Kjetil Larsen, CES, George C. Chang Chien, DO2
Corrective Exercise Specialist, Training & Rehabilitation, Oslo Norway
2 Director of Pain Management, Ventura County Medical Center, CA USA
Correspondence: Kjetil Larsen, CES, Corrective Exercise Specialist, Training & Rehabilitation, Oslo Norway; Kjetil@trainingandrehabilitation.com; Tel.: +47 975 45 192
Background: Lumbosacral plexus entrapment syndrome (LPES) is a little-known but common cause of chronic lumbopelvic and lower extremity pain. The authors document the clinical course of 61 patients who were diagnosed and treated for LPES between May 2016 and October 2018. The study is aimed to evaluate the efficacy of our proposed diagnostic and conservative treatment protocol for LPES, clinically.
Methodology: This is a retrospective cohort study of patients suffering from LPES. Patients were included in this study if they compatible symptoms with LPES with symptoms of low back, pelvic, groin, genital, thigh or calf pain after other more common etiologies have been excluded. Additionally, these patients had at least 5 positive provocative Tinel’s tests applied to various lumbopelvic and lower extremity (LPLE) nerve branches yielding => 7 (numeric rating scale) NRS, and weakness of one or more myotomes of the lower body. The group in its entirety was treated with gentle strengthening of the psoas major and piriformis muscles. The primary outcome measure was patient reported satisfaction and improvement including: Full, significant, moderate, slight, or no improvement in pain and symptoms. Patients were followed for up to two years.
Results: The most common complaints amongst the patient pool were low back, groin, pelvic, posterior/lateral calf pain. Additionally, 17 patients (28%) stated that everything in the LPLE hurts, consistent with plexalgia. 13 patients were lost to follow-up as they did not reschedule treatment, for unknown reasons. Amongst the remaining 48 patients, 25 recovered fully (52%), 12 significantly (25%), and five moderately (10,4%). Five patients had a slight improvement (10,4%), and two no improvement whatsoever (4%). The average recovery times were mostly consistent with the time of affliction. Patients with a symptom duration of less than one year, generally recovered within 4 months. One to four years, within 10,5 months. Five to nine years, 7,5 months. And, finally, more than 10 years, within 18 months.
Conclusion: Non-specific pain syndromes in the LPLE where other causes have been excluded, may be attributable to underlying LPES. In this study, a high correlation between the diagnostic & interventional protocols, and beneficial patient outcomes were demonstrated. However, more statistical and long-term research is needed.
Keywords: Pelvic girdle pain; Lumbosacral plexus entrapment syndrome; Piriformis syndrome; Nerve entrapment; Double-crush; Chronic pain; Fibromyalgia
Citation: Larsen K, Chien GCC. Lumbosacral plexus entrapment syndrome, Part two: Symptomology and rehabilitative trials. Anaesth pain & intensiv care 2019;23(2):138-144
Received: 28 February 2019, Reviewed & Accepted: 29 May 2019
INTRODUCTION
As we aimed do demonstrate in this article series’ first part,1 lumbosacral plexus entrapment syndrome (LPES) is a problem in which the lumbar and sacral plexuses become entrapped within the psoas major and by the piriformis muscles due to severe weakness or myotrauma, often resulting in diffuse pain “syndromes” in the lumbopelvic and lower extremity (LPLE) regions. The nature of LPES is similar to that of thoracic outlet syndrome (TOS), often mimicking other, peripheral etiologies of pain which may easily be misinterpreted as unrelated the pathology at hand, such as fibromyalgia.1-4
The primary purpose of this trial was to establish whether or not an association between the inclusive diagnostic criteria outlined in this article series’ first part, as well as the proposed strengthening protocols for the psoas major, piriformis and pectineus muscles, were also associated with factual patient recovery. This, both to to assess the specificity of the diagnostic criteria as well as the strengthening protocol’s efficacy in the detection and treatment of LPES. Secondary objectives were to document the prevalence of symptom locations and durations, as well as average rehabilitation time until recovery.
METHODOLOGY
In the time between May 2016 and October 2018, 61 patients whose symptoms and physical examination were compatible with LPES, were diagnosed and followed up at the first author’s [private] clinic. The patients were diagnosed with LPES based on their symptoms and the diagnostic criteria proposed and elaborated upon in the first part of this article series: Non-specific symptoms consistent with LPLE neuroanatomy, usually presenting as diffuse low back, pelvic, groin, genital, thigh or calf pain after other, more common etiologies have been excluded. At least 5 positive provocative Tinel’s tests applied to various LPLE nerve branches yielding => 7 (numeric rating scale) NRS, and weakness of one or more myotomes of the lower body. And, finally, exacerbation of pain after initiation of the proposed rehabilitative exercises in the LPLE in the patients who had greater initial morbidity, usually those with a symptom duration of more than one year’s length. Other potential causes of their pains had already either been attempted treated and found ineffective, or was excluded both by either the author or prior clinicians. 59 of 61 patients (97%) had tried other forms of treatment without experiencing significant improvement, prior to visiting the author’s clinic.
There were 30 men and 31 women, whose ages span between 16 and 62 years. Out of the total of 61 patients, 54 patients were employed, 4 on sick-leave for <= 1 year, and 3 patients were on disability as shown in Figure 1. Their symptom locations and duration, as well as average recovery times were registered. In calculating outcomes, patients who fully recovered would count as “1”, whereas significant recovery counts as “0,75”, moderate recovery as “0,5”, slight recovery as “0,25” and, finally, no improvement as “0”. The primary outcome measure was patient reported satisfaction and improvement including: Full, significant, moderate, slight, or no improvement in pain and symptoms. Patients were followed for up to two years
The patients were taught strengthening exercises for the psoas major and piriformis, and to regulate down or up in accordance with the aftermath symptoms. The patients were required to perform the exercises with appropriate technique, to demonstrate the muscles’ impairment. Symptom reproduction 1-2 weeks post exercising was considered confirmatory in the patients with a higher degree of morbidity, but was optional for those with lesser initial morbidity, generally the patients with symptom duration of less than one year, and whose symptoms were not solely related to athletic activities. Five to fifteen repetitions, one to two working sets, one to three times per week were the most common volumes used. Patients with significant morbidity would [initially] be prescribed as little as 3-5 repetitions twice per week, in order to avoid severe symptom flare-up.
RESULTS
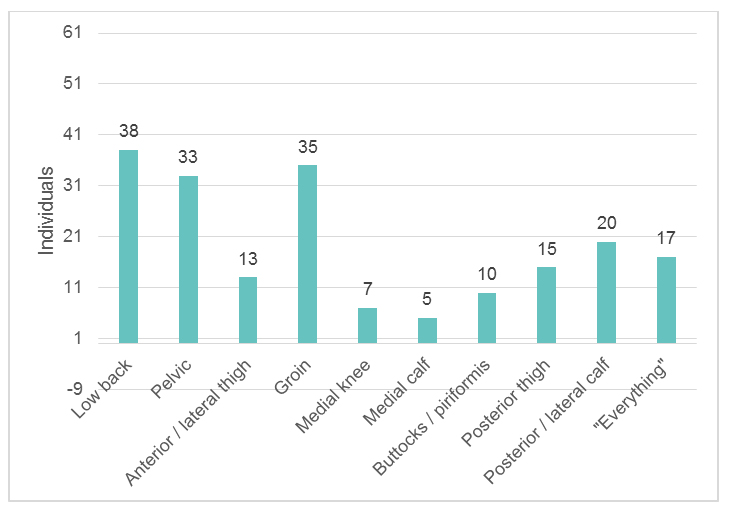
Amongst the 61 patients, long-term suffering was common, as 57 of 61 patients had been afflicted for => 1 year. 1-4 years; 31 patients. 5-9 years; 14 patients. More than ten years; 12 patients. 3-5 months; 3 patients. And, finally, 6-11 months; 1 patient. With regards to symptomology, the most common (dominant) complaints were low back (38 patients), groin (35 patients) and pelvic (33 patients) pain, which affected more than half of the patients (see Figure 2). Of lesser prevalence were posterior and lateral calf (20 patients), posterior thigh (15 patients), anterior thigh (13), buttock/piriformis (10), medial knee (7) and medial calf (5) patients. 17 patients reported that “everything” in the LPLE ached.
Figure 1: Symptom duration prevalence
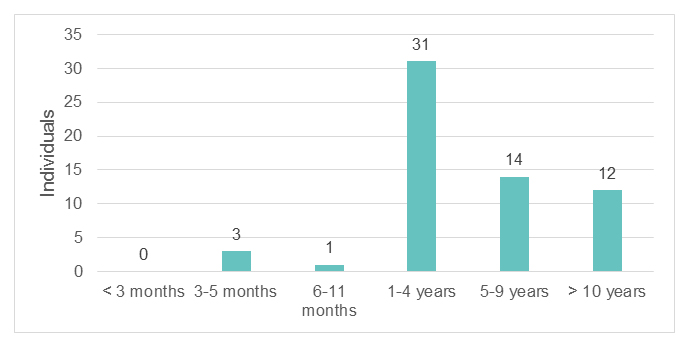
Figure 2: Symptom location prevalence
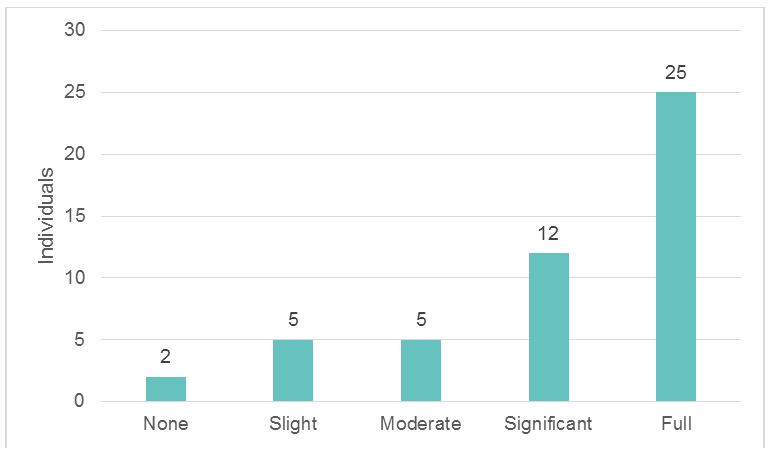
During the period in question, 13 patients stopped rescheduling follow-up sessions, for unknown reasons, and were thus excluded from the treatment outcome results (Figures 4-5). Amongst the remaining 48 patients, 25 patients (52%) fully recovered, 12 patients (25%) significantly recovered, 5 patients (10,4%) moderately recovered, 5 patients (10,4%) slightly recovered, and two patients (4,16%) did not improve whatsoever. By using the prior-mentioned variables (0 for no improvement, 0,25 for slight, 0,5 pts for moderate, 0,75 pts for significant, and 1 point for full recovery), these accumulate to 37.75 points (of 48 patients), which is equal to 78.64% of total improvement. Counting only the patients whose recoveries were above moderately improved, then 85.41% of patients (41 of 48) experienced moderate, significant or full recovery. Thus, significant total recovery rates were seen, suggesting that both the diagnosis and treatment were likely to be appropriate.
Figure 3: Symptom relief statistics
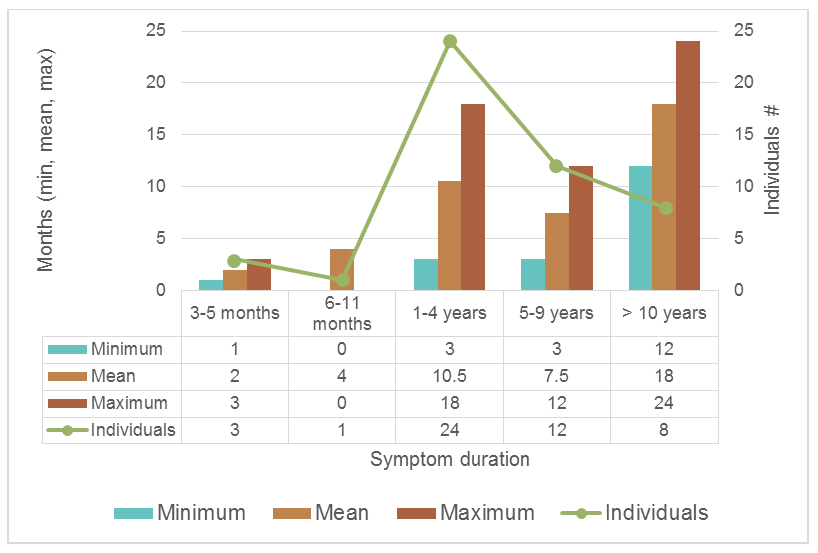
As for recovery times, significant differences were seen between the symptom-duration groups, and recovery times. Average recovery times for the different groups were, as seen in Figure 5: 3-5 months of symptoms; 2 months of recovery time. 6-11 months of symptoms; 4 months of recovery time. 1-4 years of symptoms; 10,5 months of recovery time. 5-9 years of symptoms; 7,5 months of recovery time. More than ten years of symptoms; 18 months of recovery time. Recovery times also greatly varied within each group. The main causes for this were a failure to perform the exercises correctly or doing too many repetitions, which stunted progress and significantly increased restitution time. Other noteworthy and influent factors were whether or not the patient had pain in daily life, or solely during athletic activities. For example, we found that patients whose symptoms had lasted 1-4 years had slower recovery times than those with 5-9 years of affliction. In this study, the groups with sole sports-induced pain and those with daily chronic pain were not separated, which may have contributed to this incidental aberrancy.
Figure 4: Rehabilitation time until recovery
DISCUSSION
Lumbosacral plexus entrapment syndrome is a problem whose nature is very similar, almost identical, to thoracic outlet syndrome, as it is caused by entrapment of the lumbosacral plexuses as they emerge through the psoas major or beneath the piriformis muscles,1 and may thus result in multifocal entrapment neuropathies.5-14 The symptoms of lumbosacral plexus entrapment syndrome may present in quite misleading ways, seemingly unrelated, also similar to TOS and often distal to the main site of entrapment.1-4 In this regard, clinical suspicion as well as knowledge of appropriate provocative tests, are all necessary in order to confirm its presence. Specificity is often a problem with manual testing protocols, but the risk of misdiagnosis may be mitigated by considering several diagnostic criteria rather than just one single test, similar to what is proposed by Selmonosky in his diagnostic triad for TOS,15-17 or the diagnostic cluster for sacroiliac joint dysfunction,18 which involves five tests. Additionally, the symptoms should be compatible with the pelvic and lower extremity neuroanatomy. Finally, exacerbation of the patient’s diffuse symptoms will occur one to two days post exercise, if the diagnosis is correct and appropriate technique is used.
Tinel’s test should be negative on healthy nerves; minimal pain elicitation should occur, even with firm manual pressures. Research has shown that increased pain elicitation upon manual palpation of peripheral nerves has a high sensitivity and decent specificity in the detection of impairment, due to increased mechanosensitivity.19-22 Generally, however, the entrapment may not be severe enough to be considered pathological if < 5-6 NRS. An elicited response of > 7 NRS will often correlate with the presence of LPES-relevant symptoms, in our experience. Further, conventionally, when interpreting Tinel’s test, one looks for the incurrence of radiative symptoms or paresthesia.23 However, it is our experience that the lack of conspicuous radiative pain elicitation does not exclude neuropathy nor indicate sole myofascial affection. This is usually evident by moving the provocative pressure an inch away from the respective nerve’s passage, where it will elicit significantly less pain, even if still palpating the same muscle. Further, in LPES, the full nerve’s length will generally be sensitive to palpation. For example, if the patient presents with symptoms of tarsal tunnel entrapment, and are reproducible with Tinel’s sign of the distal tibial nerve, but the sciatic nerve also hurts upon palpation all the way from the calf and up to the buttocks, this is very unlikely to be a sole distal neuropathy, but rather, indicates proximal entrapment, despite the mere distal symptoms.
Consistent findings of severe weakness of the psoas major and piriformis muscles were found during our diagnostic and rehabilitative trials. However, due to the compensatory patterns which the patient had acquired over the years, some patients needed more guidance and correction than others, in order to target the right tissues and reveal their impairment. Unfortunately, these compensatory patterns may be subtle and often require some experience with LPES in order to be identified. However, confirmatory post-exercise exacerbation will often occur regardless, even in the absence of flawless technique, unless the exercises are performed with great error. When evaluating the initial exacerbation after commencing rehabilitation, the patients reported various degrees of worsening. Further, the patients were generally more sensitive to provocative tests (Tinel’s) upon follow-up than during the initial examination, consistent with slight exacerbation. Once past the exacerbation period, which may last between three to six months, generally regarding the patients whose symptoms had continued for ≥ one year, a gradual and more linear improvement would be seen, and, consistently, reduced sensitivity upon Tinel’s test. In a few patients who fully recovered psoas major and piriformis work capacity, a near or complete loss of pain elicitation upon Tinel’s test was seen. Generally, however, once the patient reached an NRS of approximately 4-5 during Tinel’s test, presuming no focal numbness, they were also symptom free in every-day-life and during athletic activities.
Only 17 of the 61 patients surveyed (27,8%) reported that their symptoms affected the entire LPLE. One could, of course, make the argument that this is fibromyalgia and not plexopathy. However, fibromyalgia is generally considered idiopathic and incurable, whereas LPES is both treatable and curable. Treatable, as such, with simple, inexpensive approaches that the patient can do at home, if properly diagnosed and educated. And, finally, symptom exacerbation as well as increased pain upon Tinel’s sign was seen after commencing rehabilitation of the psoas major and piriformis muscles, consistent with proximal irritation of the lumbosacral plexuses and not focal idiopathic fibralgia. Thus, trial treatment may certainly be warranted if diagnostic criteria are fulfilled during physical examination, and the patient’s symptoms are compatible with denominators of LPES.
Because the treatment of LPES is done by the patient him- or herself, and only guided by the clinician, patient compliance is mandatory. It is paramount that an exercise intensity which causes no more than mild exacerbation is found and pursued. This may take some trial and error to achieve. Excess exacerbation will prolong recovery times and the patient may find themselves in a “limbo” of aggravation, with no improvement in sight, potentially resulting in loss of motivation and compliance. Thus, it is crucial that the patient schedules a follow-up minimum every 8 weeks in the beginning, to detect and correct any potential pitfalls. The main pitfalls involve doing the exercises erroneously or too intensively, both being utter inhibitors of progress. When an exercise intensity which yields mild post-rehabilitative exacerbation of 1-2 days is found, the work volume should gradually be increased over the course of several months. A rapid increase in work volume is rarely tolerated, especially by patients with higher morbidity.
Placebo was not implemented in this study. However, one could say that, because 46 of 48 patients (95,8%) of these patients had already tried several forms of therapy before visiting the author’s clinic, this reduces the likelihood of placebo. Moreover, because significant improvements were seen gradually as the piriformis and psoas major muscles got stronger, and as provocative tests reduced in pain elicitation, i.e. long-term and with compatible variables, these factors also suggest that the results are legitimate and not mere coincidence. Our study also shows that even patients with longstanding, chronic affliction may improve if properly diagnosed and treated. That being said, more statistical and long-term research is needed.
A few final words must also be uttered regarding the roles of stretching and myofascial release (MFR) in the management of nerve entrapment neuropathies. Empirically, it seems that the patients afflicted with entrapment neuropathies gradually worsen with myofascial release and similar treatments. This, especially considering the many chronic pelvic pain patients who are already hypermobile.24,25 Although stretching and MFR may temporarily ameliorate the condition, it will frequently worsen the disease long term, in our experience, as the culprit muscles are also victims of severe weakness. This phenomenon may be quite misleading to patients and clinicians alike. Empirically, the patients who have been stretching the most, are usually also the ones more difficult to treat. Therefore, it is the author’s impression that stretching and MFR as a long-term intervention for entrapment neuropathies should be considered contraindicated and potentially iatrogenic. However, importantly, their role in short-term symptom relief is probably benign and not problematic if done carefully.
CONCLUSION
Lumbar plexus entrapment syndrome is a common problem which may involve significant morbidity, often debilitating the patient. It is caused by entrapment of the lumbosacral plexuses within the psoas major and piriformis muscles, due to severe weakness of these structures. Its presentation generally involves nonspecific pain in the pelvis and lower extremities, which makes it mimic other diagnoses such as fibromyalgia or seemingly unrelated peripheral entrapments, similar to what has been reported for thoracic outlet syndrome. The protocol for identification of LPES involves a compatible patient history, along with abnormally high pain elicitations upon pressure to several of the nervous branches of the LPLE. Myotome weakness, especially of great toe extension, is often present. Further, reproduction of the patient’s symptoms as well as increased pain elicitation upon Tinel’s test after commencing appropriate rehabilitation, may be viewed as “nail in the coffin”-confirmatory. MRI may reveal tendon thickening and hypointense appearance of the psoas major and piriformis tendons, or frank interstitial edema.
The rehabilitation for LPES involves specific, gentle strengthening exercises for the psoas major and piriformis muscles with very low workloads, gradually increasing the muscles’ work capacities over the course of time. During rehabilitative trials, a positive correlation between the proposed diagnostic criteria, treatment, and beneficial outcomes was seen, resulting in a moderate improvement or greater in more than 85% of the patients who followed the programme. The treatment of LPES is safe, inexpensive, simple, and may be carried out by the patient him- or herself within the comfort of their own homes. However, its treatment span is often lengthy, and the patient must pay attention to detail as well as regulate their exercise intensity to avoid excess stimulus of the impaired musculature, as this will completely stunt progress, which may lead to loss of patient compliance and thus also the absence of recovery.
LIMITATIONS
The primary limitation of this study is the lack of LPES research. Thus, many statements in this manuscript are based on the authors’ empirical experience and data. More research is clearly needed, especially with regards to epidemiology and other relevant statistics. Another limitation of this study was that the patient sample numbers were relatively small, and the treatment carried out in a private clinical setting and may therefore not necessarily and appropriately reflect that of the common public population.
Conflict of interest: Nil
Authors’ contribution: Both authors took part in the conduct or study, preparation of the manuscript and literature search.
REFERENCES
- Larsen K, Chien GCC. Lumbosacral plexus entrapment syndrome, part one: A common yet little-known cause of chronic pelvic and lower extremity pain. Anaesth Pain Intensiv Care 2019;23(2)::124-137
- Chevalier X, Larget-Piet B. Femoral neuropathy due to psoas hematoma revisited. Report of three cases with serious outcomes. Spine (Phila Pa 1976). 1992;17(6):724–6. [PubMed]
- Anderson-Jones SR, Zhang T, Trescot AM. Lumbar plexus entrapment: pelvic. In: Peripheral nerve entrapments: Clinical diagnosis and management. Springer Peripheral Nerve Entrapments; 2016. p.527-43. DOI: 10.1007/978-3-319-27482-9_49
- Rassner L. Lumbar plexus nerve entrapment syndromes as a cause of groin pain in athletes. Curr Sports Med Rep. 2011;10(2):115-20. [PubMed] DOI: 10.1249/JSR.0b013e318214a045
- Molinari WJ, Elfar JC. The double crush syndrome. J Hand Surg Am. 2013;38(4):799-801;quiz 801. [PubMed] DOI: 10.1016/j.jhsa.2012.12.038
- Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. Lancet. 1973;2(7825):359-62. [PubMed] DOI: 10.1016/s0140-6736(73)93196-6
- Hurst LC, Weissberg D, Carroll RE. The relationship of double crush syndrome to carpal tunnel syndrome (Analysis of 1,000 cases of carpal tunnel syndrome). J Hand Surg. 1985;10(2):202-4. [PubMed]
- Osterman AL. The double crush syndrome. Orthop Clin North Am. 1988;19(1):147-55. [PubMed]
- Kane PM, Daniels AH, Akelman E. Double crush syndrome. J Am Acad Orthop Surg. 2015 Sep;23(9):558-62. [PubMed] DOI: 10.5435/JAAOS-D-14-00176.
- Merrill CA, Ferreira J, Parrino A, Moss IL. Team approach: upper-extremity numbness. JBJS Rev. 2018;6(6):e3. [PubMed] DOI: 10.2106/JBJS.RVW.17.00166
- Cohen BH, Gaspar MP, Daniels AH, Akelman E, Kane PM. Multifocal neuropathy: expanding the scope of double crush syndrome. J Hand Surg Am. 2016 Dec;41(12):1171-5. [PubMed] DOI: 10.1016/j.jhsa.2016.09.009
- Toussaint CP, Ali ZS, Heuer GG, Zager EL. “Double Crush Syndrome” in thoracic outlet syndrome. London: Springer-Verlag; 2013. p.101-4.
- Morgan G, Wilbourn AJ. Cervical radiculopathy and coexisting distal entrapment neuropathies: double-crush syndromes? Neurology. 1998;50(1):78-83. [PubMed] DOI: 10.1212/wnl.50.1.78
- Baba M, Ozaki I, Watahiki Y, Kudo M, Takebe K, Matsunaga M. Focal conduction delay at the carpal tunnel and the cubital fossa in diabetic polyneuropathy. Electromyogr Clin Neurophysiol. 1987;27(2):119-23. [PubMed]
- Selmonosky CA, Byrd R, Blood C, Blanc JS. Useful triad for diagnosing the cause of chest pain. South Med J. 1981;74(8):947-9. [PubMed] DOI: 10.1097/00007611-198108000-00015
- Selmonosky CA, Poblete Silva R. The diagnosis of thoracic outlet syndrome. myths and facts. Chilean J Surg. 2008 June;60(3):255-61.
- Selmonosky CA. The white hand sign. A new single maneuver useful in the diagnosis of thoracic outlet syndrome. Southern Med J. 2002;85:557.
- Laslett M. Evidence-based diagnosis and treatment of the painful sacroiliac joint. J Man Manip Ther. 2008;16(3):142-52. [PubMed] DOI: 10.1179/jmt.2008.16.3.142
- Khambati FA, Shetty VP, Ghate SD, Capadia GD. Sensitivity and specificity of nerve palpation, monofilament testing and voluntary muscle testing in detecting peripheral nerve abnormality, using nerve conduction studies as gold standard; a study in 357 patients. Lepr Rev. 2009 Mar;80(1):34-50. [PubMed]
- Schmid AB, Brunner F, Luomajoki H, Held U, Bachmann LM, Künzer S, et al. Reliability of clinical tests to evaluate nerve function and mechanosensitivity of the upper limb peripheral nervous system. BMC Musculoskelet Disord. 2009;10:11. [PubMed] DOI: 10.1186/1471-2474-10-11
- Hall TM, Elvey RL. Nerve trunk pain: physical diagnosis and treatment. Man Ther. 1999 May;4(2):63-73. [PubMed] DOI: 10.1054/math.1999.0172
- Nee RJ, Butler D. Management of peripheral neuropathic pain: Integrating neurobiology, neurodynamics, and clinical evidence. Phys Ther Sport. 2006;7(1):36-49. [Free Full Text]
- Tinel J. Le signe du fourmillement dans les lésions des nerfs périphériques. Presse médicale, 1915;47:388-9.
- Scheper MC, de Vries JE, Verbunt J, Engelbert RH. Chronic pain in hypermobility syndrome and Ehlers-Danlos syndrome (hypermobility type): it is a challenge. J Pain Res. 2015 Aug 20;8:591-601. [PubMed] DOI: 10.2147/JPR.S64251
- Kumar B, Lenert P. Joint hypermobility syndrome: recognizing a commonly overlooked cause of chronic pain. Am J Med. 2017 Jun;130(6):640-7. [PubMed] DOI: 10.1016/j.amjmed.2017.02.013