
Amarja Sachin Nagre, MD, DM, FCA*
*Dr Amarja Sachin Nagre, Assistant Professor, N-6, Cidco, Aurangabad, Maharashtra 431003, (India)
The rationale behind development of off pump coronary artery bypass (OPCAB) surgery is avoidance of CPB related complications in addition to other advantages like decrease in postoperative neurocognitive and renal dysfunction. It is associated with decrease in postoperative morbidity, accelerates recovery and leads to early ICU and hospital discharge. Ultrafast tracking and awake OPCAB under high thoracic epidural are significant advances. Anesthetic management of OPCAB patients is targeted to maintain hemodynamic stability and prevent myocardial ischemia during coronary grafting. Meticulous preanesthetic assessment, monitoring, titrated usage of induction agents, balanced anesthetic technique and vigilance during grafting is the essence of anesthetic management during OPCAB.
Octopus Tissue Stabilizer minimizes the motion of the small area of the heart where the bypass graft is to be attached while the rest of the heart continues to beat normally. Starfish is the positioner attached at the cardiac apex which locks the longitudinal axis of the heart, thereby allowing access to coronary vessels of the lateral and posterior walls. Intracoronary shunts secure the blood flow through the coronary vessels during the procedure.
Left anterior descending (LAD) grafting (Figure 1) involves ‘displacement’ of the heart forward and superior to facilitate LAD anastomosis by placing pericardial stay sutures and mops underneath the heart.
Left circumflex artery (LCX) grafting (Figure 2) is the most critical anastomosis as exposure is difficult which demands lifting the heart and placing it in an unphysiologic position called as ‘verticalization’, achieved by displacing heart to right side. Placing Octopus stabilizer system leads to compression of right ventricle and distortion of the tricuspid and mitral annuli. Steps to combat hypotension and hypoperfusion are opening of right pleura to accommodate RV, application of Starfish apical suction device, trendelenburg position, use of vasopressors and inotropes, judicious volume expansion as excess volume administration causes increase in left ventricular end diastolic volume (LVEDV) and hence LVEDP. This leads to decrease in coronary perfusion pressure.
Right coronary artery (RCA) grafting (Figures 3 & 4) may result in severe ischemia during clamping of RCA and complete atrioventricular block attributable to interruption of the blood flow in the AV node artery.(9)
Ultrafast tracking of Anesthesia (UFTA): The term ultrafast tracking includes shortening of prolonged postoperative ventilatory support, or even immediate extubation, reducing ICU stay and postoperative monitoring, and early discharge.13 Concerns about UFTA with early extubation include increased respiratory and cardiac workload causing myocardial ischemia, reintubation, hypothermia, shivering, inadequate analgesia, and perhaps mortality. Mediastinal bleeding requiring reexploration is a potential problem in cardiac surgery wherein a secured airway is desired. Benefits of early extubation after cardiac surgery are reduced lung trauma with decrease in the stress and discomfort of endotracheal tube suctioning and weaning from ventilation. Sedative drugs and ventilator disposables requirement is lessened. Patients are transferred early to lower dependency units. Nursing staff required to manage each patient is less. Early extubation saves cost through decreasing the usage of oxygen, ABG sampling, suction catheters, gloves, power consumption and manpower requirement.
References
- Lazar HL. Should off-pump coronary artery bypass grafting be abandoned?. Circulation. 2013 Jul 23;128(4):406-13. [PubMed] [Free full text] doi:1161/CIRCULATIONAHA.113.003388
- Sellke FW, DiMaio JM, Caplan LR, Ferguson TB, Gardner TJ, Hiratzka LF, Isselbacher EM, Lytle BW, Mack MJ, Murkin JM, Robbins RC. Comparing On-Pump and Off-Pump Coronary Artery Bypass Grafting Numerous Studies but Few Conclusions: A Scientific Statement From the American Heart Association Council on Cardiovascular Surgery and Anesthesia in Collaboration With the Interdisciplinary Working Group on Quality of Care and Outcomes Research. Circulation. 2005 May 31;111(21):2858-64. [PubMed] [Free full text]
- Chassot PG, Van der Linden P, Zaugg M, Mueller XM, Spahn DR. Off‐pump coronary artery bypass surgery: physiology and anaesthetic management. Br J Anaesth. 2004 Mar;92(3):400-13. [PubMed] [Free full text] doi:1093/bja/aeh064
- Kiessling AH, Huneke P, Reyher C, Bingold T, Zierer A, Moritz A. Risk factor
analysis for fast track protocol failure. J Cardiothorac Surg. 2013 Mar 15;8:47. [PubMed] [Free full text] doi: 10.1186/1749-8090-8-47.
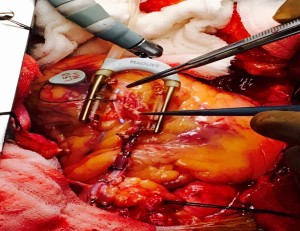
Figure 1: Left anterior descending (LAD) grafting. Intracoronary shunt kept outside the anastomosis for demonstration
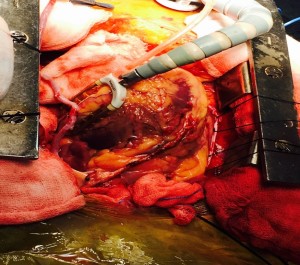
Figure 2: Left circumflex artery (LCX) grafting. Note the ‘verticalization’ of the heart.

Figure 3: Right coronary artery (RCA) grafting.
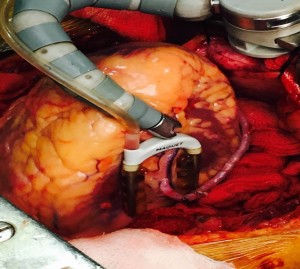
Figure 4: Right coronary artery (RCA) anastomosis.
With Prof Octavio Alfieri- the biggest name in Mitral Valve repair and Alfieri stitch is his contribution.. He demonstrated the same and stressed the importance of perioperative TEE and importance in avoiding SAM
(Courtesy: Vikram Basappanavar)
