
Dheeraj Kapoor, MD, FCCP, FACEE, FCCS*, Anand Gupta, MDS, MFDS RCPS (Glasgow)**, Deepak Thapa, DNB, DA***, Jasveer Singh, MD*
*Assistant Professor (Anesthesiology), **Assistant Professor (Oral and Maxillofacial Surgery), ***Associate Professor
Govt. Medical College and Hospital, Chandigarh-160030 (India).
Correspondence: Dr.Dheeraj Kapoor, 1207, Sector 32 B, Chandigarh, (India); Phone: 911724622549, 919646121549; E-mail: kapoor.dheeraj72@gmail.com, dheeraj.kapoor72@gmail.com
ABSTRACT
Airway management in the craniomaxillofacial trauma surgery may require some modifications of the standard intubation techniques. Nasotracheal intubation is often not an option in panfacial and midfacial injuries due to the probable presence of fractures of base of the skull and associated risk of brain trauma and iatrogenic meningitis. Submental endotracheal intubation may serve as an effective and safe alternative route in these conditions. In standard technique of submentotracheal intubation, the tube is fixed extraorally at the submental incision site with sutures to prevent displacement of the tube during the surgical intervention. But still it leaves a possibility of accidental extubation during the conversion of orotracheal to submental route and vice versa. To counteract this problem we in our institution, fix the tube at two points, one at molar teeth in intraoral region and second at skin surface externally near submental incision site ensuring a secured airway. This procedure has eliminated accidental displacement or extubation in our cases.
Key words: Craniomaxillofacial trauma; Panfacial injuries; Submentotracheal intubation; Tube Fixation technique; Molar teeth; ETT.
Citation: Kapoor D, Gupta A, Thapa D, Singh J. Two point fixation of endotracheal tube in submentotracheal intubation during craniomaxillofacial surgeries-our experience! Anaesth Pain & Intensive Care. 2012:16(3):273-275
INTRODUCTION
Airway management in the craniomaxillofacial trauma surgery requires special considerations and modifications of the standard intubation techniques. Nasotracheal intubation is often contra indicated in panfacial and midfacial injuries due to the probable presence of fractures of base of the skull and associated risk of brain trauma and iatrogenic meningitis.1 Midfacial fractures may also cause obstruction to the nasotracheal tube passage and the interference with the surgical reconstruction in that area. These fractures commonly require maxillo-mandibular fixation to restore the dental occlusion, which precludes the use of orotracheal intubation. Surgical tracheostomy may be indicated but is associated with complications such as tracheal stenosis, injury to cervical vessels or the thyroid gland, and thus should be avoided.1
Submental endotracheal intubation may serve as an effective and safe alternative route in these conditions.2-4 This technique creates a clear intraoperative surgical access, allows maxillo-mandibular fixation without any obstruction and negates the problems associated with conventional intubation through oral and nasal routes in these surgical procedures. Beside craniomaxillofacial trauma surgeries it may also be safely used in many other elective surgical procedures such as LeFort osteotomies, mandibular orthognathic surgery and rhinoplasty procedures.4,6
In standard technique of submentotracheal intubation, the tube is fixed externally at the submental incision site with sutures to prevent displacement of the tube during the surgical intervention. But still there remains a possibility of accidental extubation during the conversion of orotracheal to submental route and vice versa.4,5,7 There is also a chance of tube displacement during the intraoral manipulation by the surgeon as the part of tube in the oropharyngeal region is freely movable and acutely angulated due to the submental fixation. To counteract this problem we in our institution fix the tube inside the oral cavity by a silk suture to the molar teeth. In this novel technique the endotracheal tube is fixed at two points (Fig 1 & 2), one at molar teeth in intraoral region and second at skin surface in extra oral region near submental incision site, ensuring an extra secured airway than usual single point fixation.
Figure 1: Diagram showing fixation of ET tube at two points, intraoral and extraorally
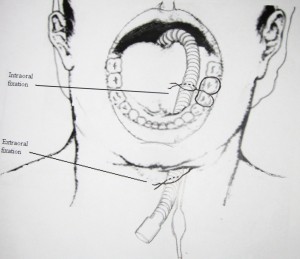
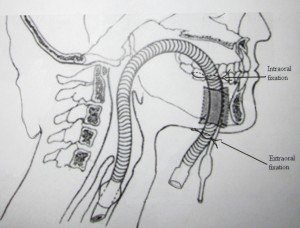
Figure 2: Diagram showing submentotracheal intubation
TECHNIQUE
The patient is initially intubated orally, preferably with flexometallic endotracheal tube with a detachable universal connector. After confirmation of the correct position and length of the tube, 2-0 silk suture is first tied around the molar teeth on the side of submental incision firmly, keeping free ends of the thread long and intact. Then the free ends of the silk thread are firmly tightened around the tube at the point it passes around the molar teeth lingual (Fig 3). This leads to secure fixation of the tube intraorally to prevent any undue movement.
Taking all aseptic precaution of the skin of the neck, lower face and end of the tube, a 1.5 cm skin incision is made in submental region, just medial to the lower border of mandible, approximately one third of the way from symphysis to the angle of mandible. By keeping the mouth open a medium size artery forceps is introduced through submental incision, keeping the direction towards the floor of the mouth staying close to the inner aspect of the mandible to avoid damage of the sublingual gland, submandibular duct and lingual nerve. Then, an incision is made in oral tented mucosa of the floor of the mouth and the artery forceps is dilated after entering the oral cavity to allow easy passage of the proximal end of the tube. We ventilate the patient with 100% oxygen before taking out connector from the tube. The deflated pilot tube cuff is held with artery forceps and is taken out through the submental incision. The tip of the artery forceps is quickly re-inserted through the submental incision to grasp the tracheal tube end to take it out through the same incision. Connector is reattached and patient is ventilated through breathing circuit.
Second fixation of tube is done at the submental incision site using 2.0 silk suture to give secure fixation to prevent displacement of the tube during the surgical intervention (Fig. 4). The fixation of tube with the molar teeth on the lingual side does not hinder any manipulation of jaws during reduction of fracture fragments or intermaxillary fixation.
Figure 3: Arrow showing intraoral fixation of ET tube at molar teeth using silk suture

Figure 4: Extraoral fixation using silk suture at skin area near submental incision site (arrow)

After completion of the surgical procedure, if extubation is desired, submental fixation point is released and the proximal end of the tube is pulled inside from proximal to the molar fixation point for orotracheal conversion, thus avoiding any displacement or change in position of the tube at the distal end. Submental incision is closed in two layers. Now the molar fixation point is released and the patient trachea is extubated after executing the standard criteria of extubation, ensuring that the patient is fully awake with intact airway reflexes.
DISCUSSION
The one point fixation technique of endotracheal tube during submental intubation is commonly employed in panfacial trauma patients. There is always a possibility of tube dislodgement during this procedure which can result in catastrophic outcomes. Studies have reported complications like accidental extubation, dislodgement or obstruction of the endotracheal tube (ETT) during submental intubation.4,5,7 Anesthesiologists often struggle to maintain the optimal position of the tube during the orotracheal to submental conversion and vice versa with one point fixation technique. We improvised securing of the ETT by applying one more fixation point intraorally to keep the tube secured during manipulation of jaws in surgical interventions and during orotracheal/submental ETT conversions. On search of PubMed, we did not found any reference pertaining to the mentioned fixation technique for submental intubation.
This fixation technique reduces the possibility of accidental extubation during orotracheal to submental conversion and vice versa. The force applied to ETT for reverting it back from submental to usual orotracheal one can result in inadvertent dislodgement of the ETT. The molar fixation of the ETT can prevent this potential catastrophe. This simple technique can be used effectively for fixation of ETT intraorally but may have certain limitations. The intraoral part of the tube once fixed cannot be manipulated during the surgical intervention thus sometimes restricting the surgical access. We have practiced this two point fixation technique in 8 patients during the last one year, with desirable outcome. We observed no change in the position of the ETT during the conversion of orotracheal tube to submental route and vice versa. In one patient we had to release the molar fixation during intraoperative period to serve the surgical requirement of extensive intraoral manipulation. No other complications like skin infections or ETT damage was noticed in these patients. Though, we strongly feel that further studies are warranted to evaluate the efficacy of this technique when compared to the conventional one point fixation technique during submental intubation to come out with more definitive outcomes.
Acknowledgement: We are grateful to Dr Ruchita Gupta (Dental Surgeon, Chandigarh) for her important contribution in the artistic work of diagrams of submental tube fixation for better description and understanding.
REFERENCES
- MacInnis E, Baig M. A modified submental approach for oral endotracheal intubation. Int J Oral Maxillofac Surg. 1999;28:344-6. [Medline]
- Altemir FH. The submental route for endotracheal intubation: a new technique. J Maxillofac Surg. 1986;14:64-5. [Medline]
- Caron G, Paquin R, Lessard MR, Trepanier CA, LandryPE. Submental endotracheal intubation: an alternative to tracheotomy in patients with midfacial and panfacial fractures. J Trauma. 2000;48:235-40. [Medline]
- Amin M, Dill-Russell P, Manisali M, Lee R, Sinton I. Facial fractures and submental tracheal intubation. Anaesthesia. 2002;57:1195-9. [Medline]
- Jundt JS, Cattano D, Hagberg CA, Wilson JW. Submental intubation: a literature review. Int J Oral Maxillofac Surg. 2012 Jan;41:46-54. Epub 2011 Sep 17. [Medline]
- Biglioli F, Mortini P, Goisis M, Bardazzi A, Boari N. Submental orotracheal intubation: An alternative to tracheotomy in transfacial cranial base surgery. Skull Base. 2003;13:189–95. [Medline]
- Chandu A, Witherow H, Stewart A. Submental intubation in orthognathic surgery: Initial experience. Br J Oral Maxillofac Surg. 2008;46:561–563. [Medline]
