
Manohar Bhat, MD1, Hemant Bhagat, DM1, Ishwar Bhukal, MD1, Neeru Sahni, MD1, Puneet Khanna, MD2, Sunil K Gupta, MCh3
1Department of Anesthesia & Intensive Care, 3Department of Neurosurgery
Postgraduate Institute of Medical Education and Research (PGIMER), Kairon Block, Sector 12, Chandigarh, 160012, (India)
2Department of Anesthesia & Intensive Care, All India Institutes of Medical Sciences (AIIMS), New Delhi, (India)
Correspondence: Dr Hemant Bhagat, DM Neuroanesthesia, Associate Professor, Department of Anesthesia & Intensive Care, Postgraduate Institute of Medical Education and Research (PGIMER), Kairon Block, Sector 12, Chandigarh, 160012, (India); Ph: +917087009529; E-mail: hembhagat@rediffmail.com; Fax: +9117227444401
ABSTRACT
Background & objective: Resection of cerebellopontine (CP) angle tumors is a technically demanding surgery in view of important neural structures in the vicinity of tumor giving limited working area to the neurosurgeon. Consequently, it is important to advocate anesthetic techniques which provide optimal surgical conditions. Moreover, the prolonged duration of surgery necessitates fast tracking of emergence from anesthesia to allow early neurological complication and reintervention. We compared the effect of propofol and desflurane on hemodynamics, brain relaxation, vasomotor response to surgical stimulus, emergence and postoperative complications in patients undergoing cerebellopontine angle tumor resection.
Setting: A tertiary care hospital in Northern India
Methodology: Thirty adult patients scheduled to undergo CP angle tumor resection were randomized to receive propofol or desflurane under a standardized anesthesia and emergence protocol. Normality of the data was checked by measures of Kolmogrov Smirnov tests of normality. Means of normally distributed data were compared using Student’s t-test for two groups and for skewed data or for scores Mann–Whitney test were applied. For time dependent changes repeated measure ANOVA was applied.
Results: The demographic and intraoperative hemodynamics were similar among the two groups. The brain relaxation scores and vasomotor response to surgical stimulus were comparable in both the groups. The time to emergence was 9.60 ± 3.3 min in the propofol and 4.7 ± 1.3 min in desflurane group (p < 0.01).
Conclusions: Both propofol and desflurane are comparable as anesthetic agents for patients undergoing CP angle tumor resection in terms of hemodynamics, brain relaxation scores and response to surgical stimulus. However, the use of desflurane in these patients is associated with faster emergence when compared with propofol.
Key words: Propofol; Desflurane; Cerebellopontine angle tumor; Tumor resection; Brain surgery; Neuroanesthesia
Citation: Bhat M, Bhagat H, Bhukal I, Sahni N, Khanna P, Gupta SK. Prospective randomized evaluation of propofol and desflurane in patients undergoing surgery for cerebellopontine angle tumors. Anaesth Pain & Intensive Care 2015;19(4):478-484
INTRODUCTION
Cerebellopontine (CP) angle tumors account for 5-10% of all intracranial tumors. Posterior fossa is a compartment of narrow confines housing vital neural structures and vasomotor centres. Surgery through this limited window is intimidating to the neurosurgeons and the anesthetic techniques should facilitate maximum brain relaxation and differentiation of vital brain structures. The intraoperative vasomotor responses are one of the original article important indicators of impingement of vital neural structures during surgery. It is in this background that the anesthetic agents should provide stable hemodynamics, provide a relaxed brain, allow recognition of vasomotor responses to surgical stimulation and also, permit early awakening at the end of surgery for early neurological evaluation.1
The choice of intravenous over inhalational anesthetics still remains controversial. Propofol reduces cerebral metabolic rate of oxygen (CMRO2) and cerebral blood flow (CBF) and its pharmacological profile permits continuous administration for maintenance of anesthesia with stable hemodynamics followed by quick emergence after infusion is stopped. 2-4 Desflurane with its blood gas partition coefficient of 0.42 also favors early emergence and at 1 MAC, it reduces CMRO2 by approximately 51% and CBF by 22%.5,6 Hence, desflurane has also gained popularity as maintenance agent in neurosurgical procedures.
This study was designed to prospectively evaluate the effects of two anesthetic agents- propofol and desflurane on intraoperative hemodynamics, brain bulge scoring, vasomotor response to surgical stimulation, emergence from anesthesia and postoperative complications in patients undergoing resection of CP angle tumor.
METHODOLOGY
Approval was sought from the institutional ethical committee of Post Graduate Institute of Medical Education and Research, Chandigarh. Written informed consent was obtained from all the patients. The present study is a preliminary randomized prospective trial conducted on 30 ASA (I-II) patients of either sex, aged between 18 and 60 years undergoing elective craniectomy forcerebellopontine angle tumor resection. Randomization was done to one of the study group by picking up an opaque sealed envelope. The study was conducted from January 2011 to December 2011. Unconscious patient and those with history of allergy to any of the study drugs were not included in the study. The patients with cardiovascular, respiratory, hepatic and renal dysfunction were excluded from the study. The preoperative radiological tumor characteristics, lower cranial nerve involvement, features of raised intracranial pressure (ICP) and presence of ventriculoperitoneal (VP) shunt for cerebrospinal fluid (CSF) diversion were recorded. All chronic medications were continued till the day of the surgery.
Preinduction monitoring consisted of 5-lead ECG, heart rate (HR), invasive blood pressure (IBP) and pulse oximetry (SpO2). Additional postinduction monitoring consisted of end-tidal carbon-dioxide (EtCO2), nasopharyngeal temperature, neuro muscular monitoring and entropy. All the patients were preloaded with 8-10 ml/kg of normal saline prior to induction. Central venous cannulation was done whenever deemed necessary.
Anesthesia Protocol
The anesthesia plan has been laid out in Table 1. The patients were induced with intravenous morphine 0.1 mg/kg followed by thiopental 4-6 mg/kg. Tracheal intubation was facilitated with vecuronium 0.1 mg/kg intravenously.
Table 1: Anesthesia Plan
| Stage | Propofol | Desflurane |
| Beginning of dural closure | Inj propofol (3 mg/kg/hr)
+ inj. diclofenac (2 mg/kg). |
Desflurane (2%)
+ inj. diclofenac (2 mg /kg) |
| Completion of skin sutures | Propofol infusion stopped | Desflurane stopped |
| Removal of head pins | Nitrous oxide off | Nitrous oxide off |
Ventilation was adjusted so as to achieve an end tidal carbon dioxide concentration of around 30-35 mm Hg. Anesthesia was maintained with either propofol (5-10 mg/kg/hr) or desflurane (end tidal conc. of 3-4%) depending upon the randomization. All the patients received supplemental nitrous oxide in oxygen (60:40) so as to maintain state entropy value of 40-60. Intermittent vecuronium was administered till the beginning of skin closure according to the need to maintain a maximum of single twitch on nerve stimulation. Morphine was supplemented if required. Following tumor excision and hemostasis, anesthetic management was according to the emergence plan laid out in Table 1.
Body temperature was maintained using a forcedair warming blanket. Following the removal of head pins, the patients were ventilated with increased oxygen flow rate at 10 lit/min. Once the patients opened their eyes or responded to verbal commands, the residual neuromuscular blockade was reversed with intravenous neostigmine 0.05 mg/ kg and glycopyrrolate 0.01 mg/kg. The trachea was extubated after adequate reversal of neuromuscular blockade, return of spontaneous respiration and airway reflexes.
Hemodynamics
The heart rate and invasive blood pressure were continuously monitored. Vasomotor response during surgical dissection and tumor resection were closely monitored. Any changes were immediately informed to the surgeon so as to minimize or avoid injury to neural structures. Intraoperative hypertension was defined as an acute increase in mean arterial blood pressure (MAP) by more than 20% of the ongoing value for more than thirty seconds. Intraoperative hypotension was defined as an acute decrease in MAP by more than 20% of the ongoing value for more than thirty seconds. If MAP fell below 70 mm of Hg and if the removal of surgical stimulus did not restore the MAP to normal, it was managed with fast infusion of crystalloids. If this was not effective, a vasopressor (mephentermine / phenylephrine) was used. Intraoperative bradycardia was defined as sudden fall in HR by more than 20% of the ongoing value. Intraoperative tachycardia was defined as sudden increase in HR by more than 20% of the ongoing value. Any other forms of arrhythmias were also monitored.
Intraoperative surgical field
The intraoperative relaxation of brain was assessed by the surgeon at the following times (a) following raising of the bone flap, (b) following dural reflection, (c) during tumor excision, (d) following dural closure. The grading was done at each time point as (1) satisfied (2) not satisfied but can manage and (3) not satisfied and intervention is required. Similarly at the time of raising the bone flap, an attending anesthesiologist also looked into the relaxation of brain and graded it as (1) within the margin of the inner table of the skull, (2) within the margin of the outer table of the skull, and (3) outside the margin of the outer table of the skull. Both the surgeon and anesthesiologist were blinded to the anesthesia protocol.
Emergence characteristics
Emergence time was measured as the time from anesthetic discontinuation till the patient responded to verbal commands. Tracheal extubation time was measured as the time from discontinuation of the anesthetic agent till extubation. The patients who responded to verbal command within 15 min of discontinuation of anesthesia were considered to have early emergence. Patients with poor cough reflex or pre-operative lower cranial nerve lesions were not extubated. However, their emergence characteristics were noted.
Assessment of coughing during emergence was made and graded as none, mild single cough, moderate >1 unsustained (≤ 5 sec) coughing, severe sustained (≥ 5 sec) bouts of coughing.7 Reaction of the patients on emergence was categorized as agitated, calm or sedated. Agitated patients were those who were restless and required pharmacological or physical restraint. Those patients who were comfortable and co-operative were considered calm. Those patients who were responding to commands but drowsy were considered sedated. Those patients who were not extubated were followed up and time to extubation or tracheostomy was noted.
Other parameters
The intraoperative use of intravenous fluids, opioids and muscle relaxants were noted. The estimated blood loss and intraoperative urine output were recorded. The patients were interviewed after twenty four hours in postoperative period for intraoperative awareness using the modified Brice interview.8 Postoperative duration of hospital stay was also noted.
Statistical Analysis
The study is a prospective pilot trial with a sample size of 15 patients in each group since no previous published study has compared emergence with use of propofol and desflurane. The statistical analysis was carried out using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 15.0 for Windows). Normality of the data was checked by measures of Kolmogrov Smirnov tests of normality. Normally distributed data were presented as mean ± standard deviation (S.D.). Skewed data were presented as median ± quartiles (interquartile range). Categorized data were presented as frequency or proportions. Means of normally distributed data were compared using Student’s t-test for two groups and for skewed data or for scores Mann–Whitney test were applied. For time dependent changes repeated measure ANOVA was applied. Proportions were compared using Chi square or Fisher’s exact test (whichever is applicable). All statistical tests were two-sided and were performed at a significance level of α = 0.05.
RESULTS
The patients in both the groups were comparable in terms of age, weight and gender (Table 2). Preoperative patient and radio-logical characteristics were similar among the two groups (Table 2). Patients with hydrocephalus underwent VP shunt
Table 2: Demographic and tumor data of the patients
| Age (years) | 37.7 ± 13.3 | 35.8 ±13.5 | 0.69 |
| Gender (male/female) | 8/7 | 7/8 | 0.71 |
| Weight (kg) | 59.1 ± 10.4 | 58.2 ± 7.8 | 0.78 |
| Raised ICP | 8 | 10 | 0.45 |
| VP shunt | 8 | 10 | 0.45 |
| Lower cranial nerve palsy | 7 | 10 | 0.26 |
| Max tumor diameter (cm) | 4.3 ± 0.8 | 4.2 ± 0.7 | 0.64 |
| Mass effect | 11 | 12 | 0.66 |
Values expressed as mean ± standard deviation or number of patients
Patients with hydrocephalus underwent VP shunt prior to the definitive surgery. There was no difference in the intraoperative characteristics among the groups (Table 3).
Heart rates were similar among the groups during the perioperative period (Figure 1).
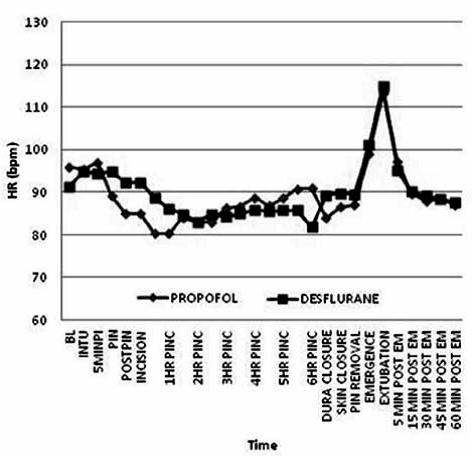 Figure 1: Comparative heart rate in both groups
Figure 1: Comparative heart rate in both groups
Analysis of MAP showed a significant rise in the patients of propofol group during pin application and at thirty minutes following incision when compared to desflurane group (Figure 2).
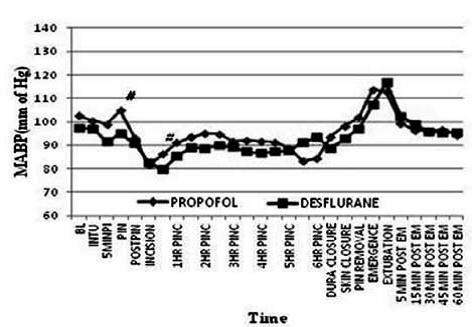 Figure 2: Comparative mean arterial pressure in both groups
Figure 2: Comparative mean arterial pressure in both groups
However this does not appear to be clinically significant. Both the groups had non-sustained rise of HR and MAP during the periextubation phase. The two anesthetics did not differ with regards to their effect on vasomotor response to surgical stimulus during tumor resection (Table 3). None of the patients had any other forms of arrhythmia during the surgery.
All the patients in the two groups had a comparable degree of brain relaxation scores (Table 3). Maximum brain bulge occurred following dural reflection in all the patients.
There was significant difference in the time to emergence from anesthesia and immediate extubation between the two groups (Table 4).
Table 3: Intraoperative procedure related data
| Parameter | Propofol
(n=15) |
Desflurane
(n=15) |
p |
| Duration of anesthesia(min) | 383 ± 94 | 415 ± 81 | 0.33 |
| Duration of surgery (min) | 322 ± 87 | 356 ± 84 | 0.27 |
| Morphine (mg) | 7.3 ±1.4 | 7.2 ± 1.5 | 0.95 |
| Vecuronium (mg) | 15.8 ± 2.7 | 16 ± 2.5 | 0.86 |
| IV Fluids (lit) | 4.1 ± 0.7 | 4.2 ± 0.9 | 0.55 |
| Estimated blood loss (ml) | 446 ±172 | 460 ± 176 | 0.83 |
| Urine output (ml) | 953 ± 227 | 980 ±193 | 0.73 |
| Temp at extubation (ºc) | 35.9 ± 0.1 | 35.9 ± 0.1 | 1 |
| Position (supine/park bench) | 12/3 | 12/3 | 1 |
Values expressed as mean ± standard deviation or number of patients
Table 4: Brain relaxation score
| Parameter | Propofol
(n=15) |
Desflurane
(n=15) |
p |
| Anesthesiologist’s grading | |||
| Bone reflection (1/2/3) | 10/4/1 | 11/4/0 | 0.59 |
| Surgeon’s grading | |||
| Bone reflection(1/2/3) | 12/3/0 | 10/4/1 | 0.56 |
| Dural reflection(1/2/3) | 6/4/5 | 6/3/6 | 0.89 |
| Tumor resection(1/2/3) | 14/1/0 | 15/0/0 | 0.31 |
| Dural closure(1/2/3) | 15/0/0 | 15/0/0 | |
Values expressed as number of patients
Patients in desflurane group had faster emergence (4.7 ± 1.3 min) compared to propofol group (9.6 ± 3.3 min) (p < 0.05). However the number of patients who had early emergence was not different among the groups. Two patients in the propofol group had delayed emergence. There were 6 patients in propofol group and 5 patients in desflurane group who underwent extubation in the operation room (OR). Patients in desflurane group had significantlyfaster time to extubation in the OR (p < 0.05). The emergence agitation and scores of coughing during periextubation period were comparable among the groups. Eighteen patients had delayed extubation in the postoperative period. The delayed extubation times were comparable among the groups. One of the patients in desflurane group underwent tracheostomy.
Table 5: Vasomotor response to surgical stimulus
| Parameter | Propofol
(n=15) |
Desflurane
(n=15) |
p |
| Bradycardia | 8 / 2 / 2 / 2 / 0 / 1 | 6 / 3 / 2 / 1 / 0 / 3 | 0.76 |
| Hypertension | 9 / 2 / 2 / 0 / 1 / 1 | 10 / 3 / 1 / 0 / 0 / 1 | 0.81 |
| Hypotension | 12 / 3 / 0 / 0 / 0 / 0 | 14 / 0 / 1 / 0 / 0 / 0 | 0.12 |
Values expressed as number of patients as 0 / 1 / 2 / 3 / 4 / 5 or more
episodes
Table 6 Emergence characteristics
| Parameter | Propofol
(n=15) |
Desflurane
(n=15) |
p |
| Early / delayed emergence | 13 / 2 | 15 / 0 | 0.14 |
| Time to emergence (min) | 9.60 ± 3.3 | 4.7 ± 1.3 | 0.01 |
| Early extubation | 6 | 5 | 0.70 |
| Time to early extubation (min) | 12.8 ± 2.3 | 9 ± 2.5 | 0.02 |
| Coughing (n / m / m / s)* | 6 / 4 / 5 / 0 | 10 / 3 / 2 / 0 | 0.29 |
| Emergence agitation (a / c / s)** | 2 / 13 / 0 | 2 / 13 / 0 | 1 |
| Time to delayed extubation (hours) | 10.7 ± 2 | 9.5 ± 2*** | 0.26 |
Values expressed as mean ± standard deviation or number of patients;
* none / mild / moderate / severe; ** agitated / calm / sedated; ***one
patient was tracheostomized
None of the patients had intraoperative awareness when assessed after 24 hours. Non-dependent brachial plexus paresis was observed in the postoperative period in one patient in propofol and two patients in desflurane group who underwent
surgery in Park Bench position. New onset facial palsy following surgery was observed in two patients in propofol group and three in desflurane group. The postoperative hospital stay was 6.6 + 1.24 in propofol group and 6.5 + 1.6 days in desflurane group (P > 0.05).
DISCUSSION
As CP angle tumor surgery is a long duration surgery and associated with vasomotor responses to surgical stimulus, there is a need for anesthetic technique which allows adequate depth of anesthesia, stable hemodynamics, brain relaxation followed by early emergence in order to assess postoperative neurosurgical complications. The two most common anesthetic agents used in neurosurgical patients are propofol and desflurane.9-12 Consequently, we designed this pilot study to evaluate the effects of propofol and desflurane in patients undergoing CP angle tumor surgery.
Maintenance of stable hemodynamics is required to maintain adequate cerebral perfusion pressure. In our study, we found stable hemodynamics with the use of propofol or desflurane. However, emergence hypertension and tachycardia was observed in both the groups. Pain experienced during craniotomy closure is responsible for hypertension and use of low dose opioids has been suggested to limit this hypertension without any untoward side effect.13
As the resection of CP angle tumors can cause surgical trauma to the areas of brain responsible for control of airway, respiration, autonomic function and consciousness, sudden change in hemodynamic parameters (heart rate, blood pressure and ECG rhythm) are reliable early warning signs of impingement of these vital structures.14 The anesthetist has to meticulously watch for any such change and alert the surgeon immediately. In the present study, the vasomotor
responses observed were comparable with the use of either anesthetic agents. Thus, despite providing adequate depth of anesthesia, both the agents do not obtund the vasomotor responses to surgical stimulus. Also, during the conduct of
study, vasomotor changes were promptly informed to the neurosurgeon and resolved as soon as the surgical stimulus was removed. In a study by Signore and colleagues, intravenous atropine original article was used to correct bradycardia during resection of acoustic neuroma.15 On the contrary, in our study, no pharmacological agents were used and releasing the surgical stimulus restored the stable hemodynamics.
Although this study was not powered to detect differences in brain relaxation between the two anesthetic agents, the intraoperative brain relaxation scores were comparable between the two groups. The brain relaxation scores were
similar with the use of propofol, sevoflurane and desflurane in a study done in patients undergoing surgery for supratentorial tumors.12 In the present study, the patients with grade III brain swelling during dural reflection were the ones who already had raised ICP. The brain bulge does not appear to be influenced by the anesthetics in these patients and it could be relieved only by release of CSF from the cistern magna.
In our study, desflurane was associated with faster emergence in comparison to propofol. The low blood gas partition coefficient of desflurane (0.42) enables early onset and offset of anesthesia.5 The difference observed can also be explained by the long duration of surgery which prolonged the context-sensitivity half time of propofol which can lead to prolonged recovery.16 The clinical significance of this difference in emergence with the use of desflurane and propofol is unclear as awakening was less than 15 min with the use of both the agents. In a similar study on patients with acoustic neuroma the emergence time was shorter with desflurane when compared to isoflurane. Considering both our study and that of Boisson- Bertrand et al, both desflurane and propofol seem reasonable for early awakening (< 15 min) in patients undergoing resection of CP angle tumors.17 There are multiple studies evaluating the effects of propofol or desflurane on emergence in patients undergoing craniotomy for supratentorial tumors. Though there may be individual differences related to method of conduct of trials, both propofol and desflurane appear acceptable in facilitating early emergence in neurosurgical patients.9-12
Early extubation was deferred in 9 patients in propofol group and 10 patients in desflurane groups due to lower cranial nerve palsies and poor cough reflex following emergence from anesthesia. The coughing scores were similar among the two groups in this study. The incidence of coughing on emergence from general anesthesia in the presence of an endotracheal tube is more than forty percent.18 The cough reflex is initiated by chemically or mechanically activating sensitive vagal afferent nerves in larynx and trachea.19 Low incidence of cough in this study might be due to the presence of lower cranial nerve palsy in most patients. In view of presence of lower cranial nerve palsy or weak cough reflex the extubation was delayed in few patients. The time to delayed extubation were not influenced by the anesthetic agent used. Similarly, the anesthetic agents did not have any bearing on the emergence agitation scores. Thus the quality of emergence appears to be similar and acceptable with use of propofol and desflurane. Similarly, the duration of postoperative hospital stay is not influenced by the choice of anesthetic agent used in our study.
Three patients in our study had brachial plexus paresis and all the three patients underwent surgery in park bench position with the nondependent side developed weakness. A case report by Satoru et al has described the association of park bench position to the brachial plexus injury on the dependent side.20 Swelling in the neck at the end of surgery was thought to compress the brachial plexus and they also hypothesized that kinking of the jugular vein due to extremely flexed neck position during surgery would have led to delayed swelling of the neck and brachial plexus. However in our case the nondependent side was involved and the reason for paresis might be the compression of brachial plexus between the clavicle and the first rib due to traction on the non-dependent arm.
LIMITATIONS
Our study has a few limitations. The present study is only a pilot trial with small sample size. The study was only single blinded in nature which is a source of potential bias. Moreover measurement of intracranial pressure would have been a better assessment of the intraoperative brain tension.
CONCLUSION
The present study concludes that both propofol and desflurane appear similar for maintenance of general anesthesia in the conduct of surgery for CP angle tumor. However, desflurane is associated with shorter time to emergence when compared to propofol, so might be a preferable anesthetic agent for maintenance in this set of patients. propofol vs desflurane in cerebellopontine surgery
Conflict of interest: None
Source of funding: This study was completed with funding from
Postgraduate Institute of Medical Education and Research (PGIMER),
Chandigarh, (India)
Author contribution:
MB: Collection of data and statistical analysis
HB: Concept, data collection, statistical analysis, manuscript writing
IB: Concept, conduction of study, manuscript editing
NS: manuscript writing, analysis of results
PK: conduction of study
SKG: Reviewing of manuscript for intellectual content
REFERENCES
- Bruder N, Ravussin P. Recovery from anesthesia and postoperative extubation of neurosurgical patients: a review. J Neurosurg Anesthesiol 1999;11:282-93.
- 2. Smith I, White PF, Nathanson M, Gouldson R. Propofol: An update on its clinical use. Anesthesiology 1994;81:1005-43.
- Vandesteene A, Trempont V, Engleman E, Deloof T, Focroul M, Schoutens A, et al.Effect of propofol on cerebral blood flow and metabolism in man. Anesthesia1988;43:42-3.
- Hogue CW, Bowdle TA, O’Leary, Duncalf D, Miguel R, Pitts M, et al. A multicentric evaluation of total intravenous with remifentanil and propofol for elective inpatient surgery. Anesth Analg 1996;83:279-85.
- Eger EL II. Inhaled anaesthetics: uptake and distribution. In: Miller RD, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Young WL, eds. Miller’s Anaesthesia. 7th ed.Philadelphia: Churchill Livingstone Elsevier; 2010:539-59.
- Mielck F, Stephan H, Buhre W, Weyland A, Sonntag H. Effects of 1MAC desflurane on cerebral metabolism, blood flow and carbon dioxide reactivity in humans. Br J Anaesth 1998;81:155-60.
- Safavi M, Honarmand A. Influence of head flexion after endotracheal intubation on intraocular pressure and cardio-respiratory response in patients undergoing cataract surgery. Ghana Med J. 2008 Sep;42(3):105-9.
- Enlund M, Hassan HG. Intraoperative awareness: Detected by the structured Brice interview? Acta Anaesthesiol Scand 2002 Apr;46(4):345-9.
- Magni G, Baisi F, Rosa I La, Imperiale C, Fabbrini V, Pennacchiotti ML, et al. No difference in emergence time and early cognitive function between sevoflurane –fentanyl and propofol remifentanil in patients undergoing craniotomy for supratentorial intracranial surgery. J Neurosurg Anesthesiol 2005;17:134-8.
- Lauta E, Abbinante C, Gaudio AD, Aloj F, Fanelli M, de Vivo P, et al. Emergence times are similar with sevoflurane and total intravenous anesthesia: results of a multicentric RCT of patients scheduled for elective supratentorial craniotomy. J Neurosurg Anesthesiol. 2010 Apr;22(2):110-8.
[PubMed] doi: 10.1097/ANA.0b013e3181c959da.
- Sneyd JR, Andrews CJ, Tsubokawa T. Comparison of propofol/remifentanil and sevoflurane/remifentanil for maintenance of anesthesia for elective intracranial surgery. Br J Anaesth 2005 Jun;94(6):778-83.
[PubMed] [Free full text] Epub 2005 Apr 15.
- Bastola P, Bhagat H, Wig J. Comparative evaluation of propofol, sevoflurane and desflurane for neuroanaesthesia: A prospective randomised study in patients undergoing elective supratentorial craniotomy. Indian J Anaesth. 2015 May;59(5):287-94.
[PubMed] [Free full text] doi: 10.4103/0019-5049.156868.
- Bhagat H, Dash HH, Bithal PK, Chouhan RS, Pandia MP. Planning for early emergence in neurosurgical patients: A randomized trial of low dose anesthetics. Anesth Analg. 2008;107:1348–55.
- Todd MM, Warner DS, Maktabi MA, et al . Neuroanaesthesia. In: Longnecker DE, Brown DL, Newman MF, Zapol WM eds. Anaesthesiology.6th ed. Newyork: Mc Graw Hill; 2008:1081-139.
- Signore L, Filipo R, Barbara M, D’Ercole P, D’Ercole P, Cordier A, Maisano C. Anesthesiological methods in acoustic neuroma surgery using translabyrinthine approach. Acta Otorhinolaryngol Ital 1993;13:13-20.
- Huges MA, Jacobs JR, Glass PSA. Context-sensitive half time in multicompartment pharmacokinetic models for intravenous anaesthetic drugs. Anesthesiology 1992;76:334-41.
- Boisson-Bertrand D, Laxenaire MC, Mertes PM. Recovery after prolonged Anesthesia for acoustic neuroma surgery: desflurane versus isoflurane. Anaesth Intensive Care 2006; 34:338-42.
- Minogue SC, Ralph J, Lampa MJ. Laryngotracheal topicalization with lidocaine before intubation decreases the incidence of coughing on emergence from general anesthesia. Anesth Analg. 2004; 99:1253-7.
- Widdicombe JG. Afferent receptors in the airway and cough. Respir Physiol. 1998 Oct; 114(1):5-15.
- Shimizu S, Sato K, Mabuchi I, Utsuki S, Oka H, Kan S, et al. Brachial plexopathy due to massive swelling of the neck associated with craniotomy in the park bench position. Surg Neurol 2009;71:504-8 .
[PubMed] doi: 10.1016/j.surneu.2007.08.043.
