Mehreen Malik1, Sana Urooj 2 , Aftab Imtiaz 3 , Arif Muhammad Arif 4
Authors’ affiliations:
Abstract
Anesthesia Preoperative evaluation holds a prime importance in improving overall patient outcomes and decreases hospital expenditure. The American Society of Anesthesiologists Physical Status scoring system ASA-PS was introduced 70 years back in clinical practice and it still holds the lime light for stratifying patient population and considering the risk index and mortality outcomes to warn the surgeon. How has it evolved since the passing years? We will see how over centuries it has evolved. ASA PS has been a significant predictor in depicting morbidity and mortality and evaluating peri-operative risks in patients going for surgery for clinicians, researchers, hospital administrators and government. Further addition of examples of modifying ASA PS status is necessary to make it more comprehensive and easier to use even for non-anesthetists to improve overall peri-operative morbidity and mortality.
Key words: ASA PS (American Society of Anesthesiology Physical Status); Peri-operative outcomes
Citation: Malik M, Urooj S, Imtiaz A, Arif AM. Evolution of ASA Physical status scoring system. Anaesth. pain intensive care 2021;25(2):225-232.
DOI: 10.35975/apic.v25i2.1476
Received: , Reviewed: , Accepted:
Introduction
Anesthesia Preoperative evaluation holds a prime importance in improving overall patient outcomes and decreases hospital expenditure. American Society of Anesthesiologists Physical Status scoring system ASA-PS was introduced 70 years back in clinical practice and it still holds the lime light for stratifying patient population and considering the Risk Index and mortality outcomes to warn the surgeon. ASA PS has been a significant predictor in depicting morbidity and mortality and evaluating peri-operative risks in patients going for surgery for clinicians, researchers, hospital administrators and government.
Evolution in the early era
The development of ASA classification has evolved over a period. In 1941 ASA published a brochure for patients undergoing surgery for the first time. In May 1941, Meyer Saklad described the six new degree ASA PS grading as a physical state of a patient to determine operative risk1. He listed the planned surgical procedure, the surgeon’s ability and skill in performing a certain procedure, postoperative care of the patient and anesthetist expertize in similar cases. Saklad gave many examples of systemic illnesses to standardize the classification. However, there was no mention of the optimization of the poor physical status of the patient.
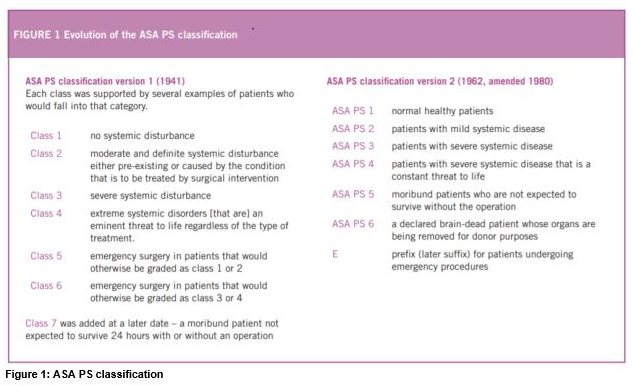
Figure 1 shows old versions of ASA Classification. Dr. Dripps et al. developed it into its current form in 1961,2 and it was adapted by ASA in 1962.3
Now it showed addition of ‘E’ with no examples.
Early drawbacks
This classification has been criticized to have inter-observer variability as it was left on the anesthetist’s judgment to put the patient in a certain grade.
Evolution in the recent past
In 1980, ASA PS added the already brain-dead patient going for surgery for organ harvesting as technology evolved and organ transplantation became common. ASA update the table giving examples on December 13, 202012 making it more comprehensive for our understanding.4-9 It was proved in these studies that by adding examples to the ASA classification even non-anesthesia personnel could place patients correctly into groups. These examples give guidelines to clinicians and may vary according to Anesthesia departments of various institutions.
Benefits of ASA classification
The ASA Classification has two benefits:
.
There are certain physical limitations that can change outcomes like those who have certain genetic predilections like malignant hyperthermia or suxamethonium apnea history, a difficult airway history or is a Jehovah’s witness.
Responsibility of the anesthetist
Even though the ASA status can be awarded while Pre-operative assignment is in process, it must be reconfirmed by the primary Anesthetist. It will be considered a deceased donor and anesthetic principals may be wary.
Issues regarding the subjectivity of ASA physical status have been silenced as its validity and authenticity has been explained in several papers.
Evolution of ASA in the future
Further addition of examples of modifying ASA PS status may still be necessary to make it more comprehensive and easier to use even for non-anesthetists to improve overall peri-operative morbidity and mortality.
Conclusion
Anesthesia preoperative evaluation holds prime importance in assessment of patient and has been a significant predictor of perioperative morbidity and mortality. It has evolved over 70 years and is still evolving to better standards. Additions of further examples are still necessary to make it useful even for non-anesthesia personnel.
In contrast, the evaluation of functional capacity that established a benchmark of the original 1941 classification was yet missing from the existing schemata and its revitalization may additionally mitigate its differences.
Authors’ contribution
All authors took equal part in the preparation of this manuscript.
References
Authors’ affiliations:
- Consultant Anesthesiologist, South City Hospital, Karachi, Pakistan.
- Assistant Professor, Department of Anesthesiology, Civil Hospital Karachi, Pakistan.
- Professor & Head, Department of Anesthesiology, Abbasi Shaheed Hospital/Karachi Medical & Dental College, Karachi, Pakistan.
- Resident Anesthesiology, Abbassi Shaheed Hospital Karachi, Pakistan.
Abstract
Anesthesia Preoperative evaluation holds a prime importance in improving overall patient outcomes and decreases hospital expenditure. The American Society of Anesthesiologists Physical Status scoring system ASA-PS was introduced 70 years back in clinical practice and it still holds the lime light for stratifying patient population and considering the risk index and mortality outcomes to warn the surgeon. How has it evolved since the passing years? We will see how over centuries it has evolved. ASA PS has been a significant predictor in depicting morbidity and mortality and evaluating peri-operative risks in patients going for surgery for clinicians, researchers, hospital administrators and government. Further addition of examples of modifying ASA PS status is necessary to make it more comprehensive and easier to use even for non-anesthetists to improve overall peri-operative morbidity and mortality.
Key words: ASA PS (American Society of Anesthesiology Physical Status); Peri-operative outcomes
Citation: Malik M, Urooj S, Imtiaz A, Arif AM. Evolution of ASA Physical status scoring system. Anaesth. pain intensive care 2021;25(2):225-232.
DOI: 10.35975/apic.v25i2.1476
Received: , Reviewed: , Accepted:
Introduction
Anesthesia Preoperative evaluation holds a prime importance in improving overall patient outcomes and decreases hospital expenditure. American Society of Anesthesiologists Physical Status scoring system ASA-PS was introduced 70 years back in clinical practice and it still holds the lime light for stratifying patient population and considering the Risk Index and mortality outcomes to warn the surgeon. ASA PS has been a significant predictor in depicting morbidity and mortality and evaluating peri-operative risks in patients going for surgery for clinicians, researchers, hospital administrators and government.
Evolution in the early era
The development of ASA classification has evolved over a period. In 1941 ASA published a brochure for patients undergoing surgery for the first time. In May 1941, Meyer Saklad described the six new degree ASA PS grading as a physical state of a patient to determine operative risk1. He listed the planned surgical procedure, the surgeon’s ability and skill in performing a certain procedure, postoperative care of the patient and anesthetist expertize in similar cases. Saklad gave many examples of systemic illnesses to standardize the classification. However, there was no mention of the optimization of the poor physical status of the patient.
Figure 1 shows old versions of ASA Classification. Dr. Dripps et al. developed it into its current form in 1961,2 and it was adapted by ASA in 1962.3
Now it showed addition of ‘E’ with no examples.
Early drawbacks
This classification has been criticized to have inter-observer variability as it was left on the anesthetist’s judgment to put the patient in a certain grade.
Evolution in the recent past
In 1980, ASA PS added the already brain-dead patient going for surgery for organ harvesting as technology evolved and organ transplantation became common. ASA update the table giving examples on December 13, 202012 making it more comprehensive for our understanding.4-9 It was proved in these studies that by adding examples to the ASA classification even non-anesthesia personnel could place patients correctly into groups. These examples give guidelines to clinicians and may vary according to Anesthesia departments of various institutions.
Benefits of ASA classification
The ASA Classification has two benefits:
- It quantifies the physiological reserve of a patient being assessed for surgery, which could be improved or optimized, or the patient may further deteriorate. ASA PS alone was proved to be a strong predictor of of outcomes.10
- Billing the patient is done based on ASA status in hospitals.Current Status
The beauty of ASA PS classification is that it can distinctly identify `AT RISK` patient in one evaluation. It can alert the level of expert anesthetist required for that case and the need of complex equipment and a backup ICU availability. It helps the surgeon to the council family regarding outcome of surgery. It also helps surgeons as a preemptive ASA PS status will help surgeons recognize and optimize the patient for surgery of a relatively unfit for anesthesia patient and prevent spot cancelation. This also helps OR management to decide the sequence of list according to the ASA status of the patient. Also, it helps the most experienced anesthetist for critical patients, which improves peri-operative outcomes.11
There are a few special conditions that do not lie in systemic illness but can exacerbate surgical risk. It can be a drug history, such as steroids or chemotherapy that causes a limitation to their daily life.
| Table 1: Current definitions and ASA approved examples | ||||
| ASA PS | Definition | Adult examples, including, but not limited to: | Pediatric examples, including, but not limited to: | Obstetric examples, including, but not limited to: |
| ASA I | A normal healthy patient | Healthy, non-smoking, minimal or no alcohol. | Healthy (no acute or chronic disease), normal BMI percentile for age | |
| ASA II | A patient with mild systemic disease | Mild disease without substantive functional limitations. Current smoker, social alcohol drinker, Pregnant, Obese(30<BMI<40), well controlled DM/HTN, mild lung disease | Asymptomatic congenital heart disease, well controlled dysrhythmias, asthma without exacerbation, well controlled epilepsy, non-insulin dependent diabetes mellitus, abnormal BMI percentile for age, mild/moderate OSA, cancer in remission, mild autism | Normal Pregnancy*,well controlled gestational HTN, controlled pre-eclampsia without severe features, Gestational DM with diet control |
| ASA III | A patient with severe systemic disease | Substantive functional limitations; One or more moderate to severe diseases. Poorly controlled DM, HTN, COPD, morbid obesity, active hepatitis, alcohol dependence or abuse, implanted pacemaker, moderate reduction of ejection fraction, ESRD undergoing regularly scheduled dialysis, history(>3 months of MI,CVA,TIA, or CAD/stents | Uncorrected stable congenital cardiac abnormality, asthma with exacerbation, poorly controlled epilepsy, insulin dependent diabetes mellitus, morbid obesity, malnutrition, severe OSA, oncologic state, renal failure, muscular dystrophy, cystic fibrosis, history of organ transplantation, brain/spinal cord malformation, symptomatic hydrocephalus, premature infant PCA<60, autism with severe limitations, metabolic disease, difficult airway, long term parenteral nutrition. Full term infants | Preeclampsia with severe features, gestational DM with complications or high insulin requirements, a thrombophilic disease requiring anticoagulation. |
| ASA IV | A patient with severe systemic disease that is a constant threat to life | Recent (<3 moths)MI,CVA,TIA or CAD/stents, ongoing cardiac or severe valve dysfunction, severe reduction of ejection fraction, shock, sepsis, DIC,ARD or ESRD not undergoing regularly scheduled dialysis |
Symptomatic congenital cardiac abnormality, congestive heart failure, active squeal of prematurity, acute hypoxic ischemic encephalopathy, shock, sepsis, disseminated intravascular coagulation, automatic implantable cardioverter-defibrillator, ventilator dependence, endocrinopathy, severe trauma, severe respiratory distress, advanced oncological state. | Preeclampsia with severe features complicated by HELLP or other adverse event, peripartum cardiomyopathy with EF<40, uncorrected/decompensated heart disease, acquired or congenital. |
| ASA V | A moribund patient who is not expected to survive without the operation | Ruptured abdominal/thoracic aneurysm, massive trauma, intracranial bleed with mass effect, ischemic bowel in the face of significant cardiac pathology or multiple organ/system dysfunction | Massive trauma, intracranial hemorrhage with mass effect, patient requiring ECMO, respiratory failure or arrest, malignant hypertension, decompensated congestive heart failure, hepatic encephalopathy, ischemic bowel or multiple organ/system dysfunction. | Uterine rupture. |
| ASA VI | A declared brain-dead patient whose organs are being removed for donor purpose | |||
| *Although pregnancy is not a disease, the parturient’s physiologic state is significantly altered from when the woman is not pregnant, hence the assignment of ASA 2 for a woman with uncomplicated pregnancy.
**The addition of “E” denotes Emergency surgery: (An emergency is defined as existing when delay in treatment of the patient would lead to a significant increase in the threat to life or body part) |
||||
There are certain physical limitations that can change outcomes like those who have certain genetic predilections like malignant hyperthermia or suxamethonium apnea history, a difficult airway history or is a Jehovah’s witness.
Responsibility of the anesthetist
Even though the ASA status can be awarded while Pre-operative assignment is in process, it must be reconfirmed by the primary Anesthetist. It will be considered a deceased donor and anesthetic principals may be wary.
Issues regarding the subjectivity of ASA physical status have been silenced as its validity and authenticity has been explained in several papers.
Evolution of ASA in the future
Further addition of examples of modifying ASA PS status may still be necessary to make it more comprehensive and easier to use even for non-anesthetists to improve overall peri-operative morbidity and mortality.
Conclusion
Anesthesia preoperative evaluation holds prime importance in assessment of patient and has been a significant predictor of perioperative morbidity and mortality. It has evolved over 70 years and is still evolving to better standards. Additions of further examples are still necessary to make it useful even for non-anesthesia personnel.
In contrast, the evaluation of functional capacity that established a benchmark of the original 1941 classification was yet missing from the existing schemata and its revitalization may additionally mitigate its differences.
Authors’ contribution
All authors took equal part in the preparation of this manuscript.
References
- Saklad M. Grading of patients for surgical procedures. Anesthesiol. 1941 May 1;2(3):281–4. [FreeFullText]
- Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA. 1961;178:261–266. [PubMed] DOI: 10.1001/jama.1961.03040420001001
- Dripps RD. New Classification of Physical Status. Anesthesiol. 1963;24:111.
- Abouleish AE, Leib ML, Cohen NH. ASA provides examples to each ASA physical status class. ASA Monitor. 2015;79:38-9.
- Hurwitz EE, Simon M, Vinta SR, et al. Adding examples to the ASA-Physical Status classification improves correct assignments to patients. Anesthesiol. 2017;126:614-22. [PubMed] DOI: 1097/ALN.0000000000001541
- Mayhew D, Mendonca V, Murthy BVS. A review of ASA physical status – historical perspectives and modern developments. Anesthesia. 2019;74:373-9. [PubMed] DOI: 1111/anae.14569
- Leahy I, Berry JG, Johnson CJ, Crofton C, Staffa SJ, Ferrari L. Does the current American Society of Anesthesiologists Physical Status Classification represent the chronic disease burden in children undergoing general anesthesia? Anesth Analg. 2019 Oct;129(4):1175-1180. [PubMed] DOI: 1213/ANE.0000000000003911
- Ferrari L, Leahy I, Staffa S, Johnson C, Crofton C, Methot C, et al. One size does not fit all: a perspective on the American Society of Anesthesiologists physical status classification for pediatric patients. Anesth Analg. 2020;130(6):1685–1692. [PubMed] DOI: 1213/ANE.0000000000004277
- errari L, Leahy I, Staffa SJ, Berry JG. The Pediatric-Specific American Society of Anesthesiologists Physical Status Score: A Multicenter Study. Anesth Analg. 2021 Mar 1;132(3):807-817. [PubMed] DOI: 1213/ANE.0000000000005025
- Davenport DL, Bowe EA, Henderson WG, Khuri SF, Mentzer RM Jr. National Surgical Quality Improvement Program (NSQIP) risk factors can be used to validate American Society of Anesthesiologists Physical Status Classification (ASA PS) levels. Ann Surg. 2006 May;243(5):636-41. [PubMed] DOI: 1097/01.sla.0000216508.95556.cc
- Fitz-Henry J. The ASA classification and peri-operative risk. Ann R Coll Surg Engl. 2011 Apr;93(3):185-7. [PubMed] DOI: 1308/rcsann.2011.93.3.185a
- ASA Physical Status Classification System Committee of Oversight: Economics. Available from: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (assessed on 19-1-2021)