
Ranajit Panigrahi1, Ritesh Roy2, Anju Prasad3, Amita Kumari Mahapatra4,
Ashok Priyadarshi5, Nishit Palo5
1MBBS, MS (Orthopedics), Professor of Orthopedics
2MBBS, MD (Anesthesia), Professor of Anesthesiology
3MBBS, MD (Pharmacology), Associate Professor of Pharmacology
4MBBS, MD (Physiology), Assistant Professor of Physiology
5MBBS,Postgraduate in Department of Orthopedic
Hi-Tech Medical College &Hospital,High Tech Hospital Rd, Pandara,Bhubaneshwar,Odisha751007, (India)
Correspondence: Prof. Dr. Ritesh Roy, Plot no-582,Jagannath Complex, Flat No-102, Sahid Nagar, Bhubaneshwar, Odisha -751007, (India); Cell: 09437101886; E-mail: drriteshroy@yahoo.com
ABSTRACT
Objective: Arthroscopic Bankart’s procedure is widely used method for shoulder instability. It may evoke variable intensity of post operative pain, which may be unbearable depending upon individual’s pain threshold.Adequate pain relief reduces surgical stress response, improves postoperative recovery and rehabilitation. We conducted this study to compare the postoperative analgesic effect of addition of dexamethasone 300 µg/kg to intra-articular ropivacainewith ropivacaineonly in arthroscopicBankart’sprocedures.
Methodology: A prospective multi-center double blind study was conducted on 45 patients undergoing arthroscopic Bankart’s procedure from Jan 2015 to June 2015. Patients were randomly assigned into 3 groups – Group I receiving 20 ml normal saline,Group II 20 ml 0.2% ropivacaine and Group III (15 ml 0.2% of ropivacaineand dexamethasone in a dose of 300 ug/kg intra-particularly. Variables assessed:analgesic effect (VAS Score), time to first postoperative analgesic request, total analgesics used during first 24 hours.
Results: Group III had significantly low pain scores for more than 24 hours as compared to Group II and Group I.Time to first analgesic requirement was the longest in Group III (1562.2± 79.10 min)(p<0.01).Intensity of pain and total analgesic requirement was also significantly less in Group III (32.2 ± 23.83 mg) (p<0.01) compared to Group II and I. No significant side-effects were noted.
Conclusion: Dexamethasone 300 µg / kg with ropivacaine intraarticularly has a superior analgesic efficacy,a much prolonged postoperative pain relief, minimal postoperative analgesia requirement and better patient compliance withnegligible side effects. Thus, we recommend dexamethasone 300 µg/ kg in arthroscopic Bankart’s procedure to facilitate early rehabilitation and good functional scores.
Keywords: Dexamethasone; Ropivacaine; Pain; Acute Pain; Pain, Postoperative; Shoulder pain; Analgesia; Shoulder
Citation:Panigrahi R, Roy R, Prasad A, Mahapatra AK, Priyadarshi A, Palo N.Intraarticular dexamethasone in pain management following arthroscopic Bankart repair. Anaesth Pain & intensive Care 2015;19(3)269- 273
INTRODUCTION
Shoulder instability is a serious disabling injury which is routinely seen in orthopedic practice. Shoulder dislocations occur predominantly in males in the 3rddecade1 with an incidence of 11-56 per100, 000 person-years.2Shoulder dislocates mostly anteriorly but also posteriorly or inferiorly.3
The arthroscopic Bankart procedure is extremely popular, effective and widely accepted for treatment of anterior shoulder instability.4 Inspite of being a minimally invasive procedure,it can evoke different levels of pain postoperatively,which at times can be unbearable depending on the individual patient’s pain tolerance.Postoperative pain affects patient’s psychology, mobilization and rehabilitation adversely and may prolong hospital stay5 and worsen the prognosis. Adequate pain relief improves postoperative recovery and rehabilitation.5
An inter-scalene block gives excellent immediate pain control, but of a short and unpredictable duration; there is a high risk that the patient experiences severe and uncontrollable pain the first night after surgery.6 Continuous nerve block gives a better pain control but is more technically and logistically demanding.7 The severity and duration of pain after surgery has a high inter-individual variation, it is challenging to safely administer an adequate dose of opiate analgesics. There has frequently been a search for a simple method for providing postoperative analgesia in these patients that would have a prolonged duration of action, be easy to administer and without any serious side effects.
The intra-articular route of drug administration utilises the peripheral receptors and administration of local anesthetics through this route is routinely done after arthroscopic knee surgery but in shoulder procedures, intraarticular analgesics are not frequently used. Previous studies have reported the use local anesthetics such as bupivacaine, ropivacaine, opioids like morphine, magnesium sulphateintra-articularly inshoulder arthroscopic procedures with variable duration of analgesiafor postoperative pain control.8-10
Although a few studies report the analgesic effect of fixed dose dexamethasone following shoulder arthroscopic procedures, we report the analgesic effects of a dexamethasone titrated by µg/kg body weight manner following arthroscopic shoulder Bankart’s repair.We compared a combination of dexamethasone- ropivacaine against ropivacaine, as well as versus normal saline following arthroscopic Bankart procedure. We hypothesized that a longer postoperative analgesia could be achieved, provided that dexamethasone 300µg/kg was safe and free from any side effects.
METHODOLOGY
In this Multicenter prospective double-blindrandomisedtrial,after clearance by the local ethical committee, 45consecutive patientswith shoulder instabilitieswho underwent elective arthroscopic Bankart’srepair from Jan 2015 to Jun 2015were included inthe studyafter they consented to participate in this study. Inclusion criteria were 15–60 years, Male/Female, no mental illnesses or allergy to dexamethasone or ropivacaine, ASA class I and II, being operated arthroscopically under general anesthesia forBankart’s lesion. Patient refusal, any previous surgery of shoulder, any known allergy or contraindication to ropivacaine, or dexamethasone, pregnancy, lactating mothers, hepatic, renal or cardiopulmonary abnormality, alcoholism, diabetes, long-term analgesic therapy, bleeding diathesis, coagulopathies, local skin site infections, hypertension were excluded from the study.
The randomization was performed based on a computer generated number by a person unaware of the study objectives who sealed the obtained codes in secure envelopes. The envelopes were given to the researcher who had no role in the treatment or evaluation. This person then gave a syringe containing the solution based on the confidential codes to the surgeon to inject into the joint cavity.
In the preoperative visit, the visual analogue scale (VAS) was obtained and the patients were questioned about any drug allergy, previous operations or drug treatment. Just before the operation, baseline heart rate (HR), mean arterial pressure (MAP) were recorded. Intraoperatively, routine ECG, HR, blood pressure (systolic, diastolic and mean) and arterial oxygen saturation (SpO2) were monitored. The anesthetic technique was standard for all patients and all the operations were performed under general anesthesia. Syringes containing 20 ml aqueous solution of either normal saline or ropivacaine[ROPIN™ 0.2%2mg/ml; Neon Laboratories Ltd. Andheri(East), Mumbai (India)]or 15 ml ropivacaine with dexamethasone 300 µg/kg body weight were injected intra-articularly at the end of surgery by treating orthopedic surgeon and sterile compression bandage applied.
Postoperatively, VAS score and vital parameters like HR, MAP were recorded at 1, 3, 6, 8, 12, 18, and 24 hrs. Diclofenac sodium (75 mg) was administered I.V. as an analgesic supplementation if the recorded VAS pain score was> 4 and was repeated every 8 h if required.The time to the first analgesic requirement and the total diclofenac use during the first 24 h after operation were also recorded. Side effects such as nausea, vomiting, bradycardia and hypotension (defined as reduction of MAP25% of baseline) were recorded.
Group I (Control group) – received 20 ml saline.
Group II- Received 20 ml (0.2%) ropivacaine hydrochloride.
Group III- Received 15ml (0.2%) ropivacaine and 300 µg/kgdexamethasone.
Variables assessed: Post operative analgesic effect (VAS score) at 1st, 3rd, 6th, 8th, 12th, 18th and 24th hour;time to first postoperative analgesic request and total analgesic used during first 24 hours were recorded.
RESULTS
Out of 45 patients, 32 were males. As regards the demographic characteristics (Table 1), there was no significant differences in the mean age, weight of the patients and duration of surgery in the groups. No sideeffects were reported during the first 24 hour after surgery.Mean arterial pressure and heart rate did not change significantly in the three groups.
Table 1: Patient characteristics of 3 groups [Data given as Mean ± SD]
|
Variables |
Group I (n=15) |
Group II (n=15) |
Group III (n=15) |
| Age(years) |
34.5 ± 10.85 |
31.2 ± 9.28 |
32.3 ± 11.4 |
| Gender(M/F) |
11/5 |
10/4 |
11/4 |
| Weight(kgs) |
66.4 ± 5.43 |
65.3 ± 8.44 |
68.2 ± 6.65 |
| Duration of Surgery(min) |
78.4 ± 21.53 |
81.3 ± 23.84 |
80.4 ± 24.74 |
VAS scores in Group III at 3rdhour (p<0.01), at 6thhour (p<0.02), at 8th hour (p<0.02), at 12thhour (p<0.05) and 18th(p<0.05)hour was least as compared to group I and II following surgery (see Figure 1)
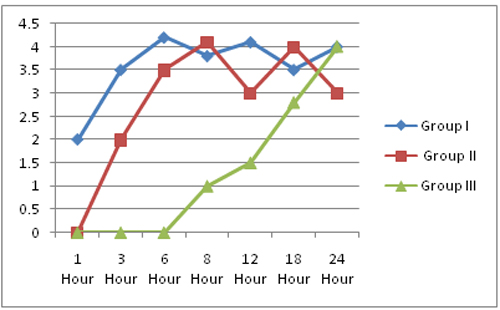
Figure1: Change in Visual Analogue Scale in 3 Groups
No incidence of nausea, vomiting, bradycardia, hypotension or other side-effects requiring intervention were reported in the subjects.
Time to first postoperative analgesia request was longest in Group III(1562.2± 79.10 min) as compared to the Group II (445.2 ± 64.3 min)and Group I (323.8 ± 56.61 min)(p<0.01). Mean total analgesic consumption in first 24 hours was least in Group III (32.2 ± 23.83 mg) followed by Group I(223.25 ± 54.83 mg)and Group II (151.72 ± 53.5 mg) (p<0.01)(see Table 2).
Table 2: Analgesia Duration and total analgesic requirement in 24 hours
|
Group I |
Group II |
Group III |
p-value |
|
| Mean time to 1st postoperative analgesic requirement (min) |
323.8 ± 56.61 |
445.2 ± 64.3 |
1562.2 ± 79.10 |
0.004 |
| Mean total analgesic(diclofenac) consumption in 24 hours (mg) |
223.25 ± 54.83 |
151.72 ± 53.5 |
32.2 ± 23.83 |
0.007 |
DISCUSSION
Arthroscopic Bankart’s repair is often associated with severe postoperative pain due to irritation of free nerve endings of synovial tissue and joint capsule during surgical excision, insertion of hardware, bone removal or soft tissue distension from irrigation fluid11. Good early rehabilitation requires postoperative pain control and mobilization.Although loco-regional anesthesia has greatly contributed as a solution for postoperative pain relief, its intra-articular administration following arthroscopic shoulder procedures is not yet in routinely clinical practice.
Dexamethasone has been used intrarticularly following shoulder arthroscopic surgeries in a few studies previously with good results,but no study has reported the analgesic effects in a dosage of 300 ug/kgwt. Our study reported the postoperative analgesic effect of dexamethasone in the dose of 300 ug/kgwt as an adjunct to ropivacaine following arthroscopicBankart’s lesion repair. We observed a long analgesic period and decreased analgesics requirement post operatively with a better patient compliance.
Dexamethasone was selected in our study because of its highly potent anti-inflammatory property with minimal mineral ocorticoid activity and devoid of potential side effects. Steroids also share a block prolonging effect due to their anti- inflammatory potency.12,13 The dense and prolonged block in the dexamethasonegroup is attributed to the synergistic action with local anesthetic ropivacaine on blockade of nociceptive C-nerve fibres.
Studies report significant pain relief, up to 12 hours post shoulder arthroscopy in patients receiving intrarticular injection of 1000mg magnesium sulphate with 10 ml normal saline but reported side effects like nausea, vomiting in few patients14 and up to 10 hours in patients receiving intrarticular ropivacaine with decreased analgesic requirement15.Whereas we observed a significant pain free period of more than 24 hours in our study in patients receiving intrarticular dexamethasone 300 ug/kgwt with 15ml of ropivacaine compared to normal saline and ropivacaine injections alone. Our patients were extremely pleased with the surgery and to our surprise, some cases did not require analgesic support even upto 30 hours.
We report a significant prolongation of analgesia and the time to first postoperative analgesic requirement (1562.2± 79.10min p< 0.01), a significant reduction in consumption of analgesic (32.2 ± 23.83 mg p< 0.01) and a significantly lower pain VAS score in the first 24 hours in the intra-articular dexamethasone group which are better as compared to the reported literature. We attribute these results to the new dosage of dexamethasone.
A limitation could be a measure of dexamethasone’s plasma concentration to correlate it with clinical findings, which may have confirmed the local effects. Intraarticular dexamethasone 300 µg/kg enhanced the postoperative analgesia after arthroscopic Bankart’s repair without any significant side effects and thus can safely and effectively be used in this procedure.
CONCLUSION
Dexamethasone with ropivacaine, intrarticularly has a superior analgesic efficacy,a much prolonged postoperative pain relief, minimal postoperative analgesic requirement and better patient compliance with negligible side effects.
REFERENCES
- Zacchilli M, Owens B. Epidemiology ofshoulder dislocations presenting toemergency departments in the UnitedStates. J Bone Joint Surg Am 2010;92(3):542–549.[PubMed]doi: 10.2106/JBJS.I.00450.
- Liavaag S, Svenningsen S, Reikerås O,Enger M, Fjalestad T, Pripp A, Brox JI.The epidemiology of shoulder dislocations in Oslo.Scand J Med SciSports 2011;21(6):e334–e340.[PubMed][Free full text]doi: 10.1111/j.1600-0838.2011.01300.x. Epub 2011 Apr 21.
- Owens B, Duffey M, Nelson B,DeBerardino T, Taylor D, Mountcastle S. The incidence and characteristics ofshoulder instability at the United StatesMilitary Academy.Am J Sports Med2007;35(7):1168–1173.[PubMed]
- Owens B, Harrast J, Hurwitz S,Thompson T, Wolf J. Surgical trends inBankart repair: an analysis of data fromthe American Board of OrthopaedicSurgery certification examination.Am J Sports Med 2011;39(9):1865–1869.[PubMed]doi: 10.1177/0363546511406869.
- Manuar MB, Majumdar S, Das A, Hajra BK, Dutta S, Mukherjee Det al. Pain relief after Arthroscopic Knee Surgery: A comparison of intra-articular ropivacaine,fentanyl, and dexmedetomidine: A prospective, double-blinded, randomized controlled study. Saudi J Anaesth. 2014 Apr;8(2):233-7. doi: 10.4103/1658-354X.130727.[PubMed]
- Boezaart A, Tighe P. New trends inregional anesthesia for shoulder surgery: avoiding devastatingcomplications. Int J Shoulder Surg2010;4(1):1–7.[PubMed][Free full text]doi: 10.4103/0973-6042.68410.
- Boezaart AP. Continuous interscaleneblock for ambulatory shoulder surgery. Best PractRes ClinAnaesthesiol 2002;16(2):295–310.[PubMed]
- Rodolà F, Vagnoni S, D’Avolio S, Vurchio M, Micci D, Chierichini A, et al. Intra-articular analgesia following arthroscopic surgery of the shoulder.Eur Rev Med Pharmacol Sci. 2001 Jul-Aug;5(4):143-6. [PubMed]
- Saritas TB, Borazan H, Okesli S, Yel M, Otelcioglu S.Is intra-articular magnesium effective for postoperative analgesia in arthroscopic shoulder surgery?Pain Res Manag. 2015 Jan-Feb;20(1):35-8. [PubMed][Free full text]
- Doss N W, Splain S H, Crimi T, Michael R, Abadir A R,Gintautas J. Intra-articular morphine, ropivacaine and morphine/ropivacaine for pain control after arthroscopy. Preliminary Observation.Proc West Pharmacol Soc. 2001;44:195-196.[PubMed]
- Ruiz-Suarez M. Postoperative pain control after shoulder arthroscopy. Orthopaedics 2008;31:1130.[PubMed]
- Johanson A, Hao J, Sjölund B. Local corticosteroid application blocks transmission in normal nociceptive C-fibres. ActaAnaesthsiolScand 1990;34:335-8.[PubMed]
- Golwala MP, Swadia VN, Aditi AD, Sridhar NV. Pain relief bydexamethasone as an adjuvant to local anesthetics in supraclavicular-brachial plexus block. J AnaesthClinPharmacol 2009;25:285-8. [PubMed]
- Saritas TB, Borazan H, Okesli S, Yel M, Otelcioglu S.Is intra-articular magnesium effective for postoperative analgesia in arthroscopic shoulder surgery? Pain Res Manag. 2015 Jan-Feb;20(1):35-8.[PubMed][Free full text]
- Rodolà F, Vagnoni S, D’Avolio S, Vurchio M, Micci D, Chierichini A, et al. Intra-articular analgesia following arthroscopic surgery of the shoulder.Eur Rev Med Pharmacol Sci. 2001 Jul-Aug;5(4):143-6. [PubMed]
