
Lata M Kulkarni, MD, DA1, Renuka Holyachi, MD2, Madhuri S. Kurdi, MD3
1Professor and Head; Department of Anesthesiology,Shridevi Institute of Medical Sciences and Research, Sira Road, Tumkur; 572106, Karnatak State, (India)
2Associate Professor of Anesthesiology, BLDE University’s Shri.B.M,Patil Medical College, Vijayapur- 586103, Karnataka, (India)
3Professor, Department of Anesthesiology, Karnataka Institute of Medical Sciences, Hubli. Karnataka (India)
Correspondence: Dr. Lata M Kulkarni, 201, Staff Quarters, Shridevi Institute of Medical Sciences & Research, Sira Road, Tumkur; 572106, Karnatak State, (India); Phone: +91 9845734615; E-mail: kulkalata700@gmail.com
ABSTRACT
Background and aims: In order to reduce endotracheal tube (ETT) induced emergence phenomenon at extubation which involves postoperative sore throat (POST), cough, hoarseness, dysphagia and hemodynamic changes, we evaluated the efficacy of vegetable gum based (VGB) Lubic gel lubrication alone or in combination with 4% intracuff alkalinized lignocaine (IAL). The vegetable gums in the gel appear to be of special significance.
Methodology: 100 patients undergoing surgical procedures under general anesthesia were randomly allocated to 4 groups of 25 each. In Group C (control group) patients, the ETT cuffs were inflated with air and lubricated with normal saline. In Group G, the cuffs were inflated with air, while in Group L and LG, cuffs were filled with IAL. The Group G and LG cuffs were lubricated with VGB lubricant gel while Group L cuffs were lubricated with normal saline. During the post-extubation period POST was studied using Visual Analogue Scale (VAS) at 15 min, 1, 2, 3 and 24 h. Incidence of cough, dysphagia, hoarseness and hemodynamic changes was recorded and compared.
Results: The mean VAS scores for POST were found to be the least in Group LG (12.6 ± 7.08) compared to Groups C (33.8 ± 9.38), G (32.52 ± 2.11) and Group L (21.6 ± 12.30) over 24 h. Incidence of cough, dysphagia, hoarseness and hemodynamic changes was least in Group LG compared to others.
Conclusion: VGB gel lubrication combined with IAL enhanced the effect of IAL, than IAL or VGB gel lubrication alone thus proving most effective in preventing emergence phenomenon at extubation.
Key words: Endotracheal tube; Extubation; Intubation; Gums; Sore throat
Citation: Kulkarni LM, Holyachi R, Kurdi MS. Vegetable gum based gel lubrication of endotracheal tube cuffs improves efficacy of alkalinized intracuff lignocaine in preventing postoperative sore throat: A randomized controlled study. Anaesth Pain & Intensive Care 2016;20(4):422-428
Received: 01 Jan 2016; Reviewed: 2 Feb, 14 Mar, 2 Dec 2016; Corrected: 30 Nov, 28 Feb, 24 Oct, 7 Dec 2016, Accepted: 28 Dec 201
INTRODUCTION
Sore throat continues to be an undesirable sequelae of endotracheal intubation with an incidence of 30-70%.1 The causative factors described are tracheal mucosal erosions due to endotracheal tube (ETT) cuff, trauma due to intubation or mucosal dehydration.2The occurrence of ETT induced sore throat, coughing, hoarseness, dysphagia and hemodynamic changes at extubation are together described as tracheal tube induced emergence phenomenon.3,4 Safety and efficacy of intracuff alkalinized lignocaine (IAL) in preventing emergence phenomenon has been shown by in vitro and in-vivo studies4,5So also lubrication of ETT with lignocaine jelly/spray and K-Y jelly, a water soluble jelly, in preventing sore throat has been studied and compared.6,7 Further it has been shown that combination of water soluble K-Y jelly with IAL is effective in preventing emergence phenomenon at extubation.8 However ingredients of K-Y jelly being purely synthetic could be harmful to mucous membranes.9 With this background we conducted a study with the vegetable gum based (VGB) water soluble gel lubrication in combination with IAL to find out the effectiveness of the VGB gel in reducing ETT induced emergence phenomena.
Our primary objective was to evaluate the efficacy of lubrication of ETT cuffs with vegetable gum based (VGB) gel and use of intracuff alkalinized lignocaine (IAL) either alone or in combination in preventing postoperative sore throat in adult patients undergoing surgeries under general anesthesia lasting for more than one hour. Prevention of hoarseness and dysphagia in the postoperative period, coughing and hemodynamic changes at extubation were the secondary objectives.
METHODOLOGY
This prospective randomized controlled study was conducted after obtaining institutional ethical committee approval and written informed consent from patients. 100 adult patients of ASA (American Society of Anesthesiologists) physical status grade I and II, scheduled to undergo elective surgical procedures lasting for more than 1 hour under were studied over a period of one year.
Patients belonged to both sexes, between 18-60 years, smokers being included. Patients with ASA grade III and IV, those with upper respiratory tract infection, sore throat, chronic obstructive lung disease, bronchial asthma, predicted difficult intubation, cardiovascular disease and hypertension were excluded from the study. Patients were randomly allocated to 4 groups using a random number table.
Group- C (control), the cuffs were inflated with air and lubricated with normal saline.
Group- G, the cuffs were inflated with air and lubricated with VGB gel.
Group-L, the cuffs were inflated with alkalinized 4% lignocaine and lubricated with normal saline.
Group- LG, cuffs were inflated with alkalinized 4% Lignocaine and lubricated with VGB gel.
Our primary objective was reduction of sore throat. Based on the previous studies7,8 we postulated that IAL and VGB gel lubrication together would reduce the incidence of sore throat by 25-30% when compared to control group and the calculated sample size was 24 that would permit a type I error of α = 0.05, confidence level of 95%,type II error of β = 0.05 and power of 80%. Enrollment of 25 patients in each group was done. There were no drop outs.
One ml of 7.5% of sodium bicarbonate was added to 5ml of 4% lignocaine to prepare alkalinized lignocaine. The VGB gel used was “Lubic™ gel” (Neon Laboratories limited, India) which is a water soluble, vegetable gum based gel. Polyvinyl chloride ETTs (Portex®) with high volume, low pressure cuffs were used. For females 7 mm and for males 8 mm internal diameter sizes were used.
The patients were not aware as to which group they were allocated. The patients were taught about the use of visual analogue scale during preoperative visit. Interventions were carried out by one anesthesiologist and the outcome parameters were noted by another anesthesiologist who was not present during intubation. All patients received tab diazepam 5 mg orally the night before and on the morning of surgery. In the operating room after adequate intravenous (IV) access, application of standard monitors, premedication with glycopyrrolate 0.01 mg/kg, buprenorphine 3 µg/kg and preoxygenation, patients were induced with 5 mg/kg of 2.5% thiopentone sodium. Endotracheal intubation was carried out under IV succinylcholine 2 mg/kg. ETT cuffs were inflated and lubricated as per random allocation of the groups. Anesthesia was maintained with nitrous oxide (N2O) and oxygen (65:35), halothane (0.5%) and vecuronium on controlled ventilation.
On the conclusion of surgery, neuromuscular block was reversed with intravenous glycopyrrolate 0.01 mg/kg and neostigmine 0.05 mg/kg.
After ensuring all the reversal criteria, patients were extubated. Intactness of the protective cough reflex and gag reflex were noted during throat suctioning. Presence of coughing, bucking, hoarseness of voice, difficulty in swallowing, and complications like laryngospasm/ bronchospasm were noted.
Hemodynamic parameters viz. pulse, blood pressure and oxygen saturation were noted at the time of extubation. The ETT cuffs were examined for any signs of rupture.
Sore throat was measured using visual analogue scale (VAS 0-100 mm; score 0 – no sore throat and score100 – worst sore throat) following extubation periods of 15 min, 1 h, 2 h, 3 h and 24 h.
The 4 groups were compared for age, sex, weight distribution, duration of surgery, distribution of smokers, hemodynamic changes at extubation and severity of sore throat as per VAS scale. Presence or absence of cough at extubation was recorded as yes or no when patient either coughed or not while breathing regularly or irregularly while deflating the cuff or extubation. Dysphagia and hoarseness were noted and the recorded using binary scale (Yes/No). SPSS version 20 was used for statistical analysis. Analysis of variance (ANOVA) was used to find statistical difference for age, weight, duration of surgery. Chi-square test was used to find difference in sex distribution and distribution of smokers. Student’s ‘t’ test was used for parametric data. Chi-square/Fishers exact test was used to find significant differences between the percentages of dysphagia, coughing and hoarseness. Tukey Krammer multiple comparison test was used for intergroup comparisons of sore throat, showing significance of ‘q’ value > 3.706 as p < 0.05. A p < 0.05 was considered to be statistically significant. Data were presented as mean ± standard deviation (SD) and percentage.
RESULTS
All the 4 groups were similar in the demographic parameters, distribution of smokers and duration of surgery (Table 1).
Table 1: Comparison of demographic variables, distribution of smokers and duration of Surgery.
| Parameters | Group C
n=25 |
Group G
n=25 |
Group L
n=25 |
Group LG
n=25 |
Test | p value+ | |||||||
| Age (Yrs) (Mean ± SD*) | 38.56 ± 10.89 | 40.9 ± 10.00 | 38.4 ± 10.5 | 35.5 ± 10.6 | Anova
F=1.11 |
p > 0.05 | |||||||
| Sex (M : F) | 10 : 15 | 10 : 15 | 10 : 14 | 12 : 13 | Chi-Square
1.53 |
p > 0.05 | |||||||
| Weight(Kg)
(Mean ± SD) |
55.42 ± 3.26 | 54.32 ± 7.56 | 54.58 ± 4.21 | 53.97 ± 5.21 | Chi-Square0.951 | p > 0.05 | |||||||
| Smokers : Non-smokers | 10 : 15 | 9 : 16 | 9 : 16 | 12 : 130 | Chi-Square
0.8352 |
p > 0.05 | |||||||
| Duration of surgery (Min)(Mean ± SD) | 113.4 ± 24.9 | 115.4 ± 24.70 | 111.8 ± 31.08 | 110.4 ± 32.65 | Anova
F=0.289 |
p > 0.05 | |||||||
*SD- Standard deviation
Fig: 1 Incidence of sore throat
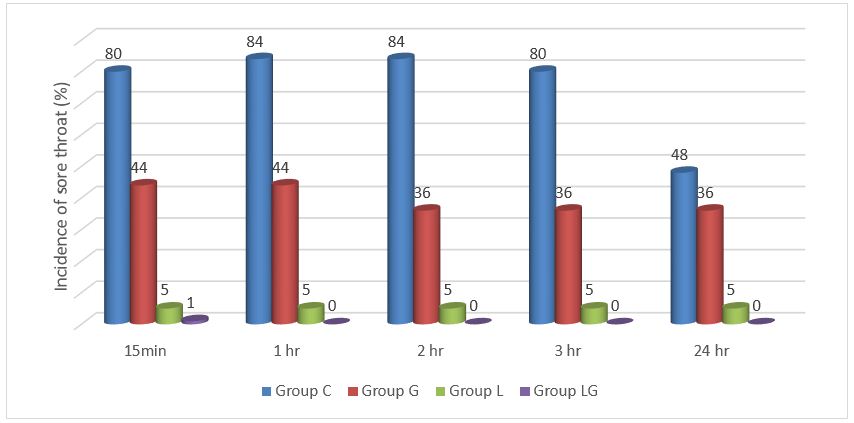
The overall incidence of sore throat among the study group ranged from none to up to 80% (Figure 1). In Groups C and G, where the common factor was air inflation of cuff with different lubricants, the incidence of sore throat was significantly less in Group G but the severity of sore throat as assessed by VAS was not significantly different. When Group L and G were compared, though there was no significant difference in the incidence of sore throat between the two groups, the VAS scores were significantly less in Gr L indicating that intracuff lignocaine alone if more effective than Gel alone. (Figure 1; Table 2).
Table 2: Comparison of incidence of sore throat among the groups (calculation based on data in Figure 1)
| Groups | 15 min | 1 h | 2 h | 3 h | 24 h |
| Group C vs. Group G | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.05 | p > 0.05 |
| Group C vs. Group L | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.0001 | p < 0.05 |
| Group C vs. Group LG | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Group G vs. Group L | p > 0.05 | p > 0.05 | p > 0.05 | p < 0.05 | p > 0.05 |
| Group G vs. Group LG | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Group L vs. Group LG | p < 0.05 | p < 0.01 | p < 0.05 | p < 0.01 | p < 0.05 |
In Groups G and LG, i.e. gel lubrication being common for differently inflated cuffs, there was significant reduction of both incidence and severity of sore throat. In Groups L and LG, where intracuff lignocaine being common to differently lubricated cuffs, both the incidence and severity of sore throat was significantly less in Group LG. Sore throat incidence was reduced nearly 90% in Group LG and 40-50% reduction was seen with gel alone compared to control group (Figure 1).
Table 3: VAS (visual analogue scale 0-100 mm) scores for sore throat (mean ± standard deviation)
| Groups
(n=25) |
15 min | 1hr | 2hrs | 3hrs | 24hrs |
| Group C | 46.8 ± 12.15 | 42.6 ± 7.65 | 41 ± 7.21 | 40.4 ± 7.05 | 33.8 ± 9.38 |
| Group G | 36.12 ± 14.13 | 35.12 ± 13.22 | 33.72 ± 12.96 | 33.52 ± 12.81 | 32.52 ± 2.11 |
| Group L | 25.6 ± 16.02 | 24.2 ± 14.83 | 22.8 ± 13.39 | 22.2 ± 13.54 | 21.6 ± 12.30 |
| Group LG | 15.00 ± 9.46 | 13.8 ± 7.25 | 13.4 ± 7.02 | 12.2 ± 6.30 | 12.6 ± 7.08 |
Table 4: Comparison of severity of sore throat among the groups – intergroup comparisons
| Groups | 15 min | 1hr | 2hrs | 3hrs | 24hrs |
| Group C vs. Group G | P < 0.05 q=4.054 | P > 0.05 q=3.324 | P > 0.05 q=3.436 | P > 0.05 q=3.290 | P > 0.05 q=0.612 |
| Group C vs. Group L | P < 0.01 q=8.048 | P < 0.001 q=8.1777 | P < 0.001 q=8.590 | P < 0.01 q=8.702 | P < 0.001 q=5.839 |
| Group C vs. Group LG | P < 0.001 q=12.07 | P < 0.001 q=12.79 | P < 0.001 q=13.02 | P < 0.001 q=13.48 | P < 0.001 q=10.14 |
| Group G vs. Group L | P < 0.05 q=3.994 | P < 0.01 q=4.853 | P < 0.01 q=5.154 | P < 0.01 q=5.412 | P < 0.01 q=5.227 |
| Group G vs. Group LG | P < 0.001 q=8.018 | P < 0.001 q=9.475 | P < 0.001 q=9.51 | P < 0.001 q=10.19 | P < 0.001 q=9.534 |
| Group L vs. Group LG | P < 0.05 q=4.024 | P < 0.01 q=4.622 | P < 0.05 q=4.437 | P < 0.01 q=4.781 | P < 0.05 q=4.308 |
Tukey Kramer multiple comparison test was used to compare the parameters between groups. According to this, if q > 3.706 then p < 0.05.
Hoarseness, dysphagia and cough and were significantly less in Group LG and Group L as compared to control group (Tables 5; Figures 2, 3 & 4). Protective reflexes viz. gag reflex, swallowing and cough reflex were intact. There were no incidence of laryngospasm, bronchospasm or cuff rupture in any of the groups.
Figure 2: Incidence of Hoarseness
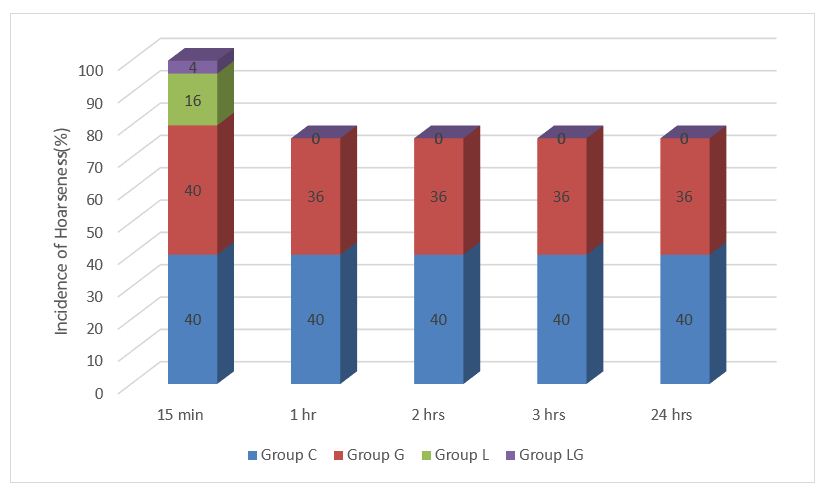
Figure 3: Comparison of dysphagia
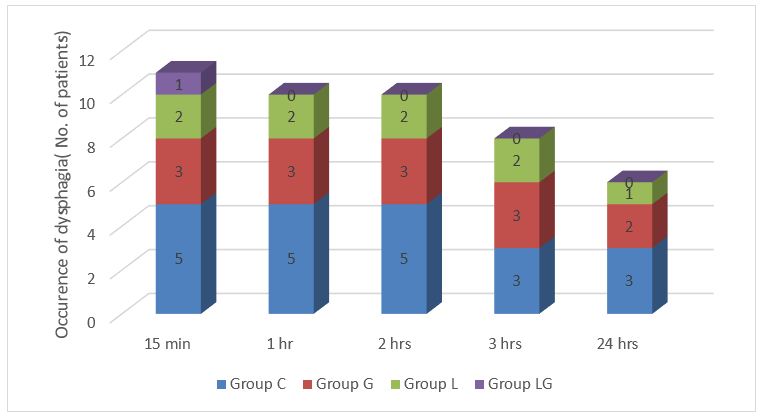
Figure 4: Changes in the hemodynamic parameters at extubation compared to baseline (%)
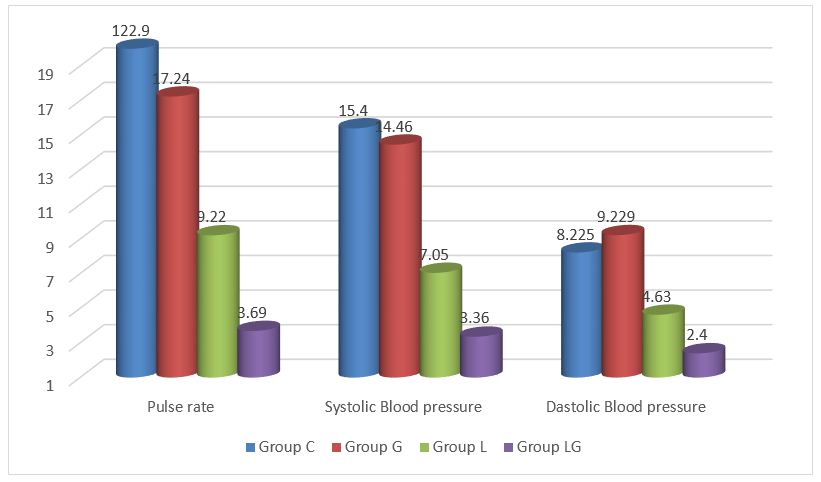
Hemodynamic changes at extubation with respect to baseline were significantly less in Groups L and LG but not Group G when compared to control group (Figure 4).
Table 5: Comparison of coughing at extubation [n (%)]
| Groups (n=25) | Cough at extubation | Chi-square | p value | |
| Yes | No | |||
| Group C | 10 (40) | 15 (60) | 9.21 |
p < 0.05 |
| Group G | 7 (28) | 18 (72) | ||
| Group L | 6 (24) | 19 (76) | ||
| Group LG | 1 (4) | 24 (96) | ||
DISCUSSION
Our study showed that combined use of vegetable based gel lubrication along with IAL was superior to either IAL or saline/VGB gel lubrication alone in preventing emergence phenomenon at extubation. Mucosal damage occurring at cuff level is thought to be an important factor for occurrence of sore throat subsequent to slow rise of cuff pressure in the air-filled cuffs during N2O anesthesia.10,11 Laryngeal epithelial inflammation, metaplasia, dysplasia and upper airway hyper-reactivity already developed in chronic smokers is further exacerbated by GA and tracheal intubation resulting in respiratory complications;12,13 as a matter of fact, we did include smokers in our study and with comparable distribution of smokers/nonsmokers among all the groups.
The Lubic™ gel used in the study for lubrication of the tracheal tubes is a water soluble gel that contains combination of synthetic and vegetable gums.14 Vegetable gums are hydrophilic and gel forming in nature. Being non-toxic, stable, biocompatible and easily available, they are considered as versatile and novel excipients in drug delivery systems for sustained release.15,16 In our study we found combination Group LG most effective. It appears that combination of VGB gel with IAL has helped in sustained release of IAL across the cuff. Sustained drug delivery systems are known to significantly improve therapeutic efficacy of drugs.15 Ours is the only study wherein the hydrophilic and lubricant properties of the vegetable gums in Lubic gel have been utilized for lubrication of ET cuffs to test reduction in ETT induced emergence phenomena. Lubrication of Proseal-LMA and endotracheal tubes with the Lubic gel have been done in other studies; however, properties of VGB gel as such were not aimed in those studies.17,18,19 Lubrication of ETT cuffs with Chamomile-extract for reduction of postoperative sore throat was found to be without much benefit.20
In the study by Estebe et al., a combination of water soluble gel lubrication of ETT cuffs with K-Y jelly and IAL was used showing better efficacy of combination group than IAL alone in preventing emergence phenomenon.8 But since K-Y jelly is totally a synthetic gel, VGB gel is a safer choice. K-Y jelly first patented in 1904 as a surgical lubricant is popular as a personal lubricant and some ingredients can be irritating to the mucous membranes.9 In comparison a vegetable gum based gel is not only safer but has its own place due to the novel properties of vegetable gums.15-16
Reports of lubrication of tracheal tube with betamethasone gel have shown effective reduction of sore throat, cough and hoarseness.21 Here steroid gel has been used for its anti-inflammatory effect assuming the potential inflammation by the ETT. Secondly as mentioned in the study itself the possibility of flaring up of local subtle infection by betamethasone gel, cannot be denied.21
Whereas combination of VGB gel lubrication with IAL in our study, we feel is, physiological where diffusion of IAL through the cuffs takes place with a sustained effect and blocks the stimulation of tracheal mucosal sensory C fibers. Thus the ETT cuff induced erosion of tracheal mucosa is prevented before the occurrence of inflammation itself. Water soluble gel lubrication also prevents aspiration across the folds of large volume cuffs.22
The hemodynamic changes in our study showed a similar trend between Groups LG and L when compared to Groups G and C.
Among various ways of lignocaine applications better outcome with intravenous and intracuff lignocaine for ETT induced postoperative complications is reported.23,24,25,26As regards the use of intracuff lignocaine,4%, 2%, 10% concentrations have been used indicating their safety and efficacy.4, 5, 25
An in-vitro, double blind study by Estebe et al. using 8.4% and 1.4% concentrations of NaHCO3 showed efficacy, safety and diffusion of lignocaine. We used 5 ml of 4% lignocaine with 1 ml of 7.5% NaHCO3 without any untoward effect.
With least incidence of hoarseness and coughing (4%) in Group LG compared to other groups and an intact cough reflex implies a distinct advantage of VGB gel with IAL over other groups. Studies comparing ETT cuffs filled with air, saline, IAL for reduction of sore throat, cough and hoarseness and have indicated superior efficacy of IAL over air and saline filled cuffs.27,28,29 Combination of lubrication with VGB gel with IAL can further enhance this effect due to sustained release.
Our study showed a satisfactory reduction of sore throat, coughing, hoarseness, dysphagia and hemodynamic disturbances at extubation and for over 24 hours with the use of IAL along with VGB Lubic gel cuff lubrication, without suppressing protective reflexes. However, VGB gel lubrication alone was not satisfactory. In the present study we did not measure cuff pressure, which can be a limitation of the study, nevertheless there was no rupture of cuffs in any case. Further studies regarding role of vegetable gums in formulation of water soluble gels and their comparison with other synthetic gels for lubrication of ET cuffs in prevention of emergence phenomena are required.
CONCLUSION
Use of combination of vegetable gum based gel lubrication of endotracheal tube cuffs and intracuff alkalinized lignocaine together is a simple, safe and effective method for prevention of emergence phenomenon at extubation than either of them used alone.
Conflict of interest: Nil declared by the authors
Authors’ contribution: LMK: Concept, study design, data interpretation, manuscript preparation and review
RHA: Data collection, preparation of manuscript
MSK: Data collection, analysis, preparation of manuscript
REFERENCES
- Chandler M. Tracheal intubation and sore throat: A mechanical explanation. Anaesthesia 2002;57:155–61. [PubMed] [Free full text]
- Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth 2002;88:582–4. [PubMed] [Free full text]
- Fagan C, Frizelle HP, Laffey J, Hannon V, Carey M. The effects of intracuff lidocaine on endotracheal-tube-induced emergence phenomena after general anesthesia. Anesth Analg 2000;91(1):201–5. [PubMed]
- Estebe JP, Dollo G, Le Corre P, Le Navoures A, Chevanne F, Le Verge R, et al. Alkalinization of intracuff lidocaine improves endotracheal tube induced emergence phenomenon. Anesth Analg 2002;94(1):227-30. [PubMed]
- Estebe JP, Gentili M, Le Corre P, Dollo G, Chevanne F, Ecoffey C. Alkalinization of intracuff lidocaine efficacy and safety. Anesth Analg 2005;101:1536–41. [PubMed]
- Kori K, Muratani T, Tatsumi S, Minami T. The influence of endotracheal tube cuff lubrication on postoperative sore throat and hoarseness. Masui 2009;58(3):342–5. [PubMed]
- Dokumo DM, Faponle AF, Bolaji BO, Adenekan AT, Olateju SOA. Effects of lidocaine and k-y jellies on sore throat, cough, and hoarseness following endotracheal anaesthesia. J West Afr Coll Surg 2011;1(3):44-61 [PubMed] [Free full text]
- Estebe JP, Delahaye S, Le Corre P, Dollo G, Le Naoures A, Chevanne F, et al. Alkalinization of intra-cuff lidocaine and use of gel lubrication protect against tracheal tube-induced emergence phenomena. Br J Anaesth 2004;92(3):361–6. [PubMed] [Free full text]
- Thomas P. Behind the label: K-Y Jelly. The Ecologist [serial online] 2007 Oct 24 [cited 3 July 2016]; Available from: URL:http://www.theecologist.org/green_green_living/behind_the_label/269286/behind_the_label_ky_jelly.html
- Combes X, Schauvliege F, Peyrouset O, Motamed C, Kirov K, Dhonneur G, et al. Intracuff pressure and tracheal morbidity: influence of filling with saline during nitrous oxide anesthesia. Anesthesiology 2001;95(5):1120–4. [PubMed] [Free full text]
- Sato K, Tanaka M, Nishikawa T. Changes in intracuff pressure of endotracheal tubes permeable or resistant to nitrous oxide and incidence of postoperative sore throat. Masui 2004 ; 53(7):767-71. [PubMed]
- Navarro LH, Lima RM, Aguiar AS, Braz JR, Carness JM, Módolo NS. The effect of intracuff alkalinized 2% lidocaine on emergence coughing, sore throat, and hoarseness in smokers. Rev Assoc Méd Bras 2012;58(2):248–53. [PubMed] [Free full text]
- Wetzel LE, Ancona AL, Cooper AS, Kortman AJ, Loniewski GB, Lebeck LL. The effectiveness of 4% intracuff lidocaine in reducing coughing during emergence from general anesthesia in smokers undergoing procedures lasting less than 1.5 hours. AANA J2008;76(2):105–8. [PubMed]
- Lubic jelly. [Online] [cited 2015 Dec 3] Available from: URL:https://www.medicineindia.org/medicine-brand-details/16838/lubic-jelly
- Avachat AM, Dash RR, Shrotriya SN. Recent investigations of plant based natural gums, mucilages and resins in novel drug delivery systems. Indian J Pharm Edu Res 2011;45(1):86-99.
- Jani GK, Shah DP, Prajapati VD, Jain VC. Gums and mucilages: Versatile excipients for pharmaceutical formulations. Asian Journal of Pharmaceutical Sciences. 2009,4(5):308-322. [Free full text]
- Misra M, Ramamurthy B. The Proseal LMA and the tracheal tube; a comparison of events at insertion of the airway device. The Internet Journal of Anaesthesiology [serial online] 2007 [cited 2015 Oct 3]; 16(2). Available from:URL:http://ispub.com/IJA/16/2/4287
- Kuragayala U, Ravinutala S, Rammurthy KR. A controlled comparison between betamethasone gel and lidocaine jelly applied over tracheal tube to reduce post-operative sore throat, cough and hoarseness of voice. International journal of contemporary medical research. 2016;3(2):442-446. [Free full text]
- Agarwal A, Gupta D, Yadav G, Goyal P, Singh PK, Singh U. An evaluation of the efficacy of Licorice Gargle for attenuating Post-operative sore throat: A Prospective Randomized, Single-blinded Study. Anesth Analg. 2009:109(1):77-81. [PubMed] doi: 10.1213/ane.0b013e3181a6ad47.
- Charuluxananan S, Sumethawattana P, Kosawiboonpol R, Somboonviboon W, Werawataganon T. Effectiveness of lubrication of endotracheal tube cuff with chamomile-extract for prevention of postoperative sore throat and hoarseness. J Med AssocThail 2004;87(2):S185-9. [PubMed]
- Sumathi PA, Shenoy T, Ambareesha M, Krishna HM. Controlled comparison between betamethasone gel and lidocaine jelly applied over tracheal tube to reduce postoperative sore throat, cough, and hoarseness of voice. Br J Anaesth 2008;100(2):215–8. [PubMed] [Free full text]
- Blunt MC, Young PJ, Patil A, Haddock A. Gel lubrication of the tracheal tube cuff reduces pulmonary aspiration. Anesthesiology 2001;95(2):377–81. [PubMed] [Free full text]
- Venkatesan T, Korula G. A comparative study between the effects of 4% endotracheal tube cuff lignocaine and 1.5 mg/kg intravenous lignocaine on coughing and hemodynamics during extubation in neurosurgical patients: a randomized controlled double-blind trial. J Neurosurg Anesthesiol 2006;18(4): 230-4. [PubMed]
- Soltani HA, Aghadavoudi O. The effect of different lidocaine application methods on postoperative cough and sore throat. J Clin Anesth. 2002;14:15–8. [PubMed]
- Altintas F, Bozkurt P, Kaya G, Akkan G. Lidocaine 10% in the endotracheal tube cuff: Blood concentrations, haemodynamic and clinical effects. Eur J Anaesthesiol 2000;17(7):436–42. [PubMed]
- D’Aragon F, Beaudet N, Gagnon V, Martin R, Sansoucy Y.The effects of lidocaine spray and intracuff alkalinized lidocaine on the occurrence of cough at extubation: a double-blind randomized controlled trial. Can J Anaesth. 2013 Apr;60(4):370-6. [PubMed] doi: 10.1007/s12630-013-9896-8.
- Jaichandran V, Bhanulakshmi I, Jagadeesh V, Thennarasu M. Intracuff buffered lidocaine versus saline or air-A comparative study for smooth extubation in patients with hyperactive airways undergoing eye surgery. South Afr J Anaesth Analg 2009;15(2):11–4. [Free full text]
- Shroff PP, Patil V. Efficacy of cuff inflation media to prevent postintubation-related emergence phenomenon: air, saline and alkalinized lignocaine. Eur J Anaesthesiol 2009;26:458–62. [PubMed] [Free full text]
- Navarro LHC, Braz JRC, Nakamura G, Lima RM, de Paula e Silva F, Módolo NSP. Effectiveness and safety of endotracheal tube cuffs filled with air versus filled with alkalinized lidocaine: A randomized clinical trial. Sao Paulo Med J 2007;125:322–8. [Free full text]a
