Nasser Ali Malik*1,
Amjid Hammodi2,
Dayanidhi Ramachandra Jaiswara3
1General Physician, Attock, (Pakistan)
2Orthopedic Surgeon, Baghdad, (Iraq)
3Orthopedic Surgeon, Shiroi, (India)
Correspondence:
Nasser Ali Malik, MBBS, General Physician, Attock, (Pakistan);
E-mail: doc.malik14@gmail.com; phone: +923340000203
Received: 29 March 2020;
Reviewed & Accepted: 5 April 2020
ABSTRACT
Background: The outbreak caused by SARS CoV-2 of the recent coronavirus disease-2019 (COVID-19) has been marked as a public health concern with a significant mortality at the global level. Lignocaine a common anesthetic agent being used for pain free surgeries for over a long period of time has expressed extensive characteristic of being an anti-inflammatory, antibacterial, direct spasmolytic, ion channel blocking and repolarization agent. We did a literature review
Methodology: Currently compiled over-view has for the first time evaluated the probable curative and therapeutic role of nebulized lignocaine drug against SARS CoV-2 by utilization of PubMed, MEDLINE, NHS Evidence and Web of Science databases.
Results: With evidence of nebulized lignocaine being used successfully in respiratory illness before and the established role of low concentration lignocaine as ion channel repolarization agent, we try to interpret and deduce the possible implication of nebulized lignocaine as possible therapeutic agent and a potential cure against SARS-CoV-2 caused respiratory illness by acting as an anti-inflammatory agent during SARS-CoV-2 caused acute lung injury and also possibly as an antiviral drug.
Conclusion: By the virtue of possessing anti-inflammatory effect and potential antiviral effects, nebulized lignocaine can be a breakthrough in the management of the current COVID-19 pandemic.
Key words: Lignocaine; Nebulized lignocaine; Respiratory illness; Severe Acute Respiratory Syndrome; SARS CoV; COVID-19; ion-channels
Citation: Malik NA, Lignocaine’s substantial role in COVID-19 management: potential remedial and therapeutic implications. Anaesth. pain & intensive care 2019;23(1):84-91
INTRODUCTION
Coronavirus disease-2019 (COVID-19) is an infectious disease that causes pneumonia. COVID-19 is third documented transfer of animal coronavirus to human in only two decades leading to an epidemic. The epidemic of COVID-19 begin in December, 2019 in Wuhan, capital city of Hubei Province, Peoples Republic of China and by now is declared as global pandemic infecting over half a million people worldwide in more than 180 countries and causing deaths of more than 20,000 people according to latest figures by World Health Organization (WHO). COVID-19 is caused by novel corona virus previously known as (2019nCoV by WHO), now known to the world as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). 1-3
SARS-CoV-2 is a virus of the same coronavirus family belonging to the Middle East Respiratory Syndrome (MERS-2012) and Severe Acute Respirator Syndrome (SARS-2007) epidemics. SARS-CoV-2 is quite similar to SARS-CoV but with few structural differences.3 SARS-CoV-2 has a broader clinical spectrum, the infection caused by it is asymptomatic at times, or a mild upper respiratory tract illness to severe viral pneumonia causing Acute Lung Injury (ALI) leading to Acute Respiratory Distress Syndrome (ARDS) and eventually respiratory failure and death.2 The frequent complications of COVID-19 include ALI, ARDS, sepsis, respiratory failure and heart failure.
SARS-CoV-2 AND ION CHANNELS
When virus enters host’s system, there is an already diversify ionic activities by the host cell suitable for viral proteins. Viral proteins target these ionic channels and form viroporin.4 Viroporins play a vital role in virus-cycle propagation and they also prompt the expression viral pathogeneses.4 The frequency of Na+ intake and Cl- discharge regulate the presence of fluid on covering the respiratory surfaces of lungs.5,6 Almost all of the respiratory viruses cause viral pathogenesis by inhibiting the amiloride-sensitive epithelial Na+ Channel (ENaC). Influenza A virus (IAV) inhibits ENaC thus disrupting the NA+ absorption of the epithelial layer leading to inflammation and edema across the epithelial layer of the lung.7-9 Respiratory Syncytial Virus (RSV) infections follows the same process of virulence as of IAV.
Severe acute respiratory corona virus protein E and S considerably disrupt the expression of ENaC protein and hence decreasing the channel activity.4,8 Severe acute respiratory syndrome coronavirus share a similarity with IAV by inhibiting protein kinase C (PKC) and increase the excitability ENaC, leading to inflammation of the epithelial respiratory surface.4,9 It is noteworthy coronavirus E 0protein, via the regulation of Ca2+ transport, activate the NLRP3 inflammasome through their viroporin activity.
ARDS AND ION CHANNELS
COVID-19 ARDS proceed in a manner from an injury to the lung parenchyma due the viral pneumonia leading to ALI or ARDS and is the leading cause of morbidity and mortality. ARDS is an expeditiously progressive illness during which the inflammation is widespread and thus, leading to extensive pulmonary edema causing failure of exchange of gasses to eventual lung failure.10,11 The gasses exchange and fluid balance of lung alveoli is managed by apical amiloride-sensitive epithelial sodium channel (ENaC) and the amiloride-insensitive cyclic nucleotide-gated cation channel (CNG) acting together with the basolaterally located Na,K-ATPase (NKA) promote transcellular sodium transport. The ion channels modulation regulate alveolar fluid clearance (AFC).12 Alveolar fluid reabsorption is of importance in cardiac and non-cardiac injury.11,13,14 Any injury to lungs causes a disturbances in NA+ and Cl- transport across the membrane thus defectively upregulating ENaC activity in the airway epithelial cells. This cytokine and chemokine induced inflammation causes disruption in ion-channel functioning causing improper AFC thus, leading to accumulation of fluid across already inflamed lung epithelium causing eventual fibrosis.14-16 A novel way to approach ARDS can be by targeting Stretch Activating ion-channels (SAC) leading to regulation of ENaC.16,17
LIGNOCAINE
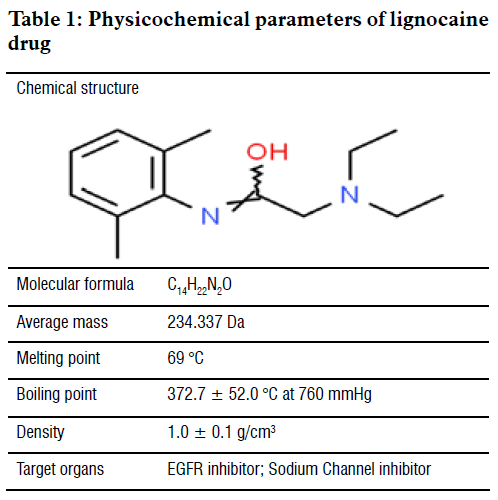
Lignocaine, the first amide base local anesthetic and class 1b antiarrhythmic drug, is an essential drug on the WHO essential drug list (Table 1). Lignocaine is most commonly used as either a local anesthesia or antiarrhythmic drug but besides these lignocaine has over the year has shown its potential as diverse drug, one with multiple effects.18 Over the year lignocaine has itself as potent anti-inflammatory medicine 19 and its anti-inflammatory properties are at par with Non-steroidal anti-inflammatory drugs or even steroids19,20 and even in long term respiratory illness,20-28 it is often considered as steroid sparring drug.
Lignocaine being an anti-euthymic drug is also a cardio-protective drug by blocking the sodium gated and repolarizing them, its anti-arrhythmic properties a very useful in arrhythmias after myocardial infarction or cardiac surgeries.29-31 Along with its ability as an anti-inflammatory drug, it also has a good anti-nociceptive and is been documented to reduce pain post-surgery or after any kind peripheral-neural block applied. Lignocaine also possess a wide range of in vitro and in vivo characteristic of being immune-modulator, anti-bacterial, and anti-cancer.32
LIGNOCAINE AND REPOLARIZING OF ION-CHANNELS
Lignocaine marked rank is being an anti-inflammatory drug but along with that, it is a very good analgesic.33 It’s being used as drug for pain modulation since ages. But the theory of local anesthetic in low dose having a better therapeutic effect was describe by Huneke Brothers in 1925.34 These effects often are exerted at dose lower than the dose required for a Na+ Channel Blockade.35-37 Until recently, in few case studies, about newly discovered anatomical points for long term management pain by admiration a simple lignocaine injection of low concentrations cleared the concept and mechanism that at low dose lignocaine acts by repolarization of depolarized ion channel in the disturbed area.38-41
NEBULIZED LIGNOCAINE
Among off-label frequent use of lignocaine is nebulized form.22,24,40,41 It has shown the ability to be very good anti-inflammatory agent by not just decreasing inflammation but also regulated mucus production and fibrosis in vitro and in vivo and also yields effective and quick results.13-28 There are also plenty study resource and clinical trials data show casing the positive steroid sparring effects of lignocaine in asthma or retractable cough.25,27,41 The systemic absorption of lignocaine in blood after nebulization is very low. Generally as compared to other routes of administrations, in case of nebulized lignocaine usually 100-200 mg for a single dose is considered safe range with a maximum of 600 mg tolerated. The concentration of lignocaine > 5mg/L is toxic and can lead to tremors, light-headedness, hallucinations or even cardiac arrest.25,40
DISCUSSION
In the light of the facts mentioned, there is strong evidence pointing towards the involvement of ion-channel regulation in the progression of COVID-19 and the potential role of lignocaine in its management. The evidences discussed here clearly show that viral propagation and replication is ion-channel dependent4,11 and the injury caused by the virus to the lung which starts from mild inflammation to ARDS causing pulmonary edema and fibrosis is also governed by cytokines and ion-channels interaction.13-17 It is also clear that lignocaine is a potent repolarizing agent when given in diluted low concentration dose.36-41 Therefore, after interpreting all the evidence and our clinical experiences, we suggest that nebulized lignocaine has potential to be used as a drug of choice against the current COVID-19.19 The following is the dose recommended: 5 mL of 0.6% lignocaine (achieved after diluting 1.5 mL of 2% lignocaine + 3.5 mL of distilled water ) given 6 hourly (4 times in 24 h) for the day of start of dry cough in suspected or diagnosed patient. The patient should be Nil per Oral for 45 minutes before and after the administration of Nebulized lignocaine. In few patients, the trials have shown lignocaine causes a brief bronchoconstriction, so it is recommended that the administration of the first dose should be monitored and if such episode occur a single dose of aerosol salbutamol42 before next session of nebulized lignocaine is enough. Along with these necessary precautions to inhibit aerosol transmission of SARS-COV-2 should also be taken and the nebulization should be done in a controlled environment.
CONCLUSION
Nebulized lignocaine can be a breakthrough in the management of the current COVID-19 pandemic bearing strong anti-inflammatory effect and potential antiviral agent. A clinical trial of the above theory can substantiate the above theory in this desperate time.
Conflict of interest: Nil declared by the authors
Authors’ contribution: All authors took part in conduct of the study, literature search and manuscript preparation and editing.
REFERENCES
Amjid Hammodi2,
Dayanidhi Ramachandra Jaiswara3
1General Physician, Attock, (Pakistan)
2Orthopedic Surgeon, Baghdad, (Iraq)
3Orthopedic Surgeon, Shiroi, (India)
Correspondence:
Nasser Ali Malik, MBBS, General Physician, Attock, (Pakistan);
E-mail: doc.malik14@gmail.com; phone: +923340000203
Received: 29 March 2020;
Reviewed & Accepted: 5 April 2020
ABSTRACT
Background: The outbreak caused by SARS CoV-2 of the recent coronavirus disease-2019 (COVID-19) has been marked as a public health concern with a significant mortality at the global level. Lignocaine a common anesthetic agent being used for pain free surgeries for over a long period of time has expressed extensive characteristic of being an anti-inflammatory, antibacterial, direct spasmolytic, ion channel blocking and repolarization agent. We did a literature review
Methodology: Currently compiled over-view has for the first time evaluated the probable curative and therapeutic role of nebulized lignocaine drug against SARS CoV-2 by utilization of PubMed, MEDLINE, NHS Evidence and Web of Science databases.
Results: With evidence of nebulized lignocaine being used successfully in respiratory illness before and the established role of low concentration lignocaine as ion channel repolarization agent, we try to interpret and deduce the possible implication of nebulized lignocaine as possible therapeutic agent and a potential cure against SARS-CoV-2 caused respiratory illness by acting as an anti-inflammatory agent during SARS-CoV-2 caused acute lung injury and also possibly as an antiviral drug.
Conclusion: By the virtue of possessing anti-inflammatory effect and potential antiviral effects, nebulized lignocaine can be a breakthrough in the management of the current COVID-19 pandemic.
Key words: Lignocaine; Nebulized lignocaine; Respiratory illness; Severe Acute Respiratory Syndrome; SARS CoV; COVID-19; ion-channels
Citation: Malik NA, Lignocaine’s substantial role in COVID-19 management: potential remedial and therapeutic implications. Anaesth. pain & intensive care 2019;23(1):84-91
INTRODUCTION
Coronavirus disease-2019 (COVID-19) is an infectious disease that causes pneumonia. COVID-19 is third documented transfer of animal coronavirus to human in only two decades leading to an epidemic. The epidemic of COVID-19 begin in December, 2019 in Wuhan, capital city of Hubei Province, Peoples Republic of China and by now is declared as global pandemic infecting over half a million people worldwide in more than 180 countries and causing deaths of more than 20,000 people according to latest figures by World Health Organization (WHO). COVID-19 is caused by novel corona virus previously known as (2019nCoV by WHO), now known to the world as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). 1-3
SARS-CoV-2 is a virus of the same coronavirus family belonging to the Middle East Respiratory Syndrome (MERS-2012) and Severe Acute Respirator Syndrome (SARS-2007) epidemics. SARS-CoV-2 is quite similar to SARS-CoV but with few structural differences.3 SARS-CoV-2 has a broader clinical spectrum, the infection caused by it is asymptomatic at times, or a mild upper respiratory tract illness to severe viral pneumonia causing Acute Lung Injury (ALI) leading to Acute Respiratory Distress Syndrome (ARDS) and eventually respiratory failure and death.2 The frequent complications of COVID-19 include ALI, ARDS, sepsis, respiratory failure and heart failure.
SARS-CoV-2 AND ION CHANNELS
When virus enters host’s system, there is an already diversify ionic activities by the host cell suitable for viral proteins. Viral proteins target these ionic channels and form viroporin.4 Viroporins play a vital role in virus-cycle propagation and they also prompt the expression viral pathogeneses.4 The frequency of Na+ intake and Cl- discharge regulate the presence of fluid on covering the respiratory surfaces of lungs.5,6 Almost all of the respiratory viruses cause viral pathogenesis by inhibiting the amiloride-sensitive epithelial Na+ Channel (ENaC). Influenza A virus (IAV) inhibits ENaC thus disrupting the NA+ absorption of the epithelial layer leading to inflammation and edema across the epithelial layer of the lung.7-9 Respiratory Syncytial Virus (RSV) infections follows the same process of virulence as of IAV.
Severe acute respiratory corona virus protein E and S considerably disrupt the expression of ENaC protein and hence decreasing the channel activity.4,8 Severe acute respiratory syndrome coronavirus share a similarity with IAV by inhibiting protein kinase C (PKC) and increase the excitability ENaC, leading to inflammation of the epithelial respiratory surface.4,9 It is noteworthy coronavirus E 0protein, via the regulation of Ca2+ transport, activate the NLRP3 inflammasome through their viroporin activity.
ARDS AND ION CHANNELS
COVID-19 ARDS proceed in a manner from an injury to the lung parenchyma due the viral pneumonia leading to ALI or ARDS and is the leading cause of morbidity and mortality. ARDS is an expeditiously progressive illness during which the inflammation is widespread and thus, leading to extensive pulmonary edema causing failure of exchange of gasses to eventual lung failure.10,11 The gasses exchange and fluid balance of lung alveoli is managed by apical amiloride-sensitive epithelial sodium channel (ENaC) and the amiloride-insensitive cyclic nucleotide-gated cation channel (CNG) acting together with the basolaterally located Na,K-ATPase (NKA) promote transcellular sodium transport. The ion channels modulation regulate alveolar fluid clearance (AFC).12 Alveolar fluid reabsorption is of importance in cardiac and non-cardiac injury.11,13,14 Any injury to lungs causes a disturbances in NA+ and Cl- transport across the membrane thus defectively upregulating ENaC activity in the airway epithelial cells. This cytokine and chemokine induced inflammation causes disruption in ion-channel functioning causing improper AFC thus, leading to accumulation of fluid across already inflamed lung epithelium causing eventual fibrosis.14-16 A novel way to approach ARDS can be by targeting Stretch Activating ion-channels (SAC) leading to regulation of ENaC.16,17
LIGNOCAINE
Lignocaine, the first amide base local anesthetic and class 1b antiarrhythmic drug, is an essential drug on the WHO essential drug list (Table 1). Lignocaine is most commonly used as either a local anesthesia or antiarrhythmic drug but besides these lignocaine has over the year has shown its potential as diverse drug, one with multiple effects.18 Over the year lignocaine has itself as potent anti-inflammatory medicine 19 and its anti-inflammatory properties are at par with Non-steroidal anti-inflammatory drugs or even steroids19,20 and even in long term respiratory illness,20-28 it is often considered as steroid sparring drug.
Lignocaine being an anti-euthymic drug is also a cardio-protective drug by blocking the sodium gated and repolarizing them, its anti-arrhythmic properties a very useful in arrhythmias after myocardial infarction or cardiac surgeries.29-31 Along with its ability as an anti-inflammatory drug, it also has a good anti-nociceptive and is been documented to reduce pain post-surgery or after any kind peripheral-neural block applied. Lignocaine also possess a wide range of in vitro and in vivo characteristic of being immune-modulator, anti-bacterial, and anti-cancer.32
LIGNOCAINE AND REPOLARIZING OF ION-CHANNELS
Lignocaine marked rank is being an anti-inflammatory drug but along with that, it is a very good analgesic.33 It’s being used as drug for pain modulation since ages. But the theory of local anesthetic in low dose having a better therapeutic effect was describe by Huneke Brothers in 1925.34 These effects often are exerted at dose lower than the dose required for a Na+ Channel Blockade.35-37 Until recently, in few case studies, about newly discovered anatomical points for long term management pain by admiration a simple lignocaine injection of low concentrations cleared the concept and mechanism that at low dose lignocaine acts by repolarization of depolarized ion channel in the disturbed area.38-41
NEBULIZED LIGNOCAINE
Among off-label frequent use of lignocaine is nebulized form.22,24,40,41 It has shown the ability to be very good anti-inflammatory agent by not just decreasing inflammation but also regulated mucus production and fibrosis in vitro and in vivo and also yields effective and quick results.13-28 There are also plenty study resource and clinical trials data show casing the positive steroid sparring effects of lignocaine in asthma or retractable cough.25,27,41 The systemic absorption of lignocaine in blood after nebulization is very low. Generally as compared to other routes of administrations, in case of nebulized lignocaine usually 100-200 mg for a single dose is considered safe range with a maximum of 600 mg tolerated. The concentration of lignocaine > 5mg/L is toxic and can lead to tremors, light-headedness, hallucinations or even cardiac arrest.25,40
DISCUSSION
In the light of the facts mentioned, there is strong evidence pointing towards the involvement of ion-channel regulation in the progression of COVID-19 and the potential role of lignocaine in its management. The evidences discussed here clearly show that viral propagation and replication is ion-channel dependent4,11 and the injury caused by the virus to the lung which starts from mild inflammation to ARDS causing pulmonary edema and fibrosis is also governed by cytokines and ion-channels interaction.13-17 It is also clear that lignocaine is a potent repolarizing agent when given in diluted low concentration dose.36-41 Therefore, after interpreting all the evidence and our clinical experiences, we suggest that nebulized lignocaine has potential to be used as a drug of choice against the current COVID-19.19 The following is the dose recommended: 5 mL of 0.6% lignocaine (achieved after diluting 1.5 mL of 2% lignocaine + 3.5 mL of distilled water ) given 6 hourly (4 times in 24 h) for the day of start of dry cough in suspected or diagnosed patient. The patient should be Nil per Oral for 45 minutes before and after the administration of Nebulized lignocaine. In few patients, the trials have shown lignocaine causes a brief bronchoconstriction, so it is recommended that the administration of the first dose should be monitored and if such episode occur a single dose of aerosol salbutamol42 before next session of nebulized lignocaine is enough. Along with these necessary precautions to inhibit aerosol transmission of SARS-COV-2 should also be taken and the nebulization should be done in a controlled environment.
CONCLUSION
Nebulized lignocaine can be a breakthrough in the management of the current COVID-19 pandemic bearing strong anti-inflammatory effect and potential antiviral agent. A clinical trial of the above theory can substantiate the above theory in this desperate time.
Conflict of interest: Nil declared by the authors
Authors’ contribution: All authors took part in conduct of the study, literature search and manuscript preparation and editing.
REFERENCES
- Wu A, Peng Y, Huang B, Ding X, Wang X, Niu P, Meng J, Zhu Z, Zhang Z, Wang J, & Sheng J. Genome composition and divergence of the novel coronavirus (2019-nCoV) originating in China. Cell Host Microbe 2020;27(3):325–328.
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, & Guan L. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020;395(10229):1054 – 1062.
- Gorbalenya AE, Baker SC, Baric RS, de Groot RJ, Drosten C, Gulyaeva AA, Haagmans BL, Lauber C, Leontovich AM, Neuman BW, & Penzar D. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Micro 2020;5:536–544.
- Hover S, Foster B, Barr JN, & Mankouri J. Viral dependence on cellular ion channels - an emerging anti-viral target?. J Gen Virol 2017;98(3):345–351.
- O'Grady SM, & Lee SY. Chloride and potassium channel function in alveolar epithelial cells. Am J Physiol Lung Cell Mol Physiol 2003;284(5):L689–L700.
- Aguilar JS, Criado M, & De Robertis E. Inhibition by local anesthetics, phentolamine and propranolol of [3H]quinuclydinyl benzylate binding to central muscarinic receptors. Eur J Pharmacol 1980;68(3):317–326.
- Kunzelmann K, Beesley AH, King NJ, Karupiah G, Young JA, & Cook DI. Influenza virus inhibits amiloride-sensitive Na+ channels in respiratory epithelia. Proc Natl Acad Sci USA. 2000;97(18):10282–10287.
- Ji HL, Song W, Gao Z, Su XF, Nie HG, Jiang Y, Peng JB, He YX, Liao Y, Zhou YJ, & Tousson A. SARS-CoV proteins decrease levels and activity of human ENaC via activation of distinct PKC isoforms. Am J Physiol Lung Cell Mol Physiol 2009;296(3):L372–L383.
- Verdiá-Báguena C, Nieto-Torres JL, Alcaraz A, Dediego ML, Enjuanes L, & Aguilella VM. Analysis of SARS-CoV E protein ion channel activity by tuning the protein and lipid charge. Biochim Biophys Acta 2013;1828(9):2026–2031.
- Surya W, Li Y, Verdià-Bàguena C, Aguilella VM, & Torres J. MERS coronavirus envelope protein has a single transmembrane domain that forms pentameric ion channels. Virus Res 2015;201:61–66.
- Nieto-Torres JL, Verdiá-Báguena C, Castaño-Rodriguez C, Aguilella VM, & Enjuanes L. Relevance of Viroporin Ion Channel Activity on Viral Replication and Pathogenesis. Viruses 2015;7(7):3552–3573.
- Donahoe M. Acute respiratory distress syndrome: A clinical review. Pulm Circ 2011;1(2):192–211.
- Hamacher J, Hadizamani Y, Borgmann M, Mohaupt M, Männel DN, Moehrlen U, Lucas R, & Stammberger U. Cytokine–ion Channel interactions in Pulmonary inflammation. Front Immunol 2018;8:1644.
- Matalon S, Bartoszewski R, & Collawn JF. Role of epithelial sodium channels in the regulation of lung fluid homeostasis. Am J Physiol Lung Cell Mol Physiol 2015;309(11):L1229–L1238.
- Peteranderl C, Sznajder JI, Herold S, & Lecuona E. Inflammatory Responses Regulating Alveolar Ion Transport during Pulmonary Infections. Front Immunol 2017;8:446.
- Wynne BM, Zou L, Linck V, Hoover RS, Ma HP, & Eaton DC. Regulation of Lung Epithelial Sodium Channels by Cytokines and Chemokines. Front Immunol 2017;8:766.
- Schwingshackl A. The role of stretch-activated ion channels in acute respiratory distress syndrome: finally a new target?. Am J Physiol Lung Cell Mol Physiol 2016;311(3):L639–L652.
- Weinberg L, Peake B, Tan C, & Nikfarjam M. Pharmacokinetics and pharmacodynamics of lignocaine: A review. World J Anesthesiol 2015;4(2):17-29.
- Cassuto J, Sinclair R, & Bonderovic M. Anti-inflammatory properties of local anesthetics and their present and potential clinical implications. Acta Anaesthesiol Scand 2006;50(3):265–282.
- Wickström K, Stavréus-Evers A, Vercauteren O, Olovsson M, Edelstam G. Effect of Lignocaine on IL-6, IL-8, and MCP-1 in Peritoneal Macrophages and Endometriotic Stromal Cells. Reprod Sci 2017;24(3):382–392.
- Özyiğit LP, Erer A, Okumuş G, Çağatay T, Kıyan E, & Erkan F. Nebulized Lidocaine as an Alternative Therapy for Reactive Airway Dysfunction Syndrome. Turk Thorac J 2016;17(2):82-83.
- Lv ZM, Chen L, & Tang J. Nebulized lidocaine inhalation in the treatment of patients with acute asthma. World J Emerg Med 2011;2(1):30-2.
- Slaton RM, Thomas RH, & Mbathi JW. Evidence for therapeutic uses of nebulized lidocaine in the treatment of intractable cough and asthma. Ann Pharmacother 2013;47(4):578–585.
- Shirk MB, Donahue KR, & Shirvani J. Unlabeled uses of nebulized medications. Am J Health Syst Pharm 2006;63(18):1704–1716.
- Lim KG, Rank MA, Hahn PY, Keogh KA, Morgenthaler TI, & Olson EJ. Long-term safety of nebulized lidocaine for adults with difficult-to-control chronic cough: a case series. Chest 2013;143(4):1060–1065.
- Serra MF, Anjos-Valotta EA, Olsen PC, Couto GC, Jurgilas PB, Cotias AC, Pão CR, Ferreira TP, Arantes AC, Pires AL, & Cordeiro RS. Nebulized lidocaine prevents airway inflammation, peribronchial fibrosis, and mucus production in a murine model of asthma. Anesthesiol 2012;117(3):580–591.
- Harrison TW, & Tattersfield AE. Effect of single doses of inhaled lignocaine on FEV1 and bronchial reactivity in asthma. Respir Med 1998;92(12):1359–1363.
- Constantino RT, Crockett SE, Vasko JS. Cardiovascular Effects of Lidocaine. Annals Thorac Surg 1969;8(5):425-436,
- Lee EH, Lee HM, Chung CH, Chin JH, Choi DK, Chung HJ, Sim JY, & Choi IC. Impact of intravenous lidocaine on myocardial injury after off-pump coronary artery surgery. Br J Anaesth 2011;106(4):487–493.
- Spracklen FH, Kimerling JJ, Besterman EM, & Litchfield JW. Use of lignocaine in treatment of cardiac arrhythmias. Br Med J 1968;1(5584):89-91.
- Müller-Edenborn B, Kania G, Osto E, Jakob P, Krasniqi N, Beck-Schimmer B, Blyszczuk P, & Eriksson U. Lidocaine Enhances Contractile Function of Ischemic Myocardial Regions in Mouse Model of Sustained Myocardial Ischemia. PLoS One. 2016;11(5):e0154699.
- Atlas of Neural Therapy: With Local Anesthetics 3rd Edition by Mathias Dosch ISBN-13: 978-3131305732.
- Kuo CP, Jao SW, Chen KM, Wong CS, Yeh CC, Sheen MJ, & Wu CT. Comparison of the effects of thoracic epidural analgesia and i.v. infusion with lidocaine on cytokine response, postoperative pain and bowel function in patients undergoing colonic surgery. Br J Anaesth 2006;97(5):640–646.
- Aguilar JS, Criado M, & De Robertis E. Inhibition by local anesthetics, phentolamine and propranolol of [3H]quinuclydinyl benzylate binding to central muscarinic receptors. Eur J Pharmacol 1980;68(3):317–326.
- Rimbäck G, Cassuto J, Wallin G, & Westlander G. Inhibition of peritonitis by amide local anesthetics. Anesthesiol 1988;69(6):881–886.
- Hammodi A. Anatomical gates for pain relief due to cervical and lumbar disc disease. Anaesth Pain Inten Care 2019;23(2):217-220.
- Hammodi, A. Coccydynia relieved by a tarsal tunnel block: a case series. J Med Case Reports 2019:13:339.
- Hammodi A. A Case Series of Cervical Disc Disease Pain Relieved by New Five Injection Spots of Lignocaine (The Anatomical Gates of Sodium Channels Blockers of the Upper Limbs). EC Orthopaed 2020;11(4):06-17.
- Hammodi A. Temporomandibular Disorders (TMDs): A New Hypothesis. EC Orthopaed 2019;10(9):698-702.
- Ruchika N. Lidocaine -An Old Drug for New Indication. J Int Pharm Sci Drug Res 2013;5:84-87.
- Burburan SM, Xisto DG, & Rocco PR. Anaesthetic management in asthma. Minerva Anestesiol 2007;73(6):357–365.
- Groeben H, Silvanus MT, Beste M, & Peters J. Combined lidocaine and salbutamol inhalation for airway anesthesia markedly protects against reflex bronchoconstriction. Chest 2000;118(2):509–515