
Lahsaee Masoud, MD*, Kamalipour Hamid, MD**, Ajeli Zahra, MD***, Kamali Karmella, MD****
*Asistant Professor of Anesthesiology, Shiraz Anesthesiology and Critical Care Research Center
**Professor of Anesthesiology, Laparoscopy Research Center
*** Anesthesiologist, Department of Anesthesiology
**** Asistant Professor of Radiology, Department of Radiology
Shiraz University of Medical Sciences, Shiraz (Iran)
Correspondence: Hamid Kamalipour,MD, Professor of Anesthesia, Department of Anesthesiology, Shiraz University of Medical Sciences, P.O.Box:71345-3168, Shiraz (Iran); Phone: +98-917-111-1112; Fax: +98-711-6284828; E-mail:kamalih@yahoo.com
ABSTRACT
Background: Laryngoscopy and endotracheal intubation is usually associated with hemodynamic changes increases in blood pressure and heart rate. We aimed to compare the hemodynamic effects of combined use of low dose thiopentone and propofol during induction of anesthesia with conventional dose of thiopentone and propofol separately.
Methodology: This trialwas conducted prospectively among90 candidates, American Society of Anaesthesiologists grade-l (ASA-I), scheduled for elective surgery, with an age range of 20-50 years. Selected patients were randomly assigned to three equal groups. Thiopentone was used in group 1, propofol in group 2, and a combination of low dose thiopentone and propofol in group 3 as an induction agent.
Heart rate and blood pressures were measured non-invasively at five different times: prior to the injection of study drugs, three minutes after the last injection of induction drug and immediately before the laryngoscopy and endotracheal intubation, as well as at the first, third and fifth minutes after endotracheal intubation.
Results: The adjusted mean values of systolic blood pressure, diastolic blood pressure, and heart rate were assessed by paired comparisons, by considering the variable of time; all changes were significantly different between Groups 1 and 2. Moreover, changes in systolic and diastolic blood pressures were significantly different between Groups 1 and 3. They were not significant for heart rate. No significant difference was documented between Groups 2 and 3; showing that in these groups the hemodynamic changes were small during drug injection, laryngoscopy, and intubation as well as until five minutes after endotracheal intubation.
Conclusion: The combined use of low dose thiopentone and propofol for anesthetic induction caused less hemodynamic changes than the higher dose of either alone. This modality of anesthesia induction may have clinical importance for the elderly patients as well as those with high blood pressure and heart diseases.
Key words: Thiopental; Propofol; Laryngoscopy; Endotracheal intubation; Anesthesia
Citation: Lahsaee M, Kamalipour H, Ajeli Z, Kamali K. A comparison of hemodynamic changes during laryngoscopy and endotracheal intubation by using three modalities of anesthesia induction. Anaesth Pain & Intensive Care 2012;16(3):247-251
INTRODUCTION
Patients undergoing laryngoscopy and endotracheal intubation are known to develop hemodynamic changes such as an increase in blood pressure (BP) and heart rate. In susceptible patients, such changes may lead to myocardial ischemia or a rise in the intracranial pressure.1-5 On the other hand most commonly used induction agents usually lower BP, while producing a tachycardia. Many studies have been conducted to determine the effects of different types of medications on these hemodynamic changes. Generally, multiple medications, including short acting narcotics and hypnotics, may be used during induction and their effects compared.1-6 Thiopentone and propofol are the most commonly used induction agents. The induction dose of thiopentone is 3-5 mg/kg, with dose-dependent hypotension as its usual side effect. The most intense effect of propofol is also hypotension; with an induction dose of 2-2.5 mg/kg it may result in a 25-40 percent drop in arterial pressure.7-9 Reducing the dosages of each of these two medications cannot induce adequate sedation for laryngoscopy and tracheal intubation; moreover, the patient will face hemodynamic problems. A study in 2004, investigated the sedating and hypnotic effects of thiopentone and propofol on two different parts of the brain. Despite similar hypnotic effects, the two drugs caused changes in the regional cerebral blood flow (rCBF). Propofol reduced rCBF in the anterior regions tending to the right side of the brain. Thiopentone initially reduced the rCBF in the cerebellum and the posterior part of brain. The overlapping points increased by the hypnotic dose of these medications.10 Contrary to these findings, another study documented the synergistic effects of propofol and thiopentone during induction of anesthesia.11
Because of controversial findings of previous studies, this trial was conducted to determine the effects of a combination of low dose thiopentone and propofol during induction of anesthesia compared with using the conventional doses of thiopentone or propofol alone.
METHODOLOGY
This trial was conducted in Nemazee, Faghihi, and Chamran hospitals in Shiraz, Southern Iran, from July to December 2010. It was approved by the Ethical Committee of Shiraz University of Medical Sciences. All patients signed informed written consent.
Overall, 90 patients were randomly selected using the table of random numbers from candidates of elective surgery, who were referred to teaching hospitals affiliated to Shiraz University of Medical Sciences. Patients, who were 20-50 years of age, fulfilled the criteria of American Society of Anesthesiologists grade-l (ASA-I), and weighted between 50 to 80 kg, were included in our study. Those with any underlying disease, drug addiction, allergy to eggs or any medications, as well as a family history of acute intermittent porphyria were not included. The airway status of each patient was examined and the patients with possible difficulty in intubation were excluded.
Selected patients were randomly assigned to three equal groups. The difference between these three groups was in the type of the hypnotics used. Thiopentone was used in Group 1, propofol in Group 2, and a combination of thiopentone and propofol in lower dose in Group 3. Table 1 presents the methods of anesthetic induction in the three groups under study.
Table 1: Methods of anesthetic induction in the three groups under study
|
Group 3 |
Group 2 |
Group 1 |
Drug used |
|
0.03 |
0.03 |
0.03 |
Midazolam (mg/kg) |
|
0.1 |
0.1 |
0.1 |
Morphine (mg/kg) |
|
2 |
2 |
2 |
Fentanyl (μg/kg) |
|
20 |
20 |
20 |
Lidocaine (mg) |
|
2.5 |
x |
5 |
Thiopentone (mg/kg) |
|
1.5 |
2.5 |
x |
Propofol (mg/kg) |
|
0.15 |
0.15 |
0.15 |
Cisatracurium (mg/kg) |
To determine the extent of hemodynamic changes during laryngoscopy and endotracheal intubation, the heart rate and blood pressure were measured at five different times: prior to the injection of drugs, three minutes after the last injection of induction drug and immediately before the laryngoscopy and endotracheal intubation, as well as in the first, third, and fifth minutes after endotracheal intubation, the data being collected by anesthesia technician. Those patients who didn’t have adequate relaxation for laryngoscopy were omitted from study.
Intravenous line was inserted, standard monitoring attached, e.g. pulse oximetry, electrocardiography (ECG), and non-invasive BP, and inj. normal saline 5 ml/kg was injected as compensatory volume expansion. Anesthesia was induced by inj. midazolam (0.03 mg/kg), followed by inj. morphine (lento, 0.1 mg/kg), and inj. fentanyl (2 μg/kg).
To relieve the local pain from propofol injection in patients receiving this medication, lidocaine (20 mg) was given to all three groups. Then the hypnotic medications were injected over 2 minutes as described in Table 1, followed by cisatracurium 0.15 mg/kg. Three minutes later, laryngoscopy and endotracheal intubation was performed in less than 30 seconds.
Statistical analysis: Data were analyzed using SPSS software, version 13.0 (SPSS Inc., Chicago, IL, USA). Within group and between group changes in mean blood pressure and heart rate were compared in the five measurements. ANOVA and post-hoc tests were used as appropriate.
RESULTS
The baseline characteristics of patients in the three groups were not significantly different in terms of mean systolic blood pressure, mean diastolic blood pressure, and mean heart rates (Table 2).
Table 2: Comparison of baseline mean systolic and diastolic blood pressures and heart rate between groups (Tukey test)
|
P value |
Standard error |
Mean difference |
Parameter |
Group |
|
0.96 0.77 0.90 |
2.71 2.25 4.29 |
-0.70 -1.53 -1.80 |
DBP HR SBP |
1 & 2 |
|
0.97 0.89 0.73 |
2.71 2.25 4.29 |
+0.53 -1.00 -3.28 |
DBP HR SBP |
1 & 3 |
|
0.89 0.97 0.94 |
2.71 2.25 4.29 |
+1.23 +0.53 -1.43 |
DBP HR SBP |
2 & 3 |
Key: SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate
The mean values of the systolic and diastolic blood pressure, as well as heart rate measured at five different times were analysed (Table 3) and the double comparison done between groups by the use of adjusted mean values (Table 4). The results of collected statistics of the tables show that the process of the changes (by cause and time) between group 1 and 2 had significant difference, also systolic, diastolic blood pressure difference between group 3 and 4 was significant too, but the difference for the mean heart rate was not significant.
The adjusted mean values of systolic blood pressure, diastolic blood pressure, and heart rate were assessed by paired comparisons. As presented in Table 4, by considering the variable of time, the differences in changes were significant between Groups 1 and 2. Moreover, the differences in changes in systolic and diastolic blood pressures
Fig 1: Mean Changes in systolic blood pressure
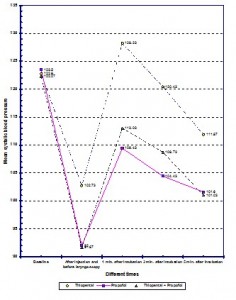
Fig 2: Mean Changes in diastolic blood pressure
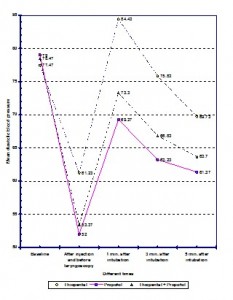
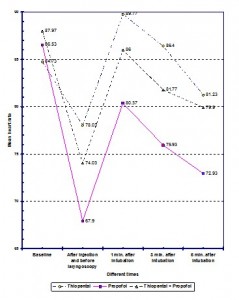 Fig 3: Mean Changes in heart rate
Fig 3: Mean Changes in heart rate
Table 3: Adjusted mean blood pressures and heart rate in the five measurements in the groups studied
|
Std. Error |
Mean (mmHg) |
Parameter |
Group |
|
1.81 1.66 2.05 |
116.88 73.62 84.60 |
SBP DBP HR |
1 |
|
1.82 1.66 2.06 |
106.70 65.13 75.99 |
SBP DBP HR |
2 |
|
1.84 1.68 2.07 |
108.11 67.64 81.69 |
SBP DBP HR |
3 |
Key: SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate
Table 4: Comparison of adjusted mean blood pressures and heart rate in five measurements between the groups
|
P value |
Standard error |
Mean difference |
Parameter |
Group |
|
0.001 0.002 0.013 |
2.59 2.36 2.92 |
+10.18 +8.49 +8.61 |
SBP DBP HR |
1& 2 |
|
0.003 0.040 0.96 |
2.58 2.36 2.92 |
+8.77 +5.98 +2.91 |
SBP DBP HR |
1 & 3 |
|
1.00 0.87 0.16 |
2.58 2.36 2.92 |
-1.41 -2.50 -5.69 |
SBP DBP HR |
2 & 3 |
Key: SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate
DISCUSSION
In this study, the researchers thoroughly benefitted from the findings of previous studies on combinations of low dose thiopentone and propofol for anesthesia induction. The results were compared with the separate use of each drug. Before laryngoscopy, all patients had a reduction in systolic and diastolic blood pressures as well as in heart rate after drug injection, whereas all these variables increased after laryngoscopy and endotracheal intubation. The effects of this increase gradually disappeared within five minutes after intubation. After the drug injection, the patients in group one, had lower decrease in blood pressure and heart rate than groups two and three. This increase was also higher than the baseline. The patients in Group 2 faced the greatest fall in blood pressure and heart rate after the injection. Moreover, compared to other groups, this group of patients had the lowest increase in blood pressure and heart rate after laryngoscopy and endotracheal intubation.
Laryngoscopy and endotracheal intubation can cause sympathetic stimulation often manifested as an increase in systolic and diastolic blood pressures and heart rate.4 Thus, anesthesiologists have been trying to use a variety of inductionmodalities to minimize hemodynamic changes. Several studies have been conducted in this regard, and various combinations of drugs have been proposed.
Thiopentone and propofol are two hypnotic medications most commonly used during anesthetic induction. In a study in 1988, an induction dose of 4 mg/kg of thiopentone caused a brief drop in systolic and diastolic blood pressure. Whereas, after laryngoscopy and tracheal intubation, considerable increase even higher than the baseline levels was documented in all these variables. In contrast, while further reduction occurred in blood pressure after injecting 2.5 mg/kg propofol, a smaller increase occurred in blood pressure and heart rate after laryngoscopy and endotracheal intubation; the patients’ blood pressure did not reach the baseline levels.12 It is documented that by using a combination of two or more medications with synergistic or additive effects, the dose of each drug can be reduced. Various medications as midazolam, propofol, alfentanil, fentanyl, and thiopentone have been proposed for this purpose.8 A study in 1991 confirmed the synergistic effects of thiopentone and propofol. By using the combination of these drugs, the effect of lower doses was similar to high doses of using each drug separately. The synergistic effects of thiopentone and propofol in the current study may be because of the interference of both drugs with the gamma-aminobutyric acid (GABA) receptors.11
A previous study examined the effects of thiopentone and propofol in different regions of the brain with two sedative and hypnotic doses. It revealed that at sedating doses, the areas of action of these medications were different in the brain. In each area of brain, decreased rCBF reflects the sedating effect of drug. Thiopentone decreased rCBF in the cerebellum and posterior regions of the brain, whereas propofol decreased it in the anterior regions of the brain. By giving hypnotic doses, both drugs had overlapped actions in different parts of the brain.10
In our study, after drug injection, decrease in blood pressure and heart rate in patients of Group 3 was lower than Group 2 and higher than Group 1. Furthermore, after laryngoscopy and endotracheal intubation, the increase in the above mentioned variables was lower in this group than in Group 1, and higher than in Group 2. In other words, the patients of this group did not have substantial decrease in blood pressure and heart rate as much as the changes induced by propofol. Likewise the increase in blood pressure and heart rate was not as high as the changes caused by thiopentone after laryngoscopy and endotracheal intubation. In general, the whole trend of changes in Group 3 was closer to Group 2. Our findings are consistent with Harris and colleagues’ study, in which the haemodynamic response to tracheal intubation was compared in 303 patients who underwent anesthesia with either thiopentone 4 mg/kg, etomidate 0.3 mg/kg, or propofol 2.5 mg/kg, with and without fentanyl 2 micrograms/kg. Arterial blood pressure decreased significantly after propofol alone, whereas it increased after thiopentone or etomidate alone.12 Increases in heart rate occurred with all medications after laryngoscopy.12
None of the 90 patients in our study faced severe stress-induced symptoms such as coughing or straining etc. during laryngoscopy and endotracheal intubation. We did not document any sudden drop in blood pressure and heart rate after the injections and any surge in these variables after laryngoscopy and endotracheal intubation. A recent trial confirmed the safety of propofol in patients with coronary artery disease and left ventricular dysfunction.13 Another recent trial found a faster onset of thiopentone effect than propofol in elderly patients.14 The safety and the efficacy of the medications used in our study is also supported by another qualitative systematic review.15
CONCLUSION
In this trial, simultaneous use of low dose thiopentone and propofol for anesthetic induction reduced the dose and hemodynamic effects of each medication used alone. The combined use of low dose of these medications caused less hemodynamic changes than the higher dose of either alone. Although, all statistically significant differences documented in this study are not necessarily clinically significant in the age group of 20-50 and patients in ASA-I; but this modality of anesthesia induction may have clinical importance for the elderly patients as well as those with high blood pressure and heart diseases needing lesser dose of medications. Future research in this field is needed to determine the appropriate doses in each group.
Acknowledgements: We would like to thank all of our colleagues at Shiraz Anesthesiology and Critical Care Research Center, who helped us conducting this study.
Funding:None
Conflict of interest: None to declare
REFERENCES
1. Maguire AM, Kumar N, Parker JL, Rowbotham DJ, Thompson JP. Comparison of effects of remifentanil and alfentanil on cardiovascular response to tracheal intubation in hypertensive patients. Br J Anaesth. 2001;86(1):90-3. [Medline]
2. Edwards ND, Alford AM, Dobson PM, Peacock JE, Reilly CS. Myocardial ischaemia during tracheal intubation and extubation. Br J Anaesth. 1994;73(4):537-9. [Medline]
3. Roy WL, Edelist G, Gilbert B. Myocardial ischemia during non-cardiac surgical procedures in patients with coronary-artery disease. Anesthesiology. 1979;51(5):393-7. [Medline]
4. Prys-Roberts C, Greene LT, Meloche R, Foëx P. Studies of anesthesia in relation to hypertension II: Hemodynamic consequences of induction and endotracheal intubation. Br J Anaesth. 1971 Jun;43(6):531-47. [Medline]
5. Hall AP, Thompson JP, Leslie NA, Fox AJ, Kumar N, Rowbotham DJ. Comparison of different doses of remifentanil on the cardiovascular response to laryngoscopy and tracheal intubation. Br J Anaesth 2000 Jan;84(1):100-2. [Medline]
6. Riznyk L, Fijałkowska M, Przesmycki K. Effects of thiopentone and propofol on heart rate variability during fentanyl-based induction of general anesthesia. Pharmacol Rep 2005 Jan-Feb;57(1):128-34. [Medline]
7. Reves JG, PSA, Lubarsky DA, et al Ed: Intravenous nonopioid anesthetics. In: Ronald D. Miller. Miller’s Anesthesia. 6th ed. Elsevier Churchill Livingstone 2005; p318-334.
8. G.B. Rushman, N.J.H. Davies and J.N. Cashman. Editors: Lee’s Synopsis of Anesthesia, 12th Ed. Reed Educational and Professional Publishing Ltd. 1999;175-179, 186.
9. Peacock JE, Lewis RP, Reilly CS, Nimmo WS. Effect of different rates of infusion of propofol for induction of anesthesia in elderly patients. Br J Anaesth 1990;65(3):346-352. [Medline]
10. Veselis RA, Feshchenko VA, Reinsel RA, Dnistrian AM, Beattie B, Akhurst TJ. Thiopentone and propofol affect different regions of the brain at similar pharmacologic effects. Anesth Analg 2004;99(2):399-408. [Medline]
11. Naguib M, Sari-Kouzel A. Thiopentone-propofol hypnotic synergism in patients. Br J Anaesth 1991;67:4-6. [Medline]
12. Harris CE, Murray AM, Anderson JM, Grounds RM, Morgan M. Effects of Thiopentone, etomidate and propofol on the hemodynamic response to tracheal intubation. Anaesthesia 1988;43 (Supplement):32-36. [Medline]
13. Singh R, Choudhury M, Kapoor PM, Kiran U. A randomized trial of anesthetic induction agents in patients with coronary artery disease and left ventricular dysfunction. Ann Card Anaesth 2010;13(3):217-23. [Medline]
14. Sørensen MK, Dolven TL, Rasmussen LS. Onset time and haemodynamic response after thiopentone vs. propofol in the elderly: a randomized trial. Acta Anaesthesiol Scand 2011;55(4):429-34 [Medline]
15. Wilbur K, Zed PJ. Is propofol an optimal agent for procedural sedation and rapid sequence intubation in the emergency department? CJEM 2001;3(4):302-10. [Medline]
