David Nugraha1, Nabila Ananda Kloping1, Resti Yudhawati2, Azham Purwandhono3, Hanik Badriyah Hidayati4
1- Faculty of Medicine, Universitas Airlangga, Surabaya, East Java, Indonesia.
2- Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, Universitas Airlangga / Dr. Soetomo General Hospital Surabaya, East Java, Indonesia.
3- Faculty of Medicine, University of Jember / Dr. Soebandi General Hospital Jember, East Java, Indonesia.
4- Department of Neurology, Faculty of Medicine, Universitas Airlangga / Dr. Soetomo General Hospital Surabaya, East Java, Indonesia.
Correspondence: Hanik Badriyah Hidayati, Phone: +62 82131035699; E-mail: hanikhidayati@yahoo.com
Abstract
Indonesia has been fighting the COVID-19 pandemic since the beginning of March 2020, and it doesn’t look that the situation is getting better any soon. Besides the country’s current strategies to minimize the rising mortality rate, a novel therapeutic intervention is required. After a thorough search in several databases, we found stem cells to be a likely candidate. Regardless of the general use of stem cells, studies showed positive results regarding the efficacy of using these in lung injuries. Especially, mesenchymal stem cells (MSCs) are known for their easy accessibility and their diverse mechanisms of action, including MSCs immunomodulatory antiviral effect, and its ability to improve lung function. Moreover, some researches perceived these components to be applicable in COVID-19 patients with end stage acute respiratory distress syndrome (ARDS). While randomized clinical trials are still in progress, many case reports show MSCs to be an advantageous alternative to suppress the cytokine storm and help regulate the immune system. This review summarizes the common functions of MSCs and highlights its therapeutic assets to fully tackle this global pandemic.
Key word: Mesenchymal Stem Cells; Cell Therapy; COVID-19; SARS-CoV-2; ARDS
Abbreviations: COVID-19 – Coronavirus Disease; MSC – Mesenchymal Stem Cell; ARDS – Acute Respiratory Distress Syndrome
Citation: Nugraha D, Kloping NA, Yudhawati R, Purwandhono A, Hidayati HB. A current update in COVID-19 associated acute respiratory distress syndrome: Focus on mesenchymal stem cell therapy. Anaesth. pain intensive care 2020;24(6):671-681.
DOI: https://doi.org/10.35975/apic.v24i6.1404
Received: 25 August 2020, Reviewed: 16 September 2020, Revised: 22 September 2020, Accepted: 29 September 2020
Introduction
Since August 7, 2020, Indonesia’s COVID-19 cases have set a new record. Indonesia has surpassed Peoples Republic of China with the total of 121,226 cases, 5,593 deaths, and 77,557 recovered.1 Adapting WHO’s six prioritized strategies, Indonesia has adopted several strategies to suppress the spread of COVID-19.2 Ever since the first case was confirmed to be positive, measures taken included large scale social restrictions, strict stay-at-home orders, improvement in healthcare services, and provision of personal protective equipment (PPEs) to healthcare workers across the country.3,4 Nevertheless, the virus is still circulating among the community with over 1000 new cases per day.1 There have been reports that hospitals taking care of COVID-19 patients have reached their total capacity.5
Aside from restraining virus transmission, a novel treatment plan is required to lessen the growing number of deaths caused by COVID-19. One of the suggested measure is the use of stem cells. Stem cells have been widely used in auto-immune and transplantation medicine, and can also be used in lung injuries.6,7 As the development of cell therapy grows, the researchers all around the world are now constantly trying to apply novel stem cell treatment in COVID-19 patients, particularly mesenchymal stem cells (MSCs). MSCs have attracted much attention due to their readily accessible source, their ability to easily expand to a large numbers, capability to repetitive therapeutic usage, and being without any known adverse events reported. It is compulsory to understand better the rationale and potential mechanisms of MSCs actions towards respiratory viral infections.8 This review aims to present an overview of the MSCs and their potential implication in treating COVID-19 infection.
This literature review was constructed by comprehensive data searching in several databases such as PubMed, Science Direct, Scopus, The Cochrane Library, and other websites. We searched all relevant related articles with keywords such as cell therapy, mesenchymal stem cells, COVID-19, SARS-CoV-2, ARDS, and its synonym during the search strategy. Boolean operators (AND, OR, NOT) were applied to broaden and narrow the search results with the following combination ((Cell therapy OR Mesenchymal Stem Cell) AND ((COVID-19 OR SARS-CoV2) AND ARDS)). Subsequently, we included all articles including comprehensive cohort studies, case reports, randomized controlled trials, and systematic reviews, as well as meta-analyses regarding MSCs therapy in COVID-19 patients until August 2020. The search was limited to articles published in the past ten years with language restriction to English and Bahasa Indonesia, as convenient to the reviewers. Some data regarding COVID-19 infection in Indonesia were also taken from acknowledged authorized websites.
COVID-19 Overview
Ever since the early 2000s, coronavirus (Co-V) has invaded the world as one of its most significant health problems. In 2002 SARS-Co-V (Severe Acute Respiratory Syndrome-Co-V) was first found in China and it brought upon an outbreak until 2004. In 2012 MERS (Middle East Respiratory Syndrome) Co-V was detected in Saudi Arabia in patients suffering from flu-like symptoms.9 In the late 2019, China discovered a new kind of pneumonia caused by the novel coronavirus, which has been labeled as corona virus disease-2019 (COVID-19) by WHO. The virus was first confirmed in Indonesia on 2 March 2020.2 Later on 11th March, WHO declared COVID-19 as a global pandemic.
Coronavirus is a single strand, positive RNA genome with 26-32kb, and is labeled as the largest RNA virus.9,10 Similar to SARS-CoV, COVID-19 uses angiotensin-converting enzyme 2 (ACE2) receptor to enter the host’s cells.10,11 Coronavirus will use the S protein on its surface to bind with the ACE2 receptor and inserts virus particles into host cells.10 ACE2 receptors are highly expressed in the lung, especially in the apical region within the alveolar space, but can also be found in other organs such as the heart, kidney and intestine.12,13 Additionally, studies also found protease activators such as TMPRSS2 and lysosomal proteases in cell entry.14 The host immune reaction is also similar to common acute viral infections. Immunoglobulin-M (Ig-M) antibodies of SARS-CoV can last upto 12 weeks, while IgG antibodies can last for a very long time. Although it is not confirmed yet, an animal experiment with rhesus macaques showed neutralizing antibodies of COVID-19 is enough to prevent reinfection in the first few days of recovery.15
The most common clinical features of COVID-19 are fever, cough and myalgia. There are also cases where patients showed congestion, sore throat, rhinorrhea, and diarrhea. Nonetheless, all COVID-19 patients exhibit bilateral ground-glass opacities in their radiographic images of the chest. Laboratory abnormalities that are frequently seen are lower lymphocyte count, higher lactate dehydrogenase, C-reactive protein and creatine kinase.16,17 Reports from immunological assessment stated that interleukin (IL)-6 was higher in patients in critical condition. IL-10, granulocyte-colony stimulating factor (G-CSF), monocyte chemoattractant protein 1 (MCP1), macrophage inflammatory protein (MIP) 1- α, and tumor necrosis factor (TNF-α) also increase in severe infections.12 From these rising cytokine levels, the uncontrolled systemic pro-inflammatory response could then trigger ARDS, thus leading to multiple organ failure, ultimately ending into death. Patients with ARDS showed a disturbance in homeostasis with elevating pro-inflammatory cytokines such as IFN-α, IFN-γ, IL-1-β, IL-6, IL-12, IL-18, IL-33, TNF-α, TGF-β and chemokines.11
Although the number of cases of SARS-CoV2-induced pneumonia patients is continuously increasing, there is no specific therapy. The current treatment has a limited effect on lung inflammation and regeneration. Considering the over-reactivity inflammatory state of SARS-CoV2, agents that modulate the immune response are being explored as alternative treatments for the management of moderate to critical COVID-19.18 Choices for treatment can be classified into RNA-dependent RNA polymerase inhibitors (remdesivir, favipiravir, ribavirin); interferons; protease inhibitors (lopinavir/ritonavir, chloroquine, hydroxychloroquine, azithromycin, teicoplanin, monoclonal antibodies); convalescent plasma; herbal medications and other considerations namely corticosteroids. Patients are given supportive treatment to maintain hydration and nutrition.19 Antipyretic, antimicrobial agents, and oxygen therapy are also prescribed as required.20,21 Corticosteroids are the most commonly prescribed medication. However, the associated adverse effect need to be monitored attentively.21 In India, hydroxychloroquine is now recommended for prophylactic use and recommended for healthcare personnel taking care of COVID-19 patients.22 Immunoglobulin from healed patients (convalescent plasma) is also deemed to be safe and effective, but it is prioritized for critically ill patients.23
MSCs Potential Clinical Applications as an Alternative Yet Promising Choice
Stem cells are the origin of all different types of cells in the human body. There are five types of stem cells: totipotent or omnipotent, which is the beginning of all life forms (zygote); pluripotent is usually known as the embryonic stem cells which will differentiate into the germinal layers (mesoderm, endoderm and ectoderm); multipotent are limited to a specific germ layer such as hematopoietic stem cell in the bone marrow; oligopotent or somatic stem cells can only differentiate into a more specific line, for instance myeloid stem cells; and lastly unipotent which can only multiply into one kind of cell type (muscle cell).7,24 Therapies involving stem cells are being used in many diseases. From preclinical and clinical trials stem cells are shown to have a positive effect on auto-immune diseases (type 1 diabetes mellitus), chronic myeloid leukemia, cirrhosis, pulmonary fibrosis, Crohn’s disease, cardiovascular diseases (heart failure), as well as neurodegenerative diseases.24,25 Nevertheless, among other stem cells, MSCs are seen as a rising star in cell therapy. MSCs are distinguished from others by their surface expressions. For instance, surface markers are CD73, CD90, CD105, human leukocyte antigen (HLA) Class I, etc. They also secrete various growth factors, cytokines, and immunomodulatory molecules.26,27 MSCs are mainly collected from the bone marrow, but can be found in adipose tissue, synovial tissue, lung, umbilical cord, and peripheral blood.26 Furthermore, MSCs are easy to isolate because they can maintain their characteristics for a long term.25 Due to MSCs chemotactic ability to migrate towards the damaged tissue, they are preferable to be administered through intravenous injection. This mechanism is similar to leukocytes, where some suggested that MSCs were also attracted to chemoattractants released by the injured site. Studies hypothesized that MSCs used a proteolytic enzyme called matrix metalloproteinase (MMPs) to move and attach to endothelial cells.28
What makes MSCs so promising are the end product of their interaction with the immune system. MSCs will interact with monocytes/macrophages, dendritic cells (DCs), T cells, B cells, and natural killer (NK) cells. MSCs are known to have at least five capacities (Figure 1) namely trophic/anti-apoptotic, anti-inflammatory, anti-bacterial, antiviral, and improving lung function.29–31 The anti-apoptotic properties of MSCs are believed to be mediated by production of growth factor and other chemokines to induce cell proliferation and angiogenesis.31 These molecules comprise of vascular endothelial growth factor (VEGF), insulin growth factor (IGF), hepatocyte growth factor (HGF), fibroblast growth factor-7 (FGF7), and interleukin-6 (IL-6).30–32 Besides anti-apoptotic properties, MSCs will stimulate paracrine factors as well as modulate the balance of pro and anti-inflammation. Paracrine mechanism took place when MSCs are directly in contact with the immune cells, thus cytokines such as TGF-beta, IL-10, and IL-1RA, nitric oxide, and indoleamine 2,3 dioxygenase (IDO) are released from MSCs. These cytokines will then affect the proliferation and activation of naïve and effector T cells.6 In addition, IDO has the potential to inhibit viral replication and reduce viral load.33
In response to inflammatory stimuli, MSCs secrete growth factor and key immunomodulatory anti-inflammatory cytokines such as PGE2, TGF- β1, HGF, SDF-1, NO, indoleamine 2,3-dioxygenase, IL-4, IL-6, IL-10, etc.31,34 In addition, MSCs indirectly induce the transition of T helper-1 (TH1) cells to T helper-2 (TH2) and shift macrophages from M1 to anti-inflammatory, tissue healing M2 state induced by directly secretes PGE2 and finally M2 will increase IL-4 and IL-10 production.29,30,35 Development of Th-17 pro-inflammatory cells is also suppressed by secreting anti-inflammatory cytokines.6,28 Studies suggested that monocyte differentiation into DCs are disturbed, as well as of DCs role as antigen presenting cells. Additionally, B cells proliferation, differentiation, and chemotaxis are also impeded by MSCs. Nevertheless, since MSCs help to regulate the immune system, they are not affected by the cytotoxic effect of other immune cells.28
Several anti-bacterial substrates secreted by MSCs have been identified. MSCs promote bacterial clearance directly by secreting lipocalin-2, LL-37, beta defensin-2, toll-like receptor (TLR4). MSCs will indirectly activate the phagocytic ability of neutrophils and alveolar macrophages when reprogramming them to an anti-inflammatory phenotype.30,36 There are also reports stating that LL-37 has the ability as an antiviral by degrading viral membrane.37
In the case of respiratory viral infections (SARS CoV-2), MSCs had two different potential antiviral mechanisms. First is by constitutively increasing levels of MSC-specific interferon-stimulated genes (ISGs) that has antiviral protection role, and secondly in response to interferon makes broad viral resistance by ISG induction.38,39 Furthermore, MSCs may interact with immune cells and promote T-regulatory cells (Tregs), which enhances virus clearance.29 MSCs could serve as an integrated innate antiviral defense that could lead to therapeutic advantages in COVID-19 patients. In these patients, ARDS may manifest itself as impaired alveolar fluid clearance, which is associated with higher morbidity and mortality. The secretion of keratinocyte growth factor (KGF) and angiopoietin-1 (Ang-1) by MSCs essentially contribute to the restoration of alveolar-capillary barriers disrupted as part of ARDS pathogenesis.38 Beside KGF and Ang-1, FGF7 secreted by MSCs is also taking a significant role to improve alveolar fluid clearance.30 To sum up, a pro-inflammatory environment like IFN-gamma can trigger immunomodulatory aspects of MSCs, and a higher level of an anti-inflammatory agent will terminate MSCs immunosuppressive mechanism.
MSCs Therapy for ARDS
Acute lung injury (ALI) is a disease characterized by capillary membrane injury, causing pulmonary edema and atelectasis.40 The main clinical manifestation is an acute onset of hypoxic respiratory failure, which can subsequently trigger a cascade of profound complications and even death. ALI is an old terminology which previously used to describe mild acute respiratory distress syndrome (ARDS) with PaO2/FiO2 (PF) ratio of 200-300.29 The current definition of ARDS is clinical, based on measurement of hypoxemia, the initial occurrence of injury, and bilateral infiltrates finding on chest x-ray without any cardiogenic cause.29 ARDS develops most commonly in the setting of pneumonia (bacterial and viral being more common than fungal), non-pulmonary sepsis, aspiration of gastric and/or oral and esophageal contents and major trauma such as blunt or penetrating injuries as well as burns.41
Most of the COVID-19 patients suffer from ARDS. A single-centered retrospective study in Wuhan, China reported that approximately 67% of critically ill COVID-19 patients develop ARDS with considerable mortality rate.42 This respiratory distress peaks at 7 to 10 days with manifestations of immune dysregulation, including cytokine storm with the rise of cytokine levels (IL-6, IL-8, IL-1, IL2R, IL-10, and TNF-α), lymphopenia (in CD4+ and CD8+ T cells), and decreases in IFN-γ expression in CD4+ T cells.17 To date, many therapeutics efforts have been proposed regarding ARDS management, yet none have proven to be effective, and thus supportive strategies including low tidal volume mechanical ventilation, the institution of antibiotics, and fluid restriction remain the mainstay of therapy.43 Nevertheless, an increasing number of clinical investigations of cell-based therapies, primarily MSCs has been conducted. Recent data in models of respiratory virus-associated ARDS with MSCs administration showed promising results.
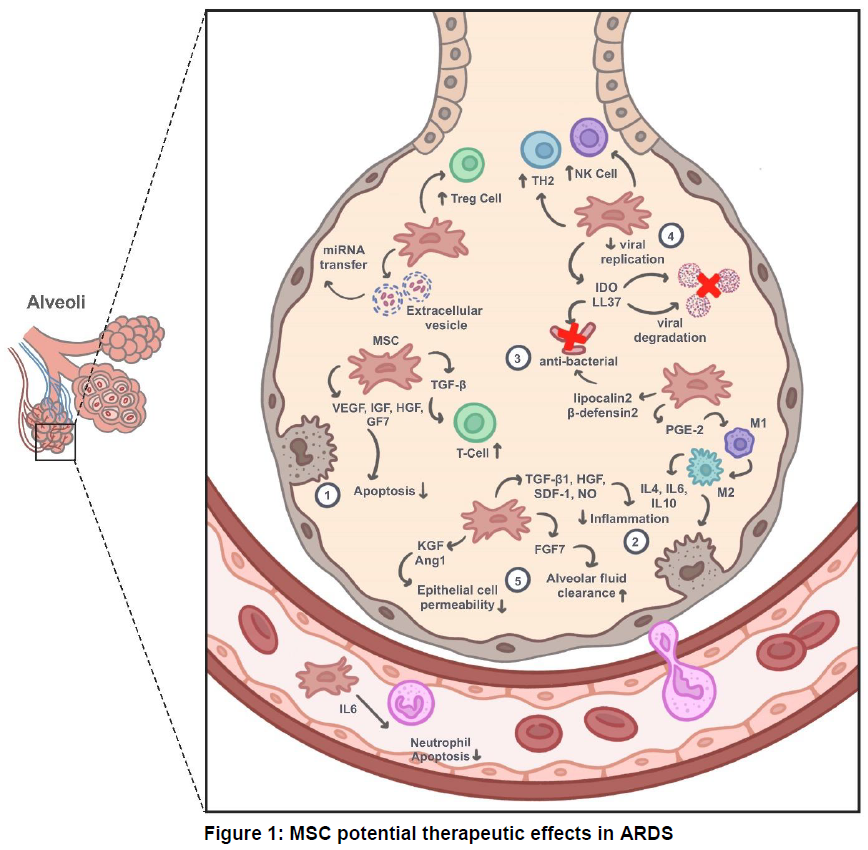
Mesenchymal stem cell (MSC) has five potential roles, which makes MSCs so promising. First, they secrete several growth factors and chemokines like vascular endothelial growth factor (VEGF), insulin growth factor (IGF), hepatocyte growth factor (HGF), fibroblast growth factor (FGF7). Second, MSC secretes key immunomodulatory anti-inflammatory cytokines such as PGE2, TGF-β1, HGF, SDF-1, NO, indoleamine 2,3-dioxygenase (IDO), IL-4, IL-6, IL-10. Third, lipocalin-2, LL-37, beta defensin-2 have an anti-bacterial effect. Fourth, IDO and LL-37 also have antiviral activity. Fifth, MSC enhances alveolar lung function through its paracrine factors like KGF, Ang-1, and FGF7.
A single-centered, open-label, randomized study, RUMCESS (NCT 01849237), reported that a group treated with MSCs (1 x 106 MSC IV) showed a significant increase in 28-days survival rates (57% vs. 15%) and was associated with lower SOFA-scores.44 Another study conducted by Simonson et al. reported that after being treated with 2 x 106 cells/kg bone marrow stromal cells (BMSCs), their subjects showed a decrease in epithelial apoptosis markers, alveolar-capillary fluid leakage, miRNA, and chemokines in plasma and BAL fluid.45 Following intravenous administration, the majority of MSCs will accumulate in the pulmonary vascular bed and interact with the capillary endothelial cells.38 In the case of ARDS, this action may be a beneficial as this would facilitate a high local concentration of MSCs directly at the site of inflammation. MSCs will secrete several paracrine signals that can play a significant role in protecting or recovering alveolar epithelial cells, enhance lung function, and reduce inflammation.46
Current Evidence on MSCs Treatment
Since the outbreak of SARS CoV-2 in December 2019, cell-based therapy, in particular MSCs, exhibits favorable results, as described earlier, to cure lung injuries. As of 31st July 2020, there are 52 COVID-19 clinical trial using various sources of MSCs registered on the NIH website www.clinicaltrials.gov (Table 1). There are 23 trials using allogenic MSCs, while only three trials using autologous MSCs; the remaining trials were unspecified. Among these, 14 trials used UC-MSCs, seven trials used AD-MSCs, five trials used BMSCs, and four trials used WJ-MSCs. Autologous cells are used less often because it needs more time to be processed, thus it is not feasible for the deteriorating patient’s condition.47 Dental pulp MSCs were used in two studies, one trial used olfactory mucosa MSCs, the second trial used exosome derived MSCs. One study used core blood cell, while the remaining did not specify the type of MSCs.
Table 1 : Ongoing MSCs clinical trials for COVID-19
Legend: C-19 - Coronavirus disease; ARDS - Acute respiratory distress syndrome; MSC - Mesenchymal stem cell;
UC-MSC - umbilical cord-derived mesenchymal stem cell; WJ-MSC - Wharton-Jelly derived mesenchymal stem cell;
AD-MSC - Adipose-derived mesenchymal stem cell; NYR – Not yet recruiting
A prospective, non-randomized, open-label cohort study used exosome derived BMSCs in treating severe COVID-19 patients.48 The cells were administered intravenously over 60 min, and the outcome was observed for the next five days. Overall, the survival rate was over 83%. 71% of the patients (17/24) recovered with no adverse events. The patients' clinical status and oxygenation (PaO2/FiO2) improved significantly as well as the laboratory findings, including lymphocyte and neutrophil counts, CRP, and D-Dimer levels. Additionally, it is widely accepted to use exosome derived MSCs. The exosome properties provide protective paracrine effects without having to inject living cell; therefore it could prevent immunological adverse events.34,38
Another single-centered, open-label pilot study in Beijing, China, administered BMSCs into seven COVID-19 patients with various degrees of severity. One patient was categorized as critically ill, four with a severe condition, and two had mild symptoms. They injected 106 cells/kg BMSCs intravenously and followed them for 14 days. Neither toxicity or allergy, nor other adverse events were reported, and the patients displayed clinical improvement of their pulmonary function and symptoms after 2-4 days.49 Along with this study, Rogers et al. showed that infused MSCs did not interact with the ACE2 receptor and TMPRSS2, which implied that MSCs would not associate with SARS-CoV-2.29
A 65-year-old female critically ill COVID-19 patient indicated a good clinical remission after MSCs treatment.50 After antiviral and glucocorticoid management failed to show any improvement, she received UC-MSCs (5 x 107 cells) intravenously. After the second administration, neutrophil count decreased, lymphocytes increased as well as CD3+T cell, CD4+T cell, and CD8+T cell back to normal. On the CT scan findings, it was reported that the pneumonia imaging greatly improved, and she was finally released from the hospital with a negative swab test. This finding suggested that MSCs could improve patient outcomes even in elderly. A meta-analysis revealed that MSCs treatment did decrease the mortality rate in COVID-19 patients.51 From these reported cases, there were notable improvements in lung compliance and tidal volume in COVID-19-induced ARDS treated with MSCs.
Limitations in MSCs therapy
Before resolving the use of MSCs for the recommended therapy, several things need to be acknowledged. Stem cells therapy is a complicated one, and there are cases where unwanted side effects did occur. Even though MSCs are relatively safe, a study reported immunosuppression in some patients with injured lungs, causing secondary infection.52 A similar case was also described in patients receiving MSCs as immunosuppressive after having hematopoietic stem cell transplantation.53 More in-depth research in utilizing MSCs is needed to prevent unwanted differentiation of MSCs in local engrafted setting. Lastly, despite the positive impact of the paracrine and endocrine mechanism by MSCs, they may stimulate proangiogenic factors (VEGF, HGF, angiopoietin-1, platelet-derived growth factor, and placental growth factor) which is in line with augmenting tumor growth.28,52,53 Long term use of MSCs could also cause the production of allo-antibodies, while single use of MSCs are harmless and did not cause any dangerous immune response.28 More trials are necessary to know the side effects that MSCs may carry.
Conclusion and recommendation
In conclusion, although there is no standardized therapy for SARS Co-V2, MSC is a promising alternative treatment. Several studies, both pre-clinical and early clinical, have provided tantalizing clues that MSCs can provide a consistent therapeutic benefit. Moreover, the majority of previous results confirmed that MSCs are capable of dampening the over-reactivity inflammation cascade, decreasing infection, improving lung recovery, and increase the survival rate. It may take several months even years to develop a vaccine, and even if it's effective, it will not completely eradicate the ongoing infection. Further clinical trials regarding MSCs-based therapies in ARDS are urgently needed, including investigation regarding its safety.
Conflict of interest
No funding was used for the preparation of this review.
Authors’ contribution
DN: concept, literature search, manuscript writing, figure illustration
NAK: concept, literature search, manuscript editing
RY: manuscript editing
AP: bibliography editing
HBH: concept, manuscript editing
References
1- Faculty of Medicine, Universitas Airlangga, Surabaya, East Java, Indonesia.
2- Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, Universitas Airlangga / Dr. Soetomo General Hospital Surabaya, East Java, Indonesia.
3- Faculty of Medicine, University of Jember / Dr. Soebandi General Hospital Jember, East Java, Indonesia.
4- Department of Neurology, Faculty of Medicine, Universitas Airlangga / Dr. Soetomo General Hospital Surabaya, East Java, Indonesia.
Correspondence: Hanik Badriyah Hidayati, Phone: +62 82131035699; E-mail: hanikhidayati@yahoo.com
Abstract
Indonesia has been fighting the COVID-19 pandemic since the beginning of March 2020, and it doesn’t look that the situation is getting better any soon. Besides the country’s current strategies to minimize the rising mortality rate, a novel therapeutic intervention is required. After a thorough search in several databases, we found stem cells to be a likely candidate. Regardless of the general use of stem cells, studies showed positive results regarding the efficacy of using these in lung injuries. Especially, mesenchymal stem cells (MSCs) are known for their easy accessibility and their diverse mechanisms of action, including MSCs immunomodulatory antiviral effect, and its ability to improve lung function. Moreover, some researches perceived these components to be applicable in COVID-19 patients with end stage acute respiratory distress syndrome (ARDS). While randomized clinical trials are still in progress, many case reports show MSCs to be an advantageous alternative to suppress the cytokine storm and help regulate the immune system. This review summarizes the common functions of MSCs and highlights its therapeutic assets to fully tackle this global pandemic.
Key word: Mesenchymal Stem Cells; Cell Therapy; COVID-19; SARS-CoV-2; ARDS
Abbreviations: COVID-19 – Coronavirus Disease; MSC – Mesenchymal Stem Cell; ARDS – Acute Respiratory Distress Syndrome
Citation: Nugraha D, Kloping NA, Yudhawati R, Purwandhono A, Hidayati HB. A current update in COVID-19 associated acute respiratory distress syndrome: Focus on mesenchymal stem cell therapy. Anaesth. pain intensive care 2020;24(6):671-681.
DOI: https://doi.org/10.35975/apic.v24i6.1404
Received: 25 August 2020, Reviewed: 16 September 2020, Revised: 22 September 2020, Accepted: 29 September 2020
Introduction
Since August 7, 2020, Indonesia’s COVID-19 cases have set a new record. Indonesia has surpassed Peoples Republic of China with the total of 121,226 cases, 5,593 deaths, and 77,557 recovered.1 Adapting WHO’s six prioritized strategies, Indonesia has adopted several strategies to suppress the spread of COVID-19.2 Ever since the first case was confirmed to be positive, measures taken included large scale social restrictions, strict stay-at-home orders, improvement in healthcare services, and provision of personal protective equipment (PPEs) to healthcare workers across the country.3,4 Nevertheless, the virus is still circulating among the community with over 1000 new cases per day.1 There have been reports that hospitals taking care of COVID-19 patients have reached their total capacity.5
Aside from restraining virus transmission, a novel treatment plan is required to lessen the growing number of deaths caused by COVID-19. One of the suggested measure is the use of stem cells. Stem cells have been widely used in auto-immune and transplantation medicine, and can also be used in lung injuries.6,7 As the development of cell therapy grows, the researchers all around the world are now constantly trying to apply novel stem cell treatment in COVID-19 patients, particularly mesenchymal stem cells (MSCs). MSCs have attracted much attention due to their readily accessible source, their ability to easily expand to a large numbers, capability to repetitive therapeutic usage, and being without any known adverse events reported. It is compulsory to understand better the rationale and potential mechanisms of MSCs actions towards respiratory viral infections.8 This review aims to present an overview of the MSCs and their potential implication in treating COVID-19 infection.
This literature review was constructed by comprehensive data searching in several databases such as PubMed, Science Direct, Scopus, The Cochrane Library, and other websites. We searched all relevant related articles with keywords such as cell therapy, mesenchymal stem cells, COVID-19, SARS-CoV-2, ARDS, and its synonym during the search strategy. Boolean operators (AND, OR, NOT) were applied to broaden and narrow the search results with the following combination ((Cell therapy OR Mesenchymal Stem Cell) AND ((COVID-19 OR SARS-CoV2) AND ARDS)). Subsequently, we included all articles including comprehensive cohort studies, case reports, randomized controlled trials, and systematic reviews, as well as meta-analyses regarding MSCs therapy in COVID-19 patients until August 2020. The search was limited to articles published in the past ten years with language restriction to English and Bahasa Indonesia, as convenient to the reviewers. Some data regarding COVID-19 infection in Indonesia were also taken from acknowledged authorized websites.
COVID-19 Overview
Ever since the early 2000s, coronavirus (Co-V) has invaded the world as one of its most significant health problems. In 2002 SARS-Co-V (Severe Acute Respiratory Syndrome-Co-V) was first found in China and it brought upon an outbreak until 2004. In 2012 MERS (Middle East Respiratory Syndrome) Co-V was detected in Saudi Arabia in patients suffering from flu-like symptoms.9 In the late 2019, China discovered a new kind of pneumonia caused by the novel coronavirus, which has been labeled as corona virus disease-2019 (COVID-19) by WHO. The virus was first confirmed in Indonesia on 2 March 2020.2 Later on 11th March, WHO declared COVID-19 as a global pandemic.
Coronavirus is a single strand, positive RNA genome with 26-32kb, and is labeled as the largest RNA virus.9,10 Similar to SARS-CoV, COVID-19 uses angiotensin-converting enzyme 2 (ACE2) receptor to enter the host’s cells.10,11 Coronavirus will use the S protein on its surface to bind with the ACE2 receptor and inserts virus particles into host cells.10 ACE2 receptors are highly expressed in the lung, especially in the apical region within the alveolar space, but can also be found in other organs such as the heart, kidney and intestine.12,13 Additionally, studies also found protease activators such as TMPRSS2 and lysosomal proteases in cell entry.14 The host immune reaction is also similar to common acute viral infections. Immunoglobulin-M (Ig-M) antibodies of SARS-CoV can last upto 12 weeks, while IgG antibodies can last for a very long time. Although it is not confirmed yet, an animal experiment with rhesus macaques showed neutralizing antibodies of COVID-19 is enough to prevent reinfection in the first few days of recovery.15
The most common clinical features of COVID-19 are fever, cough and myalgia. There are also cases where patients showed congestion, sore throat, rhinorrhea, and diarrhea. Nonetheless, all COVID-19 patients exhibit bilateral ground-glass opacities in their radiographic images of the chest. Laboratory abnormalities that are frequently seen are lower lymphocyte count, higher lactate dehydrogenase, C-reactive protein and creatine kinase.16,17 Reports from immunological assessment stated that interleukin (IL)-6 was higher in patients in critical condition. IL-10, granulocyte-colony stimulating factor (G-CSF), monocyte chemoattractant protein 1 (MCP1), macrophage inflammatory protein (MIP) 1- α, and tumor necrosis factor (TNF-α) also increase in severe infections.12 From these rising cytokine levels, the uncontrolled systemic pro-inflammatory response could then trigger ARDS, thus leading to multiple organ failure, ultimately ending into death. Patients with ARDS showed a disturbance in homeostasis with elevating pro-inflammatory cytokines such as IFN-α, IFN-γ, IL-1-β, IL-6, IL-12, IL-18, IL-33, TNF-α, TGF-β and chemokines.11
Although the number of cases of SARS-CoV2-induced pneumonia patients is continuously increasing, there is no specific therapy. The current treatment has a limited effect on lung inflammation and regeneration. Considering the over-reactivity inflammatory state of SARS-CoV2, agents that modulate the immune response are being explored as alternative treatments for the management of moderate to critical COVID-19.18 Choices for treatment can be classified into RNA-dependent RNA polymerase inhibitors (remdesivir, favipiravir, ribavirin); interferons; protease inhibitors (lopinavir/ritonavir, chloroquine, hydroxychloroquine, azithromycin, teicoplanin, monoclonal antibodies); convalescent plasma; herbal medications and other considerations namely corticosteroids. Patients are given supportive treatment to maintain hydration and nutrition.19 Antipyretic, antimicrobial agents, and oxygen therapy are also prescribed as required.20,21 Corticosteroids are the most commonly prescribed medication. However, the associated adverse effect need to be monitored attentively.21 In India, hydroxychloroquine is now recommended for prophylactic use and recommended for healthcare personnel taking care of COVID-19 patients.22 Immunoglobulin from healed patients (convalescent plasma) is also deemed to be safe and effective, but it is prioritized for critically ill patients.23
MSCs Potential Clinical Applications as an Alternative Yet Promising Choice
Stem cells are the origin of all different types of cells in the human body. There are five types of stem cells: totipotent or omnipotent, which is the beginning of all life forms (zygote); pluripotent is usually known as the embryonic stem cells which will differentiate into the germinal layers (mesoderm, endoderm and ectoderm); multipotent are limited to a specific germ layer such as hematopoietic stem cell in the bone marrow; oligopotent or somatic stem cells can only differentiate into a more specific line, for instance myeloid stem cells; and lastly unipotent which can only multiply into one kind of cell type (muscle cell).7,24 Therapies involving stem cells are being used in many diseases. From preclinical and clinical trials stem cells are shown to have a positive effect on auto-immune diseases (type 1 diabetes mellitus), chronic myeloid leukemia, cirrhosis, pulmonary fibrosis, Crohn’s disease, cardiovascular diseases (heart failure), as well as neurodegenerative diseases.24,25 Nevertheless, among other stem cells, MSCs are seen as a rising star in cell therapy. MSCs are distinguished from others by their surface expressions. For instance, surface markers are CD73, CD90, CD105, human leukocyte antigen (HLA) Class I, etc. They also secrete various growth factors, cytokines, and immunomodulatory molecules.26,27 MSCs are mainly collected from the bone marrow, but can be found in adipose tissue, synovial tissue, lung, umbilical cord, and peripheral blood.26 Furthermore, MSCs are easy to isolate because they can maintain their characteristics for a long term.25 Due to MSCs chemotactic ability to migrate towards the damaged tissue, they are preferable to be administered through intravenous injection. This mechanism is similar to leukocytes, where some suggested that MSCs were also attracted to chemoattractants released by the injured site. Studies hypothesized that MSCs used a proteolytic enzyme called matrix metalloproteinase (MMPs) to move and attach to endothelial cells.28
What makes MSCs so promising are the end product of their interaction with the immune system. MSCs will interact with monocytes/macrophages, dendritic cells (DCs), T cells, B cells, and natural killer (NK) cells. MSCs are known to have at least five capacities (Figure 1) namely trophic/anti-apoptotic, anti-inflammatory, anti-bacterial, antiviral, and improving lung function.29–31 The anti-apoptotic properties of MSCs are believed to be mediated by production of growth factor and other chemokines to induce cell proliferation and angiogenesis.31 These molecules comprise of vascular endothelial growth factor (VEGF), insulin growth factor (IGF), hepatocyte growth factor (HGF), fibroblast growth factor-7 (FGF7), and interleukin-6 (IL-6).30–32 Besides anti-apoptotic properties, MSCs will stimulate paracrine factors as well as modulate the balance of pro and anti-inflammation. Paracrine mechanism took place when MSCs are directly in contact with the immune cells, thus cytokines such as TGF-beta, IL-10, and IL-1RA, nitric oxide, and indoleamine 2,3 dioxygenase (IDO) are released from MSCs. These cytokines will then affect the proliferation and activation of naïve and effector T cells.6 In addition, IDO has the potential to inhibit viral replication and reduce viral load.33
In response to inflammatory stimuli, MSCs secrete growth factor and key immunomodulatory anti-inflammatory cytokines such as PGE2, TGF- β1, HGF, SDF-1, NO, indoleamine 2,3-dioxygenase, IL-4, IL-6, IL-10, etc.31,34 In addition, MSCs indirectly induce the transition of T helper-1 (TH1) cells to T helper-2 (TH2) and shift macrophages from M1 to anti-inflammatory, tissue healing M2 state induced by directly secretes PGE2 and finally M2 will increase IL-4 and IL-10 production.29,30,35 Development of Th-17 pro-inflammatory cells is also suppressed by secreting anti-inflammatory cytokines.6,28 Studies suggested that monocyte differentiation into DCs are disturbed, as well as of DCs role as antigen presenting cells. Additionally, B cells proliferation, differentiation, and chemotaxis are also impeded by MSCs. Nevertheless, since MSCs help to regulate the immune system, they are not affected by the cytotoxic effect of other immune cells.28
Several anti-bacterial substrates secreted by MSCs have been identified. MSCs promote bacterial clearance directly by secreting lipocalin-2, LL-37, beta defensin-2, toll-like receptor (TLR4). MSCs will indirectly activate the phagocytic ability of neutrophils and alveolar macrophages when reprogramming them to an anti-inflammatory phenotype.30,36 There are also reports stating that LL-37 has the ability as an antiviral by degrading viral membrane.37
In the case of respiratory viral infections (SARS CoV-2), MSCs had two different potential antiviral mechanisms. First is by constitutively increasing levels of MSC-specific interferon-stimulated genes (ISGs) that has antiviral protection role, and secondly in response to interferon makes broad viral resistance by ISG induction.38,39 Furthermore, MSCs may interact with immune cells and promote T-regulatory cells (Tregs), which enhances virus clearance.29 MSCs could serve as an integrated innate antiviral defense that could lead to therapeutic advantages in COVID-19 patients. In these patients, ARDS may manifest itself as impaired alveolar fluid clearance, which is associated with higher morbidity and mortality. The secretion of keratinocyte growth factor (KGF) and angiopoietin-1 (Ang-1) by MSCs essentially contribute to the restoration of alveolar-capillary barriers disrupted as part of ARDS pathogenesis.38 Beside KGF and Ang-1, FGF7 secreted by MSCs is also taking a significant role to improve alveolar fluid clearance.30 To sum up, a pro-inflammatory environment like IFN-gamma can trigger immunomodulatory aspects of MSCs, and a higher level of an anti-inflammatory agent will terminate MSCs immunosuppressive mechanism.
MSCs Therapy for ARDS
Acute lung injury (ALI) is a disease characterized by capillary membrane injury, causing pulmonary edema and atelectasis.40 The main clinical manifestation is an acute onset of hypoxic respiratory failure, which can subsequently trigger a cascade of profound complications and even death. ALI is an old terminology which previously used to describe mild acute respiratory distress syndrome (ARDS) with PaO2/FiO2 (PF) ratio of 200-300.29 The current definition of ARDS is clinical, based on measurement of hypoxemia, the initial occurrence of injury, and bilateral infiltrates finding on chest x-ray without any cardiogenic cause.29 ARDS develops most commonly in the setting of pneumonia (bacterial and viral being more common than fungal), non-pulmonary sepsis, aspiration of gastric and/or oral and esophageal contents and major trauma such as blunt or penetrating injuries as well as burns.41
Most of the COVID-19 patients suffer from ARDS. A single-centered retrospective study in Wuhan, China reported that approximately 67% of critically ill COVID-19 patients develop ARDS with considerable mortality rate.42 This respiratory distress peaks at 7 to 10 days with manifestations of immune dysregulation, including cytokine storm with the rise of cytokine levels (IL-6, IL-8, IL-1, IL2R, IL-10, and TNF-α), lymphopenia (in CD4+ and CD8+ T cells), and decreases in IFN-γ expression in CD4+ T cells.17 To date, many therapeutics efforts have been proposed regarding ARDS management, yet none have proven to be effective, and thus supportive strategies including low tidal volume mechanical ventilation, the institution of antibiotics, and fluid restriction remain the mainstay of therapy.43 Nevertheless, an increasing number of clinical investigations of cell-based therapies, primarily MSCs has been conducted. Recent data in models of respiratory virus-associated ARDS with MSCs administration showed promising results.
Mesenchymal stem cell (MSC) has five potential roles, which makes MSCs so promising. First, they secrete several growth factors and chemokines like vascular endothelial growth factor (VEGF), insulin growth factor (IGF), hepatocyte growth factor (HGF), fibroblast growth factor (FGF7). Second, MSC secretes key immunomodulatory anti-inflammatory cytokines such as PGE2, TGF-β1, HGF, SDF-1, NO, indoleamine 2,3-dioxygenase (IDO), IL-4, IL-6, IL-10. Third, lipocalin-2, LL-37, beta defensin-2 have an anti-bacterial effect. Fourth, IDO and LL-37 also have antiviral activity. Fifth, MSC enhances alveolar lung function through its paracrine factors like KGF, Ang-1, and FGF7.
A single-centered, open-label, randomized study, RUMCESS (NCT 01849237), reported that a group treated with MSCs (1 x 106 MSC IV) showed a significant increase in 28-days survival rates (57% vs. 15%) and was associated with lower SOFA-scores.44 Another study conducted by Simonson et al. reported that after being treated with 2 x 106 cells/kg bone marrow stromal cells (BMSCs), their subjects showed a decrease in epithelial apoptosis markers, alveolar-capillary fluid leakage, miRNA, and chemokines in plasma and BAL fluid.45 Following intravenous administration, the majority of MSCs will accumulate in the pulmonary vascular bed and interact with the capillary endothelial cells.38 In the case of ARDS, this action may be a beneficial as this would facilitate a high local concentration of MSCs directly at the site of inflammation. MSCs will secrete several paracrine signals that can play a significant role in protecting or recovering alveolar epithelial cells, enhance lung function, and reduce inflammation.46
Current Evidence on MSCs Treatment
Since the outbreak of SARS CoV-2 in December 2019, cell-based therapy, in particular MSCs, exhibits favorable results, as described earlier, to cure lung injuries. As of 31st July 2020, there are 52 COVID-19 clinical trial using various sources of MSCs registered on the NIH website www.clinicaltrials.gov (Table 1). There are 23 trials using allogenic MSCs, while only three trials using autologous MSCs; the remaining trials were unspecified. Among these, 14 trials used UC-MSCs, seven trials used AD-MSCs, five trials used BMSCs, and four trials used WJ-MSCs. Autologous cells are used less often because it needs more time to be processed, thus it is not feasible for the deteriorating patient’s condition.47 Dental pulp MSCs were used in two studies, one trial used olfactory mucosa MSCs, the second trial used exosome derived MSCs. One study used core blood cell, while the remaining did not specify the type of MSCs.
Table 1 : Ongoing MSCs clinical trials for COVID-19
| No | NCT | Status | Phase | Conditions | Type of Stem Cell | Locations |
| 1 | NCT04444271 | Recruiting | 2 | C-19 | MSCs | Pakistan |
| 2 | NCT04416139 | Recruiting | 2 | C-19 | MSCs | Mexico |
| 3 | NCT04429763 | NYR | 2 | C-19 | UC-MSCs | N/A |
| 4 | NCT04315987 | NYR | 2 | C-19 Pneumonia | MSCs | Brazil |
| NCT04456361 | Active, not recruiting | 1 | C-19 ARDS | WJ-MSCs | Mexico | |
| 6 | NCT04252118 | Recruiting | 1 | C-19 | MSCs | China |
| 7 | NCT04366271 | Recruiting | 2 | C-19 | MSCs | Spain |
| 8 | NCT04366323 | Recruiting | 2 | C-19 | Allogenic AD-MSCs | Spain |
| 9 | NCT04313322 | Recruiting | 1 | C-19 | WJ-MSCs | Jordan |
| 10 | NCT04336254 | Recruiting | 1 | C-19 | Allogeneic dental pulp stem cells | China |
| 11 | NCT04346368 | NYR | 1 | C-19 | BM-MSCs | China |
| 12 | NCT04288102 | Active, not recruiting | 2 | C-19 | UC-MSCs | China |
| 13 | NCT04273646 | NYR | N/A | Pneumonia, C-19 | UC-MSCs | China |
| 14 | NCT04348435 | Enrolling by invitation | 2 | C-19 | AD-MSCs | USA |
| 15 | NCT04382547 | Enrolling by invitation | 1 | Pneumonia, C-19 | Allogenic pooled olfactory mucosa-derived MSCs | Belarus |
| 16 | NCT04366063 | Recruiting | 3 | C-19 | MSCs | Iran |
| 17 | NCT04339660 | Recruiting | 1 | C-19 | UC-MSCs | China |
| 18 | NCT04428801 | NYR | 2 | C-19 | Autologous AD-MSCs | N/A |
| 19 | NCT04349631 | Enrolling by invitation | 2 | C-19 | AD-MSCs | USA |
| 20 | NCT04457609 | Recruiting | 1 | C-19 | UC-MSCs | Indonesia |
| 21 | NCT04352803 | NYR | 1 | Pneumonia, C-19 | autologous AD-MSCs | N/A |
| 22 | NCT04302519 | NYR | 1 | C-19 | Dental pulp MSCs | N/A |
| 23 | NCT04490486 | NYR | 1 | ARDS, C-19 | UC-MSCs | USA |
| 24 | NCT04355728 | Recruiting | 1 | ARDS, C-19 | UC-MSCs | USA |
| 25 | NCT04461925 | Recruiting | 1 | Pneumonia, C-19 | Placenta-Derived MSCs | Ukraine |
| 26 | NCT04371601 | Active, not recruiting | 1 | Pneumonia, C-19 | MSCs | China |
| 27 | NCT04348461 | NYR | 2 | ARDS, C-19 | Allogeneic AD-MSCS | N/A |
| 28 | NCT04362189 | Recruiting | 2 | C-19 | AD-MSCs | USA |
| 29 | NCT04390152 | NYR | 1 | ARDS, C-19 | WJ-MSCs | Colombia |
| 30 | NCT04452097 | NYR | 1 | ARDS, C-19 | UC-MSCs | N/A |
| 31 | NCT04371393 | Recruiting | 3 | ARDS, C-19 | MSCs | USA |
| 32 | NCT04397796 | NYR | 1 | C-19 | Bone Marrow derived MSCs | N/A |
| 33 | NCT04494386 | Recruiting | 1 | ARDS, C-19 | Umbilical Cord Lining Stem Cells | USA |
| 34 | NCT04377334 | NYR | 2 | ARDS, C-19 | MSCs | Germany |
| 35 | NCT04345601 | NYR | 1 | ARDS, C-19 | MSCs | USA |
| 36 | NCT04390139 | Recruiting | 2 | ARDS, C-19 | WJ-MSCs | Spain |
| 37 | NCT04392778 | Recruiting | 1 | Pneumonia, C-19, MOF | MSCs | Turkey |
| 38 | NCT04467047 | NYR | 1 | C-19 | MSCs | N/A |
| 39 | NCT04398303 | NYR | 1 | Pneumonia, C-19 | UC-MSCs | N/A |
| 40 | NCT04361942 | Recruiting | 2 | Pneumonia, C-19 | MSCs | Spain |
| 41 | NCT03042143 | Recruiting | 1 | ARDS, C-19 | UC-MSCs | UK |
| 42 | NCT04269525 | Recruiting | 2 | Pneumonia, C-19 | UC-MSCs | China |
| 43 | NCT04389450 | Recruiting | 2 | ARDS, C-19 | MSCs | USA |
| 44 | NCT04447833 | Recruiting | 1 | ARDS, C-19 | MSCs | Sweden |
| 45 | NCT04437823 | Recruiting | 2 | C-19 | UC-MSCs | Pakistan |
| 46 | NCT04491240 | Enrolling by invitation | 2 | Pneumonia, C-19 | MSCs-derived exosomes | Russia |
| 47 | NCT04333368 | Recruiting | 1 | ARDS, C-19 | WJ-MSCs | France |
| 48 | NCT04299152 | NYR | 2 | Pneumonia, C-19 | Cord blood stem cell | N/A |
| 49 | NCT04466098 | NYR | 2 | Pneumonia, ARDS, C-19 | MSCs | USA |
| 50 | NCT04445220 | NYR | 1 | C-19, Acute kidney injury | Allogenic MSCs | N/A |
| 51 | NCT04400032 | NYR | 1 | ARDS, C-19 | MSCs | Canada |
| 52 | NCT04276987 | NYR | 1 | C-19 | MSCs-derived exosomes | N/A |
UC-MSC - umbilical cord-derived mesenchymal stem cell; WJ-MSC - Wharton-Jelly derived mesenchymal stem cell;
AD-MSC - Adipose-derived mesenchymal stem cell; NYR – Not yet recruiting
A prospective, non-randomized, open-label cohort study used exosome derived BMSCs in treating severe COVID-19 patients.48 The cells were administered intravenously over 60 min, and the outcome was observed for the next five days. Overall, the survival rate was over 83%. 71% of the patients (17/24) recovered with no adverse events. The patients' clinical status and oxygenation (PaO2/FiO2) improved significantly as well as the laboratory findings, including lymphocyte and neutrophil counts, CRP, and D-Dimer levels. Additionally, it is widely accepted to use exosome derived MSCs. The exosome properties provide protective paracrine effects without having to inject living cell; therefore it could prevent immunological adverse events.34,38
Another single-centered, open-label pilot study in Beijing, China, administered BMSCs into seven COVID-19 patients with various degrees of severity. One patient was categorized as critically ill, four with a severe condition, and two had mild symptoms. They injected 106 cells/kg BMSCs intravenously and followed them for 14 days. Neither toxicity or allergy, nor other adverse events were reported, and the patients displayed clinical improvement of their pulmonary function and symptoms after 2-4 days.49 Along with this study, Rogers et al. showed that infused MSCs did not interact with the ACE2 receptor and TMPRSS2, which implied that MSCs would not associate with SARS-CoV-2.29
A 65-year-old female critically ill COVID-19 patient indicated a good clinical remission after MSCs treatment.50 After antiviral and glucocorticoid management failed to show any improvement, she received UC-MSCs (5 x 107 cells) intravenously. After the second administration, neutrophil count decreased, lymphocytes increased as well as CD3+T cell, CD4+T cell, and CD8+T cell back to normal. On the CT scan findings, it was reported that the pneumonia imaging greatly improved, and she was finally released from the hospital with a negative swab test. This finding suggested that MSCs could improve patient outcomes even in elderly. A meta-analysis revealed that MSCs treatment did decrease the mortality rate in COVID-19 patients.51 From these reported cases, there were notable improvements in lung compliance and tidal volume in COVID-19-induced ARDS treated with MSCs.
Limitations in MSCs therapy
Before resolving the use of MSCs for the recommended therapy, several things need to be acknowledged. Stem cells therapy is a complicated one, and there are cases where unwanted side effects did occur. Even though MSCs are relatively safe, a study reported immunosuppression in some patients with injured lungs, causing secondary infection.52 A similar case was also described in patients receiving MSCs as immunosuppressive after having hematopoietic stem cell transplantation.53 More in-depth research in utilizing MSCs is needed to prevent unwanted differentiation of MSCs in local engrafted setting. Lastly, despite the positive impact of the paracrine and endocrine mechanism by MSCs, they may stimulate proangiogenic factors (VEGF, HGF, angiopoietin-1, platelet-derived growth factor, and placental growth factor) which is in line with augmenting tumor growth.28,52,53 Long term use of MSCs could also cause the production of allo-antibodies, while single use of MSCs are harmless and did not cause any dangerous immune response.28 More trials are necessary to know the side effects that MSCs may carry.
Conclusion and recommendation
In conclusion, although there is no standardized therapy for SARS Co-V2, MSC is a promising alternative treatment. Several studies, both pre-clinical and early clinical, have provided tantalizing clues that MSCs can provide a consistent therapeutic benefit. Moreover, the majority of previous results confirmed that MSCs are capable of dampening the over-reactivity inflammation cascade, decreasing infection, improving lung recovery, and increase the survival rate. It may take several months even years to develop a vaccine, and even if it's effective, it will not completely eradicate the ongoing infection. Further clinical trials regarding MSCs-based therapies in ARDS are urgently needed, including investigation regarding its safety.
Conflict of interest
No funding was used for the preparation of this review.
Authors’ contribution
DN: concept, literature search, manuscript writing, figure illustration
NAK: concept, literature search, manuscript editing
RY: manuscript editing
AP: bibliography editing
HBH: concept, manuscript editing
References
- Peta Sebaran | Gugus Tugas Percepatan Penanganan COVID-19 [Internet]. [cited 2020 Aug 7]. Available from: https://covid19.go.id/peta-sebaran
- Djalante R, Lassa J, Setiamarga D, Sudjatma A, Indrawan M, Haryanto B, et al. Review and analysis of current responses to COVID-19 in Indonesia: Period of January to March 2020. Prog Disaster Sci. 2020;6:100091. [Free Full Text] DOI: 1016/j.pdisas.2020.100091
- Setiati S, Azwar MK. COVID-19 and Indonesia. Acta Med Indones. 2020;52(1):84–89. [PubMed] [Free Fulltext]
- COVID-19 developments in Indonesia [Internet]. [cited 2020 Aug 7]. Available from: https://indonesien.ahk.de/en/infocenter/news/news-details/covid-19-developments-in-indonesia
- Jakarta’s Makeshift Covid-19 Hospital Nears Limit of Capacity [Internet]. [cited 2020 Aug 7]. Available from: https://jakartaglobe.id/news/jakartas-makeshift-covid19-hospital-nears-limit-of-capacity
- Behnke J, Kremer S, Shahzad T, Chao C-M, Böttcher-Friebertshäuser E, Morty RE, et al. MSC Based Therapies—New Perspectives for the Injured Lung. J Clin Med. 2020;9(3):682. [PubMed] [Free Full Text] DOI: 3390/jcm9030682
- Zakrzewski W, Dobrzyński M, Szymonowicz M, Rybak Z. Stem cells: Past, present, and future. Stem Cell Res Ther. 2019;10(1):1–22. [PubMed] [Free Full Text] DOI: 1186/s13287-019-1165-5
- Golchin A, Seyedjafari E, Ardeshirylajimi A. Mesenchymal Stem Cell Therapy for COVID-19: Present or Future. Stem Cell Rev Reports. 2020;16(3):427–33. [PubMed] [Free Full Text] DOI: 1007/s12015-020-09973-w
- Su S, Wong G, Shi W, Liu J, Lai ACK, Zhou J, et al. Epidemiology , Genetic Recombination , and Pathogenesis of Coronaviruses. Trends Microbiol. 2016;xx:1–13. [PubMed] [Free Full Text] DOI: 1016/j.tim.2016.03.003
- Fehr AR, Perlman S. Coronaviruses: An Overview of Their Replication and Pathogenesis. Method Mol Biol. 2015;1282(1):1–23. [PubMed] [Free Full Text] DOI: 1007/978-1-4939-2438-7_1
- Li X, Geng M, Peng Y, Meng L, Lu S. Molecular immune pathogenesis and diagnosis of COVID-19. J Pharm Anal. 2020;10(2):102–8. [PubMed] [Free Full Text] DOI: 1016/j.jpha.2020.03.001
- Yuki K, Fujiogi M, Koutsogiannaki S. COVID-19 pathophysiology: A review. Clin Immunol. 2020;215:108427. [Free Full Text] DOI:1016/j.clim.2020.108427
- Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W, et al. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses. 2020;12(4):372. [PubMed] [Free Full Text] DOI: 3390/v12040372
- Shang J, Wan Y, Luo C, Ye G, Geng Q, Auerbach A, et al. Cell entry mechanisms of SARS-CoV-2. 2020;2020:1–8. [PubMed] [Free Full Text] DOI: 1073/pnas.2003138117
- Bao L, Deng W, Gao H, Xiao C, Liu J, Xue J, et al. Lack of Reinfection in Rhesus Macaques Infected with SARS-CoV-2. bioRxiv. 2020;2020.03.13.990226. [Free Full Text] DOI: 1101/2020.03.13.990226
- Fu L, Wang B, Yuan T, Chen X, Ao Y. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J Infect. 2020;80:656-665. [PubMed] [Free Full Text] DOI: 1016/j.jinf.2020.03.041
- Zhang X, Cai H, Hu J, Lian J, Gu J, Zhang S, et al. Epidemiological, clinical characteristics of cases of SARS-CoV-2 infection with abnormal imaging findings. Int J Infect Dis. 2020 May;94:81–7. [PubMed] [Free Full Text] DOI: 1016/j.ijid.2020.03.040
- Immune-Based Therapy | Coronavirus Disease COVID-19 [Internet]. [cited 2020 Aug 17]. Available from: https://www.covid19treatmentguidelines.nih.gov/immune-based-therapy/
- Tu H, Tu S, Gao S, Shao A, Sheng J. Current epidemiological and clinical features of COVID-19 ; a global perspective from China. J Infect. 2020;81:1–9. [PubMed] [Free Full Text] DOI: 1016/j.jinf.2020.04.011
- Jean S-S, Lee P-I, Hsueh P-R. Treatment options for COVID-19: The reality annd challenges. J Microbiol Immunol Infect. 2020;53(3):436. [PubMed] [Free Full Text] DOI: 1016/j.jmii.2020.03.034
- Tobaiqy M, Qashqary M, Al-dahery S, Mujallad A, Hershan AA, Kamal MA, et al. Infection Prevention in Practice Therapeutic management of patients with COVID-19 : a systematic review. Infect Prev Pract. 2020;2(3):100061. [Free Full Text] DOI: 1016/j.infpip.2020.100061
- Sharma S, Basu S, Shetti NP, Aminabhavi TM. Current treatment protocol for COVID-19 in India. Sensors Int. 2020;1(June):100013. [Free Full Text] DOI: 1016/j.sintl.2020.100013
- Rojas M, Rodríguez Y, Monsalve DM, Acosta-Ampudia Y, Camacho B, Gallo JE, et al. Convalescent plasma in Covid-19: Possible mechanisms of action. Autoimmun Rev. 2020 Jul;19(7):102554. [PubMed] [Free Full Text] DOI: 1016/j.autrev.2020.102554
- Kolios G, Moodley Y. Introduction to Stem Cells and Regenerative Medicine. Respiration. 2013;85(1):3–10. [PubMed] [Free Full Text] DOI: 1159/000345615
- Ullah I, Subbarao RB, Rho GJ. Human mesenchymal stem cells - current trends and future prospective. Bioscience Reports. 2015;25(2):e00191. [PubMed] [Free Full Text] DOI: 1042/BSR20150025
- Williams AR, Hare JM. Mesenchymal Stem Cells: biology, pathophysiology, translational findings, and therapeutic implications for cardiac disease. Circ Res. 2011 Sep 30;109(8):923–40. [PubMed] [Free Full Text] DOI: 1161/CIRCRESAHA.111.243147
- Pittenger MF, Discher DE, Péault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. npj Regen Med. 2019;4(1). [Free full text] DOI: 1038/s41536-019-0083-6
- Musiał-Wysocka A, Kot M, Majka M. The Pros and Cons of Mesenchymal Stem Cell-Based Therapies. Cell Transplant. 2019 Jul 24;28(7):801–12. [PubMed] [Free full text]DOI: 10.1177/0963689719837897
- Rogers CJ, Harman RJ, Bunnell BA, Schreiber MA, Xiang C, Wang FS, et al. Rationale for the clinical use of adipose-derived mesenchymal stem cells for COVID-19 patients. J Transl Med. 2020;18(1):1–20. [Free full text] DOI: 1186/s12967-020-02380-2
- Walter J, Ware LB, Matthay MA. Mesenchymal stem cells: Mechanisms of potential therapeutic benefit in ARDS and sepsis. Lancet Respir Med. 2014;2(12):1016–26. [PubMed] DOI: 10.1016/S2213-2600(14)70217-6
- Murphy MB, Moncivais K, Caplan AI. Mesenchymal stem cells: Environmentally responsive therapeutics for regenerative medicine. Exp Mol Med. 2013;45(11):e54-16. [Free full text] DOI:1038/emm.2013.94
- Zou X, Zhang G, Cheng Z, Yin D, Du T, Ju G, et al. Microvesicles derived from human Wharton’s Jelly mesenchymal stromal cells ameliorate renal ischemia-reperfusion injury in rats by suppressing CX3CL1. Stem Cell Res Ther. 2014;5(2):1–13. [PubMed] [Free full text] DOI: 1186/scrt428
- Tripathi S, Tecle T, Verma A, Crouch E, White M, Hartshorn KL. The human cathelicidin LL-37 inhibits influenza a viruses through a mechanism distinct from that of surfactant protein d or defensins. J Gen Virol. 2013;94(PART11):40–9. [PubMed] [Free full text] DOI: 1099/vir.0.045013-0
- Abraham A, Krasnodembskaya A. Mesenchymal stem cell-derived extracellular vesicles for the treatment of acute respiratory distress syndrome. Stem Cells Transl Med. 2020;9(1):28–38. [PubMed] [Free full text]DOI: 10.1002/sctm.19-020510.1002%2Fsctm.19-0205
- Parekkadan B, Milwid JM. Mesenchymal stem cells as therapeutics. Annu Rev Biomed Eng. 2010;12:87–117. DOI: 1146/annurev-bioeng-070909-105309
- Sung DK, Chang YS, Sung SI, Yoo HS, Ahn SY, Park WS. Anti-bacterial effect of mesenchymal stem cells against Escherichia coli is mediated by secretion of beta- defensin- 2 via toll- like receptor 4 signalling. Cell Microbiol. 2016;18(3):424–36. [PubMed] [Free full text] DOI: 1111/cmi.12522
- Li F, Karlsson H. Antiviral Effect of IDO in Mouse Fibroblast Cells During Influenza Virus Infection. Viral Immunol. 2017;30(7):542–4. DOI: 1089/vim.2016.0140
- Khoury M, Khoury M, Cuenca J, Cuenca J, Cruz FF, Cruz FF, et al. Current status of cell-based therapies for respiratory virus infections: Applicability to COVID-19. Eur Respir J. 2020;55(6). [PubMed] [Free full text] DOI: 1183/13993003.00858-2020
- Wu X, Dao Thi VL, Huang Y, Billerbeck E, Saha D, Hoffmann HH, et al. Intrinsic Immunity Shapes Viral Resistance of Stem Cells. Cell. 2018; [PubMed] [Free full text] DOI: 1016/j.cell.2017.11.018
- Matthay MA, Zemans RL, Zimmerman GA, Arabi YM, Beitler JR, Mercat A, et al. Acute respiratory distress syndrome. Nat Rev Dis Prim. 2018; [PubMed] [Free full text] DOI: 1038/s41572-019-0069-0
- Zheng G, Huang L, Tong H, Shu Q, Hu Y, Ge M, et al. Treatment of acute respiratory distress syndrome with allogeneic adipose-derived mesenchymal stem cells: A randomized, placebo-controlled pilot study. Respir Res. 2014;15(1):1–10. [PubMed] [Free full text] DOI:1186/1465-9921-15-39
- Xiaobo Yang, Yuan Yu, Jiqian Xu, Huaqing Shu, Jia’an Xia, Hong Liu, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020; [Free full text] DOI:1016/S2213-2600(20)30079-5
- McIntyre LA, Moher D, Fergusson DA, Sullivan KJ, Mei SHJ, Lalu M, et al. Efficacy of mesenchymal stromal cell therapy for acute lung injury in preclinical animal models: A systematic review. PLoS One. 2016;11(1):1–16. [PubMed] [Free full text] DOI: 1371/journal.pone.0147170
- Galstian GM, Parovichnikova EN, Makarova PM, Kuzmina LA, Troitskaya V V., Gemdzhian E, et al. The Results of the Russian Clinical Trial of Mesenchymal Stromal Cells (MSCs) in Severe Neutropenic Patients (pts) with Septic Shock (SS) (RUMCESS trial). Blood. 2015; DOI: 1182/blood.V126.23.2220.2220
- Simonson OE, Mougiakakos D, Heldring N, Bassi G, Johansson HJ, Dalén M, et al. In Vivo Effects of Mesenchymal Stromal Cells in Two Patients With Severe Acute Respiratory Distress Syndrome. Stem Cells Transl Med. 2015;1199–213. [PubMed] [Free full text] DOI: 5966/sctm.2015-0021
- Zhao Q, Ren H, Han Z. Mesenchymal stem cells : Immunomodulatory capability and clinical potential in immune diseases. J Cell Immunother. 2016;2(1):3–20. DOI: 10.1016/j.jocit.2014.12.001
- Yen BL, Yen ML, Wang LT, Liu KJ, Sytwu HK. Current status of mesenchymal stem cell therapy for immune/inflammatory lung disorders: Gleaning insights for possible use in COVID-19. Stem Cells Transl Med. 2020;1–12. DOI: 1002/sctm.20-0186
- Sengupta V, Sengupta S, Lazo A, Woods P, Nolan A, Bremer N. Exosomes Derived from Bone Marrow Mesenchymal Stem Cells as Treatment for Severe COVID-19. Stem Cells Dev. 2020;29(12):747–54. DOI: 1089/scd.2020.0080
- Leng Z, Zhu R, Hou W, Feng Y, Yang Y, Han Q, et al. Transplantation of ACE2- Mesenchymal stem cells improves the outcome of patients with covid-19 pneumonia. Aging Dis. 2020;11(2):216–28. DOI: 14336/AD.2020.0228
- Liang B, Chen J, Wu H, Yang W, Li Y, Li J, et al. Clinical remission of a critically ill COVID-19 patient treated by human umbilical cord mesenchymal stem cells. Medicine. 2020;16(49):9179–85. [PubMed] DOI: 10.1097/MD.0000000000021429
- Qu W, Wang Z, Hare JM, Bu G, Mallea JM, Pascual JM, et al. Cell-based therapy to reduce mortality from COVID-19: Systematic review and meta-analysis of human studies on acute respiratory distress syndrome. Stem Cells Transl Med. 2020;1–16. [PubMed] [Free full text] DOI: 1002/sctm.20-0146
- Harrell CR, Sadikot R, Pascual J, Fellabaum C, Jankovic MG, Jovicic N, et al. Mesenchymal Stem Cell-Based Therapy of Inflammatory Lung Diseases: Current Understanding and Future Perspectives. Stem Cells Int. 2019;2019. [PubMed] [Free full text] DOI: 1155/2019/4236973
- Lukomska B, Stanaszek L, Zuba-Surma E, Legosz P, Sarzynska S, Drela K. Challenges and Controversies in Human Mesenchymal Stem Cell Therapy. Stem Cells Int. 2019;2019. DOI: 1155/2019/9628536