
Medhat Hannallah, MD, FFARCS*, Michael Rasmussen, MD**, John Carroll, MD***,
Aline Charabaty, MD***, Caren Palese, MD***, Nadeem Haddad, MD****
*Professor, **Senior Resident
Department of Anesthesiology, Georgetown University Hospital, Washington, DC (USA).
***Assistant Professor, ****Associate professor
Department of Medicine, Division of Gastroenterology, Georgetown University Hospital, Washington, DC (USA).
Correspondence: Medhat Hannallah, MD, FFARCS, Department of Anesthesiology, Georgetown University Hospital, 3800 Reservoir Road, SW, Washington DC, 20007, (USA); Phone: 202-444-6680; Email: hannallm@gunet.georgetown.edu
ABSTRACT
Background: Dexmedetomidine provides sedation with minimal respiratory depression which is a desirable characteristic in patients with obstructive sleep apnea (OSA). This observational study prospectively evaluated the efficacy and safety of dexmedetomidine/ propofol anesthesia for patients with OSA characteristics without endotracheal intubation during upper gastrointestinal(GI) endoscopy.
Methodology: Twenty patients undergoing upper GI endoscopy who were considered high probability of having OSA based on an adjusted neck circumference greater than 48 were enrolled in the study. Dexmedetomidine 1 mcg/kg bolus was given over 10 min followed by propofol boluses until adequate depth of anesthesia was achieved. Propofol infusion was used to maintain anesthesia. Blood pressure, heart rate, and O2 saturation were recorded before, during, and after the procedure. The endoscopists evaluated the anesthesia condition on a 10 points numerical scale. Post-Anesthesia Care Unit (PACU) time was recorded. The following day, patients were questioned about complications and were asked to evaluate their overall anesthesia experience on a 10 points numerical scale.
Results: Fifteen males and five females aged 51 ± 8 years were enrolled. Their BMI was 34.7 ± 8.4, and their adjusted neck circumference was 53.4 ± 3.4. Propofol induction dose was 0.8 ± 0.4 mg/kg; and PACU time was 67.5 ± 26.7 min. Two patients developed transient hypoxemic episodes during the procedure. Transient hypotension was experienced by three patients during the procedure and three patients in PACU. The evaluation score was 9 ± 1.7 by the endoscopists, and 8 ± 2.3 by the patients. After discharge, 16 patients complained of drowsiness, two patients reported dysphoric symptoms, and one patient complained of dry mouth.
Conclusions: Dexmedetomidine / propofol combination can provide satisfactory anesthesia for upper GI endoscopy in OSA patients. The technique provides an alternative to endotracheal intubation in these high risk patients. The prolonged induction and recovery times, however, may limit its routine use.
Keywords: Propofol; Dexmedetomidine; Sedation for endoscopy
Citation: Hannallah M, Rasmussen M, Carroll J, Charabaty A, Palese C, Haddad N. Evaluation of dexmedetomidine/propofol anesthesia during upper gastrointestinal endoscopy in patients with high probability of having obstructive sleep apnea. Anaesth Pain & Intensive Care 2013;17(3):258-260
INTRODUCTION
Patients with obstructive sleep apnea (OSA) are at increased risk of anesthesia-related morbidity and mortality.1,2 Providing anesthesia to these patients during upper gastrointestinsal(GI) endoscopy is particularly challanging. The literature provides only general guidelines about the anesthetic management of OSA patients during upper GI endoscopy. The American Society of Anesthesiologists practice guidelines for the perioperative management of patients with OSA states that general anesthesia with a secure airway is preferable to deep sedation without a secure airway in these patients, particularly for procedures that may mechanically compromise the airway.3 Upper GI endoscopy falls under such category of procedures. Endotracheal intubation of OSA patients, however, is not without its own risks, particularly if performed in a minimally equipped outpatient facility. Dexmedetomidine, an α2 agonist, provides sedation with minimal respiratory depression.4-6 It also has analgesic and antisialagogue properties which are desirable for cases involved with airway instrumentation. Dexmedetomidine has been successfully used during awake fiberoptic intubation, monitored anesthesia care and as a supplement to general anesthesia.7-9 Propofol has been widely and effectively used as a sedative agent during GI endoscopy.10 This observational study prospectively evaluated the efficacy and safety of dexmedetomidine/propofol anesthesia without endotracheal intubation for patients with high probability of having OSA undergoing upper GI endoscopy. It is the first study to provide detailed description of the technique.
METHODOLOGY
With IRB approval and written informed consent, 20 outpatients undergoing upper GI endoscopy alone or with ultrasound examination, Barrx procedure, or colonoscopy were enrolled in the study. All patients were considered high probability of having OSA based on an adjusted neck circumference greater than 48.11 (Table 1) Exclusion criteria included inpatient status, age <18 yr or >65 yr, unstable or life-threatening medical conditions, liver disease, heart rate < 60 BPM, systolic BP < 100 mmHg, EKG changes suggestive of conduction abnormalities, opioids use, pregnancy, and allergy to propofol, dexmedetomidine, eggs or soybean. An intravenous line was started and routine monitors (BP, EKG, pulse oximetry, and capnography) were applied to the patients. Supplemental oxygen was delivered by nasal cannula. Dexmedetomidine 1 µg/kg (maximum 100 µg) was given over 10 min intravenously. The patients were then turned onto the left lateral decubitus position and bite blocks were placed between the teeth. Propofol was given in small intravenous boluses until the patients were judged to be adequately anesthetized for the procedure to start. The depth of anesthesia was tested by inserting a soft rubber nasal airway deep into the oral cavity. Propofol infusion rate was titrated and additional propofol boluses were given at the discretion of the anesthesiologist to maintain adequate depth of anesthesia during the procedure based on observation of patients’ movement, vital signs, and respiratory status. Various airway maneuvers including chin lift, jaw thrust, insertion of a nasal airway, or mask ventilation were used if needed to maintain adequate ventilation and oxygenation. Blood pressure, heart rate, and O2 saturation were recorded before, during, and after the procedure. The lowest systolic blood pressure, heart rate, and oxygen saturation readings were noted. At the conclusion of the procedures, the endoscopists evaluated the anesthesia conditions on a 10 points numerical scale (‘10’ is for perfect conditions with no patient response or movement, and ‘1’ is for the worst conditions where excessive patient response and movement caused frequent interruption of the procedure). The duration of the procedures and the propofol dose used were recorded. At the conclusion of the procedures, the patients were transferred to the endoscopy suite Post Anesthesia Care Unit (PACU) where they were monitored during their recovery period. The PACU nurses were asked to follow the routine recovery and discharge protocols. The patients were discharged from PACU at the discretion of the recovery nurses when all discharge criteria were met. PACU time (time between the end of anesthesia and the patients’ arrival at the discharge area) were recorded. The following day, the patients received a follow-up call and were questioned about complications such as nausea, vomiting or drowsiness. They were asked to evaluate their overall anesthesia experience on a 10 points numerical scale (10 is for perfect). Patients who had received anesthesia for previous GI procedures were asked to compare the 2 experiences, and attempts were made to obtain the previous anesthesia records.
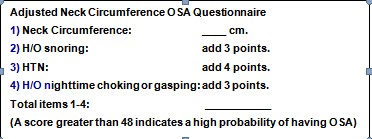
Box 1: Adjusted Neck Circumference OSA Questionnaire11
RESULTS
Fifteen males and five females aged 51 ± 8 years were enrolled. Their BMI was 34.7 ± 8.4 kg/m2 (range 22 – 62 kg/m2); and their adjusted neck circumference was 53.4 ± 3.4 (range 50 – 63). Seven had definitive OSA diagnoses. Propofol induction dose was 0.8 ± 0.4 mg/kg (range 0.2 – 1.8 mg/kg); and PACU time was 67.5 ± 26.7 min (range 26 – 134 min). In thirteen patients a nasal airway was used to maintain a patent airway. Two patients developed transient hypoxemic episodes (O2 saturation < 85%) during the procedure; one was corrected by jaw thrust and insertion of a nasal airway, and the other required mask ventilation using an Ambu bag. Transient hypotension (systolic blood pressure < 90 mmHg) requiring vasopressors support was experienced by 3 patients during the procedure and 3 patients in PACU. No patient developed heart rate < 45 beats per minute. The evaluation score was 9 ± 1.7 (range 4 -10) by the endoscopists; and 8 ± 2.3 (range 1 – 10) by the patients. Post-discharge, 16 patients complained of drowsiness, 2 patients reported dysphoric symptoms, and one patient complained of dry mouth. We were able to obtain the anesthesia records of seven patients during previous GI procedures. For 2 patients the two experiences were comparable, for 3 patients the previous experience was better, and for 2 patients the dexmedetomidine/propofol experience was better (Details in Table 2).
Box 2:Patients who had previous upper GI endoscopy with recoverable anesthetic data.
|
Table 3: Propofol Induction Dose and Phase 1 Time
DISCUSSION
The prevalence of gastroesophageal reflux disease (GERD) is higher in patients with OSA than in the general population.12 This could be explained by the fact that obesity is a key risk factor for both OSA and GERD.13 Patients with OSA, therefore, frequently present for diagnostic and/or therapeutic upper gastrointestinal (GI) endoscopy. Since these patients are at increased risk of anesthesia-related morbidity and mortality, anesthetizing them during upper GI endoscopy is particularly challenging.
The American Society of Anesthesiologists practice guidelines for the perioperative management of patients with OSA states that general anesthesia with a secure airway is preferable for procedures that may mechanically compromise the airway such as upper GI endoscopy. Endotracheal intubation of OSA patients, however, is not without its own risks, particularly if performed in a minimally equipped outpatient facility. It would be advantageous, therefore, to utilize an anesthetic technique that can maintain OSA patients’ airway and ventilation without endotracheal intubation during upper GI endoscopy. In this study we evaluated such a technique based on the combined administration of dexmedetomidine and propofol. Dexmedetomidine provides sedation without respiratory depression, a characteristic that could make it particularly suitable for sedating OSA patients. In addition, it has analgesic and anti-sialagogue properties which are desirable for cases involved with airway instrumentation. In our experience, the 1 µg/kg bolus of dexmedetomidine does not provide adequate sedation on its own for upper GI endoscopy. Propofol was, therefore, used to supplement dexmedetomidine. The initial bolus was not followed by a continuous dexmedetomidine infusion since the duration of the initial loading dose of dexmedetomidine outlasts the short duration of these procedures.
Dexmedetomidine/propofol combination was generally effective in providing anesthesia without endotracheal intubation in these high risk patients. The fact that most patients required some airway support is not surprising considering the fact that OSA patients develop airway obstruction during their natural sleep. Needless to say rescue plans and airway devices should be immediately available.
Hypotension or hypertension can result from the use of α2 agonists.5 At lower doses, the dominant action of α2 agonists is sympatholysis mediated by the α2A adrenergic receptor subtype. At higher doses of α2 agonists, such as those achieved by rapid IV administration, hypertension dominates by activation of α2B adrenoceptors, located on smooth muscle cells in resistance vessels. It is, therefore, recommended, that loading boluses of dexmedetomidine be administered slowly. The 10 min induction time delayed the start of the procedures and was the endoscopists’ major issue with the technique.
PACU time in this study is considerably longer than our routine PACU time when propofol alone is used. In a previous IRB approved study performed at our hospital, propofol was the sole anesthetic used in 16 patients without OSA undergoing upper GI endoscopy. In that study the PACU time was 33.4 ± 5.9 min (range 23 – 46 min). This is half the PACU time in the current study. Prolonged sleepiness was the main reason for the delayed discharge from PACU when dexmedetomidine was used. The treatment of hypotension in 3 patients might have contributed to the delay in their discharge. The prolonged PACU stay following dexmedetomidine can be a major drawback in a busy outpatient facility.
Prolonged drowsiness at home was a major disadvantage of the technique from the patients’ perspective. Some patients, nonetheless, thought that drowsiness was preferable to the bitter taste of viscous lidocaine or to the aftereffects of endotracheal intubation.
It is difficult to explain the dysphoria that two patients experienced following dexmedetomidine/propofol anesthesia. In a study that sought to determine the response to increasing plasma concentrations of dexmedetomidine in volunteers, one subject developed relatively profound and unexplained agitation that necessitated discontinuation of the infusion.4 The potential of dexmedetomidine to cause dysphoria or agitation requires further investigation.
In the aforementioned study, when propofol was used alone, the induction dose was 2.0 ± 0.5 mg/kg, more than double the propofol induction dose when dexmedetomidine was used. This suggests that dexmedetomidine has a significant propofol dose sparing effect.
The Adjusted Neck Circumference OSA screening questionnaire we used in this study has been in use at our institution for many years and is felt to be simple and reliable in identifying patients who are high risk of having OSA. It has not, however, been as extensively validated as the more widely used STOP-Bang questionnaire.14 Further studies are, therefore, needed to validate the sensitivity and specificity of the ‘Adjusted Neck Circumference’ questionnaire.
CONCLUSION
Dexmedetomidine/propofol combination can provide satisfactory anesthesia for upper GI endoscopy in OSA patients. It can minimize the need for endotracheal intubation in these high risk patients and allow the procedure to be more safely performed in minimally equipped outpatient facilities. The technique nonetheless has its limitations and potential side effects. The prolonged induction and recovery times, in particular, may limit its routine use.
REFERENCES
- Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth analg 2008;107:1543-63. [PubMed]
- Kaw R, Pasupuleti V, Walker E, Ramaswamy A, Foldvary-Schafer N. Postoperative complications in patients with obstructive sleep apnea. Chest 2012;141:436-41. [PubMed]
- Practice guidelines for the perioperative management of patients with obstructive sleep apnea. Anesthesiology 2006;104:1081-93.
- Rudra A, Chatterjee S, Das T, Sengupta S, Maitra G, and Kumar P. Obstructive sleep apnoea and anaesthesia. Indian J Crit Care Med. 2008 Jul-Sep; 12(3): 116–123.[Free Full Text]
- Ebert T, Hall J, Barney J, Uhrich T, Colinco M. The effects of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology 2000;93:382-94.
- Kamibayashi T, Maze M. Clinical uses of alpha-2-adrenergic agonists. Anesthesiology.2000;93:1345–9. [PubMed]
- Hall J, Uhrich T, Barney J, Arian S, Ebert TJ. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg 2000;90: 699-795. [PubMed]
- Candiotti KA, Bergese SD, Bokesch PM, Feldman MA, Wisemandle W, Bekker AY. Monitored Anesthesia Care with Dexmedetomidine: A Prospective, Randomized, Double-Blind, Multicenter Trial.Anesth Analg. 2010;110:47–56. [PubMed]
- Hofer RE, Sprung J, Sarr MG, Wedel DJ. Anesthesia for a patient with morbid obesity using dexmedetomidine without narcotics. Can J Anesth 2005;52(2):176-80. [PubMed]
- Scher CS, Gitlin MC. Dexmrdetomidine and low-dose ketamine provide adequate sedation for awake fiberoptic intubation. Can J Anesth2003;50:607-10. [PubMed] [RPD Publicationsm]
- Wang D, Chen C, Chen J, Xu Y, Wang L, Zhu Z, et al. The use of propofol as a sedative agent in gastrointestinal endoscopy: A meta-analysis. PLoS One 2013;8(1): e53311. [PubMed]
- Felmons W. Obstructive sleep apnea. N Engl J Med 2002;347:498-504.[Google Search]
- Ing AJ, Ngu MC, Breslin AB. Obstructive sleep apnea. Am J Med 2000;108:120S-25S.[PubMed]
- Talwar V, Caestecker J. What is the relationship between gastro-esophageal reflux and obstructive sleep apnea? Dig Liver Dis 2006;38:82-4.[Google Search]
- Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score indicates a high probability of obstructive sleep apnea. Br J Anaesth 2012;108:768-75. [PubMed]
