
*Sujit Vasudevan Nair, MD*, Khalifa Abdullah Mohammed Al-Ghafri, MRCS**, Aziz Haris, MD, STARCSI*, Rashid Manzoor Khan, MD* and Naresh Kaul, MD*
*Department of Anesthesia & ICU
** Department of Orthopedic
National Trauma Center, Khoula Hospital, Muscat (Sultanate of Oman)
Correspondence: Dr. Naresh Kaul, Sr. Consultant, Department of Anesthesia & ICU, Muscat (Sultanate of Oman); GSM: 00 968 99366241; E-mail: nassn@gmail.com,
A quadric-lumen central venous catheter was placed via the right subclavian route in a 15 year old healthy girl undergoing corrective surgery for scoliosis (D4 – L1) in the prone position under general anaesthesia. The distal most catheter port was kept closed as free flow of blood was absent in this channel. All other ports were working well. As the surgery progressed over next 45 min, central venous pressure and peak airway pressure gradually increased with a concurrent fall in blood pressure. All this was initially attributed to pressure being exerted over the back of the chest by the operating surgeon and a misplaced chest bolster. Also added to the confusion was observation of blood tinged watery fluid in the operative field which was erroneously attributed to be CSF leak from a dural rent. Fluids and other medications continued to be administered via the central line ports. It was only when hypotension was noted to be unresponsive to ephedrine injection via the central line that attention was directed to the possibility of accidental hydrothorax secondary to migration of the distal end of the central line. Immediate postoperative AP view of the chest X-ray confirmed this (Fig 1). Appropriate corrective measures were instituted and patient made an uneventful recovery.
Clinical Pearls: 1. Aspirate free flow of relatively dark colored blood via the needle prior to introduction of the J-tip guide wire. 2. Ascertain free flow of blood via all lumens of the catheter prior to its fixation. 3. Re-aspirate blood after administration of 50-100 ml fluid,change of patient position, and whenever in doubt.
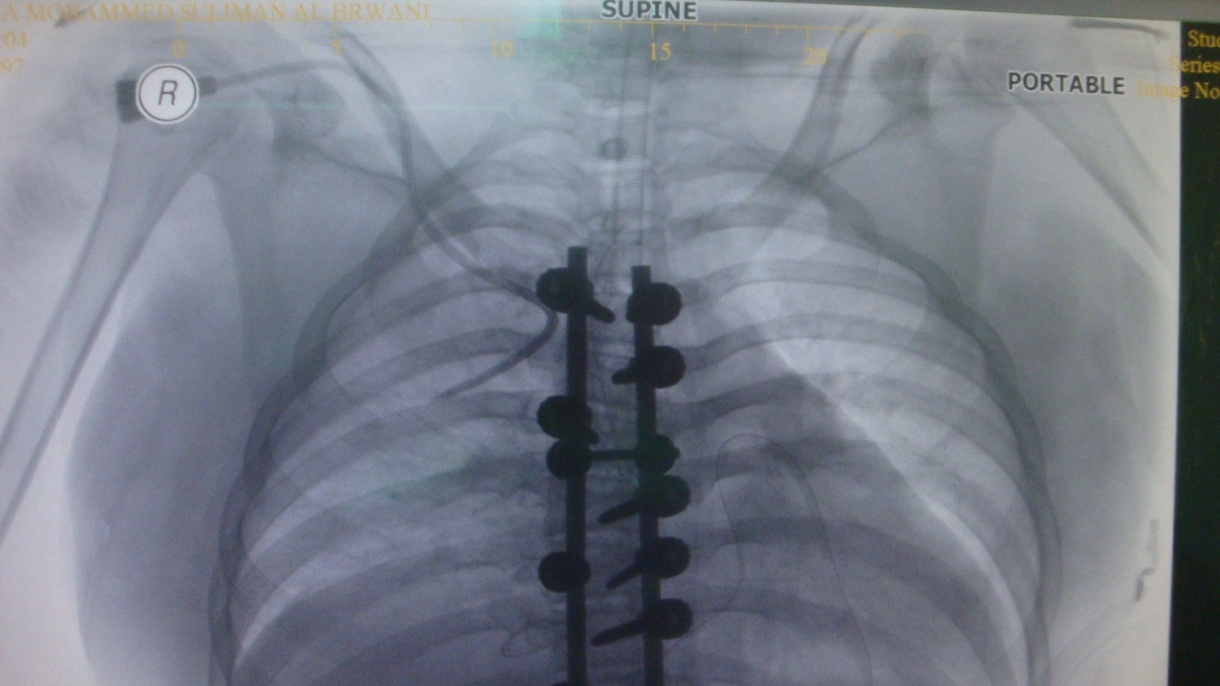
Fig 1: Immediate postoperative chest x-ray (antero-posterior view) showing malpositioned subclavian central venous catheter.
