Seyfi Kartal, Gülay Kip, Ayşegül Küçük, Ali Atan, Özlem Erdem, Mustafa Kavutçu
Department of Anesthesiology and Reanimation, Trabzon Kanuni Training and Research Hospital, Trabzon, Turkey.
Correspondence: Seyfi Kartal, Department of Anesthesiology and Reanimation, Trabzon Kanuni Training and Research Hospital, University of Health Science Turkey, Turkey.
E-mail: drseyfikartal@gmail.com; Phone: +90 462 341 56 56
Abstract
Objectives: Ischemia-reperfusion (IR) injury is a complex phenomenon, which is known to cause cell damage. In this study, we aimed to investigate the protective effects of dexmedetomidine on lung in the renal IR model in diabetic rats
Materials and Methods: After approval of the ethics committee, diabetes was induced by streptozocin (55 mg/kg) and then 24 Wistar Albino rats were randomly divided into 4 groups. Diabetic control group (group DC), diabetic dexmedetomidine (group DD), diabetic ischemia-reperfusion (group DIR), diabetic ischemia-reperfusion - dexmedetomidine (group DIR-D). In DD and DIR-D groups, 100 µ/kg dexmedetomidine was administered intraperitoneally 30 minutes before renal ischemia-reperfusion administration. In group DIR, and both artery and vein were clamped by an atraumatic vascular clamp for 120 minutes, then allowed reperfusion for 120 minutes. After then, biochemical and histopathological parameters of lung tissue samples were evaluated.
Results: Histopathologically, neutrophil infiltration/aggregation, alveolar wall thickness, and total lung injury scores were found to be significantly higher in the DIR group than in the DC, DD and DIR-D groups. In addition, neutrophil infiltration/aggregation, alveolar wall thickness, and total lung injury scores were significantly higher in the DD and DIR-D groups compared to the DC group. We found that Catalase, Paraoxonase-1 activities and malondialdehyde levels were significantly increased in DIR group compared to DC, DD and DIR-D groups (p= 0.008, p<0.0001 and p=0.001 respectively).
Conclusion: It was found that dexmedetomidine administered in diabetic rats partially corrected ischemia-reperfusion -related damage in the lung. We think that dexmedetomidine administration before renal IR has a protective effect in in diabetic rats.
Key words: Dexmedetomidine, ischemia-reperfusion, lung, renal, diabetes
Citation: Kartal S, Kip G, Küçük A, Atan A, Erdem Ö, Kavutçu M. The efficacy of dexmedetomidine on lung injury induced by renal ischemia/reperfusion in diabetic rats. Anaesth. pain intensive care 2020;24(3):272-277
Received: 17 may 2020; Reviewed: 31 May 2020; Accepted for publication: 6 June 2020
_________________________________________________________________________________
Introduction
It is a known fact that ischemia-reperfusion injuries (IR) can affect many organs in the body. The various factors are responsible for the pathogenesis of ischemia-reperfusion injury.1 Recent studies have shown that acute renal I/R causes some disfunction in both adjacent and distant organs such as heart, liver, brain, and small intestines.2 The lung is also prone to injury because of its large microcapillary network.3 Lung injury is characterized by many parameters including neutrophil infiltration/aggregation, alveolar wall thickness,4 and total lung injury score. After ischemic acute renal failure, the pulmonary injury was noticed, which is characterized by non-cardiogenic edema and neutrophil infiltration.5
Dexmedetomidine is an alpha-2 adrenergic agonist and is used for its sedative, analgesic, sympatholytic properties. Due to these beneficial effects, it is frequently preferred in trauma patients. In addition, It is shown that dexmedetomidine may reduce systemic inflammation.6 The protective effects of dexmedetomidine on ischemic injury due to I/R have been described in both adjacent and distant organs (such as pulmonary, cardiac, liver and renal). The risk of distant organ damage due to lipid peroxidation secondary to I/R has increased in diabetic patients compared to the normal population.7 In the case of I / R, there is no effective treatment of distal organ damage and it is still a serious problem.
In this study, we aimed to investigate the protective effects of dexmedetomidine on lung in the renal IR model in diabetic rats.
Methodology
Settings
This study was carried out at the Animal Experiments Laboratory of Gazi University after the approval of the Animal Ethics Local Ethics Committee (Number 18.015). The entire study methodology was performed in accordance with the guideline for the protection and care of experimental animals. 24 male Wistar albino rats weighing 200-250 gr were used for the experiment.
Procedures
The animals were allowed to access free water and food for 2 hours before the procedure with a 12-hour dark-light cycle in standard metal cages. 100 mg/kg (i.p.) of ketamine hydrochloride (Ketalar ®, Eczacıbaşı Parke-Davis, Istanbul, Turkey) was given to provide anesthesia by the cannulation of rats' tail. All procedures were performed in the supine position. Streptozotocin (STZ; Sigma Chemical, St Louis, MO, USA) at a single dose of 55 mg/kg was administered intraperitoneally (IP) to induce diabetes. After 48 hours, in case blood glucose was below 250 mg/dl, the streptozocin dose was repeated. If the blood glucose level above 250 mg/dl then it was accepted as diabetic. The experimental protocol was applied to the rats 4 weeks after the formation of diabetes.
Wistar albino rats (n:24) were randomly divided into 4 groups. Diabetic control group (Group DC), diabetic dexmedetomidine (Group DD), diabetic IR (Group DIR), diabetic IR- dexmedetomidine (Group DIR-D). In Group DD and DIR-D, 100 µg/kg dexmedetomidine was administered intraperitoneally 30 minutes before renal IR administration. In Group DIR and DIR-D both artery and vein were clamped by an atraumatic vascular clamp for 120 minutes. Then, the clamp was removed and reperfusion was achieved for 120 minutes. After the reperfusion period, biochemical and histopathological parameters of lung tissue samples were evaluated.
In Group DC, the rats were anesthetized with ketamine and no additional anesthetic agent were administered. In Group DC, an only midline laparotomy was performed and IR was not applied. In Group DIR, rats were anesthetized with ketamine and were not given dexmedetomidine. After proper disinfection, a midline laparotomy was performed. The left renal pedicle was released and both left renal artery and vein were clamped with an atraumatic vascular clamp. After 120 minutes of ischemia, reperfusion for 120 minutes was applied. In Group DD, after anesthesia, 100 µ/kg dexmedetomidine was administered intraperitoneally. IR was not applied. In Group DIR-D, 100 µ/kg dexmedetomidine was administered intraperitoneally 30 minutes before renal IR administration. Lung tissues were excised and removed, and then rats were sacrificed. Biochemical and histopathological parameters were evaluated.
Measurements of MDA levels and CAT and PON-1 activities in lung tissue
Measurement of Malondialdehyde (MDA) levels, thiobarbituric acid (TBA) reactive substances assay was performed by Van Ye et al method.8 The reaction with TBA at 90-100˚C was used to determine the MDA level, as MDA or similar substances react with TBA and produce a pink pigment that has an absorption maximum of 532 nm. To ensure protein precipitation, the sample in room temperature is mixed with cold 20% (wt/vol) trichloroacetic acid and the precipitate is then centrifuged for 10 min 3000 rpm at room temperature to form a pellet.
An aliquot of the supernatant is then placed into an equal volume of 0.6% (wt/vol) TBA in a boiling water bath for 30 min. Following cooling, sample and blank absorbance were read at 532 nm and the results expressed as nmol/mg protein, based on a graph where 1,1,3,3-tetramethoxypropane has been used as MDA standard.
The Catalase (CAT) activity is based on the measurement of absorbance decrease due to H2O2 consumption at 240 nm by Aebi H method.9
Paraoxonase (PON)-1 activity was measured the rate of hydrolysis of paraoxon by monitoring the increase of absorbance at 405 nm and at 25 °C by Brites FD. method. The basal assay mixture included 1.0 mM paraoxon and 1.0 mM CaCl2 in Tris/HCl buffer (pH: 8.0, 100 mM). The definition of 1 unit of paraoxonase activity was taken as 1 millimole of p-nitrophenol formed per min.10 The CAT and PON 1 activities were given in IU/mg protein.
Samples protein amount was determined by Lowry O method, BSA was used standard protein.11
Histopathological evaluation of the lung
Histopathological analysis in lung tissue sections were performed blindly by histopathologist as in twenty-five different areas randomly determined in each preparation without overlap in each preparation.
Histological tissue damage was evaluated by light microscopy by hemotoxylin-eosin staining. The severity of lung injury; evaluated with a 4-point scale (0: No damage, 1: mild injury, 2: moderate injury, 3: severe injury).
Statistical analysis
All data obtained from the semi-quantitative analyses were calculated using Statistical Package for the Social Sciences (SPSS) 22.0 (IBM, Armonk, NJ, USA) statistics program. Compliance with normal distribution was checked by the Kolmogorov-Smirnov test. In the evaluation of more than two independent groups with normal distribution, analyses were performed by using Kruskal-Wallis test. A Bonferroni adjusted Mann-Whitney U test was used after a significant Kruskal-Wallis findings to determine which group differs from the others. Results are expressed as mean ± standard error (SE). Statistical significance was set at a p < 0.05.
Results
Oxidant parameters (CAT and PON activities, MDA levels) were evaluated. We found that CAT and PON activities and also MDA levels were significantly increased in DIR group compared to DC, DD, and DIR-D groups (p = 0.008, p < 0.0001 and p = 0.03. 01 respectively). MDA levels were significantly increased in DIR group compared to DC, DD, and DIR-D groups (p < 0.0001, p < 0.0001 and p = 0.002 respectively).
Also MDA levels were higher in Group DIR-D compared to Group DC (p = 0.044). PON activities were significantly increased in DIR group compared to DC, DD, and DIR-D groups (p = 0.003, p = 0.003 and p = 0.013 respectively). Similarly, CAT activities were significantly increased in DIR group compared to DC, DD and DIR-D groups (p < 0.0001, p = 0.004 and p = 0.006 respectively). All results related to oxidant parameters are shown in Table 1.
Comparison of the findings for lung tissue neutrophil infiltration/aggregation revealed a significant difference among the groups (p < 0.0001). Neutrophil infiltration/aggregation was significantly higher in the DIR group than in the DC DD, and DIR-D groups (p < 0.0001, p = 0.002 and p = 0.016, respectively).
Neutrophil infiltration/aggregation was also significantly higher in the DIR and DIR-D groups than in the DC group (p < 0.0001 and p < 0.0001, respectively). (Table 2; Figures 1-4).
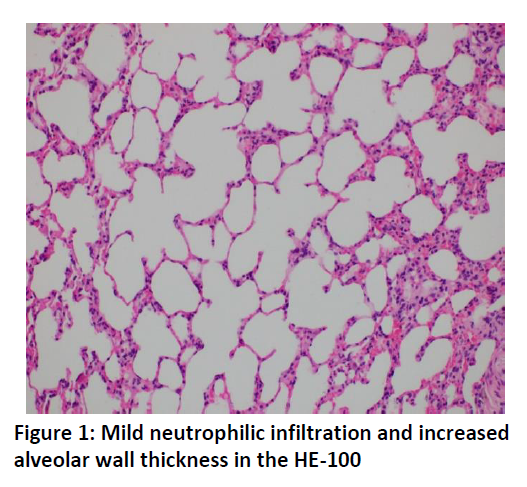
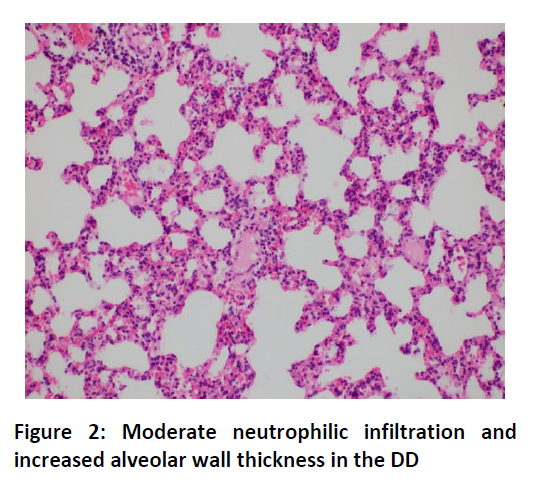
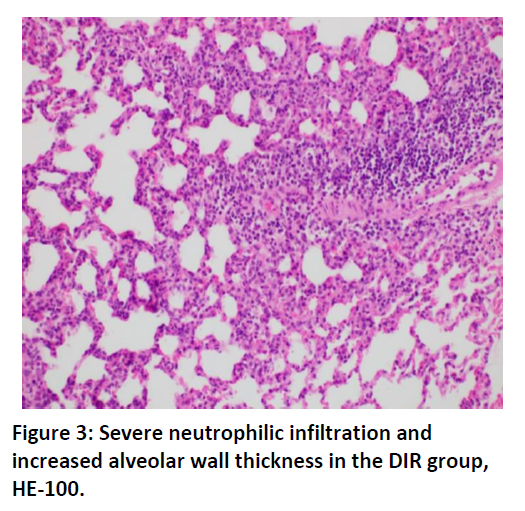
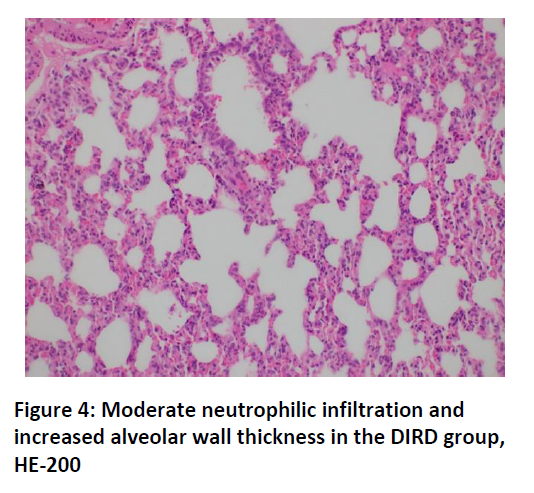
Alveolar wall thickening in lung tissue was significantly higher in the DIR group than in the DC, DD, and DIR-D groups (p < 0.0001, p = 0.001, and p = 0.001, respectively). Alveolar wall thickening was also significantly higher in the DIR and DIR-D groups than in the DC group (p < 0.0001 and p < 0.0001, respectively) (Table 2; Figures 1-4).
The lung tissue injury score was significantly higher in the DIR group than in the DC, DD, and DIR-D groups (p < 0.0001, P < 0.001 and p = 0.001, respectively). In addition, the lung tissue injury score was significantly higher in the DIR and DIR-D groups than in the DC group (p < 0.0001 and p < 0.0001, respectively) (Table 2; Figures 1-4).
Discussion
IR is a complex and biphasic process, which causes cell damage. IR injury is very important for not only adjacent organs but also distant organs. After the blood flow is re-established, reperfusion increases the rate of injury resulted from the ischemic period and aggravates the damage.1 Ischemia and/or reperfusion may be responsible for lung injury due to IR. Various ischemia-reperfusion injury models have been applied12,13 and many studies have been conducted about this issue.14,15
It is known that diabetes may affect microcirculation. Also, IR affects microcirculation. Therefore, the present study was conducted on diabetic rats to determine the effects of dexmedetomidine on lung injury in diabetic rats. In this study, which was planned for diabetic rats induced by STZ, dexmedetomidine was shown to alleviate lung damage due to renal IR. Lung tissue damage, and oxidative stress parameters (CAT and PON activities and MDA, levels) were evaluated by spectrophotometrically. Similar to hepatic IR, Renal IR cause systemic inflammation and may affect multiple organs such as intestine, lung, and heart.1,16 In another study, they found that acute renal failure regardless of renal ischemia might cause pulmonary injury.17 Although only limited information is available kidney-lung interactions, one previous study found that dexmedetomidine attenuated lung injury induced by renal IR.18
We found that dexmedetomidine reduced lung injury due to IR. Previous studies showed that the expression of Intercellular adhesion molecule -1 (ICAM-1) and due to Tumor necrosis factor-alpha (TNF alfa) release might be responsible for local and distant organ injuries due to IR and induce neutrophil trafficking, and these effects could be attenuated by pre and post dexmedetomidine.18,19 Also, Gu et al. found that dexmedetomidine attenuated inflammatory response by reducing myeloperoxidase activity.19 In 24 hours after renal IR, neutrophil accumulation was found in the lungs.4 Previous studies showed that some enzymes could be considered as indicators of intracellular antioxidants such as CAT which is an indicator of antioxidant activity. MDA is considered a marker of cell wall peroxidation. We used CAT and MDA levels to determine the effects of dexmedetomidine on lung injury. We found that CAT and MDA levels were lower in the group given dexmedetomidine.
Dexmedetomidine has been shown to be effective to reduce local, cardiac ischemia, reperfusion injury.20 It is possible that dexmedetomidine may protect the lungs because it is known to have kidney protective effect on IR injury. Creatinine and urea are highly toxic substances that may play a role in lung injury.7 A previous study showed that inflammatory lung injury with IR was correlated with serum creatinine and kidney pathologies.4 However, it is difficult to evaluate mice kidney functions.
In animal studies, it has been shown that dexmedetomidine reduce the mortality rate and inflammatory responses.21 A previous study showed that dexmedetomidine reduced the rate of ventilation-induced lung injury in rats.22 In addition, dexmedetomidine infusion was shown to improve kidney functions.23 The protective feature of dexmedetomidine is thought to be related to the local renal protective feature and it may have positive effects on multi-organ failure.18 Moreover, if alfa-2 adrenoceptor antagonist such as atipamezole is given before dexmedetomidine application, the effects of dexmedetomidine on ICAM-1 and TNF-alfa are reduced.18
In our study, neutrophil infiltration/aggregation, alveolar wall thickness, and total lung injury scores were found to be significantly higher in Group DIR, but lower in the group given dexmedetomidine (Group DIR-D), which indicates that dexmedetomidine has protective effects on lung injury. Eroglu et al. reported that the prevention of the tissue injury after the IRI was demonstrated with most of the intravenous anesthetics like dexmedetomidine in both animal and clinical studies.24 In the future, the studies should be focused on the dosage of the anesthetics related to diminishing the tissue injuries and should be required in order to investigate the effects of the anesthetics on molecular levels.
Conclusion
In this study we found that 100 µg/kg dexmedetomidine administration intraperitoneally 30 minutes before ischemia in diabetic rats partially corrected IR-related damage in the lung. We think that dexmedetomidine administration before renal IR has a protective effect in diabetic rats.
Conflict of interest:
None declared by the authors
Authors’contribution
KS: Designing and conducting the work
KG: Manuscript editing
KA, EÖ: Histopathological evaluation of the study
AA: Literature search
KM: Biochemical examination of the study
AM: Final approval of the study
References
Department of Anesthesiology and Reanimation, Trabzon Kanuni Training and Research Hospital, Trabzon, Turkey.
Correspondence: Seyfi Kartal, Department of Anesthesiology and Reanimation, Trabzon Kanuni Training and Research Hospital, University of Health Science Turkey, Turkey.
E-mail: drseyfikartal@gmail.com; Phone: +90 462 341 56 56
Abstract
Objectives: Ischemia-reperfusion (IR) injury is a complex phenomenon, which is known to cause cell damage. In this study, we aimed to investigate the protective effects of dexmedetomidine on lung in the renal IR model in diabetic rats
Materials and Methods: After approval of the ethics committee, diabetes was induced by streptozocin (55 mg/kg) and then 24 Wistar Albino rats were randomly divided into 4 groups. Diabetic control group (group DC), diabetic dexmedetomidine (group DD), diabetic ischemia-reperfusion (group DIR), diabetic ischemia-reperfusion - dexmedetomidine (group DIR-D). In DD and DIR-D groups, 100 µ/kg dexmedetomidine was administered intraperitoneally 30 minutes before renal ischemia-reperfusion administration. In group DIR, and both artery and vein were clamped by an atraumatic vascular clamp for 120 minutes, then allowed reperfusion for 120 minutes. After then, biochemical and histopathological parameters of lung tissue samples were evaluated.
Results: Histopathologically, neutrophil infiltration/aggregation, alveolar wall thickness, and total lung injury scores were found to be significantly higher in the DIR group than in the DC, DD and DIR-D groups. In addition, neutrophil infiltration/aggregation, alveolar wall thickness, and total lung injury scores were significantly higher in the DD and DIR-D groups compared to the DC group. We found that Catalase, Paraoxonase-1 activities and malondialdehyde levels were significantly increased in DIR group compared to DC, DD and DIR-D groups (p= 0.008, p<0.0001 and p=0.001 respectively).
Conclusion: It was found that dexmedetomidine administered in diabetic rats partially corrected ischemia-reperfusion -related damage in the lung. We think that dexmedetomidine administration before renal IR has a protective effect in in diabetic rats.
Key words: Dexmedetomidine, ischemia-reperfusion, lung, renal, diabetes
Citation: Kartal S, Kip G, Küçük A, Atan A, Erdem Ö, Kavutçu M. The efficacy of dexmedetomidine on lung injury induced by renal ischemia/reperfusion in diabetic rats. Anaesth. pain intensive care 2020;24(3):272-277
Received: 17 may 2020; Reviewed: 31 May 2020; Accepted for publication: 6 June 2020
_________________________________________________________________________________
Introduction
It is a known fact that ischemia-reperfusion injuries (IR) can affect many organs in the body. The various factors are responsible for the pathogenesis of ischemia-reperfusion injury.1 Recent studies have shown that acute renal I/R causes some disfunction in both adjacent and distant organs such as heart, liver, brain, and small intestines.2 The lung is also prone to injury because of its large microcapillary network.3 Lung injury is characterized by many parameters including neutrophil infiltration/aggregation, alveolar wall thickness,4 and total lung injury score. After ischemic acute renal failure, the pulmonary injury was noticed, which is characterized by non-cardiogenic edema and neutrophil infiltration.5
Dexmedetomidine is an alpha-2 adrenergic agonist and is used for its sedative, analgesic, sympatholytic properties. Due to these beneficial effects, it is frequently preferred in trauma patients. In addition, It is shown that dexmedetomidine may reduce systemic inflammation.6 The protective effects of dexmedetomidine on ischemic injury due to I/R have been described in both adjacent and distant organs (such as pulmonary, cardiac, liver and renal). The risk of distant organ damage due to lipid peroxidation secondary to I/R has increased in diabetic patients compared to the normal population.7 In the case of I / R, there is no effective treatment of distal organ damage and it is still a serious problem.
In this study, we aimed to investigate the protective effects of dexmedetomidine on lung in the renal IR model in diabetic rats.
Methodology
Settings
This study was carried out at the Animal Experiments Laboratory of Gazi University after the approval of the Animal Ethics Local Ethics Committee (Number 18.015). The entire study methodology was performed in accordance with the guideline for the protection and care of experimental animals. 24 male Wistar albino rats weighing 200-250 gr were used for the experiment.
Procedures
The animals were allowed to access free water and food for 2 hours before the procedure with a 12-hour dark-light cycle in standard metal cages. 100 mg/kg (i.p.) of ketamine hydrochloride (Ketalar ®, Eczacıbaşı Parke-Davis, Istanbul, Turkey) was given to provide anesthesia by the cannulation of rats' tail. All procedures were performed in the supine position. Streptozotocin (STZ; Sigma Chemical, St Louis, MO, USA) at a single dose of 55 mg/kg was administered intraperitoneally (IP) to induce diabetes. After 48 hours, in case blood glucose was below 250 mg/dl, the streptozocin dose was repeated. If the blood glucose level above 250 mg/dl then it was accepted as diabetic. The experimental protocol was applied to the rats 4 weeks after the formation of diabetes.
Wistar albino rats (n:24) were randomly divided into 4 groups. Diabetic control group (Group DC), diabetic dexmedetomidine (Group DD), diabetic IR (Group DIR), diabetic IR- dexmedetomidine (Group DIR-D). In Group DD and DIR-D, 100 µg/kg dexmedetomidine was administered intraperitoneally 30 minutes before renal IR administration. In Group DIR and DIR-D both artery and vein were clamped by an atraumatic vascular clamp for 120 minutes. Then, the clamp was removed and reperfusion was achieved for 120 minutes. After the reperfusion period, biochemical and histopathological parameters of lung tissue samples were evaluated.
In Group DC, the rats were anesthetized with ketamine and no additional anesthetic agent were administered. In Group DC, an only midline laparotomy was performed and IR was not applied. In Group DIR, rats were anesthetized with ketamine and were not given dexmedetomidine. After proper disinfection, a midline laparotomy was performed. The left renal pedicle was released and both left renal artery and vein were clamped with an atraumatic vascular clamp. After 120 minutes of ischemia, reperfusion for 120 minutes was applied. In Group DD, after anesthesia, 100 µ/kg dexmedetomidine was administered intraperitoneally. IR was not applied. In Group DIR-D, 100 µ/kg dexmedetomidine was administered intraperitoneally 30 minutes before renal IR administration. Lung tissues were excised and removed, and then rats were sacrificed. Biochemical and histopathological parameters were evaluated.
Measurements of MDA levels and CAT and PON-1 activities in lung tissue
Measurement of Malondialdehyde (MDA) levels, thiobarbituric acid (TBA) reactive substances assay was performed by Van Ye et al method.8 The reaction with TBA at 90-100˚C was used to determine the MDA level, as MDA or similar substances react with TBA and produce a pink pigment that has an absorption maximum of 532 nm. To ensure protein precipitation, the sample in room temperature is mixed with cold 20% (wt/vol) trichloroacetic acid and the precipitate is then centrifuged for 10 min 3000 rpm at room temperature to form a pellet.
An aliquot of the supernatant is then placed into an equal volume of 0.6% (wt/vol) TBA in a boiling water bath for 30 min. Following cooling, sample and blank absorbance were read at 532 nm and the results expressed as nmol/mg protein, based on a graph where 1,1,3,3-tetramethoxypropane has been used as MDA standard.
The Catalase (CAT) activity is based on the measurement of absorbance decrease due to H2O2 consumption at 240 nm by Aebi H method.9
Paraoxonase (PON)-1 activity was measured the rate of hydrolysis of paraoxon by monitoring the increase of absorbance at 405 nm and at 25 °C by Brites FD. method. The basal assay mixture included 1.0 mM paraoxon and 1.0 mM CaCl2 in Tris/HCl buffer (pH: 8.0, 100 mM). The definition of 1 unit of paraoxonase activity was taken as 1 millimole of p-nitrophenol formed per min.10 The CAT and PON 1 activities were given in IU/mg protein.
Samples protein amount was determined by Lowry O method, BSA was used standard protein.11
| Table 1: Biochemical parameters of lung tissue [Mean ± SE] | |||||
| Parameter | Group DC
(n = 6) |
Group DD
(n = 6) |
Group DIR
(n = 6) |
Group DIR-D
(n = 6) |
P** |
| MDA (nmol/mg pro) | 3.37 ± 0.46* | 4.25 ± 0.38* | 7.12 ± 0.59 | 4.77 ± 0.36*+ | < 0.0001 |
| CAT (IU/mg pro) | 300.00 ± 29.27* | 298.60 ± 13.17* | 494.67 ± 57.89 | 337.00 ± 38.37* | 0.008 |
| PON (IU/mg pro) | 6.28 ± 0.63* | 7.47 ± 0.87* | 10.35 ± 0.53 | 7.63 ± 0.37* | 0.001 |
| MDA; Malondialdehyde, CAT: Catalase, PON: Paraoxonase
p**: Significance level with Kruskal Wallis test p < 0.05 *p < 0.05: compared with Group DIR + p < 0.05: compared with Group DC |
|||||
Histopathological analysis in lung tissue sections were performed blindly by histopathologist as in twenty-five different areas randomly determined in each preparation without overlap in each preparation.
| Table 2: Histopathological parameters of lung tissue [Mean ± SE] | |||||
| Parameters | Group DC
(n = 6) |
Group DD
(n = 6) |
Group DIR
(n = 6) |
Group DIR-D
(n = 6) |
P** |
| Neutrophil infiltration- aggregation | 0.33 ± 0.21* | 1.00 ± 0.00*+ | 1.83 ± 0.17 | 1.00 ± 0.26*+ | < 0.0001 |
| Alveolar wall thickness | 1.00 ± 0.00* | 2.00 ± 0.00*+ | 2.67 ± 0.21 | 2.17 ± 0.17*+ | < 0.0001 |
| Total Score | 1.33 ± 0.18* | 3.00 ± 0.00*+ | 4.50 ± 0.35 | 3.17 ± 0.31*+ | < 0.0001 |
| p**: Significance level with Kruskal Wallis test p < 0.05
*p < 0.05: compared with Group DIR + p < 0.05: compared with Group DC |
|||||
Statistical analysis
All data obtained from the semi-quantitative analyses were calculated using Statistical Package for the Social Sciences (SPSS) 22.0 (IBM, Armonk, NJ, USA) statistics program. Compliance with normal distribution was checked by the Kolmogorov-Smirnov test. In the evaluation of more than two independent groups with normal distribution, analyses were performed by using Kruskal-Wallis test. A Bonferroni adjusted Mann-Whitney U test was used after a significant Kruskal-Wallis findings to determine which group differs from the others. Results are expressed as mean ± standard error (SE). Statistical significance was set at a p < 0.05.
Results
Oxidant parameters (CAT and PON activities, MDA levels) were evaluated. We found that CAT and PON activities and also MDA levels were significantly increased in DIR group compared to DC, DD, and DIR-D groups (p = 0.008, p < 0.0001 and p = 0.03. 01 respectively). MDA levels were significantly increased in DIR group compared to DC, DD, and DIR-D groups (p < 0.0001, p < 0.0001 and p = 0.002 respectively).
Also MDA levels were higher in Group DIR-D compared to Group DC (p = 0.044). PON activities were significantly increased in DIR group compared to DC, DD, and DIR-D groups (p = 0.003, p = 0.003 and p = 0.013 respectively). Similarly, CAT activities were significantly increased in DIR group compared to DC, DD and DIR-D groups (p < 0.0001, p = 0.004 and p = 0.006 respectively). All results related to oxidant parameters are shown in Table 1.
Comparison of the findings for lung tissue neutrophil infiltration/aggregation revealed a significant difference among the groups (p < 0.0001). Neutrophil infiltration/aggregation was significantly higher in the DIR group than in the DC DD, and DIR-D groups (p < 0.0001, p = 0.002 and p = 0.016, respectively).
Neutrophil infiltration/aggregation was also significantly higher in the DIR and DIR-D groups than in the DC group (p < 0.0001 and p < 0.0001, respectively). (Table 2; Figures 1-4).
Alveolar wall thickening in lung tissue was significantly higher in the DIR group than in the DC, DD, and DIR-D groups (p < 0.0001, p = 0.001, and p = 0.001, respectively). Alveolar wall thickening was also significantly higher in the DIR and DIR-D groups than in the DC group (p < 0.0001 and p < 0.0001, respectively) (Table 2; Figures 1-4).
The lung tissue injury score was significantly higher in the DIR group than in the DC, DD, and DIR-D groups (p < 0.0001, P < 0.001 and p = 0.001, respectively). In addition, the lung tissue injury score was significantly higher in the DIR and DIR-D groups than in the DC group (p < 0.0001 and p < 0.0001, respectively) (Table 2; Figures 1-4).
Discussion
IR is a complex and biphasic process, which causes cell damage. IR injury is very important for not only adjacent organs but also distant organs. After the blood flow is re-established, reperfusion increases the rate of injury resulted from the ischemic period and aggravates the damage.1 Ischemia and/or reperfusion may be responsible for lung injury due to IR. Various ischemia-reperfusion injury models have been applied12,13 and many studies have been conducted about this issue.14,15
It is known that diabetes may affect microcirculation. Also, IR affects microcirculation. Therefore, the present study was conducted on diabetic rats to determine the effects of dexmedetomidine on lung injury in diabetic rats. In this study, which was planned for diabetic rats induced by STZ, dexmedetomidine was shown to alleviate lung damage due to renal IR. Lung tissue damage, and oxidative stress parameters (CAT and PON activities and MDA, levels) were evaluated by spectrophotometrically. Similar to hepatic IR, Renal IR cause systemic inflammation and may affect multiple organs such as intestine, lung, and heart.1,16 In another study, they found that acute renal failure regardless of renal ischemia might cause pulmonary injury.17 Although only limited information is available kidney-lung interactions, one previous study found that dexmedetomidine attenuated lung injury induced by renal IR.18
We found that dexmedetomidine reduced lung injury due to IR. Previous studies showed that the expression of Intercellular adhesion molecule -1 (ICAM-1) and due to Tumor necrosis factor-alpha (TNF alfa) release might be responsible for local and distant organ injuries due to IR and induce neutrophil trafficking, and these effects could be attenuated by pre and post dexmedetomidine.18,19 Also, Gu et al. found that dexmedetomidine attenuated inflammatory response by reducing myeloperoxidase activity.19 In 24 hours after renal IR, neutrophil accumulation was found in the lungs.4 Previous studies showed that some enzymes could be considered as indicators of intracellular antioxidants such as CAT which is an indicator of antioxidant activity. MDA is considered a marker of cell wall peroxidation. We used CAT and MDA levels to determine the effects of dexmedetomidine on lung injury. We found that CAT and MDA levels were lower in the group given dexmedetomidine.
Dexmedetomidine has been shown to be effective to reduce local, cardiac ischemia, reperfusion injury.20 It is possible that dexmedetomidine may protect the lungs because it is known to have kidney protective effect on IR injury. Creatinine and urea are highly toxic substances that may play a role in lung injury.7 A previous study showed that inflammatory lung injury with IR was correlated with serum creatinine and kidney pathologies.4 However, it is difficult to evaluate mice kidney functions.
In animal studies, it has been shown that dexmedetomidine reduce the mortality rate and inflammatory responses.21 A previous study showed that dexmedetomidine reduced the rate of ventilation-induced lung injury in rats.22 In addition, dexmedetomidine infusion was shown to improve kidney functions.23 The protective feature of dexmedetomidine is thought to be related to the local renal protective feature and it may have positive effects on multi-organ failure.18 Moreover, if alfa-2 adrenoceptor antagonist such as atipamezole is given before dexmedetomidine application, the effects of dexmedetomidine on ICAM-1 and TNF-alfa are reduced.18
In our study, neutrophil infiltration/aggregation, alveolar wall thickness, and total lung injury scores were found to be significantly higher in Group DIR, but lower in the group given dexmedetomidine (Group DIR-D), which indicates that dexmedetomidine has protective effects on lung injury. Eroglu et al. reported that the prevention of the tissue injury after the IRI was demonstrated with most of the intravenous anesthetics like dexmedetomidine in both animal and clinical studies.24 In the future, the studies should be focused on the dosage of the anesthetics related to diminishing the tissue injuries and should be required in order to investigate the effects of the anesthetics on molecular levels.
Conclusion
In this study we found that 100 µg/kg dexmedetomidine administration intraperitoneally 30 minutes before ischemia in diabetic rats partially corrected IR-related damage in the lung. We think that dexmedetomidine administration before renal IR has a protective effect in diabetic rats.
Conflict of interest:
None declared by the authors
Authors’contribution
KS: Designing and conducting the work
KG: Manuscript editing
KA, EÖ: Histopathological evaluation of the study
AA: Literature search
KM: Biochemical examination of the study
AM: Final approval of the study
References
- Montalvo-Jave EE, Escalante-Tattersfi eld T, Ortega-Salgado JA, Piña E, Geller DA. Factors in the pathophysiology of the liver ischemia–reperfusion injury. J Surg Res. 2008;147:153–159. [PubMed] DOI: 1016/j.jss.2007.06.015
- Kelly KJ. Distant effects of experimental renal ischemia/ reperfusion injury. J Am Soc Nephrol. 2003;14:1549–1558. [PubMed] DOI: 1097/01.asn.0000064946.94590.46
- Rabb H, Chamoun F, Hotchkiss J. Molecular mechanisms underlying combined kidney-lung dysfunction during acute renal failure. Contrib Nephrol. 2001;132:41–52. [PubMed] DOI: 1159/000060080
- Grigoryev DN, Liu M, Hassoun HT, Cheadle C, Barnes KC, Rabb H. The local and systemic inflammatory transcriptome after acute kidney injury. J Am Soc Nephrol. 2008;19:547–558. [PubMed] DOI: 1681/ASN.2007040469
- Deng J, Hu X, Yuen PS, Star RA. Alpha-melanocyte-stimulating hormone inhibits lung injury after renal ischemia/ reperfusion. Am J Respir Crit Care Med. 2004;169:749–756. [PubMed] DOI: 1164/rccm.200303-372OC
- Qiao H, Sanders RD, Ma D, Wu X, Maze M. Sedation improves early outcome in severely septic Sprague Dawley rats. Crit Care. 2009;13(4):R136. [PubMed] DOI: 1186/cc8012
- Rajakumaraswamy N, Ma D, Hossain M, Sanders RD, Franks NP, Maze M. Neuroprotective interaction produced by xenon and dexmedetomidine on in vitro and in vivo neuronal injury models. Neurosci Lett. 2006;409:128–133. [PubMed] DOI: 1016/j.neulet.2006.09.020
- Van Ye TM, Roza AM, Pieper GM, Henderson J Jr, Johnson CP, Adams MB. Inhibition of intestinal lipid peroxidation does not minimize morphologic damage. J Surg Res. 1993;55:553-558. [PubMed] DOI: 1006/jsre.1993.1183
- Aebi H. Catalase. In: H.U.Bergmeyer. methods of enzymatic analysis. New York and London: Academic Press; 1974. p.673-677.
- Brites FD, Verona J, Schreier LE, Fruchart JC, Castro GR, Wikinski RL. Paraoxonase 1 and platelet-activating factor acetylhydrolase activities in patients with low hdl-cholesterol levels with or without primary hypertriglyceridemia. Arch Med Res. 2004;35:235-240. [PubMed] DOI: 1016/j.arcmed.2004.02.002
- Lowry O, Rosenbraugh N, Farr L, Randall R. Protein measurement with folin phenol reagent. J Biol Chem. 1951;182:265-275. [PubMed]
- Yamamoto K, Wilson DR, Baumal R. Outer medullary circulatory defect in ischemic acute renal failure. Am J Pathol. 1984;116:253-261. [PubMed]
- Arendshorst WJ, Finn WF, Gottschalk CW. Pathogenesis of acute renal failure following temporary renal ischemia in the rat. Circ Res. 1975;37:558-568. [PubMed] DOI: 1161/01.res.37.5.558
- Tufek A, Tokgoz O, Aliosmanoglu I, Alabalik U, Evliyaoglu O, Ciftci T, et al. The protective effects of dexmedetomidine on the liver and remote organs against hepatic ischemia reperfusion injury in rats. Int J Surg. 2013;11:96-100. [PubMed] DOI: 1016/j.ijsu.2012.12.003
- Wang Y, Ji M, Chen L, Wu X, Wang L. Breviscapine reduces acute lung injury induced by left heart ischemic reperfusion in rats by inhibiting the expression of ICAM-1 and IL-18. Exp Ther Med. 2013;6:1322-1326. [PubMed] DOI: 3892/etm.2013.1287
- Carden DL, Granger DN. Pathophysiology of ischaemiareperfusion injury. J Pathol. 2000;90:255–266. [PubMed] DOI: 1002/(SICI)1096-9896(200002)190:3<255::AID-PATH526>3.0.CO;2-6
- Hoke TS, Douglas IS, Klein CL, He Z, Fang W, Thurman JM, et al. Acute renal failure after bilateral nephrectomy is associated with cytokine-mediated pulmonary injury. J Am Soc Nephrol. 2007;18:155–164. [PubMed] DOI: 1681/ASN.2006050494
- Gu J, Chen J, Xia P, Tao G, Zhao H, Ma D. Dexmedetomidine attenuates remote lung injury induced by renal ischemia-reperfusion in mice. Acta Anaesthesiol Scand. 2011;55:1272–1278. [PubMed] DOI: 1111/j.1399-6576.2011.02526.x
- Hoke TS, Douglas IS, Klein CL, He Z, Fang W, Thurman JM, et al. Acute renal failure after bilateral nephrectomy is associated with cytokine-mediated pulmonary injury. J Am Soc Nephrol. 2007;18(1):155–164. [PubMed] DOI: 1681/ASN.2006050494
- Koçoğlu H, Karaaslan K, Gonca E, Bozdogan O, Gulcu N. Preconditioning effects of dexmedetomidine on myocardial ischemia/reperfusion injury in rats. Curr Ther Res. 2008;69:150-158. [PubMed] DOI: 1016/j.curtheres.2008.04.003
- Taniguchi T, Kurita A, Kobayashi K, Yamamoto K, Inaba H. Dose- and time-related effects of dexmedetomidine on mortality and inflammatory responses to endotoxin-induced shock in rats. J Anesth. 2008;22:221–228. [PubMed] DOI: 1007/s00540-008-0611-9
- Yang CL, Tsai PS, Huang CJ. Effects of dexmedetomidine on regulating pulmonary inflammation in a rat model of ventilator-induced lung injury. Acta Anaesthesiol Taiwan. 2008;46:151–159. [PubMed] DOI: 1016/S1875-4597(09)60002-3
- Frumento RJ, Logginidou HG, Wahlander S, Wagener G, Playford HR, Sladen RN. Dexmedetomidine infusion is associated with enhanced renal function after thoracic surgery. J Clin Anesth. 2006;18:422–426. [PubMed] DOI: 1016/j.jclinane.2006.02.005
- Eroglu A. The effect of intravenous anesthetics on ischemia-reperfusion injury. Biomed Res Int. 2014;2014:821513. [PubMed] DOI: 1155/2014/821513