
Muhammad Saleh Khaskheli, FCPS, MSc (Pain Medicine)*, Bashir Ahmed Khuhro**, Abdul Hakeem Jamali***
*Associate Professor & Chairman, Anaesthesia, SICU and Pain
**Consultant Physician
***Assistant Professor, Surgical Unit-I, Department of surgery
PMUMH Nawabshah (Pakistan)
Correspondence: Dr. Muhammad Saleh Khakheli, Associate Professor & Chairman, Anaesthesia, SICU and Pain, PMUMH Nawabshah (Pakistan)
ABSTRACT
Objective: To determine the socio-demographic characteristics, clinical profile and outcome of the tetanus patients.
Study Design: Case Series
Place and duration of Study: SICU of Peoples University of Medical and Health sciences (PUMHS) Nawabshah, from January 2010 to December 2012.
Methodology: The information obtained from the attendants of patients who presented with clinical features of tetanus and classified into generalized and cephalic types and; severity was classified into mild, moderate severe and very severe. Treatment was started immediately with protocol of supportive care; neutralization of circulating toxin and eradication of the source of tetanospasmin. Details of socio-demographic data, clinical features, complications and outcome were recorded and entered in a questionnaire before analysis.
Results: twenty two cases of tetanus were studied included males were 16 and females were 6. Six of 22 (27.3%) patients had prior tetanus immunization while the other sixteen (72.7%) patients were not vaccinated or did not know their tetanus immunization status. Lower limbs were most common of portal of entry 15 (68.2%). Most of patients (95.5%) have generalized tetanus and 5 (22.7%) patients had very severe disease. Body stiffness/spasm (100%), trismus (100%) and dysphagia (68.2%) were the three commonest presenting complaints. Complications of tetanus were documented in 16 (72.7%) patients. Overall mortality was 68.2 %.
Conclusion: Tetanus prevalence is still high in interior Sind and is associated with high morbidity and mortality rate.
Key words: Tetanus; Tetanospasmin; Mortality; Mortality rate; Universal primary immunization
Citation: Khaskheli MS, Khuhro BA, Jamali AH.Tetanus: still a killer in adults. Anaesth Pain & intensive Care 2013;17(2):149-153
INTRODUCTION
Tetanus is a neurological disorder, characterized by increased muscle tone and spasms that is caused by tetanospasmin, a powerful protein toxin elaborated by Clostridium tetani.1 Since the introduction of active immunization in 1940; it has become an old forgotten disease in the developed countries.2 But it still remains an important cause of death in most developing countries.3
In the developing countries tetanus is common in adults due to lack of effective immunization program, inappropriate treatment of injuries4 and decline in protective antibodies in elderly.5,6
The global incidence of tetanus is still estimated at one million cases annually, with a case fatality ratio ranging from 6% to 72% depending on the availability of well equipped intensive care unit.7 About one million cases of tetanus occur annually worldwide,8 resulting in death of about half a million people each year.9 Mortality from tetanus approaches close to fifty percent in developing countries like Pakistan.
Tetanus occurs sporadically and almost always affects non-immunized, partially immunized, or fully immunized persons who fail to maintain adequate immunity with booster doses of vaccine.11, 12 It is therefore very important, in order to have protection against tetanus, that all age groups have the universal primary immunization with subsequent maintenance of adequate antitoxin levels by means of appropriately timed boosters.12, 13
Four clinical forms of tetanus are recognized and they include generalized, localized, cephalic and neonatal tetanus.11-14 Spasm related respiratory compromise, hospital acquired pneumonia and autonomic instability is usually the main causes of morbidity and mortality of this disease.14,15 The diagnosis of tetanus is based entirely on clinical findings.1
In Pakistan, like in most of the developing countries in the world, tetanus is endemic and it remains a public health problem even today. The objective of this study was to know the socio-demographic characteristics and the clinical profile, as well as the outcome of the tetanus patients who were admitted at ICU of Peoples University of Medical and Health sciences Hospital Nawabshah Pakistan.
METHODOLOGY
This was descriptive case series study done at ICU department of Peoples Medical College Hospital (PMCH) Nawabshah for period of three years between January 2010 and December 2012. PMCH is tertiary care teaching hospital for the Peoples University of Medical and Health Sciences Nawabshsah (PUMHS). The hospital has a 08-bed adult multi-disciplinary Intensive Care Unit (ICU) which is headed by a consultant anaesthesiologist and run by trained ICU staff. Tetanus patients are usually referred from medical, surgical and Gyne/Obs departments. Ethical approval to study was obtained from the PUMHS ethics review committee.
The study included adult patients of more 15 years of age who presented with clinical features of tetanus that was diagnosed clinically and based on the presence of one or more of the following:-
1. Trismus
2. Rigidity of the neck and or abdomen
3. Reflex spasms
Tetanus was classified into generalized and cephalic types. Patients with trismus and generalized rigidity with or without generalized spasms were classified as having generalized tetanus. Tetanus restricted to head and neck was classified as cephalic tetanus. After diagnosis the severity was classified into mild, moderate severe and very severe according to the system reported by Ablett16 and treatment was started immediately with three objectives i.e. supportive care; neutralization of circulating toxin and eradication of the source of tetanospasmin. Almost all patients were managed with tetanus toxoid, human tetanus immunoglobulin, Magnesium sulphate, antibiotic therapy (penicillin and metronidazole), wound care (wound toilet and debridement), muscle relaxants Acetaminophen a skeletal muscle relaxant, sedatives, heparin prophylaxis and artificial ventilation. Supportive treatment such as balanced fluid and calorie intake prevention of gastric stress ulcer, prevention of pressure sores were provided in all patients.
Details of demographic data (age, sex, occupation), tetanus immunization history, suspected portal of entry of infection, clinical presentations, management, related complications, duration of intensive care unit admission, length of hospitalization, and outcome were recorded and entered in a questionnaire before analysis.
The statistical analysis was performed using statistical package for social sciences (SPSS) version 15.0. The mean ± standard deviation (SD), median and ranges were calculated for continuous variables whereas proportions and frequency tables were used to summarize categorical variables.
RESULTS
Total 22 cases of tetanus were admitted during the period of study.
Males were 16 (72.7%) and females were 6 (27.3%). Their ages ranged from 12 to 80 years with a mean of 34.54 ± 23.78 years. Fourteen (63.6%) were below 40 years of age, while 08 (36.4%) were aged 40 years and above. The majority of patients were farmers (63.6%) (Table 1).
Table 1: Demographic characteristic of the patients
|
Characteristics |
N(%) |
| Male |
16 (72.7) |
| Female |
6 (27.3) |
| < 40 years |
14 (63.6) |
| > 40 years |
8 (36.4) |
| Occupation
Farmer Labourer Housewife Student |
12(54.5) 3(13.6) 4(18.2) 3(13.6) |
| Immunization status
Vaccinated Not Vaccinated |
6 (27.3) 16 (72.7) |
| Portal of Injury
Lower Limb Upper or others |
12(54.5) 3(13.6) |
Regarding history of tetanus immunization status only six (27.3%) patients had prior tetanus immunization but no documentary proof, while the other sixteen (72.7%) patients were not vaccinated or did not know their tetanus immunization status.
Lower limbs were most common of portal of entry 15 (68.2%) and prick, laceration, burns were the most common injuries. The portals of entry were not identified in 31.8% of cases (Table 1).
Twenty one (95.5%) patients had generalized tetanus and only one (4.5%) patient had localized tetanus. Regarding the severity according to Ablett classification system five (22.7%) patients had very severe disease (Table 2).
Table 2: Clinical parameters
|
Characteristics |
DATA |
| Pulse (mean ± SD) |
101.95 ± 42.76 |
| Blood Pressure (mean ± SD)
Systolic Diastolic |
113.95 ± 44.54 72.81 ± 26.63 |
| Temperature (mean ± SD) |
89.54 ± 29.02 |
| O2 Saturation (mean ± SD) |
85.68 ± 27.95 |
| Severity [n(%)]
Mild Moderate Severe Very Severe |
2 (9.1) 5 (22.7) 10 (45.5) 5 (22.7) |
| Symptoms [n(%)]
Body stiffness/spasm Trismus Dysphagia Fever Body aches Backache Headache Abdominal pain Shortness of breath Chest pain |
22 (100) 22 (100) 22 (100) 3 (13.6) 9 (40.9) 04 (18.2) 3 (13.6) 02 (9.1) 02 (9.1) 01(4.5) |
Body stiffness/spasm (100%), trismus (100%) and dysphagia (68.2%) were the three commonest presenting complaints (Table 2).
Initially all the patients who were admitted in the ICU did not required ventilatory support. The tracheostomy was done in only 6 (27.3%) cases that developed severe pneumonia and respiratory failure and required ventilator support. The average days on ventilatory support were 17 days (1-26 days).
Complications of tetanus were documented in 16 (72.7%) patients. Pneumonia, respiratory failure developed in 08 (36.4%) patients, cardiovascular in 3 (13.6%), renal complications (renal failure) in 1 (4.5%), neurological complications (seizures) in 02 (9.1%).
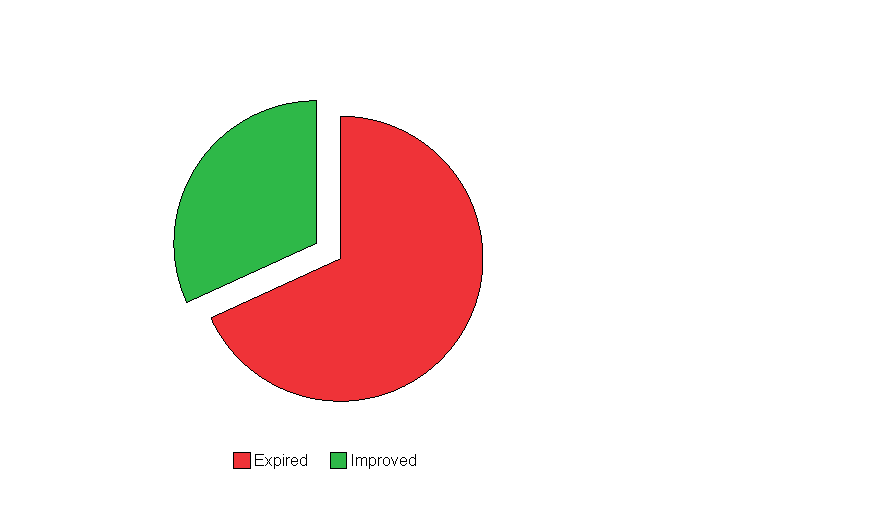
Of the 22 patients, 7 (31.8%) patients improved and discharged and fifteen patients expired accounting for an overall mortality of 68.2 %.( Figure 1) Majority of the deaths occurred in the first few days; six died in the first 05 days. ATG received by all survivors and 7 (31.8%) of expired persons didn’t receive ATG due to unavailability.
Figure 1: Outcome of the 22 tetanus patients
Mean duration of ICU stay was 8.63 ± 9.41 days (1-34 days). The mean duration of hospitalization for survivors was 13.00 with median of 6.00 days.
DISCUSSION
Tetanus, though not uncommon, carries high morbidity and mortality despite availability of effective vaccines in developing countries.3,18,19 Our study reflects this observation that majority (72.7%) of our patients were not vaccinated or did not know their tetanus immunization status. This high incidence of tetanus in our country and other developing countries is likely due to low levels of health awareness and unavailability of resources to manage the disease.4.5 this finding calls for wide immunization campaign and health education to reduce the incidence of this disease.
Our study showed that most of patients were male as reflected in other national and international studies.6,11,13-15,19-21 This could be explained as follows: First that men spend more time in outdoor like farming activities and other types of field work and more prone to penetrating injuries. Hence, they are more likely to be exposed to causative organism, C. tetani, which is ever-present in soil in a tropical country like Pakistan. Second, low vaccination rates among males in the community as compared to females and children who gets their vaccination during pregnancy and childhood respectively. Health education in the regard of vaccination among males as well as females is highly needed to prevent from contracting this serious disease.
In our study the tetanus patients were quite young as observed by most of studies in developing counties14,15,17,18,20,21 but studies in developed countries observed tetanus in older patients.11,14 This observation can be explained by the fact that in developing countries tetanus is common in the young due to lack of effective immunization program and inappropriate treatment of injuries.4,13 whereas in developed countries tetanus occurs mainly in elderly due to decline in protective antibodies.5,6
In our study majority of the tetanus patients (54.5%) were farmers as observed in other national and international studies.6,14,15,18-20 But one study in Nigeria reported students and civil servants as the majority of cases.24 This pattern of occupational risk group in our study can be explained by the fact that farmers are more likely to be exposed to the causal organism as they works in the fields.
The most common portal of entry in this study was injuries in the lower limbs injuries as observed by other studies.11,18,21,22 This is in contrast to Joshi et al15 who reported upper limbs as the most common portal of entry. This lower limb predominance in this study could be explained by the fact that C. tetani exists in soil; hence, any lower limb injury would be open to contamination and infection by this organism, bearing in mind that most tetanus patients were farmers. Also, the predominance of lower limbs in our study is thought to be result from poor protective footwear. The portals of entry were not identified in 31.8% of cases reflecting that the injuries were likely to be trivial to be recalled. Trivial wounds on the lower limbs as possible portals of entry for tetanus infection are common because most people in the rural areas do not wear shoes.
Body stiffness/spasm, trismus and dysphagia were observed in all tetanus patients in our series as observed in other studies.4,11,14 Hence, a high index of suspicion for tetanus is vital whenever patients present with any of these symptoms; as tetanus is essentially a clinical diagnosis and laboratory results as well as cultures are of little diagnostic value.5
In this study tracheostomy was performed in only 36.4% of patients for ventilatory support which is in contrast with other studies which reported that all tetanus patients underwent tracheostomy.11,24 The tracheostomy in the management of tetanus patients, especially in severe condition, will undoubtedly prevent death due to asphyxia from laryngeal muscle spasm, respiratory muscle spasm and aspiration.25 The low rate of tracheostomy in our study may be responsible for high mortality rate among tetanus patients.
Complication rate in our study were high as compared to other studies.6, 14 However, the presence of complication did not significantly affect the outcome of tetanus patients. Our complication pattern was fairly similar to what was reported by Feroz and Rahman in Bangladesh.18 We could not find any obvious reason in literature to explain this similarity. Much attention must therefore be paid to prevent these complications through early diagnosis and management and possibly lethal bugs in our ICU resulted in nosocomial severe pneumonia that leads to respiratory failure.
The outcome of patients with tetanus has been reported variably. Overall, mortality is approximately 10-50%, however in certain age groups e.g. neonates it is as high as 90-95%.26 in this study, mortality rate was very high 68.2%, as compared to other national and international studies. Mahsud et al20 observed 19.3% at D. I. Khan, KPK Pakistan, Mohammed et al27 and Chalya et al19 showed similar mortality rate, whereas Mchembe & Mwafongo13 in Tanzania have reported higher mortality rate of 72.7% The high mortality rate could be due to the gross inadequacy of human and material resources to manage severe tetanus in the intensive care units, typical of developing countries. Various factors have been known to affect the prognosis.15 The poor prognostic factors in this study included age ≥ 40 years, nosocomial pneumonia severity of tetanus and very late arrival. Most of the deaths in our series were attributed to pulmonary and cardiac complications as observed in other studies.18,28
In our study, only 31.8% of the patients were cured who received tetanus toxoid before discharged as other studies showed.28 This finding calls for a need to provide health education on primary immunization and scheduled booster immunization that have greatly found to reduce the incidence of tetanus.
The overall mean duration of hospital stay in this study was 8.63 ± 9.41 days (1-34 days) which is almost same as compared to other studies.13,11,15,22 In one study, the overall mean duration of hospital stay was 83.0 days.8 Chalya et al19 observed an average ICU stay of 19.3 days (range 1-26 days). Prolonged duration of hospital stay has an impact on hospital resources as well as on increased cost of health care, loss of productivity and reduced quality of life.
CONCLUSION
Tetanus is still not an uncommon disease in our setting, although it is a totally preventable disease and is associated with very high morbidity and mortality. Males, especially the farmers, are commonly affected. The incidence of tetanus can be reduced significantly by an effective immunization program especially in the farmers and proper wound management of the injured as well as public awareness programmes.
Acknowledgements
We are grateful to house officers in the ICU for their support in data collection. We also like to thank all ICU staff for their cordial help during this study.
Authors’ contributions
1) Khaskheli MS designed the study and arranged submission of the manuscript. Supervised the write up of the manuscript and editing of the manuscript.
2) Khuhro BA Contributed in literature search, data analysis, manuscript writing and editing
3) Jamali AH participated in study design, participated in study design, and edited the manuscript before submission.
All the authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
REFERENCES
- Brian S Schwartz. Tetanus, Bacterial and Chlamydial infections. In: Papadakis MA, McPhee SJ, editors. Current Medical Diagnosis and Treatment 52nd Edition, San Francisco, Mc Graw-Hill 2013: 1429-30.
- Bleck TP. Clostridium Tetani. In: Mandell GL, Bennett JE, Dolin R, editors. In: Principles and Practices of Infectious Diseases. 6th edition. vol 2. Philadelphia: Churchill Livingstone; 2005. pp. 2817–22.
- Dietz V, Milstien JB, van Loon F, Cochi S, Bennett J. Performance and potency of tetanus toxoid: implications for eliminating neonatal tetanus. Bull WHO 1996, 74:619-28. [PubMed] [Free Full Text]
- Sandford JP: Tetanus-Forgotten but not gone. N Engl J Med 1995, 332:812-3. [PubMed] [Free Full Text]
- Amare A1, Yami A: Case-fatality of adult Tetanus at Jimma University Teaching Hospital, Southwest Ethiopia. African Health Sciences 2011, 11(1):36-40. [PubMed] [Free Full Text]
- Oladiran I, Meier DE, Ojelade AA, Olaolorun DA, Adeniran A, Tarpley JL: Tetanus: Continuing problem in the developing world. World J Surg 2002, 26(10):1282-85. [PubMed]
- Mirinda-Fiho DB, Alencar Ximenes RA, Barour AA, Vaz VL, Vieira AG, Goncalves-Albuquerque VM. Randomized control trial of tetanus treatment with ant tetanus immunoglobulin by the intrathecal or intramuscular route. BMJ 2004; 328: 615. [PubMed] [Free Full Text]
- Tahery J, Morris DP, Birzgalis AR. Tetanus: The Forgotten Disease. A rare cause of dysphagia and trismus. J laryngol Otol 2004; 118: 974–76. [PubMed]
- Khichi GQ. Tetanus neonatorum in Bahawalpur. Pak Paed J 1997; 21:31-6. [Pakmedinet]
- Lau LG, Kong KO, Chew PH: A ten-year retrospective study of tetanus at a general hospital in Malaysia. Singapore Med J 2001, 42(8):346-50. [PubMed]
- Edlich RF, Hill LG, Mahler CA, Cox MJ, Becker DG, Horowitz JH: Management and prevention of tetanus. J Long Term Eff Med Implants 2003, 13(3):139-54. [PubMed]
- Mchembe MD, Mwafongo V: Tetanus and its treatment outcome in Dar es Salaam: need for male vaccination. East African Journal of Public Health 2005,2: 22-23. [Publisher’s Abstract]
- Younas NJ, Abro AH, Das K, Abdou AMS, Ustadi AM, Afzal S: Tetanus: Presentation and outcome in adults. Pak J Med Sci 2009, 25(5):760-65. [Publisher’s Abstract] [Free Full Text]
- Joshi S, Agarwal B, Malla G, Karmacharya B: Complete elimination of tetanus is still elusive in developing countries: a review of adult tetanus cases from referral hospital in Eastern Nepal. Kathmandu Univ Med J (KUMJ) 2007, 5(3):378-81. [PubMed]
- Ablett JJL: Analysis and main experience in 82 patients treated in Leeds tetanus unit. Edited by: Ellis M. In: Symposium on tetanus in Great Britain. Leeds; 1967:1.
- Anuradha S: Tetanus in adults-A continuing problem: An analysis of 217patients over 3 years from Delhi, India, with special emphasis on predictors of mortality. Med J Malaysia 2006, 61(1):7-14. [PubMed]
- Feroz AHM, Rahman MH: A Ten-year Retrospective Study of Tetanus at a Teaching hospital in Bangladesh. J Bangladesh Coll Phys Surg 2007, 25:62-9. [Publisher’s Abstract] [Free Full Text]
- Chalya PL, Joseph BM, Ramesh MD, Nkinda M, Stephen EM, Japhet MG. A 10-year experience with Tetanus at a tertiary hospital in north western Tanzania: A retrospective review of 102 cases. World Journal of Emergency Surgery. 2011; 6:20. [PubMed] [Free Full Text]
- Mahsud IU, Khan HU, Khattak AM, Wazir FU, Shah SH. Mortality rate in adult tetanus patients in district D. I. Khan, NWFP- Pakistan. Biomedica July-Dec 2005, 21: 86-9. [Pakmedinet] [Free Full Text]
- Iqbal S, Iman N, Rahman S, Haroon M. Trends of tetanus patients in north of patients in north of Pakistan. j. med. sci. 2012, 20:2: 90-3. [Publisher’s Abstract] [Free Full Text]
- Qadir M, Murad R, Mumtaz S, Azmi AA, Rehman R, Hani O, Aziz N. Frequency Of Tetanus Toxoid Immunization Among College/University Female Students Of Karachi. J Ayub Med Coll Abbottabad 2010; 22(1): 147-49. [PubMed]
- Naeem M, Zia-Ul-Islam M, Abbas SH, Adil M, Khan A, Naz SM, Khan MU . Coverage And Factors Associated With Tetanus Toxoid Vaccination Among Married Women Of Reproductive Age: A Cross Sectional Study In Peshawar. J Ayub Med Coll Abbottabad 2010; 22(3): 136-40. [PubMed]
- Chukwubike OA, God’spower AE: A 10-year review of outcome of management of tetanus in adults at a Nigerian tertiary hospital. Ann Afr Med 2009, 8(3):168-72. [PubMed] [Free Full Text]
- Fasunla AJ: Challenges of Tracheostomy in Patients Managed for Severe Tetanus in a Developing Country. Int J Prev Med 2010, 1(3):176-81. [PubMed] [Free Full Text]
- Bhatia R, Parbharkar S, Grover VK: Tetanus. Neurol India 2002, 50:398-407. [PubMed]
- Mohammed W, Bhojo AK, Nashaa T, Rohma S, Nadir AS, Aseem S: Autonomic nervous system dysfunction predicts poor prognosis in patients with mild to moderate tetanus. BMC Neurology 2005, 5:2. [PubMed] [Free Full Text]
- Galazka A, Gasse F. The present status of tetanus and tetanus vaccination. Curr Top Microbiol Immunol. 1995; 195:31–53. [PubMed]
- Zziwa GB: Review of tetanus admissions to a rural Ugandan Hospital.UMU press; 2009:7(3):199-202. [Publisher’s Abstract] [Free Full Text]
