical skill rating during residency.5 Raman et al found that the USMLE Step 2 scores, number of honors in medical school clerkships, and membership of Alpha Omega Alpha Honor Medical Society demonstrated the strongest correlations with resident performance in orthopedic.6
Another significant odd was that the candidates with regular small-group discussions during their study leave had 16.21 times higher odds of passing the Part–1 examination. In our system, the duration of study leave was about 10–14 days minimum, and a final revision in the form of a group discussion with friends within that time was helpful for their performance. On the basis of this result, it can be said that it is important for all training centers to provide adequate study leave and this will allow more time for candidates to do revision in groups. Lake also showed that students who actively participate in small-group discussions perform better in MCQ-format examinations compared to those who attend lecture courses. Besides being actively involved in small-group discussions, the schedule of discussion must be systematic.7 Rytkönen et al stated that both the success and the academic progression of students correlated most strongly with organized learning.8 A study by Rahman et al concluded that the discussion method is more effective than the lecture method in teaching social studies.9
There are only a few studies discussing the factors affecting academic performance in anesthesiology training. Bowhay and Watmough selected 3303 graduates from 19 medical schools in the United Kingdom and compared their performance in the MCQ section of the first part of the FRCA examination. The results showed that males performed remarkably better than females in all subjects, even though females outnumbered males in taking the MCQs.1 On the basis of the SLR test, the current study also showed that male candidates had a 2.91 times higher chance of passing the Part–1 examination at the first attempt than female candidates. Watmough and Bowhay compared the performance of graduates by country of primary medical qualification in Part–1 of the UK Royal College of Anesthetists examination. The candidates from Australia, New Zealand, South Africa, Zimbabwe, and the United Kingdom performed significantly better than the mean for the group and those from Egypt, Iraq, Ireland, and Pakistan.10
The limitation of this study was that the sample consisted of students from a single center. The results concerning the factors affecting performance for the Part–1 examination might have been clearer with a bigger sample involving all candidates from the 5 universities involved in the examination. This study can be a first step toward further extensive assessment of the program in the future.
Conclusions
The main factors affecting academic performance in the first attempt at the Part–1 MMed-Anesthesiology examination were the duration of medical service 5 years or shorter, single attempt at the entrance examination, and regular small-group discussions during study leave.
Conflict of Interest
Authors declare no conflict of interest.
Authors’ Contribution
ATMY, WMNWH: Conception, design, execution, analysis, interpretation of the data, drafting and final approval of manuscript
WMNWH: Critical revision
MHH, MSBY: Conception, design, interpretation of the data, critical revision and final approval of manuscript
WFWMS: Conception, design, critical revision and final approval of manuscript
NMY: Conception, design, interpretation of the data and final approval of manuscript
References
Authors affiliations:
- Department of Anesthesiology & Intensive Care, School of Medical Sciences Hospital, Health Campus, Universiti Sains Malaysia USM, 16150 Kubang Kerian, Kelantan, Malaysia.
- Department of Medical Education, School of Medical Sciences, Health Campus, USM, 16150 Kubang Kerian, Kelantan, Malaysia.
- Department of Biostatistics & Research Methodology, School of Medical Sciences, Health Campus, USM, 16150 Kubang Kerian, Kelantan, Malaysia.
Abstract
Background: It has been observed that some candidates do very well in postgraduate examinations and get through in the very first attempt, whereas the others may not do very well and have to go for multiple attempts to get through the same examination. This study aimed to determine the factors affecting the performance and the success rate in the first attempt in the Master of Medicine (Anesthesiology) Part–1 examination.
Methodology: This was a cross-sectional study involving 73 postgraduate candidates who passed the Master of Medicine (Anesthesiology) Part–1 examination between 2016 and 2017. The candidates were required to respond to various questions about various factors assumed to be affecting their performance, including sociodemographic factors, pre–training, and in–training factors. Statistical analysis of the received responses was done and linked to the performance in the Part-1 examination.
Results: The candidates with more than 5 y of medical service had 85% lower odds than those with 5 or fewer years (adjusted OR 0.15; 95% CI 0.03–0.81; p = 0.027). Those who passed the entrance examination after 2 or more attempts also had 80% lower odds than those who passed at the first attempt (adjusted OR 0.20; 95% CI 0.06–0.70; p = 0.011). The odds of the candidates who often had small-group discussions during their study leave were 16.21 times higher to pass than those who seldom had any discussion (adjusted OR 16.21; 95% CI 1.81–145.41; p = 0.013).
Conclusions: The success in the Master of Medicine (Anesthesiology) Part–1 examination in first attempt was determined by a shorter duration of medical service, single attempt at the entrance examination, and regular small-group discussions.
Key words: Anesthesiology; Postgraduate; Medicine; Examination; Candidate
Abbreviations: UKM – Universiti Kebangsaan Malaysia; USM – Universiti Sains Malaysia; OSCE – Objective Structured Clinical Examination; SPM – Sijil Pelajaran Malaysia
Citation: Yusoff ATM, Hassan WMNW, Hassan MH, Yusoff MSB, Shukeri WFWM, Yaacob NM. A study of the factors affecting the academic performance of postgraduate examinees in the Master of Medicine (Anesthesiology) Part-1 examination. Anaesth. pain intensive care 2021;25(4):478–486.
DOI: 10.35975/apic.v25i4.1568
Received: April 16, 2021, Reviewed: May 30, 2021, Accepted: 2 June 2021
Introduction
The Master of Medicine in Anesthesiology (MMed-Anesthesiology) is a postgraduate clinical program in Malaysia that was established in 1988, with the main objective of producing more anesthesiologists in Malaysia using a structured training program. In the beginning, there were two different systems running independently according to the curriculum decided by each university. The curriculum that was initiated jointly by the University of Malaya (UM) and Universiti Kebangsaan Malaysia (UKM) in 1988 mostly resembled the format of the Australia–New Zealand examination, whereas the curriculum by Universiti Sains Malaysia (USM) in 1993 was similar to the format of the UK examination.
The format of the MMed-Anesthesiology UM–UKM examination consisted of an aptitude test at 6th month of enrollment, followed by the Part–1 examination at 18 months and the Part–2 examination at the end of the 4th year. The Part–1 examination comprised of a written part and viva voce in 2 main subjects – physiology/clinical measurement and pharmacology, which were assessed separately.
On the contrary, the format of the MMed-Anesthesiology USM examination was slightly different. The Part-1 examination was taken at the end of year 1, and the Part-2 examination was at the end of the year 4 without any aptitude test. The format of the examination consisted of theory and clinical examination in the form of short cases and viva voce, as well as the Objective Structured Clinical Examination (OSCE). All subjects were combined in one theory paper, and there was no separation between physiology and pharmacology.
The move to standardize the MMed-Anesthesiology program in Malaysia was initiated by the formation of the Conjoint Board Committee consisting of the 3 main universities, UM–UKM–USM, in order to standardize the quality of training and skills of anesthesiologists in Malaysia. After a few years, 2 other main universities—Universiti Putra Malaysia and International Islamic University of Malaysia—also joined the committee. The decision to standardize training and examination focused more on mutual understanding and a paradigm shift in clinical specialty training at that time toward the conjoint program of the main universities in Malaysia. There is no previous study comparing the effectiveness of 2 different systems of anesthesiology training in Malaysia. According to a study by Bowhay and Watmough on the first part of the Fellowship of the Royal College of Anaesthetists (FRCA) examination, notable change in the curriculum did not lead to performance deterioration in postgraduate examination in medical schools in the United Kingdom.1 The first Conjoint Examination for Part-2 was started in 2008, and the Part-1 was started in 2014. The format of the Part-1 examination adopted more of the old format of the MMed-Anesthesiology UM–UKM examination with the omission of the aptitude test, and the examination was conducted at the end of the year 1. There are 2 main subjects in the Part-1 Examination, which are pharmacology and physiology/clinical measurement. Each subject consists of theory and viva. Theory consists of 80 multiple-choice questions (MCQs) and 6 short-answer questions (SEQs), and the candidates must pass the theory examination to be able to proceed to the viva for each subject. The candidates are considered to have passed the Part-1 examination if they clear all sections for both subjects. Those who fail the examination repeat only the failed subject, and 3 consecutive repeat examinations are allowed for each candidate, with 1 extra appeal if still unable to pass after 3 repeat examinations.
The Part-1 Conjoint Examination is considered tough, and the passing rate has been around 30%–50% since the first examination. As stated by Bowhay and Watmough in their study, passing the primary FRCA examination at the first attempt for graduates of each medical school is very difficult, and the average pass percentage was 56.1%.1 There are many potential factors that might be affecting the performance of postgraduate candidates. Lane et al. stated that individual proficiency mediated the relationship between performance accomplishments and academic performance of postgraduate students.2
This study determined the factors affecting the pass percentage at the first attempt of the Part–1 MMed-Anesthesiology examination, including sociodemographic, pre–training, and in–training aspects.
.
Methodology
This is a cross-sectional study conducted after obtaining approval from the Institutional Ethics Committee (USM/JEPeM approval code: 17090413) and written consent from the candidates. The inclusion criteria were postgraduate students in USM who passed their Part–1 Conjoint Examination for MMed-Anesthesiology between 2016 and 2017, and the exclusion criteria involved those who passed the Part-1 examination using the old format of examination.
A total of 73 eligible candidates were included in this study, and the group that passed the Part–1 examination at the first attempt and the group that required multiple attempts to pass were compared. All the candidates were required to respond to questionnaires online, with a timeline of one week. The questionnaires were self-administered, and the duration to answer these questionnaires was about 20 min. They contained 35 items and were divided into 6 parts:
Part–1: The demographic data and socioeconomic background of the candidates
Part 2: The academic background before joining the program, including the Malaysian Certificate of Education for secondary school or well known as the “Sijil Pelajaran Malaysia” (SPM) result
Part 3: The background of medical service before joining MMed-Anesthesiology training
Part 4: The background of MMed-Anesthesiology training
Part 5: The assessment of facilities for study and clinical training, availability of teaching program, involvement of academic supervisor, involvement of other specialists, adequacy of time to study, and
| Table 1 (C): In-training characteristics of the participants | |||
| Parameter | In-training characteristics | Pass after ≥ 2nd attempt (n = 47) | Pass at 1st attempt
(n = 26) |
| Campus placement | Out-campus In-campus |
33.0 (70.2) 14.0 (29.8) |
17.0 (65.4) 9.0 (34.6) |
| Hospital placement
|
Peninsular Malaysia Sabah-Sarawak |
42.0 (91.3) 4.0 (8.7) |
19.0 (73.1) 7.0 (26.9) |
| Facilities for study
|
Very poor – fair Good - excellent |
31.0 (66.0) 16.0 (34.0) |
13.0 (50.0) 13.0 (50.0) |
| Facilities for clinical training | Very poor – fair Good - excellent |
16.0 (34.0) 31.0 (66.0) |
6.0 (23.1) 20.0 (76.9) |
| Availability of teaching programme | Very poor – fair Good - excellent |
24.0 (52.2) 22.0 (47.8) |
9.0 (34.6) 17.0 (65.4) |
| Academic supervisor was helpful | Very poor – fair Good - excellent |
27.0 (57.4) 20.0 (42.6) |
10.0 (38.5) 16.0 (61.5) |
| Other lecturers/ specialists were helpful | Very poor – fair Good - excellent |
24.0 (51.1) 23.0 (48.9) |
8.0 (30.8) 18.0 (69.2) |
| Time to study was adequate | Very poor – fair Good - excellent |
33.0 (70.2) 14.0 (29.8) |
14.0 (53.8) 12.0 (46.2) |
| Time spending to study per day | Very poor – fair Good - excellent |
39.0 (83.0) 8.0 (17.0) |
18.0 (69.2) 8.0 (30.8) |
| Had a small discussion group | Seldom (Never-once per mo) Often (Few times/mo - every day) |
13.0 (27.7) 34.0 (72.3) |
4.0 (16.0) 21.0 (84.0) |
| Attended scheduled tutorials/ classes | Seldom (Never – once per mo) Often (Few times/ mo - every day) |
6.0 (12.8) 41.0 (87.2) |
5.0 (20.0) 20.0 (80.0) |
| Impromptu discussion with seniors /specialists | Seldom (Never – once per mo) Often (Few times/ mo - every day) |
14.0 (29.8) 33.0 (70.2) |
5.0 (20.0) 20.0 (80.0) |
| Practised past years questions | Seldom (Never – once per mo) Often (Few times/ mo - every day) |
8.0 (17.0) 39.0 (83.0) |
5.0 (20.0) 20.0 (80.0) |
| Extra classes with lecturers | Seldom (Never – once per mo) Often (Few times/ mo - every day) |
18.0 (38.3) 29.0 (61.7) |
10.0 (40.0) 15.0 (60.0) |
| Small group discussion during study leave | Seldom (Never – once per mo) Often (Few times/ mo - every day) |
15.0 (31.9) 32.0 (68.1.) |
1.0 (4.0) 24.0 (96.0) |
| Average working hours per week | ≤ 72 h/week > 72 h/week |
35.0 (76.1) 11.0 (23.9) |
21.0 (80.8) 5.0 (19.2) |
| Average on call per mo | < 4 per mo 4 – 8 per mo |
7.0 (14.9) 40.0 (85.1) |
0.0 (0.0) 26.0 (100.0) |
| Went home late due to work | Seldom (Never – once per mo) Often (Few times / mo - Every day) |
6.0 (12.8) 41.0 (87.2) |
5.0 (20.0) 20.0 (80.0) |
| Felt happy working with current colleagues | Seldom (Never – once per mo) Often (Few times / mo - Every day) |
3.0 (6.4) 44.0 (93.6) |
0.0 (0.0) 25.0 (100.0) |
| Felt energetic during working | Seldom (Never – once per mo) Often (Few times / mo - Every day) |
5.0 (10.6) 42.0 (89.4) |
1.0 (4.0) 24.0 (96.0) |
| Able to meet family/wife/husband | Seldom (Never – once per mo) Often (Few times / mo - Every day) |
7.0 (14.9) 39.0 (83.0) |
5.0 (20.0) 20.0 (80.0) |
| All categorical data are expressed in n (%) and numerical data in mean (SD) | |||
allocation of time to study per day. These factors were initially assessed in 5 grades: (i) very poor, (ii) poor, (iii) fair, (iv) good, and (v) excellent. These were further narrowed down to 2 groups: (i) very poor to fair and (ii) good to excellent
Part 6: The assessment of the availability of small discussion groups, regularity in attending scheduled classes, regularity of impromptu discussions with seniors, regularity of practicing past-year questions, availability of extra classes, availability of small-group discussions during study leave, frequency of going home late from work, level of happiness while working with colleagues, level of energy during working, and availability of time to meet family members. These factors were assessed in 7 categories: (i) never, (ii) a few times per year or less, (iii) once a month or less, (iv) a few times per month, (v) once a week, (vi) a few times per week, and (vii) every day. These were further narrowed down to 2 groups: (i) seldom (never to once a month) and (ii) often (a few times per month to every day).
Data were analyzed using SPSS Statistics (v.25; IBM Corp. Armonk, NY, USA). All the factors were initially analyzed using the simple logistic regression (SLR) test, and the factors that had a p < 0.25 were included in the multiple logistic regression (MLR) test. A p < 0.05 was considered statistically significant.
Results
The eligible candidates were 73 and the survey response rate was 100%. The descriptive statistics of sociodemographic, pre–training, and in–training factors are presented in Tables 1 (A, B and C).
On the basis of the SLR test, there were few factors that had a p < 0.25 that was significant to proceed for the MLR test. Significant factors in sociodemographic characteristics were gender, race, and spouse’s profession (Table 2).
Significant factors in pre–training characteristics were the number of A grades in the SPM result, duration of medical service, duration of anesthesia service, number of attempts for the entrance examination, and age on first attempts (Table 3).
Significant factors in in–training characteristics were the hospital placement, study facilities, teaching program, helpful academic supervisors, helpful other lecturers/specialists, adequate time to study, time spent studying per day, small-group discussions, and small-group discussions during study leave (Table 4).
| Table 2: Simple logistic regression analysis to determine sociodemographic factors associated with academic performance (pass at 1 attempt) | |||||
| Variables | Crude b | Crude OR (95% CI) | Wald | p-value | |
| Age group (years) | £ 30 > 30 |
0 -0.47 |
1 0.96 (0.34, 2.70) |
0.01 |
0.930 |
| Gender
|
Female Male |
0 1.07 |
1 2.91 (1.08, 7.83) |
4.46 |
*0.035 |
| Race
|
Malay Non-Malay |
0 0.76 |
1 0.21 (0.80, 5.70) |
2.28 |
*0.131 |
| Marital status
|
Single Married |
0 0.15 |
1 1.16 (0.42, 3.25) |
0.08 |
0.776 |
| Number of Children | -0.09 | 0.92 (0.58, 1.45) | 0.13 | 0.716 | |
| Spouse job
|
Non-HCP HCP No spouse |
0 -1.743 -0.96 |
1 0.18 (0.04, 0.77) 0.38 (0.12, 1.21) |
5. 69 2. 69 |
*0.017 0.101 |
| Loan
|
Yes No |
0 0.61 |
1 0.54 (0.03, 9.07) |
0.18 |
0.671 |
| Family income (Rs. Per mo) | 5000 – 10000 >10000 |
0 -0.191 |
1 1.21 (0.45, 3.27) |
0.14 |
0.706 |
| *p < 0.25; HCP – Healthcare Professional | |||||
| Table 3: Simple logistic regression analysis to determine pre-training factors associated with academic performance (pass at 1 attempt) | |||||
| Variables | Crude b | Crude OR (95% CI) | Wald | p-value | |
| Types of secondary school | Daily school Boarding school |
0 -0.44 |
1 0.65 (0.25, 1.70) |
0.79 |
0.374 |
| Number of A grades in SPM | |
0.19 | 1.21 (0.94, 1.55) | 2.14 | *0.143 |
| Type of university during undergraduate | Local Overseas |
0 -0.32 |
1 1.38 (0.52, 3.64) |
0.43 |
0.51 |
| Duration of undergraduate | 5 y > 5 y |
0 -0.25 |
1 0.78 (0.24, 2.55) |
0.17 |
0.680 |
| Duration of medical services | 5 y > 5 y |
0 -1.65 |
1 0.19 (0.05, 0.73) |
5.85 |
*0.016 |
| Duration of anesthesia services | ≤ 3 y > 3 y |
0 -1.35 |
1 0.26 (0.08, 0.87) |
4.76 |
*0.029 |
| Number of attempts for entry exam | 1 Attempt 2 1 attempt |
0 -1.53 |
1 0.22 (0.08, 0.62) |
8.13 |
*0.004 |
| Age on first attempt | -0.321 | 0.73 (0.49, 1.08) | 4.35 | *0.116 | |
| *p < 0.25 | |||||
On the basis of the MLR test, only the duration of medical service, number of attempts for the entrance examination, and small-group discussions during study leave were significantly associated with passing at the first attempt in the Part–1 examination (Table 5).
The group with a duration of medical service longer than 5 y had 85% lower odds of passing at the first attempt of the Part–1 examination than the group with less than 5 y of service (adjusted OR 0.15; 95% CI 0.03–0.81; p = 0.027). Those who passed the entrance examination after more than 1 attempt had 80% lower odds of passing at the first attempt of the Part–1 examination than those who passed the entrance examination at the first attempt (adjusted OR 0.20; 95% CI 0.06–0.70; p = 0.011), and the candidates with regular small-group discussions during their study leave had 16.21 times higher odds of passing at the first attempt of the Part–1 examination than those who seldom (adjusted OR 16.21; 95% CI 1.81–145.41; p = 0.013).
Discussion
This study showed that the main factors that determined the higher chance of passing the examination at the first attempt were the duration of medical service for at least 5 years, single attempt at the entrance examination, and regular small-group discussions during study leave.
The minimal criteria for joining the MMed-Anesthesiology program include the completion of 3 years of compulsory medical service, a year of experience in anesthesia service, and passing the entrance examination. Normally, those with longer durations of medical service fail to get through the entrance examination. Our result showed that those with a long duration of medical service (>5 years) had lower odds by 85% to pass the Part–1 examination at the first attempt. Candidates with a strong academic background should be able to clear the entrance examination at the first attempt as well as the subsequent Part–1 examination despite a short duration in medical service before joining the program. According to the descriptive data of this study, 88.5% of the candidates who passed the Part–1 examination at the first attempt had at least 5 years of medical service. When they are in the service for long, they might become complacent in performing routine tasks, lack of motivation to attend specialty training and increased family commitment. A study by Dieste et al to determine the influence of years of experience on the performance of professionals in the software
| Table 4: Simple logistic regression analysis to determine training factors associated with academic performance (pass at 1 attempt) | |||||
| Variables | Crude b | Crude OR (95% CI) | Wald | p-value | |
| Candidate placement
|
In-campus Out-campus |
0 -0.22 |
1 0.80 (0.29, 2.23) |
0.18 |
0.671 |
| Hospital placement Part–1 | Peninsular Malaysia Sabah-Sarawak |
0 1.35 |
1 3.87 (1.01, 14.81) |
3.90 |
*0.048 |
| Facilities for study
|
Very poor – fair Good - excellent |
0 0.66 |
1 1.94 (0.73, 5.15) |
1.76 |
*0.185 |
| Facilities for clinical training | Very poor – fair Good – excellent |
0 0.54 |
1 1.72 (0.58, 5.14) |
0.95 |
0.331 |
| Availability of teaching programme | Very poor – fair Good - excellent |
0 0.81 |
1 2.25 (0.83, 6.08) |
2.55 |
*0.110 |
| Academic supervisor was helpful | Very poor – fair Good - excellent |
0 0.77 |
1 2.16 (0.81,5.75) |
2.38 |
*0.123 |
| Other lecturers/ specialists were helpful | Very poor – fair Good - excellent |
0 0.85 |
1 2.35 (0.86, 6.45) |
2.74 |
*0.098 |
| Adequate time to study | Very poor – fair Good - excellent |
0 0.70 |
1 2.02 (0.75, 5.45) |
1.93 |
*0.165 |
| Time spent on studies per day | Very poor – fair Good - excellent |
0 0.77 |
1 2.17 (0.70, 6.69) |
1.81 |
*0.179 |
| Small group discussions | Seldom (Never-once per mo) Often (Few times/mo - every day) |
0 0.80 |
1 2.23 (0.65, 7.67) |
1.61 |
*0.205 |
| Attended scheduled tutorial | Seldom (Never-once per mo) Often (Few times/mo - every day) |
0 -0.54 |
1 0.59 (1.16, 2.15) |
0.65 |
0.420 |
| Impromptu discussion with seniors / specialists | Seldom (Never-once per mo) Often (Few times/mo - every day) |
0 0.53 |
1 1.70 (0.53, 5.43) |
0.80 |
0.373 |
| Practice past year questions | Seldom (Never-once per mo) Often (Few times/mo - every day) |
0 -0.36 |
1 0.70 (0.20, 2.49) |
0.30 |
0.581 |
| Extra class with lecturers | Seldom (Never- once per mo) Often (Few times/mo - every day) |
0 -0.07 |
1 0.93 (0.35, 2.51) |
0.02 |
0.888 |
| Small group discussions during leave | Seldom (Never- once per mo) Often (Few times/mo - every day) |
0 2.42 |
1 11.25 (1.39, 91.17) |
5.14 |
*0.023 |
| Average working hours per week | ≤ 72 h/week > 72 h/week |
0 -0.28 |
1 0.76 (0.23, 2.48) |
0.21 |
0.647 |
| Went home late due to work | Seldom (Never- once per mo) Often (Few times/mo - every day) |
0 -0.54 |
1 0.59 (1.16, 2.15) |
0.65 |
0.420 |
| Able to meet family/wife/husband | Seldom (Never- once per mo) Often (Few times/mo - every day) |
0 -0.36 |
1 0.70 (0.20, 2.49) |
0.30 |
0.581 |
| *p < 0.25 | |||||
industry showed that the experience gained in the industry does not appear to have any effect on quality and productivity and is a poor predictor of performance.3 Other than the minimal duration of 3 years in medical service, passing the entrance examination is another important prerequisite for entering the MMed-Anesthesiology program. This study showed that the candidates with at least 2 attempts at the entrance examination had 80% lower odds of passing the Part–1 examination at the first attempt than those with a straight pass of the entrance examination. Establishing the link between the
| Table 5: Multiple logistic regression analysis to determine factors associated with academic performance (pass at 1 attempt) | |||||
| Variables | Adj. b | Adj. OR (95% CI) | Wald | p-value
|
|
| Duration of medical service | £ 5 years > 5 years |
0 -1.88 |
1 0.15 (0.03, 0.81) |
4.86 |
0.027 |
| Number of attempts for entry exam | 1 attempt > 1 attempt |
0 -1.60 |
1 0.20 (0.06, 0.70) |
6.42 |
0.011 |
| Small group discussion during study leave | Seldom (Never-once per mo) Often (Few times / mo - every day) |
0 2.79 |
1 16.21 (1.81, 145.41) |
6.19 |
0.013 |
| Forward LR method applied. Classification table=78.9% overall percentage correct, Hosmer-Lemeshow test p-value=0.997, Area under ROC curve=83.4%. No influential outlier, no multicollinearity, and no interaction. | |||||
entrance examination and the Part–1 examination, it can be seen that those who struggle to pass the entrance examination had difficulties in their first attempt at the Part–1 examination. The gap between passing the entrance examination and the first attempt at the Part–1 examination is approximately 18 mos. According to descriptive data, 73.1% of the candidates in the group that passed the Part–1 examination at the first attempt were found to clear the entrance examination in a single attempt, whereas only 37.0% in the group that passed the Part–1 examination in 2 or more attempts were taking a single attempt at the entrance examination.. This finding indirectly indicate that the entrance examination is an effective way to identify excellent and average candidates for the MMed-Anesthesiology program. There were some studies looking at the relationship of selection criteria with resident performance. A study by Burkhardt et al showed that academic performance in medical schools was not associated with clinical performance in emergency medicine residency.4 Egol et al stated that high scores on the United States Medical Licensing Examination (USMLE) Step 1 have been shown to correlate with high orthopedic in-training examination scores and an improved surgical skill rating during residency.5 Raman et al found that the USMLE Step 2 scores, number of honors in medical school clerkships, and membership of Alpha Omega Alpha Honor Medical Society demonstrated the strongest correlations with resident performance in orthopedic.6
Another significant odd was that the candidates with regular small-group discussions during their study leave had 16.21 times higher odds of passing the Part–1 examination. In our system, the duration of study leave was about 10–14 days minimum, and a final revision in the form of a group discussion with friends within that time was helpful for their performance. On the basis of this result, it can be said that it is important for all training centers to provide adequate study leave and this will allow more time for candidates to do revision in groups. Lake also showed that students who actively participate in small-group discussions perform better in MCQ-format examinations compared to those who attend lecture courses. Besides being actively involved in small-group discussions, the schedule of discussion must be systematic.7 Rytkönen et al stated that both the success and the academic progression of students correlated most strongly with organized learning.8 A study by Rahman et al concluded that the discussion method is more effective than the lecture method in teaching social studies.9
There are only a few studies discussing the factors affecting academic performance in anesthesiology training. Bowhay and Watmough selected 3303 graduates from 19 medical schools in the United Kingdom and compared their performance in the MCQ section of the first part of the FRCA examination. The results showed that males performed remarkably better than females in all subjects, even though females outnumbered males in taking the MCQs.1 On the basis of the SLR test, the current study also showed that male candidates had a 2.91 times higher chance of passing the Part–1 examination at the first attempt than female candidates. Watmough and Bowhay compared the performance of graduates by country of primary medical qualification in Part–1 of the UK Royal College of Anesthetists examination. The candidates from Australia, New Zealand, South Africa, Zimbabwe, and the United Kingdom performed significantly better than the mean for the group and those from Egypt, Iraq, Ireland, and Pakistan.10
The limitation of this study was that the sample consisted of students from a single center. The results concerning the factors affecting performance for the Part–1 examination might have been clearer with a bigger sample involving all candidates from the 5 universities involved in the examination. This study can be a first step toward further extensive assessment of the program in the future.
Conclusions
The main factors affecting academic performance in the first attempt at the Part–1 MMed-Anesthesiology examination were the duration of medical service 5 years or shorter, single attempt at the entrance examination, and regular small-group discussions during study leave.
Conflict of Interest
Authors declare no conflict of interest.
Authors’ Contribution
ATMY, WMNWH: Conception, design, execution, analysis, interpretation of the data, drafting and final approval of manuscript
WMNWH: Critical revision
MHH, MSBY: Conception, design, interpretation of the data, critical revision and final approval of manuscript
WFWMS: Conception, design, critical revision and final approval of manuscript
NMY: Conception, design, interpretation of the data and final approval of manuscript
References
- Bowhay AR, Watmough SD. An evaluation of the performance in the UK Royal College of Anaesthetists primary examination by UK medical school and gender. BMC Med Educ. 2009;2(7):84–94. [PubMed] DOI: 1186/1472-6920-9-38
- Lane J, Lane AM, Kyprianou A. Self-efficacy, self-esteem and their impact on academic performance. Soc Behav Pers. 2004;32(3):247–256. DOI: 2224/sbp.2004.32.3.247
- Dieste O, Aranda AM, Uyaguari F, Turhan B, Tosun A, Fucci D, et al. Empirical evaluation of the effects of experience on code quality and programmer productivity: an exploratory study. Empir Softw Eng. 2017;22(5):2457–2542. DOI: 1007/s10664-016-9471-3 [FreeFullText]
- Burkhardt JC, Parekh KP, Gallahue FE, London KS, Edens MA, Humbert AJ, et al. A critical disconnect residency selection factors lack correlation with intern performance. J Grad Med Educ. 2020;12(6):696–704. [PubMed] DOI: 4300/JGME-D-20-00013.1
- Egol KA, Collins J, Zuckerman JD. Success in orthopaedic training: resident selection and predictors of quality performance. J Am Acad Orthop Surg. 2011;19(2):72–80. [PubMed] DOI: 5435/00124635-201102000-00002
- Raman T, Alrabaa RG, Sood A, Maloof P, Benevenia J, Berberian W. Does residency selection criteria predict performance in orthopaedic surgery residency? Clin Orthop Relat Res. 2016; 474:908–914. [PubMed] DOI: 1007/s11999-015-4317-7
- Lake DA. Student performance and perceptions of a lecture-based course compared with the same course utilizing group discussion. Phys Ther. 2001;81(3):896–902. [PubMed] DOI:1093/ptj/81.3.896
- Rytkönen H, Parpala A, Lindblom-Ylänne S, Virtanen V, Postareff L. Factors affecting bioscience students’ academic achievement. Instr Sci. 2012;40(2):241–256.
- Rahman F, Khalil JK, Jumani NB, Ajmal M, Malik S, Sharif M, et al. Impact of discussion method on students' performance. Int J Bus Soc Sci. 2011;2(7):84–94. [FreeFullText]
- Watmough S, Bowhay A. An evaluation of the impact of country of primary medical qualification on performance in the UK Royal College of Anaesthetists’ examinations. Med Teach. 2011;33(11):938–940. [PubMed] DOI: 3109/0142159X.2011.588736