
Hetavi U. Contractor1, Vibhuti A. Shah2, Vidhi A. Gajjar3
1Senior Resident cum Tutor; 2 Associate Professor; 3 Assistant Professor
Department of Anesthesia, AMC MET Medical College, Sheth L.G. General Hospital, Ahmedabad, Gujarat (India)
Correspondence: Dr Hetavi U. Contractor, SR cum Tutor, Department of Anesthesia, AMC MET Medical College, Sheth L.G. General Hospital, NR Rambaug Fire Station, Opp. Vyayam Vidhyalay, Maninagar, Ahmedabad, Gujarat, India 380008; E-mail: drpiyushpujara@gmail.com
ABSTRACT
Aims and objectives: To study the effect of ultrasound guided superficial cervical plexus and interscalene brachial plexus block for clavicular surgery.
Methodology: Thirty American Society of Anesthesiologists (ASA) physical status I and II patients undergoing clavicular surgery, ages 20-60 years were selected. All routine non- invasive monitors were applied and IV line was secured. Ultrasound guided superficial cervical plexus block and interscalene brachial plexus block were given. Injection dexmedetomidine 1 µg/kg infusion over 10 min was started. Block efficacy was evaluated. Any complication or side effects were noted. Sedation was assessed using Ramsay sedation score. Perioperative hemodynamics were charted. Duration of motor block was noted as time of shoulder abduction 3cm from time of block. Duration of analgesia was noted as time for first demand of analgesic from time of block.
Results: All the thirty patients allowed clavicular surgeries under combined interscalene brachial plexus and superficial cervical plexus block. No major complications and side effects were noted.
Conclusion: USG guided combined superficial cervical plexus and interscalene brachial plexus block are effective for clavicular surgery without any major complication and may be used in place of general anesthesia or blocks by other techniques.
Key words: Ultrasound; Superficial cervical plexus block; Interscalene brachial plexus block; Dexmedetomidine; Ramsay sedation scale
Citation: Contractor HU, Shah VA, Gajjar VA. Ultrasound guided superficial cervical plexus and interscalene brachial plexus block for clavicular surgery. Anaesth Pain & Intensive Care 2016;20(4):447-450
Received: 20 Jul 2016; Reviewed: 10 Oct, 14 Nov 2016; Corrected: 17 Dec 2016; Accepted: 19 Dec 2016
INTRODUCTION
The anatomy of neck, particularly nerve anatomy in relation to clavicle is complex. The distal clavicle and anterior superior shoulder area derives its nerve supply from both brachial plexus and cervical plexus. The cervical plexus innervates C2, C3 and C4 sensory dermatomes. The cervical plexus supplies fascia and skin above clavicle and shoulder up to the region of acromion. Depending upon the source, the innervation of the skin overlying the clavicle varies between C3 and C5, while the sclerotome distribution of clavicle varies from C4 to C6. The brachial plexus innervates the entire upper extremity, both motor and sensory; specifically the skin over deltoid. Thus any single block is usually insufficient for complete coverage of clavicular surgical pain.
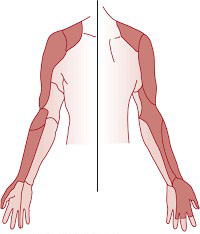
Figure 1: Coverage by brachial plexus block
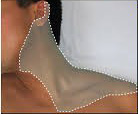
Figure 2: Coverage by superficial cervical plexus block
Peripheral nerve blocks used to anesthetize patients for clavicular surgeries are superficial cervical plexus block, interscalene brachial plexus block or combined superficial cervical and interscalene brachial plexus block.
Interscalene Brachial Plexus Block
It is useful for shoulder surgeries including lateral two thirds of clavicle, proximal humerus and shoulder surgeries.1 The block can be performed by conventional(Winne’s approach), with the use of PNS and with the use of USG. Interscalene block is an invasive procedure with serious complications like Horner’s syndrome, diaphragmatic hemiparesis, epidural, subarachnoid or vertebral artery injection, if not performed carefully and should be performed by or under instructions of trained person using appropriate equipment.
Superficial Cervical Plexus Block
It is useful for surgeries like carotid endarterectomy, superficial neck surgeries and for clavicular surgeries in combination with the interscalene brachial plexus block. With the use of USG technique drug can be deposited in the vicinity of C2, C3 and C4 roots and complications like too deep innervation of needle and puncture of neighbouring structures can be avoided.
But keeping in mind the dual innervation of clavicle, in this study we intended to study the use of combined superficial cervical plexus and interscalene brachial plexus block for conducting clavicular surgery.
METHODOLOGY
After obtaining approval of the institutional ethics committee and written informed consent from all the participants, a prospective study was undertaken.
A total of 30 patients of ASA 1 & 2, 20-60 years of age, undergoing elective orthopedic clavicular surgeries in our hospital were selected.
Patients with infection at the puncture site, coagulopathy, hypersensitivity to drugs used, pregnant females, psychiatric and neurological disease, and patients with severe COPD were excluded.
All patients were kept fasting overnight. In the operating room, all patients were connected to electrocardiography, peripheral oxygen saturation (SpO2) and non‑invasive blood pressure monitor and all the basal parameters were recorded. An IV line was obtained with 18 or 20 gauge cannula. After prior premedication with 4 mg of ondansetron all the patients were preloaded with 10 ml/kg of lactated ringer’s solution.
The patient were placed in supine position with 45º head up and after turning the head to opposite side USG guided interscalene brachial plexus block and superficial cervical plexus block were given. 10-15ml of 1.5% lignocaine with adrenaline plus 5-10 ml of 0.5% bupivacaine were given in interscalene brachial plexus block and 0.25% 10 ml bupivacaine were given in superficial cervical plexus block.
After giving block all patients were given inj. dexmedetomidine 1 µg/kg over 10 minutes. Efficacy of block was assessed for motor and sensory effect. Perioperative hemodynamics were charted.
The level of sedation was evaluated using Ramsay Sedation Scale till the patient was discharged from PACU. Excessive sedation was defined as a score greater than 4/6.
Duration of motor block was noted as time of shoulder abduction by 3 cm from the time of block. Duration of analgesia was noted as time for first demand of analgesic from time of any complications of block e.g. ptosis, meiosis (Horner’s syndrome), respiratory distress, hoarseness of voice, were noted.
Hypotension (systolic blood pressure less than 90 mmHg or more than 20% fall from base line value) bradycardia (heart rate < 50/min) and postoperative complications if any were noted and treated appropriately.
RESULTS
The demographic data of the patients are given in Table 1.
Table 1: The demographic data and ASA grade of the present study.
| Parameter | Study group |
| Age(years) | 34.37 ± 9.01 |
| Male | 17 |
| Female | 13 |
| ASA 1/ 2 | 16 / 14 |
| Weight (kg) | 56.73 ± 7.52 |
| Height (cm) | 165.30 ± 3.41 |
Vital signs recorded during the study are given in Table 2. All the parameters remained stable throughout the perioperative period.
Table 2: Vital data of the participants (mean ± SD)
| Parameters | Observation |
| Pulse rate (beats / min) | 90 ± 5.4 |
| Systolic BP (mmHg) | 134 ± 6.1 |
| Diastolic BP (mmHg) | 82 ± 2.6 |
| SpO2 (%) | 98 ± 2.7 |
| Ramsay sedation score | 2.09 ± 0.1 |
| Duration of analgesia (hours) | 4.61 ± 1.08 |
The complications noted during the study period were Horner’s syndrome in 8/30 (26.7%) patients and hoarseness of voice in 5/30 (16.7%) patients. No other complication was noted.
DISCUSSION
General anesthesia and regional anesthesia have been successfully used for upper extremity and clavicular surgeries.2,3 Both types of anesthesia have their own sets of advantages and disadvantages. Modern anesthesiology is the science of managing reflexes associated with surgery. Most of these reflexes are initiated by noxious stimuli resulting from surgery or trauma. These reflexes can be managed at the end organ e.g. with beta blockers to counteract hypertension and tachycardia, in respiration to noxious stimulus muscle relaxants to prevent spinal cord mediated reflexive movement. Second site where these reflexes can be interrupted is in the CNS using opioids but these come with many unwanted and unpleasant side effects like tolerance, nausea, constipation and respiratory depression.
Perhaps the optimal place to interrupt this noxious stimulus is the place of its origin itself. This is the prime use of regional anesthesia in modern practice where in it blocks the relay of pain to spinal cord and brain. Regional anesthesia provide excellent analgesia, while minimizing opioids related side effects by reducing the needs of opioids. Nerve block anesthesia being cheaper than GA has many advantages such as anesthesia targeted at the operative site, excellent postoperative pain relief, decreased opioid use and reduced recovery time.4,5
Regional anesthesia in clavicular surgeries can be successfully managed using combined interscalene and superficial cervical plexus block. The combination of these two blocks successfully covers the complicated sensory innervation of clavicle providing excellent intra operative analgesia and muscle relaxation. Regional analgesia results in opioids sparing, early ambulance, decreased postoperative nausea and vomiting and shorter hospital stay.6 On the other hand, general anesthesia also has disadvantage of postoperative nausea and vomiting, delayed recovery. Some perceived disadvantage of interscalene block vs general anesthesia are block performance time which is taken care of by use of USG.
Use of ultrasound in anesthesiology has revolutionised the practice of regional anesthesia. In this study we used USG guided interscalene block and superficial cervical clavicular brachial plexus block. Several studies have examined the effect of USG in quality of interscalene block. Kapral et al compared USG guided vs PNS guided interscalene block and found greater motor and sensory effect with USG.7 Similarly, a randomized study by Liu et al, examining ultrasound vs nerve stimulator for ISB in randomized patients revealed increased motor blockade assessed after five minutes as well as decreased needle attempts for the Ultrasound group.8 Mc Naught et al. noted decreased needle attempts for USG group also decreased minimum effective analgesic volume of local anesthesia and decreased pain 30 min postoperatively when compared to PNS group.9 The USG group also have revealed decreased Incidence of phrenic nerve blockade and respiratory complications and decreased vascular puncture.10 The ultrasound use decreases incidence of diaphragmatic hemi paresis.11When examining ultrasound placement vs. Nerve stimulator placement of ISB catheters in randomized patients, Fredrickson et al demonstrated greater effectiveness in ultrasound group requiring less local anesthetic volumes and fewer needle attempts.12
In our study all the patients were vitally stable throughout the surgery and also postoperatively. Loading dose of dexmedetomidine was given prior to surgical incision in our study. As dexmedetomidine has a role in modulating pain, inhibiting the pain transmission and perception of pain, its role as a pre-emptive analgesic needs to be assessed. It gives best sedation to the patient so that patient can be comfortable intraoperatively being hemodynamic stable.
In our study Horners syndrome was observed in 8/30 (26.7%) patients and hoarseness of voice in 5/30 (16.7%) patients. No other significant side effects were noted. In our study combined interscalene brachial plexus and superficial cervical plexus block also provided postoperative analgesia and made patients early ambulatory and comfortable.
CONCLUSION
We conclude that USG guided combined superficial cervical plexus and brachial plexus block is effective for clavicular surgery and may be used as sole anesthetic technique. It avoids the complications associated with general anesthesia and use of opioids.
Conflict of interest: None declared.
Sources of funding: Nil.
Authors’ contribution: All of the authors took part in the conduct of the study and the manuscript preparation.
REFERENCES
- Borgeat A, Ekatodramis G. Anaesthesia for shoulder surgery, Best Pract Res Clin Anesthesiol. 2002 Jun;16(2):211-225. [PubMed]
- Hadzic A, Arliss J, Kerimoglu B, Karaca PE, Yufa M, Claudio RE, et al. A comparison of infraclavicular nerve block versus general anesthesia for hand and wrist day-case surgeries. Anaesthesiology. 2004 Jul;101(1):127–32. [PubMed] [Free full text]
- Mariano ER, Chu LF, Peinado CR, Mazzei WJ. Anaesthesia- controlled time and turnover time for ambulatory upper extremity surgery performed with regional versus general anaesthesia. J Clin Anesth. 2009 Jun;21(4):253-7. [PubMed] [Free full text] doi: 10.1016/j.jclinane.2008.08.019
- Maga JM, Cooper L, Gebhard RE. Outpatient regional anaesthesia for upper extremity surgery update (2005 to present) distal to shoulder. Int Anesthesiol Clin. 2012 Winter;50(1):47-55. [PubMed] doi: 10.1097/AIA.0b013e31821a00a8.
- Ilfeld BM, Wright TW, Enneking FK, Vandenborne K. Total elbow arthroplasty as an outpatient procedure using a continuous infraclavicular nerve block at home: a prospective case report. Reg Anesth Pain Med. 2006 Mar-Apr;31(2):172-6. [PubMed]
- Hadzic A, Williams BA, Karaca PE, Hobeika P, Unis G, Dermksian J, et al For outptient rotator cuff surgery, nerve block anesthesia provides superior same day recovery over general anesthesia. Anesthesiology. 2005 May;102(5):1001-1007. [PubMed] [Free full text]
- Kapral S, Greher M, Huber G , Willschke H, Kettner S, Kdolsky R, et al., Ultrasonographic guidance improves the success rate of interscalene brachial plexus blockade. Reg Anaesth Pain Med..2008 May-Jun;33(3):253–258. [PubMed] doi: 10.1016/j.rapm.2007.10.011.
- Liu SS, Zayas VM, Gordon MA, Beath JC, Maalouf DB, Paroli L. et al., “A prospective, randomized, controlled trial comparing ultrasound versus nerve stimulator guidance for interscalene block for ambulatory shoulder surgery for postoperative neurological symptoms. Anaesth Analg. 2009 Jul;109(1):265–271. [PubMed] doi: 10.1213/ane.0b013e3181a3272c.
- McNaught A, Shastri U, Carmichael N, Awad IT, Columb M, Cheung J, et al. Ultrasound reduces the minimum effective local anaesthetic volume compared with peripheral nerve stimulation for interscalene block. Br J Anaesth 2011 Jan;106(1):124-130. [PubMed] [Free full text] doi: 10.1093/bja/aeq306.
- Riazi S, Carmichael N, Awad I, Holtby RM, McCartney CJ. Effect of local anaesthetic volume (20 vs 5 ml) on the efficacy and respiratory consequences of ultrasound-guided interscalene brachial plexus block. Br J Anaesth 2008 Oct;101(4)549-56. [PubMed] [Free full text] doi: 10.1093/bja/aen229
- Renes SH, Rettig HC, Gielen MJ, Wilder-Smith OH, van Geffen GJ. Ultrasound-guided low-dose interscalene brachial plexus block reduces the incidence of hemidiaphragmatic paresis. Reg Anesth Pain Med. 2009 Sep-Oct;34(5):498–502. [PubMed]. doi: 10.1097/AAP.0b013e3181b49256.
- Fredrickson MJ, Ball CM, Dalgleish AJ. A prospective randomized comparison of ultrasound guidance versus neurostimulation for interscalene catheter placement. Reg Anesth Pain Med. 2009 Nov-Dec;34(6):590-4. [PubMed]
