
M.M. Rifat Chowdhury1, MdShafiqul Islam2, D.K. Bhowmick2,
Md Mustafa Kamal3,AKMAkhtaruzzaman4
1Resident; 2Assistant Professor;3Associate Professor; 4Professor of Neuroanesthesia
+Department of Anesthesia, Analgesia and Intensive Care Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka (Bangladesh)
Correspondence: Dr AKM Akhtaruzzaman, Professor of Neuroanesthesia
Department of Anesthesia, Analgesia and Intensive Care Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka(Bangladesh);Phone: +8801819220195; Email: akhtaruzzaman.akm@gmail.com
ABSTRACT
Background and Aims: Hypotensive anesthesia is preferred in craniotomy. Current study was conducted to evaluate the effects of oral clonidine premedication upon hemodynamic status, dural tightness and quality of anesthesia using 3 point scoring system in patients scheduled for craniotomy under general anesthesia.
Methodology: Amongst twenty two selected cases they were grouped equally in this randomized single – blind comparative study. GroupA and B patientsreceived sugar tablet and oral clonidine 3 µg/kg as a premedication respectively. Monitoring of hemodynamic variables like heart rate, systolic arterial pressure, diastolic arterial pressure, mean arterial pressure, SpO2, ETCO2anddural tightness were performed.
Results: Diastolic arterial pressure was significantly low in Group B during positioning, performing burr hole and during dura incision. Mean arterial pressure was highly significantfor Group B during positioning. Heart rate change was significantly high for Group B during burr hole. Regarding dural tightness, 10 patients in Group Band 6 in Group A had no dural swelling.1 patient in Group Band 5 patients in Group A had minimal swelling and surgery continued. Once all results being assessed using ‘Three point scoring system’, it became highly significant in Group B with respect to Group A.
Conclusion: Oral clonidine premedication provides optimal hemodynamic stability and good neuro-surgical comprising heart rate, mean arterial pressure and dural tightness. ‘Three point scoring system’ seems to be an effective tool for intra-operative monitoring of patients undergoing supra-tentorial craniotomy.
Keywords: Clonidine, Neuroanesthesia, Supra-tentorial space occupying lesion, Craniotomy, Hemodynamic, Dural tightness.
Citation: Chowdhury MMR, Islam MS, Bhowmick DK, Kamal MM, Akhtaruzzaman AKM. Effects of clonidine on hemodynamic response and dural tightness in patients with supra-tentorial space occupying lesion undergoing craniotomy- a placebo controlled comparative study. Anaesth Pain & Intensive Care 2015;19(3)233-239
INTRODUCTION
Craniotomy induced surgical stimuli predisposes sympathetic activation and marked changes in systemic arterial pressure, cerebral blood flow and intracranial pressure. Cerebrovascular changes can cause raised ICP, decrease in cerebral perfusion pressure, more marked in patients having deranged auto-regulation and compromised cerebral compliance. Obtundation of the hemodynamic responses to painful stimuli is a prerequisite to ensure optimal cerebral homeostasis during neurosurgical procedure.
Alpha 2 adrenargic receptors are distributed widely within and outside the CNS, mostly in the region of pons and medulla which regulates transmission of sympathetic nervous system stimulation from higher centers to the periphery. Pre-synaptic α2-receptors activation inhibits release of nor-epinephrine. Whereas, α2-adrenoceptors situated post-synaptic in the dorsal horn andon vascular smooth muscle when stimulated prevents nociceptive signal transmission and causes vasoconstriction respectively.1,2
Clonidine is used primarily for its α2 receptor mediated antihypertensive effects. Stimulation of α2 receptors by Clonidine in the central nervous system has role on sedation for which clonidine is widely used as an adjunct to anesthesia and pain medicine3.
Clonidine reduces sympathetic tone and the release of nor-epinephrine from nerve terminals4. During general anesthesia, clonidine reportedly enhances intra-operative circulatory stability by reducing catecholamine levels.5 Therefore, the use of clonidine during surgery has been proposed as a way of improving perioperative hemodynamics, decreasing both the intracranial pressure and anesthetic requirements. Clonidine is well absorbed after oral administration. The peak concentration in plasma and the maximal hypotensive effect are observed 1 to 3 hours after an oral dose. The elimination half-life of the drug ranges from 6 to 24 hours, with a mean of about 12 hours.6
This central and peripheral effect of clonidine may explain the improvement in metabolic control. Clonidine given as a premedication improves cardiovascular stability and blunts the cardiovascular response to laryngoscopy, intubation and surgery.7 Clonidine prevents fluctuation of hemodynamics throughout the entire perioperative period, which is very important in neurosurgical patients.8
This study was designed to determine whether premedication with oral clonidine provide optimal hemodynamic stability, as well as good neurosurgical compliances for craniotomy under general anesthesia and the three point scoring system can evaluate the patient’s hemodynamic condition and the dural tightness, ultimately quality of surgical anesthesia.
METHODOLOGY
This randomized single-blind comparative study was conducted from January to September 2014at Bangabandhu Sheikh Mujib Medical University, Bangladesh.
After institutional ethical committee approval and informed written consent, a total of 22 patients of ASA physical status 1and2, aged 30-50 years undergoing craniotomy under general anesthesia were recruited. They were grouped randomly by lottery method composed of 11 patients in each group where Group A received oral sugar tablet and Group B received oral clonidine 3 µg/kg.
Patient’s refusal to participate in the study, emergency surgery, ASA–more than II, patient with morbid obesity, hypertension, on β blocker or α blocker, having coagulopathy or patient taking anti-platelet medications were excluded.
Patients received sugar tablet or clonidine tablet 90 minutes before induction of general anesthesia. A large bore intravenous catheter was placed. Electrocardiogram leads, blood pressure cuff and pulse-oximeter were also placed. Every patient’s received inj. Midazolam 1mg intravenously before induction. Once pre-oxygenated with 100% oxygen for three minutes, inj. vecuronium 0.1mg/kg followed by propofol (2mg/kg), fentanyl 2µg/kg were given intravenously. Each patient was intubated with proper size endotracheal tube and Capnometer was placed with it. Anesthesia was maintained with N2O in O2 (60:40) andisoflurane at a MAC less than 0.5%. Inj.fentanyl in increments of 0.4µg/kg9andinj. vecuronium was administered using syringe-pump at 1 µg /kg/min. Bladder catheterization was done. Proper positioning of patient with care of pressure areas and padding of eyes were done. Both groups received mannitol20% 1 gm/kg (IV) when scalp incision was given. Controlled ventilation was adjusted to maintain ETCO2 at 28-32 mmHg in both groups. The time intervals between induction of anesthesia, intubation, and pin head-holder application were also kept as constant as possible, with time between induction of anesthesia and pin head-holder application never exceeding 30 min. Hemodynamic variables like systolic arterial pressure, diastolic arterial pressure, mean arterial pressure and heart rate of all patients were continuously recorded by using Philips monitor (IntelliVue MP30, Germany).All these were recorded before induction, just after intubation, during positioning, local infiltration, skin incision, burr hole, dura incision, 30 min and 60 min after dura opening respectively.
Optimal anesthetic condition concerning dural tightness were assessed by scoring system in many occasions by different authors in their study.10,11In this study we used ‘three point scoring system’ based on mean arterial pressure, heart rateand dural tightness. Each was assessed withscoresof1-3, total point rangedfrom 3 to 9.
Mean arterial pressure rated 1 point if it was < 60-70 mmHg, 2 point if it was 71- 90 mmHg and 3 point if it was > 91 mmHg.
Heart rate rated 1 point if it was <70 b/min, 2 point if it was 71-90 b/min and 3 point if it was > 91 b/min.
Dural tightness rated 1 point if there was no swelling, 2 points if there was minimal swelling but surgery continued and 3 points if there was severe swelling and surgery was postponed. Dural condition and tension were measured subjectively by surgeons. Tension of dura was used as a guide. Just before opening the dura, surgeons were asked to provide an assessment of the condition of the brain.
Isoflurane and N2O were discontinued after skin closure. Patients were reversed with neostigmine 0.05 mg/kg and atropine 0.015 mg/kg and Extubation was done when adequate spontaneous ventilation resumed.
Adverse effects like hypotension (SAP<90 mmHg), bradycardia (HR <60bpm), respiratory depression, nausea, vomiting or allergic manifestations if occurred were recorded.
Statistical analysis was done using software SPSS (Statistical Package for Social science), version 17. Demographic data and hemodynamic data were analyzed using unpaired student’s t-test. Dural tightness and three point scoring system were analyzed using chi-squire (X2) test. Statistically significance was set at p-value <0.05.
RESULT
Two groups matched statistically comprising age (p= 0.18), weight(p= 0.92) and sex (p=1.00) having no difference between them (Table 1).
Table 1: Demographic variables
|
Variables |
Group A |
Group B |
p-value |
|
| Age (years) |
41.73 ±8.95 |
39.0 ±6.66 |
0.18 (NS) |
|
| Weight (kg) |
60.09 ±6.77 |
61.91 ±6.73 |
0.92 (NS) |
|
|
Sex |
Male |
6 (54.55) |
7 (63.64) |
1.00 (NS) |
| Female |
5 (45.45) |
4 (36.36) |
||
All values were presented as mean ± SD or in frequencies. Data were analyzed using unpaired student’s t-test and Chi-square test as appropriate. Statistically significance was set at p-value <0.05. (NS- Not significant)
Hemodynamic variables like heart rate (p= 0.44), systolic arterial pressure (p= 0.60) and diastolic arterial pressure (p= 0.27) were almost identical in both groups which were insignificant.
Systolic arterial pressure of Group B before induction was 127 ± 10 mmHg and during different evaluation period varied from 127.27 ± 10 mmHg to 94.82 ± 5 mmHg. On the other hand SAP of Group A before induction was 136.0 ± 12 mmHg and during different evaluation period ranged from 141.46 ± 28 mmHg to 110.90 ± 16 mmHg. The changes were not statistically significant in both groups.
Although diastolic arterial pressures of both the groups were within acceptable range during different observation period, Group B exhibited relatively low during positioning, burr hole and dura incision which were significant statistically (p=<0.05).
Mean arterial pressure of both groups followed the same trend regarding fluctuation of pressure as that of systolic arterial pressure, having no statistically significant changes. Only MAP during positioning in clonidine group revealed change which was significant statistically (p ≤ 0.05)(Figure 1).
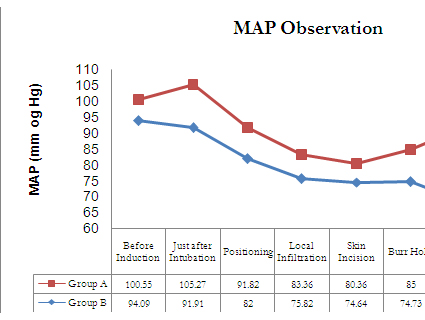
Figure 1: Comparison of mean arterial pressure
In Group B, heart rate (Figure 2) found gradually decline and then rise again after dura was opened. On the other hand in Group A, though heart rate was rising initially but started to fall after intubation. No statistically significant changes were found during different evaluation periods except during burr hole which was statistically significant (p ≤ 0.05).
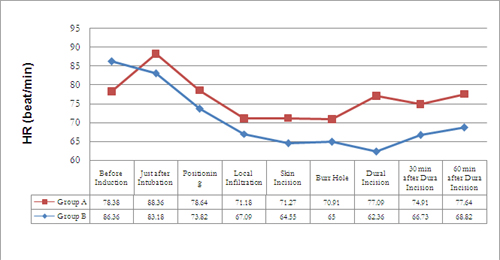
Figure 2: Comparison of mean heart rate at different time interval
In GroupB 10 (90.9%) patients had had no dural swelling while 1 patient (9.09%) had minimal swelling and the surgery continued. On the other hand in GroupA6 (54.5%) patients had no dural swelling but the remaining 5 (4 5.5%) patients developed minimal swelling and surgery continued (Figure 3).
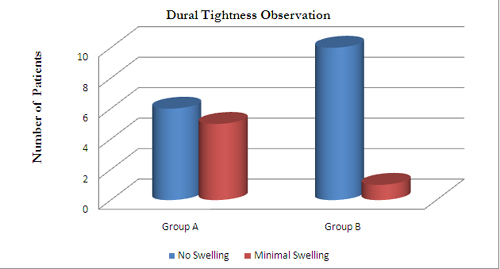
Figure3: Comparison of dural tightness during dural incision in twogroups
The ‘three point scores’ were obtained from mean arterial pressure, heart rate and dural tightness during dural opening (Table 2). Among Group B, we found 9 patients (81.82%) had scored 3-4, which was considered as good and the rest 2 patients (18.18%) scored 5-7, considered as acceptable with respect to three points score. On the contrary only 1 patient (90.91%) scored 3-4 in Group A, considered as good but the remaining 10 patients (90.91%) had acceptable scores between5-7. No group had scored “8-9”. Group B became significant statistically (P< 0.01) in comparison to Group A.
Table 2: Three points scoring in both groups [n (%)]
|
Scoring |
Group |
p-Value |
Significancelevel |
|
|
A |
B |
|||
| Good (Score 3-4) |
1(9.09) |
9(81.82) |
<0.01*** |
HS |
| Acceptable (Score 5-7) |
10(90.91) |
2(18.18) |
||
| Not acceptable (Score 8-9) |
0(0.0) |
0(0.0) |
||
Values were expressed as number and within parentheses are percentages over column total. Data were analyzed usingChi-squire test. Statistically significance was set at p-value <0.05. (HS– Highly Significant)
DISCUSSION
Craniotomy is the most common surgical management for supra-tentorial space occupying lesion, where hypotensive anesthesia is preferred. Well Controlled hemodynamic variables is considered gold standard, where maintenance of optimal cerebral perfusion pressure is desired.
Clonidine possesses some unique properties that make it a suitable adjunct for managing neurosurgical patients intra-operatively. Clonidine decreases total peripheral resistance, renal vascular resistance, heart rate and blood pressure12 through α2-receptor mediated action. It depresses electrical function and decreases cortical response, thereby leads to reduced anesthetic requirements associated with clonidine administration.13
Positioning (head-holder insertion) is an intense painful stimulus which simultaneously with endotracheal intubation and surgical incision remarkably increases mean arterial pressure and heart rate14. Most institutions follow the technique of tightening head holder in anesthetized patients using pressure equals to 80 pounds. To avoid undesired elevation in blood pressure, heart rate and ICP, obtunding these stimuli should be preferred during neurosurgery.
The effect of clonidine on intra-operative hemodynamic status as well as dural tightness during dural incision was evaluated. In this study, we collected data of mean arterial pressure and heart rate at same time. In addition, data for dural tightness during dural incision to establish three point scoring system were also collected. In a previous study by Selina et.Al,15 monitoring of only mean arterial pressure and pulse were done not including dural tightness into consideration.
Both the groups did not differ with respect to age, weight and sex. All preoperative baseline hemodynamic variables were almost identical in both groups (p>0.05). Effect of clonidine on hemodynamic responses was monitored. Just after intubation there was increase inSAP from (136 ± 12) mmHg to (141 ± 28) mmHgin Group A where as in Group Btherewas a slight decrease from (127 ± 10) mmHg to (124 ± 18) mmHg (p= 0.17). This correlates with another study,16 where the effect of clonidine pre-medication on hemodynamic responses was measured during micro-laryngoscopy and fiberopticbronchoscopy.
Baseline HR in Group B was higher but per-operative HR was lower than the Group A. In addition, in Group B, HR change to laryngoscopy was not observed. This correlates with other studies17 that had demonstrated a bradycardia or unchanged HR as the response to intubation after clonidine pretreatment.
Clonidine reduced baseline MAP in comparison to placebo group. Nevertheless, insignificant difference regarding blood pressure response to laryngoscopy between groups was revealed. Possibly this result predicts the desired optimal level of anesthesia conducted to patients according to titration.
Our study shows the changes in mean pressure at different time intervals following intubation. The mean pressure of both groups at different time intervals from intubation followed the similar pattern as systolic and diastolic blood pressure did. The mean pressure of the Group B decreased steadily throughout the intra-operative period, while that of the Group A showed fluctuation in successive period of evaluation. In a previous study,18 oral clonidine (5µg/kg) was used as pre-anesthetic medication and observed the fluctuation of mean arterial pressure during head pin insertion in case of skull base procedure. According to their study fluctuation of mean arterial pressure was minimum.
Mean arterial pressure was lower in most of the period for Group B. It was highly significant during positioning (p=0.01) in clonidine group. There was highly significant change in diastolic arterial pressure during positioning (p= 0.04), burr hole (p= 0.03) and dural incision (p= 0.001) in case of diastolic arterial pressure, inGroup B.
Only 6 (54.54%) patients of GroupA and10 (90.91%) patients of GroupB had no dural swelling but it was statistically insignificant. Considering three point scoring system with MAP, HR and Dural tightness during dura opening, Group B became highly significant(p≤ 0.01) in comparison to Group A.
Hypotension is a potential complication when clonidine co-administered with anesthetic induction agents. In our study, no patient in both groups required rescue treatment for hypotension. In another study19 vasopressors were required for 8 patients in clonidine group and 2 patients in placebo group where CPP came down below 60 mmHg. Perhaps it was due to different method of clonidine administration. Intravenous clonidine has the propensity to develop accentuated hypotension compared to orally administered form. No other complications were observed.
CONCLUSION
The present study shows that oral clonidine premedication in Neuroanesthesia for patients with supra-tentorial space occupying lesion provides stable hemodynamics and optimal intra-cranial pressure intra-operatively. Moreover, in our opinion ‘3 point scoring system’ represents an effective tool to assess per-operative condition in supra-tentorial craniotomy.
Conflict of interests: The authors have no conflicts of interest to disclose.
Funding: None
Authors Contribution:
MMRC: Data collection
MSI: Manuscript writing
DKB: Protocol designing, reference collection
MMK: Data collection
AKMA: Statistical analysis, manuscript correction, over-all supervision
REFERENCES
- Calzada BC, De Artinano AA. Alpha-adrenoceptor subtypes. Pharmacol Res 2001;44(3):195-208.[PubMed]
- ScheininM, PihlavisisM. Molecular pharmacology of α2 adenoreceptor agonists, in Scholz J, Tonner PH (eds): Bailliere’s Best Practice and Research: Clinical Anesthesiology α2-Adenoreceptor Agonists in Anaesthesia and Intensive Care, London, Bailliere Tindall, 2000;247-60.
- Kamibayashi T, Maze M. Clinical uses of alpha 2-adrenergic agonists. Anesthesiology 2000;93(5):1345-49.[PubMed][Free full text]
- Quintin L, Roudot F, Roux C, Macquin I,Basmaciogullari A, GuyeneT, et al. Effect of clonidine on thecirculation and vasoactive hormones after aortic surgery.Br J Anaesth. 1991;66:108-115. [PubMed][Free full text]
- Edward Morgan, Jr. Maged, S. Mikhail, Michael J. Murray. Clinical Anesthesiology 5th edition, New York, McGraw-Hill, 2013;245.
- Atlas D, Steer M L. Clonidine p-isothiocyanate, an affinity label for alpha 2-adrenergic receptors on human platelets. Proc Natl AcadSci U S A, 1982;79(5):1378–82.[PubMed][Free full text]
- Engelman E, Lipszyc M, Gilbart E, Linden P, Bellens B, Romphey A, et al. Effect of clonidine on anaesthetic drug requirements and hemodynamic response during aortic surgery. Anesthesiology 1989;71(2):178-188.[PubMed][Free full text]
- Costello TG, Cormack JR. Clonidine premedication decreases hemodynamic responses to pin head-holder application during craniotomy. AnesthAnalg 1998;86(5):1001–4.[PubMed]
- Priyanka S, Sourabh M, Atmaram P, Varshali K, Sushma L. A comparison study of dexmedetomidine vs clonidine for sympathoadrenal response, perioperative drug requirements and cost analysis. Asian Pacific Journal of Tropical Disease12/2012; 2(Suppl 2). DOI: 10.1016/S2222-1808(12)60271-0
- Santra S, Das B. Subdural pressure and brain condition during propofol vs isoflurane – nitrous oxide anaesthesia in patients undergoing elective supratentorialtumour surgery. Indian J Anaesth. 2009 Feb;53(1):44-51.[PubMed][Free full text]
- Petersen KD, Landsfeldt U, Cold GE, Petersen CB, Mau S, Hauerberg J, et al. Intracranial pressure and cerebral hemodynamic in patients with cerebral tumors: a randomized prospective study of patients subjected to craniotomy in propofol–fentanyl, isoflurane–fentanyl, or sevoflurane–fentanyl anesthesia. Anesthesiology 2003;98(2):329-336. [PubMed][Free full text]
- Svensson TH, Bunney BS, Aghajanian GK. Inhibition of both noradrenergic and serotonergic neurons in brain by the a adrenergic agonist clonidine. Brain Res 1975;92:291-306.[PubMed]
- Ghignone M, Calvillo O, Quintin L. Anesthesia and hypertension: the effect of clonidine on perioperative hemodynamics and isoflurane requirements. Anesthesiology 1987;67(1):3-10.[PubMed][Free full text]
- Shapiro HM, Wyte SR, Harris AB, Galindo A. Acute intraoperative hypertension in neurosurgical patients: mechanical and pharmacologic factors. Anesthesiology 1972;37(4):399-405.[PubMed]
- Selina F, Talha KA, Akhtaruzzaman AKM. Effect of oral clonidine on stability of mean blood pressure in craniotomy. Journal of Medical Science Research 2007;9(1):8-14.[PubMed]
- Matot I, Sichel JY, Valeri Y, Yaacov G. Effect of clonidine premedication on haemodynamic responses to Microlaryngoscopy and Rigid bronchoscopy. Anesthesia and Analgesia 2000;91(4):828-833.[PubMed]
- Chadha R, Padmanabham V, Joseph A, Mohandas K. Oral clonidine pretreatment for haemodynamic stability during craniotomy. Anaesth Intensive Care. 1992;20(3):341-344.[PubMed]
- JellishWS ,Theard MA, Cheng MA, Leonetti JP, Crowder CM, Tempelhoff R. The effects of clonidine premedication and scalp infiltration of lidocaine on hemodynamic responses to laryngoscopy and skull pin head-holder insertion during skull base procedures. Skull Base 2001;11(3):169–176.[PubMed]
- Favre, J.B. Gardaz, J. P. Ravussin, P. Effect of clonidine on ICP and on the hemodynamic responses to nociceptive stimuli in patients with brain tumors.J NeurosurgAnesthesiol. 1995;7(3):159-167.[PubMed]
